Structure of the pharynx
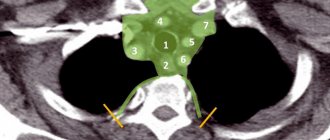
In an adult, the pharynx is a funnel-shaped tube about 10–15 cm long, located behind the nasal and oral cavities and larynx. The upper wall of the pharynx is fused with the base of the skull; in this place on the skull there is a special protrusion - the pharyngeal tubercle. The cervical spine is located behind the pharynx, so the lower border of the pharynx is determined at the level between the VI and VII cervical vertebrae: here it narrows and passes into the esophagus. Large vessels (carotid arteries, internal jugular vein) and nerves (vagus nerve) are adjacent to the lateral walls of the pharynx on each side.
According to the organs located anterior to the pharynx, it is divided into 3 parts: upper - nasal, middle - oral - and lower - laryngeal.
Nasopharynx The nasal part of the pharynx (nasopharynx) serves only to conduct air. From the nasal cavity, air enters this part of the pharynx through 2 large openings called choanae. Unlike other parts of the pharynx, the walls of its nasal part do not collapse, because they are firmly fused with the neighboring bones.
Oropharynx The oral part of the pharynx (oropharynx) is located at the level of the oral cavity. The function of the oral part of the pharynx is mixed, since both food and air pass through it. The transition point from the oral cavity to the pharynx is called the pharynx. From above, the pharynx is limited by a hanging fold (velum palatine), ending in the center with a small tongue. With each swallowing movement, as well as when pronouncing guttural consonants (g, k, x) and high notes, the velum palatine rises and separates the nasopharynx from the rest of the pharynx. When the mouth is closed, the tongue adheres tightly to the tongue and creates the necessary tightness in the oral cavity, preventing the lower jaw from sagging.
Laryngeal part of the pharynx The laryngeal part of the pharynx is the lowest part of the pharynx, lying behind the larynx.
On its front wall there is an entrance to the larynx, which is closed by the epiglottis, which moves like a “lifting door”. The wide upper part of the epiglottis descends with each swallowing movement and closes the entrance to the larynx, preventing food and water from entering the respiratory tract. Water and food move through the laryngeal part of the pharynx into the esophagus.
Chronic processes
Among chronic lesions of the pharynx, the following are often diagnosed:
- Chronic pharyngitis is a disease characterized by lesions of the mucous membrane of the pharyngeal posterior wall and lymphoid tissue as a result of acute or chronic damage to the tonsils, paranasal sinuses, and so on.
- Pharyngomycosis is damage to the tissues of the pharynx caused by yeast-like fungi and developing against the background of immunodeficiency.
- Chronic tonsillitis is an autoimmune pathology of the palatine tonsils. In addition, the disease is allergic-infectious and is accompanied by a persistent inflammatory process in the tissues of the palatine tonsils.
Interaction of the pharynx with the tympanic cavity
On the side walls of the nasal part of the pharynx, on each side there is an opening of the auditory tube, which connects the pharynx with the tympanic cavity. The latter belongs to the organ of hearing and is involved in sound transmission. Due to the connection between the tympanic cavity and the pharynx, the air pressure in the tympanic cavity is always equal to atmospheric pressure, which creates the necessary conditions for the transmission of sound vibrations. Any person has probably encountered the effect of stuffy ears when taking off from an airplane or going up in a high-speed elevator: the ambient air pressure changes quickly, but the pressure in the tympanic cavity does not have time to adjust. The ears become blocked, the perception of sounds is impaired. After some time, hearing is restored, which is facilitated by swallowing movements (yawning or sucking on a lollipop). With each swallow or yawn, the pharyngeal opening of the auditory tube opens and a portion of air enters the tympanic cavity.
Treatment of the pharynx and esophagus in the department of thoracoabdominal surgery and oncology
Treatment in the department is carried out under the programs of compulsory medical insurance, voluntary medical insurance, VMP, as well as on a commercial basis. Read how to get treatment at the Department of Thoracoabdominal Surgery and Oncology of the Russian Scientific Center for Surgery.
