Home | About us | Delivery | Advertisers | Login | Registration
The pharmacy is closed on Sundays and holidays.
- Medicines
- dietary supplementsVitamins
- Categories from A to Z
- Brands from A to Z
- Products from A to Z
- Medical equipment
- beauty
- Child
- Care
- Honey products appointments
- Herbs and herbal teas
- Medical nutrition
- Journey
- Making medicinesStock
Pharmacy online is the best pharmacy in Almaty, delivering medicines to Almaty. An online pharmacy or online pharmacy provides the following types of services: delivery of medicines, medicines to your home. Online pharmacy Almaty or online pharmacy Almaty delivers medicines to your home, as well as home delivery of medicines in Almaty.
my basket
Apteka84.kz is an online pharmacy that offers its customers medicines, medicinal and decorative cosmetics, dietary supplements, vitamins, baby food, intimate products for adults, medical equipment and thousands of other medical and cosmetic products at low prices. All data presented on the Apteka84.kz website is for informational purposes only and is not a substitute for professional medical care. Apteka84.kz strongly recommends that you carefully read the instructions for use contained in each package of medicines and other products. If you currently have any symptoms of the disease, you should seek help from a doctor. You should always tell your doctor or pharmacist about all the medicines you take. If you feel you need further help, please consult your local pharmacist or contact our GP online or by telephone.
© 2021 Pharmacy 84.
Dangers of using sleeping pills for sleep disorders. Poluektov M.G.
Oksana Mikhailovna Drapkina , professor, doctor of medical sciences:
- We continue. We are transported to an area that is not very well known to us, it seems to me, but very interesting: neurology. Poluektov Mikhail Guryevich will talk about the dangers of using sleeping pills for sleep disorders.
Mikhail Guryevich Poluektov , associate professor, candidate of medical sciences:
– Good afternoon, dear colleagues. Today we will talk about one of the biggest problems in Russian somnology - the problem of abuse of sleeping pills. What does this entail?
At one time, at an international conference, we presented data where we tried to analyze the frequency of requests for specialized help in somnology centers, in centers where sleep disorders are dealt with, by patients with different diagnoses. And it turned out that in first place, more than half of the requests were related to the so-called secondary insomnia - secondary insomnia. And more than half of the cases of secondary insomnia, secondary insomnia, were associated with a form of insomnia such as dependence on sleeping pills.
I want to remind you again about insomnia. What is this anyway? How to diagnose it? Insomnia, or insomnia, is not a disease, it is a clinical syndrome. He has three main points for diagnosis. Firstly, these are any sleep disorders. That is, if a person has trouble falling asleep, if he wakes up often, if he wakes up early in the morning and then cannot fall asleep - all this is insomnia. Any complaints of sleep disturbances are actually insomnia. These disorders occur when a person has enough time to sleep. This is the second starting point for diagnosing this syndrome. And the third point is that the consequences of such sleep disturbance are disruption of daytime functioning. These can be a variety of disorders: drowsiness, irritability, a feeling of fatigue, difficulty concentrating, even gastroenterological complaints. That is, the range of daytime consequences of insomnia is quite wide. It is very important that insomnia is not just one disease. There are 9 types of insomnia, for some of which sleeping pills are strictly contraindicated.
Not long ago, we published a study that was conducted in Chuvashia at the department of Andrei Vasilyevich Golenkov, at the psychiatry department, where the frequency of sleep disorders was analyzed in a sample of the population of the Russian Federation. And it turned out that about 20% of respondents in the general population are dissatisfied with their sleep. They answered affirmatively when asked whether they had sleep disturbances often or constantly. But what bothered us most about the results of this study was that 4.5% of all respondents - not those who were dissatisfied with their sleep, but all respondents in general - took sleeping pills constantly or almost constantly. If, for example, we compare this with data from foreign studies, then only 0.2% of the general population takes sleeping pills, for example, in Western Europe or the United States of America. That is, the frequency of use of sleeping pills in the Russian Federation is several tens of times higher.
