Share with friends
Stopping medications should only be done under the guidance of your doctor. This is usually done gradually, reducing the dosage every few days. But in the case of phase inversion, when you switch from depression to hypomania or mania, withdrawal may occur more quickly.
If you're considering switching antidepressants or stopping taking them altogether, it's worth knowing how your body might respond to chemical changes in your body, and even more important to know how you can ease withdrawal symptoms.
Best possible situation: you don't even need to read this article because there is no syndrome (yay!).
Another possibility is that you are experiencing withdrawal reactions, but you are prepared for them and know that they are temporary.
What to expect after stopping antidepressants
Many symptoms are associated with depression or anxiety, so it's worth keeping an eye on how you feel and how long it lasts. Withdrawal syndrome often manifests itself as:
- Panic attacks
- Poor motor coordination
- Strong emotionality
- Dizziness or inability to concentrate
- Insomnia and/or nightmares
- Fever
- Strange twitching and “bumps”
- Loss of appetite
- Nausea
This doesn't sound very nice. Withdrawal syndrome is not a pleasant thing. But if you're experiencing any of the above, remember: it won't last forever. Everything will be alright. We have a list of tips to help you feel better during this difficult time.
How to properly stop the drug
It is advisable to stop taking all antidepressants gradually. A stepwise reduction in dosage allows time for the brain neurons to adapt to the new concentration of substances. With the correct dosage reduction, drug withdrawal goes smoothly and without consequences.
A drug withdrawal regimen must be prescribed by the attending physician. It can have two development paths. The first is a complete refusal of antidepressants, the second is replacing the drug with another. In the first case, the dosage of amitriptyline is reduced by approximately 25 mg per month. If the patient does not tolerate such a reduction, by 10 mg once every two weeks. On average, complete cessation of use can be achieved after about 6 months.
In the second case, the dosage of the drug is reduced more quickly, but under the guise of another antidepressant. Thus, the dosage of one substance is gradually reduced, and the second is increased.
Sometimes patients complain of anxiety, panic attacks and other symptoms of the disease when the drug is discontinued. As a rule, this is not associated with withdrawal symptoms and is psychogenic in nature. The patient is afraid of being in the same state that led him to take amitriptyline, so he begins to notice familiar symptoms. Such people need a course of psychotherapy in order to teach them how to live without drug support.
Do not stop taking antidepressants unless directed by a psychiatrist
It's easy to make a decision like, “I don't want to burden the doctor,” and start changing or stopping medications on your own. But please do not change anything without your doctor's instructions, even if it is a small reduction in the dosage of your medication. Antidepressants are useful but are potent substances, so it is important to consult a professional about any minor changes.
When you visit your psychiatrist, ask how best to change your treatment. Your doctor can usually make a plan to reduce your dosage instead of stopping suddenly. If you start a new medicine, it will likely be introduced gradually while reducing the level of your current medicine. This will help alleviate withdrawal symptoms.
Prepare for panic attacks
You may feel panicked while coming off antidepressants, either occasionally or constantly. If you have already experienced panic attacks, use the techniques that already suit you. If you haven't encountered them, place a paper bag next to your bed so you can breathe into it during attacks. Practice deep breathing and counting objects in the room until your heartbeat calms down.
Have a cry
Tears go hand in hand with panic attacks. In some cases you may be very tearful. Our advice is to cry if you want to. It's nothing to be ashamed of, and honestly, tears can make you feel quite refreshed. Do not be afraid.
AMITRYPTYLINE ZENTIVA
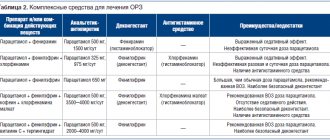
Interaction
Combined use with serotonergic active substances (such as SSRIs, SSRIs, MAO inhibitors, lithium preparations, triptans, tramadol, linezolid, L-tryptophan, St. John's wort preparations) may cause the development of serotonin syndrome.
Monoamine oxidase inhibitors
Concomitant use of amitriptyline and MAO inhibitors can cause serotonin syndrome (agitation, confusion, tremor, myoclonus, hyperthermia are possible). Amitriptyline can be prescribed 14 days after stopping treatment with irreversible MAO inhibitors and at least 1 day after stopping therapy with the reversible MAO type A inhibitor, moclobemide.
MAO inhibitors can be prescribed 14 days after stopping amitriptyline.
Selective serotonin reuptake inhibitors
Caution must be exercised when co-using amitriptyline with selective serotonin reuptake inhibitors (fluoxetine, fluvoxamine). Their simultaneous administration leads to an increase in the concentration of amitriptyline in the blood plasma due to inhibition of the CYP2D6 isoenzyme involved in the metabolism of TCAs. Patients receiving such therapy should be under strict medical supervision due to the risk of toxic reactions.
Anticholinergic drugs
Because TCAs, including amitriptyline, may potentiate the effects of anticholinergics on the eye, central nervous system, bowel, and bladder, their concomitant use should be avoided due to the risk of paralytic ileus.
When taking TCAs in combination with anticholinergics or antipsychotics, especially in hot weather, hyperpyrexia may develop.
Sympathomimetics
Amitriptyline may enhance the effects of adrenaline, norepinephrine, ephedrine, isoprenaline, phenylephrine and phenylpropanolamine on the cardiovascular system. As a result, anesthetics, decongestants and other drugs containing these substances should not be used simultaneously with amitriptyline.