To schedule a consultation, call:
+7 (499) 248 13 91 +7 (903) 728 24 52 +7 (499) 248 15 55
Submit a request for a consultation by filling out the form on our website and attaching the necessary documents.
The structure and significance of the tonsils
In the nasal part of the pharynx there are such important formations as the tonsils, which belong to the lymphoid (immune) system. They are located on the path of possible introduction of foreign substances or microbes into the body and create a kind of “security posts” on the border of the internal and external environment for the body.
The unpaired pharyngeal tonsil is located in the area of the fornix and posterior wall of the pharynx, and the paired tubal tonsils are located near the pharyngeal openings of the auditory tube, i.e., in the place where microbes, along with the inhaled air, can enter the respiratory tract and tympanic cavity. Enlargement of the pharyngeal tonsil (adenoid) and its chronic inflammation can lead to difficulty in normal breathing in children, so it is removed.
In the area of the pharynx, at the border of the oral cavity and pharynx, there are also paired palatine tonsils - on the side walls of the pharynx (sometimes in everyday life they are called tonsils) - and the lingual tonsil - at the root of the tongue. These tonsils play a significant role in protecting the body from pathogens that enter through the mouth. With inflammation of the palatine tonsils - acute or chronic tonsillitis (from the Latin tonsilla - tonsil) - there may be a narrowing of the passage to the pharynx and difficulty swallowing and speech.
Thus, in the pharynx area, a kind of ring of tonsils is formed, which participate in the body’s defense reactions. The tonsils are significantly developed in childhood and adolescence, when the body grows and matures.
Inflammatory acute processes
Among the inflammatory diseases that occur acutely, the following can be distinguished:
- Acute pharyngitis is damage to the lymphoid tissue of the pharynx due to the proliferation of viruses, fungi or bacteria in it.
- Candidiasis of the pharynx is damage to the mucous membrane of the organ by fungi of the genus Candida.
- Acute tonsillitis (tonsillitis) is a primary lesion of the tonsils, which is infectious in nature. Sore throats can be: catarrhal, lacunar, follicular, ulcerative-filmic.
- An abscess in the area of the root of the tongue is purulent tissue damage in the area of the hyoid muscle. The cause of this pathology is infection of wounds or as a complication of inflammation of the lingual tonsil.
Structure of the pharyngeal wall
The basis of the pharyngeal wall is formed by a dense fibrous membrane, which is covered on the inside by the mucous membrane and on the outside by the muscles of the pharynx. The mucous membrane in the nasal part of the pharynx is lined with ciliated epithelium - the same as in the nasal cavity. In the lower parts of the pharynx, the mucous membrane acquires a smooth surface and contains numerous mucous glands that produce a viscous secretion, which helps the bolus of food slide when swallowing.
Among the muscles of the pharynx, longitudinal and circular are distinguished. The circular layer is much more pronounced and consists of 3 constrictor muscles (constrictors) of the pharynx. They are located in 3 floors, and their sequential contraction from top to bottom leads to the pushing of the food bolus into the esophagus. When swallowing, two longitudinal muscles expand the pharynx and lift it towards the bolus of food. The muscles of the pharynx work in concert with every swallowing movement.
Benign tumors
Benign tumors are considered any voluminous neoplasms that comply with the “rule of three NOTs”:
- they do not metastasize,
- do not infiltrate nearby tissues
- and do not recur after removal.
Pharynx tumors
Benign neoplasms of the pharynx include adenoma, lipoma, neurofibroma, papilloma, teratoma, angioma, plasmacytoma and cysts.
In mild cases (with small sizes and specific localization), benign laryngeal formations do not affect the quality of life, only changing the voice. Larger lesions can cause difficulty swallowing and even breathing.
Esophageal tumors
Benign tumors of the esophagus occur in 5-7% of cases of all cancers of the digestive tract. These pathologies equally often affect men and women. Mostly patients over 35 years of age suffer. Depending on the histological structure, neoplasms can be very different.
