The symptom complex of vegetative-vascular dystonia includes many manifestations that affect the functioning of almost all organs. Extrasystole with VSD is a very common symptom and accompanies almost every VSD patient. It is exclusively neurological in nature and in most cases does not threaten the patient’s life, but it brings a lot of inconvenience and leads to an exacerbation of the disease.
Causes
NVEs develop due to many reasons.
Even a simple sneeze or fear can cause extraordinary contraction of the myocardium. The most common culprits of extrasystoles are various heart diseases: coronary disease, cardiomyopathy, congenital and acquired defects, myocarditis, pericarditis, chronic heart failure, etc. Also, supraventricular extrasystole develops with the following factors, conditions and diseases:
- violation of autonomic regulation (autonomous dysfunction syndrome);
- physical and emotional stress;
- neurotic disorders;
- reflex irritation of the cardiac nerves in diseases of the gastrointestinal tract: duodenal ulcer, cholelithiasis;
- presence of bad habits;
- coffee addiction;
- taking pills: antidepressants, psychostimulants to reduce appetite, vasoconstrictor nasal drops, medications for high blood pressure. Even some antiarrhythmic drugs in some cases cause EVE;
- infectious diseases;
- severe diseases of the respiratory system: bronchial asthma, chronic broncho-obstructive pulmonary disease;
- pathology of endocrine organs: Graves' disease, Hashimoto's thyroiditis, diabetes mellitus;
- excess or deficiency of minerals in the body (calcium, magnesium, sodium);
- chest injuries.
In some cases, the cause of the rhythm disturbance cannot be identified. Then a diagnosis of “NVE of unknown etiology” is made.
Classification and types
There are many types of NLEs, divided according to different characteristics.
Depending on the source of the impulse, atrial extrasystoles and extrasystoles (ES) from the atrioventricular (AV) connection are distinguished. Based on the number, they distinguish between single and double. Three or more ES in a row is already considered an episode of tachycardia (also called a “jog”).
In my patients, I often observe such an ECG phenomenon as allorhythmia - the regular occurrence of extrasystoles. There are the following types:
- bigeminy - the appearance of ES on the cardiogram after each normal contraction of the heart (read more about this phenomenon here)
- trigeminy - after every second complex;
- quadrigeminy - after every third complex.
Depending on the cause, the following types of NVEs are distinguished:
- functional - during physical activity, reflex effects;
- organic - for heart diseases;
- toxic - in case of drug overdose;
- mechanical - for injuries.
Single extrasystoles
The most benign variant of NVE, mainly found in healthy individuals, are single supraventricular extrasystoles. They almost always go unnoticed by humans and do not pose a threat to health.
Diagnosis and treatment of extrasystoles
Extrasystoles can be detected on an electrocardiogram, as well as during daily Holter monitoring. Rare extrasystoles do not require treatment if, after examining the patient, no heart disease is detected. If the examination reveals that the extrasystoles are associated with some other disease (diseases of the gastrointestinal tract, endocrine diseases, inflammatory diseases of the heart muscle), the underlying disease is treated.
The doctor should explain what the patient should avoid and what non-drug methods can alleviate the condition and relieve extrasystoles. It is very important that extrasystole caused by disorders of the nervous system and psycho-emotional overload is treated by prescribing sedatives or sedatives. In our age of stress, a properly selected sedative often completely relieves the patient of extrasystoles.
The prescription of antiarrhythmic drugs occurs with mandatory consideration of the types of extrasystoles and heart rate. The selection of antiarrhythmic drugs is made strictly individually and only by a doctor. Remember! All antiarrhythmic drugs have a proarrhythmic effect, that is, they themselves can cause or intensify arrhythmia.
Our doctors select medications based on the latest Russian and international recommendations. Moreover, they have the opportunity to select a drug under ECG control, and the patient does not have to constantly be in the cardiac center. For this we use a remote ECG analysis system. In addition, treatment is monitored using Holter monitoring on average once a month.
If the effect of the drug is good, extrasystoles disappear or are significantly reduced. As a rule, medications need to be taken continuously. In some cases, it is possible to discontinue the medication. But at the same time, the dose of the medication is gradually reduced over a long period of time, since abrupt discontinuation of treatment leads to the recurrence of extrasystoles.
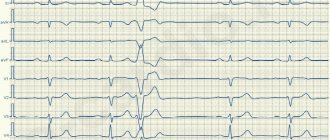
Signs on ECG
Supraventricular extrasystole is very easy to recognize on a cardiogram. Main features:
- extraordinary (extrasystolic) appearance of a pathological deformed P wave and the following unchanged QRST complex;
- the presence of a compensatory pause, i.e. a straight line on the film.
If the P wave has a different shape in different leads, this phenomenon is called polytopic atrial extrasystole. Its detection is highly likely to indicate a heart or lung disease and requires a more thorough diagnosis.
It happens that after an extraordinary P wave there is no QRST complex. This happens when atrial extrasystole is blocked. ES from the atrioventricular junction differs in that the P wave is negative or not recorded at all due to overlap with the T wave.
When taking an ECG at rest, extrasystoles may not be detected. Therefore, in order to “catch” them and find out how often they occur, I prescribe Holter monitoring to my patients. In case of concomitant diseases, a person undergoes a cardiac ultrasound (EchoCG).
After supraventricular ES, the pause lasts less than with ventricular ES.
Why do extrasystoles occur during VSD?
Cardiac “dancing” in vegetative-vascular dystonia can occur when both parts of the autonomic nervous system are disrupted.
If the sympathetic department fails, extrasystoles appear after physical exertion. They are poorly controlled by sedatives, and may even intensify after taking them.