And most often, the use of sleeping pills is associated with so-called secondary insomnia, secondary insomnia. There are primary forms of insomnia, which I will talk about a little later, and there are secondary forms. Usually no one really tries to look for the cause of insomnia. If there is any diagnosis of the underlying disease, a diagnosis of insomnia is also added to it. There, “Dyscirculatory encephalopathy. Insomnia”, “Gastroesophageal reflux disease. Insomnia." In reality, everything is not so simple, of course. We can talk about the presence of a cause-and-effect relationship with the underlying disease if sleep disturbance begins after the onset of the underlying disease or simultaneously with it and if periods of change in the clinical picture of the underlying disease are also accompanied by a change in the severity of sleep disturbance. Then we have no doubt that this insomnia is secondary. For example, in case of pain syndromes, when the back hurts or the joint hurts, then, of course, do not go to sleep until the appropriate medications are taken. When the exacerbation subsides, sleep is restored. This is a very typical example of typical secondary insomnia.
Insomnia in mental disorders is also a very common form of secondary insomnia, accompanies almost any mental disorder: anxiety disorders, depressive disorders, panic disorders, and sleep disorders are very common in schizophrenia. That is, this is a very characteristic symptom of mental illness.
Another form of secondary insomnia is insomnia due to diseases of the internal organs and nervous system. I have already touched on this topic a little. In patients with cerebral strokes, for example, sleep disturbances are very common - 57% of the hospital population of such patients have sleep disturbances.
In general, the probability of detecting insomnia in various forms of pathology not associated with a mental disorder is very high. That is, insomnia occurs in a variety of diseases: heart disease, arterial hypertension, arrhythmias, and various respiratory problems. But most often, insomnia disorders and sleep disorders occur in diseases of the nervous system. In this table we see that sleep disorders occur 6 times more often in patients with neurological diseases than in a comparable control group without such diseases. This is much more common than, for example, in people with diabetes, genitourinary problems, and so on. That is, neurological diseases lead after mental disorders in the frequency of occurrence of insomnia (insomnia).
And a very big problem with secondary insomnia is insomnia associated with taking medications or other substances. This is where I began the story that more than half of the patients who turn to specialized centers for help have precisely this diagnosis - insomnia associated with drug dependence, or insomnia associated with taking medications. Most often, this is insomnia associated with taking benzodiazepine sleeping pills. You know that in the Russian Federation certain benzodiazepine sleeping pills are extremely common and are used completely uncontrolled. There may be barbituric dependence - very popular drugs contain phenobarbital. If you roughly recalculate, then, for example, 100 drops of Valocordin is approximately one tablet of Phenobarbital. Phenobarbital is a first-generation sleeping pill that has many unwanted side effects. Alcohol: also drinking alcohol, alcohol abuse is accompanied by the development of a specific form of insomnia associated specifically with alcohol dependence. With “recreational substances” - we mean energy tonics, some substances associated with spending time at night - we still don’t come across that often in our practice, and this is not such a pronounced problem, at least in those centers in whom we work.
We said that there are forms of secondary insomnia that are associated with certain diseases, and there are forms of primary insomnia. And the most common medical error is the use of sleeping pills in some forms of primary insomnia. There is only one form of primary insomnia for which sleeping pills should be taken. And it has indeed been proven that if sleeping pills are prescribed in time for, for example, a form of insomnia called “adaptive insomnia”, or “acute insomnia”, or “reaction to stress”, then the person gets out of this stressful state faster and recovers faster. This is, in fact, the most common everyday insomnia. Over the course of a year, 1/5 of the population experiences this form of insomnia because stress happens all the time. But most often, this insomnia resolves spontaneously without the need to resort to any sleeping pills. But if it drags on, if it lasts for more than three months after the stress factor ends, then, most likely, we will be talking about another form of sleep disorder, which I will talk about a little later. This is the only form of primary insomnia that is not associated with any disease, in which the prescription of a sleeping pill is indicated and helps to quickly get out of this stressful state.
What drugs are used most often? The most commonly used ligands are the GABA-A receptor complex. This is how it looks beautiful in an electronic photograph. It is also called the Costa complex. This is an ion channel that is surrounded by five protein subunits, a molecule of gamma-aminobutyric acid attaches to certain sites, and benzodiazepines attach to certain sites. Benzodiazepines increase the affinity of this receptor for GABA - GABA begins to act more strongly and causes a stronger inhibitory effect. And the hypnotic effect of the drug, or sedative, or anxiolytic, or muscle relaxant, depends on which type of one of the five subunits the hypnotic drug is attached to.