The most common are adenomas, papillomas, and esophageal polyps. Less common are myxomas, rhabdomyomas, leiomyomas, and hemangiomas.
Benign tumors of the esophagus are extremely rare, including:
- Polyps are growths on the mucous membrane,
- Adenoma is a tumor of the mucous glands,
- Leiomyoma is a tumor of muscle tissue,
- Lipoma growing from adipose tissue
- Cysts are hollow formations in the epithelial layer.
Benign tumors of the esophagus have a slow growth rate. This causes the absence of clinical symptoms in the early stages of the disease. The patient may not even suspect the presence of a tumor for years and lead a normal life.
Treatment
Treatment of laryngeal and pharynx formations is most often performed surgically. Drug therapy is used only in cases of small sizes and quite often turns out to be ineffective. It consists of influencing the formation of certain drugs (glucocorticosteroids, alkaline oil solutions) by inhalation or direct application to the surface of the larynx. In most cases, treatment of benign formations of the hypopharynx cannot be done without surgical intervention.
Methods of surgical treatment of tumors of the larynx and pharynx are divided into two groups:
- Removal of formations using a “cold” micro-tool: biting, excision and cutting off. If the mass is a fluid-filled cyst, treatment may involve needling. This technique is minimally invasive. In this case, manipulations are performed under local anesthesia. The disadvantage of this treatment is the impossibility of precise visual control during manipulation, which increases the risk of capturing healthy tissue or, conversely, incomplete removal of the formation, as well as possible damage to the vocal cords with irreversible changes in the voice.
- Removal of tumors of the larynx and pharynx using laser and electrode coagulation, cryodestruction and ultrasound. Most often, such operations are performed endoscopically - with access through the oral cavity - however, if the tumor is large or its deep location, laryngofissure, a full-scale surgical operation with open access, is indicated. For the most precise surgical instrumentation, a special microscope can be used. This type of surgery is performed under general anesthesia.
How does swallowing occur?
Swallowing is a reflex act, as a result of which a bolus of food is pushed from the mouth into the pharynx and then moves into the esophagus. Swallowing begins with food irritating the receptors in the oral cavity and the back wall of the pharynx. The signal from the receptors enters the swallowing center located in the medulla oblongata (brain section). Commands from the center are sent through the corresponding nerves to the muscles involved in swallowing. The bolus of food, formed by the movements of the cheeks and tongue, is pressed against the palate and pushed towards the pharynx. This part of the act of swallowing is voluntary, that is, it can be suspended at the request of the swallower. When a bolus of food reaches the level of the pharynx (at the root of the tongue), swallowing movements become involuntary.
Swallowing involves the muscles of the tongue, soft palate and pharynx. The tongue moves the food bolus, while the velum palatine rises and approaches the back wall of the pharynx. As a result, the nasal part of the pharynx (respiratory) is completely separated from the rest of the pharynx by means of the velum palatine. At the same time, the neck muscles lift the larynx (this is noticeable by the movements of the protrusion of the larynx - the so-called Adam's apple), and the root of the tongue presses on the epiglottis, which descends and closes the entrance to the larynx. Thus, when swallowing, the airways are closed. Next, the muscles of the pharynx itself contract, causing the bolus of food to move into the esophagus.
Symptoms
Signs of the disease appear even with large benign tumors, when they directly begin to interfere with digestion or put pressure on neighboring organs. The most common symptoms of the pathology are:
- Difficulty swallowing (dysphagia). The tumor mechanically prevents food from passing through the esophagus. The patient must wash down food with water; it is difficult for him to eat meat, bread and solid foods.
- Mild or moderate chest pain in the projection of the esophagus. The discomfort is caused by compression of the nerve endings by the tumor.
- Belching, nausea, vomiting. These signs are a consequence of digestive disorders.
- Weight loss, general weakness. Caused by metabolic disorders due to the long-term existence of the tumor.