Drugs that reduce sympathetic activity
Amitriptyline may reduce the hypotensive effect of guanethidine, betanidine, reserpine, clonidine and methyldopa. When taking TCAs concomitantly, it is necessary to adjust antihypertensive therapy.
CNS depressants
When used simultaneously with Hi-histamine receptor blockers, clonidine, alcohol and barbiturates, the inhibitory effect on the central nervous system may be enhanced. Amitriptyline may enhance the effects of other drugs that depress the central nervous system.
Drugs that prolong
the QT
interval The simultaneous use of amitriptyline and drugs that prolong the QT interval - antiarrhythmics (quinidine), antihistamines (astemizole and terfenadine), some antipsychotics (especially pimozide and sertindole), cisapride, halofantrine and sotalol - increases the risk of developing ventricular arrhythmia.
Antifungal drugs
Antifungal drugs, for example, fluconazole, terbinafine, increase the serum concentration of tricyclic antidepressants and, accordingly, their toxicity. Fainting and the development of paroxysms of ventricular tachycardia ( torsade
de pointes ) are possible.
Barbiturates and inducers of microsomal liver enzymes
Barbiturates and other inducers of microsomal liver enzymes, such as rifampicin and carbamazepine, can increase the metabolism of TCAs, and as a result, reduce the concentration of TCAs in the blood plasma and reduce their effectiveness.
Cimetidine, methylphenidate and slow calcium channel blockers
When used simultaneously with cimetidine, methylphenidate and blockers of “slow” calcium channels, it is possible to slow down the metabolism of amitriptyline, increase its concentration in the blood plasma and develop toxic effects.
Neuroleptics
When co-prescribed with antipsychotics, it should be taken into account that TCAs and antipsychotics mutually inhibit each other's metabolism, lowering the threshold for convulsive readiness.
Indirect anticoagulants
With the simultaneous use of amitriptyline and indirect anticoagulants (coumarin or indadione derivatives), the anticoagulant activity of the latter may increase.
Glucocorticosteroid drugs
Amitriptyline may enhance depression caused by glucocorticosteroids (GCS).
Anticonvulsants
When used together with anticonvulsants, it is possible to enhance the inhibitory effect on the central nervous system, reduce the threshold of convulsive activity (when used in high doses) and reduce the effectiveness of the latter.
Antithyroid drugs
Due to the risk of arrhythmias, special caution must be exercised when prescribing amitriptyline to patients with hyperthyroidism or patients receiving antithyroid drugs.
Concomitant use with drugs for the treatment of thyrotoxicosis increases the risk of developing agranulocytosis.
Anticholinergics, phenothiazines and benzodiazepines
When used together with anticholinergic blockers, phenothiazines and benzodiazepines, a mutual enhancement of the sedative and central anticholinergic effects and the risk of epileptic seizures is possible (lowering the threshold of convulsive activity)
Oral contraceptives
Estrogen-containing oral contraceptives and estrogens may increase the bioavailability of amitriptyline. A dose reduction of either estrogen or amitriptyline may be necessary to restore efficacy or reduce toxicity. However, discontinuation of the drug may be necessary.
Acetaldehyde dehydrogenase inhibitors
Concomitant use with disulfiram and other acetaldehyde dehydrogenase inhibitors may increase the risk of developing psychotic conditions and confusion.
Phenytoin
TCAs may increase serum concentrations of phenytoin and, accordingly, increase the risk of its toxic effects (ataxia, hyperreflexia, nystagmus, tremor).
St. John's wort
The simultaneous use of amitriptyline and drugs containing St. John's wort can lead to increased metabolism of amitriptyline and a decrease in the maximum serum concentration of amitriptyline by 20 %,
due to the induction of its metabolism by the liver isoenzyme CYP3A4. Theoretically, it is possible to increase the risk of serotonin syndrome.
Lithium
With the simultaneous use of lithium drugs and TCAs, the risk of psychotic symptoms and toxic complications from the central nervous system may increase, even against the background of therapeutic concentrations of lithium in the blood plasma. Cases of mania, myoclonus, tremor, tonic-clonic seizures, memory disorders, confusion, disorganization of thinking, hallucinations, serotonin syndrome and neuroleptic malignant syndrome, which began a few days after the start of combination therapy, have been described; in most cases, discontinuation of therapy with either TCAs or lithium preparations was required. Elderly patients are especially prone to such reactions.
Make time for withdrawal symptoms
Especially if you're stopping treatment completely, take a week or two off of difficult tasks to deal with it. Even a couple of days off can help. Give yourself time to adjust.
Of course, not everyone can take time off at any time, but you can start clearing out your medications before the weekend, or at least clearing out your schedule. If you feel very sick from withdrawal, stay in bed as long as you can. Long sleep will help you recover.
Don't forget to go to the store before you start taking off your medications. If you're feeling dizzy and panicky, you may have a hard time leaving the house until it passes.
Treatment of fever, nausea and diarrhea
If you feel unwell, you can take regular medications to relieve the symptoms.
For example:
- Anti-motion sickness tablets for dizziness
- Paracetamol in case of fever and/or headache
- Dioralyte for vomiting
If you don't want to drink all those bags, drink plenty of fluids)