Benzodiazepine drugs are non-selective. If we use hypnotics as benzodiazepines, they attach to the alpha-1 subunits of this complex, and to the alpha-2, to the alpha-3, 5, and accordingly they produce a whole range of effects, both desirable ones, such as a sedative and hypnotic effect, and undesirable if we use them as sleeping pills - amnestic, muscle relaxant effect. The anxiolytic effect is rather desirable.
More modern sleeping pills have a different structure - not benzodiazepine. These are Zaleplon, Zopiclone, Zolpidem - the so-called Z-drugs. They have a high affinity specifically for the alpha-1 subunit and almost do not bind to other subunits. They are considered to have less potential for unwanted side effects than their predecessor benzodiazepine hypnotics.
What problems most often arise when using benzodiazepine-type sleeping pills? This is tolerance (addiction), that is, gradually it is necessary to use a larger and larger dose of the drug to get the same effect. Dependence, withdrawal syndrome - the criterion for addiction specifically includes the development of withdrawal syndrome: when we stop a drug, sleep disturbances sharply increase, a whole range of side effects arise, primarily of a vegetative nature, and psychomotor agitation occurs. These are very undesirable effects that are really very poorly tolerated by patients.
Worsening sleep apnea – I’ll talk about this a little further. Decreased memory, attention, reaction time - so-called cognitive toxicity. This is due to the fact that many benzodiazepine drugs that are used as sleeping pills have a very long half-life and continue to act both in the morning and during the day because they have not yet left the body in sufficient quantities. For actively working people, this can really become a problem, or, for example, when driving a car.
So-called behavioral toxicity is a problem for older people, of course, primarily. Again, in the morning, when an elderly person gets up, and the effect of the sleeping pill has not yet worn off, this can lead to unwanted falls, which can be fraught with complications for older people.
Daytime drowsiness – also due to the long half-life, the beneficial effect of the sleeping pill becomes harmful.
Another approach to the use of these sleeping pills is not to increase GABAergic transmission, when we increase the inhibitory effect on the brain, putting it to sleep, but to inhibit the activating brain systems. It is one of the most important activating brain systems containing histamine and has arousal properties that promote wakefulness. If you block the receptors in this system, then the balance between the activating and inhibitory brain systems will be disrupted: the person will fall asleep. This is the ideology of using central histamine receptor blockers.
For this, the drug Doxylamine is used, for example. This is a blocker of the H1 subtype, as I already said, of histamine receptors. It has a sedative and hypnotic effect. The half-life of the drug is 10 hours. Not as small, but significantly smaller than many commonly prescribed benzodiazepine sleeping pills. It is usually prescribed for a short period of time in acute forms of insomnia. Prescribed according to regular prescriptions. It can be used in pregnant women throughout the entire period of pregnancy - this is written in the new instructions for the drug.
There are certain restrictions on the use of this drug. It is not used in children, but should be used with caution if sleep apnea is suspected. Again, we need to talk about apnea further. With caution - for patients over 65 years of age due to possible dizziness and delayed reactions with the risk of falling. And due to the fact that it has an anticholinergic effect, it is contraindicated in patients with closed-angle glaucoma and prostate adenoma. That is, this sleeping pill has restrictions on its use.
What to do with a patient who 10 years ago came to the doctor, asked him for a sleeping pill, was prescribed it (most likely, it was a benzodiazepine sleeping pill), and now 10 years later he comes and says: “Doctor, they are no longer helping me.” two or three tablets of this drug. Give me something else"? This is a really big problem, you need to work a lot with this patient, and here is an algorithm for working with such patients. First, it is necessary to reduce the dose of the drug. Do not immediately remove the drug, but gradually reduce it in order to avoid the sudden onset of withdrawal symptoms. Unfortunately, in the Russian Federation there are no sedative-hypnotic drugs that would be dosed in drops, when it would be possible, for example, to gradually reduce the same Diazepam by one drop per night. But we recommend that patients somehow divide these tablets into several parts.
Then, if we manage to minimize the dose of the drug, go from, for example, three tablets to two, to one tablet, we transfer the patient to a non-hypnotic drug, which has side sedative and hypnotic effects. Most often these are antidepressants with sedative effects: Mianserin, Trazodone.
In the future, if we manage to get away from a typical sleeping pill, addiction does not develop to antidepressants, then in the future it is possible to get away from antidepressants: reduce the dose of the drug, switch to lighter over-the-counter medications.
If this does not help, if the patient cannot tolerate the period of dose reduction, the withdrawal period, we probably have the only remedy - the so-called drug holidays. Some patients can live and sleep relatively tolerably for years according to this scheme: 1 plus 1, 3 plus 1. What is the essence of this scheme? For three weeks, for example, the patient takes a sleeping pill, for three weeks he does not take a sleeping pill, but takes anything: sedative herbs, but most often these are over-the-counter medications. This is necessary in order to restore sensitivity to the original drug. And the patient himself already knows that he will indeed sleep very poorly for three weeks, he will suffer, but he will still sleep, because sleep is a basic need of the body. But for the next three weeks he will sleep wonderfully, and during these three weeks he will not develop an addiction. At the same time, it is important to support him: we prescribe behavioral therapy, limit the time he spends in bed, limit daytime sleep, for example, teach him how to follow the rules of sleep hygiene, and there are so-called “supporting” visits, when the doctor and the patient simply talk, “Is everything being followed? "
I said that another problem with the use of many sleeping pills is the risk of worsening a condition called obstructive sleep apnea, or Pickwickian syndrome. Here is a classic picture of this fat guy Joe, who served a certain gentleman and kept getting into strange situations where he fell asleep while eating, fell asleep while ringing the bell, and fell asleep all the time. Therefore, since it was Charles Dickens's first novel, The Pickwick Papers, the syndrome was long called Pickwickian Syndrome.
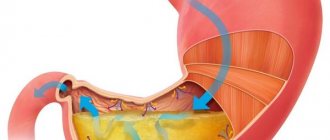
And then it turned out that this condition is due to the fact that during sleep such people, most often with morbid obesity, experience a huge number of breath holds, and because of this they are almost unable to fall into deep sleep. For years they do not get deep sleep, and therefore have constant daytime sleepiness. This is most often associated with morbid obesity. Here we see how different the lumen of the upper respiratory tract is in such patients, and when they fall asleep, this lumen becomes even smaller.
One of the main pathogenetic mechanisms for the development of complications in this condition is fluctuations in blood pressure associated with changes in the level of blood oxygen saturation and sympathetic hyperactivation.
At the same time, if sleeping pills are taken, then a very unpleasant phenomenon is observed when there is a discoordination of muscle contractions of those muscles that maintain the lumen of the upper respiratory tract, which prevent them from closing during inhalation, and the diaphragm.
In the upper graph we see that during the respiratory cycle there is a synchronous activation of these muscles, and when using, for example, alcohol, the activation of the hypoglossal muscle, which is responsible for ensuring the lumen of the airways, is significantly reduced. And a situation arises that the muscles of the upper respiratory tract do not have time to prepare for the negative air pressure that enters the respiratory tract during inhalation, and obstruction may occur. Most often it occurs in people with an existing diagnosis of sleep apnea. Therefore, the vast majority of sleeping pills are contraindicated in patients with sleep apnea. Benzodiazepine drugs have contraindications in their instructions. Even the most modern Z-drugs have restrictions on their use, including Doxylamine: the instructions also say that they should be used with caution in cases of this type of violation.
What should you do if you have sleep apnea? For sleep apnea, the treatment of choice is a device called a CPAP machine. Through a mask, which is placed on the patient’s face before going to bed, air is supplied, which constantly keeps the airways open and prevents them from collapsing. It is the treatment of choice for moderate to severe sleep apnea.
So, when should you prescribe sleeping pills to avoid these unwanted effects? Sleeping pills are prescribed for acute insomnia, for acute insomnia (under stress, for example, during an exacerbation of the underlying disease), but for chronic insomnia, non-drug treatment methods take priority: normalization of sleep hygiene and behavioral methods. Sleeping pills are not used.
Currently, sleeping pills that can be used in long courses are not registered in the Russian Federation. They are known: Eszopiclone, extended-release Zolpidem and Ramelteon, but they have not yet reached us. Thank you for your attention.