If the functioning of the parasympathetic system is disrupted, in addition to cardiac symptoms, digestive disorders are of concern: epigastric pain, diarrhea, bloating. A cup of coffee or sweet tea or a brisk walk will help relieve such an attack.
If the cause is psychological, treatment measures are directed in the other direction.
Most often, dystonics are bothered by two types of extrasystole:
- Ventricular. Usually makes itself felt in the first half of the day. It is caused by disturbances in mental balance, for example, great joy or grief. It also appears when the weather changes or when drinking strong drinks. Other provoking factors include magnesium and calcium deficiency, osteochondrosis. It all starts with an intense beat in the heart area, followed by a pause. The patient becomes covered in cold, sticky sweat and develops a feeling of fear. Despair sets in, he cannot choose a comfortable position for himself, becomes numb or begins to fuss. The violence of his heart leads him into an uncontrollable state, causing him a lot of suffering.
- Supraventricular. The most common type of arrhythmia in VSD. The causes of this condition coincide with those of the ventricular form. In addition, dystonics who are addicted to antiarrhythmic and diuretic drugs are at risk. Patients claim that the condition worsens when lying down. It is this sign that indicates that the cardiac failure is functional in nature.
Treatment: when, how and with what
Supraventricular extrasystoles are almost always benign. If extraordinary contractions of the heart are single, are not accompanied by any symptoms and do not provoke the occurrence of severe rhythm disturbances, treatment of supraventricular extrasystole is not required. The main thing is to fight its cause.
When EVE worsens the patient's condition, I prescribe drug therapy. The most effective drugs for stopping SE are beta-blockers - Bisoprolol, Metoprolol. If there are contraindications to their use (for example, severe bronchial asthma), I transfer the patient to slow calcium channel blockers - Verapamil, Diltiazem. Read about how extrasystole is treated with medications here.
As for traditional methods, to date there is no convincing evidence of their effectiveness. In my practice, I recommend that patients under no circumstances replace traditional treatment with traditional medicine. But if you have a different opinion, we invite you to read the material here.
If the development of NVE is associated with emotional stress or a neurotic disorder, you can take sedatives and make an appointment with a psychotherapist.
The main criteria for the success of therapy are the cessation of symptoms and normalization of the patient’s condition.
In rare cases, when drug treatment does not have the expected positive effect, surgical intervention is used, in particular, a technique such as radiofrequency catheter ablation. I usually prescribe this operation to young patients, since with age the risk of developing severe complications, including death, increases.
It is extremely rare, for health reasons, that an open access operation is performed, with dissection of the chest and removal of the portion of the myocardium where extraordinary impulses are formed.
Why are supraventricular extrasystoles dangerous and what are their consequences?
Extraordinary supraventricular extrasystoles themselves do not pose a threat to human life and often go unnoticed. However, they can provoke the appearance of more severe rhythm disturbances: supraventricular tachycardia, atrial fibrillation and flutter, which lead to a sharp decrease in blood pressure, deterioration of blood supply to the myocardium and an increased risk of blood clots in the heart. A combination is often observed .
Long-term polytopic and blocked ES are considered the most unfavorable.
The consequences of supraventricular extrasystole are determined by the presence of: coronary heart disease, chronic heart failure, etc. The rhythm disturbance itself almost does not cause any complications.
Extrasystole and other signs of VSD
Considering that extrasystoles cause severe discomfort to dystonics and knock them out of their normal state, they become the cause of the development of other symptoms of VSD. These include:
- increased sweating;
- irritation;
- worry and anxiety;
- weakness and malaise;
- chills and feeling of heat.
Panic attacks that occur during heart dances become the basis for the formation of cardioneurosis. A dystonic person risks developing a phobia against the background of such interruptions in the heart.
Attacks of arrhythmia that occur at night disturb the sleep of the sufferer and provoke insomnia. It can also accompany him as a result of constant worry and anxiety.
Extrasystoles in neurocirculatory dystonia, despite their harmlessness, cause circulatory disorders, including cerebral circulation. As a result, the patient experiences attacks of suffocation, lack of air, and dizziness. Shortness of breath appears.
One of the complications provoked by extraordinary heart contractions during VSD is a panic attack. It begins with an attack of panic and fear, accompanied by a feeling of anxiety and tension. Other symptoms include tachycardia, internal trembling and sweating, nausea, suffocation and dizziness. Characterized by unpleasant sensations in the heart area, tingling and numbness of the arms and legs. The panicker is overcome by fear of death, consciousness is confused, and thinking is impaired.
Thus, arrhythmia, being a sign of VSD, provokes the development of other symptoms of the disease and aggravates its course.
Expert advice
Despite the fact that most often EVEs are relatively harmless, if they occur frequently and are accompanied by symptoms (feelings of freezing, interruptions in heart function, dizziness, feeling of lightheadedness), you should consult a doctor to find out the cause, including examination for cardiac problems. and other diseases. I try to explain to my patients that eliminating the causative factor is of no small importance in the treatment of EVE. Therefore, I give recommendations for lifestyle changes: you need to quit smoking, try to avoid severe stress, and significantly limit the consumption of alcohol and coffee. If a person develops signs of EVE while taking medications, be sure to tell the doctor about it. Reducing the dosage or changing the medication often helps get rid of extrasystoles.
What is characteristic of vegetative-vascular dystonia
It is important for a VSD patient to understand that his arrhythmia is of a functional nature. And no matter where exactly and in what quantity it occurs, one thing is clear: the heart is healthy, and the reason lies in something completely different.
Extrasystole in such patients manifests itself when a large amount of adrenaline enters the blood. But as soon as it decreases to normal, all sensations subside. That is, the problem is temporary and reversible. But patients tolerate it very hard. For them, this is like death: heart failures catch them suddenly, they can be repeated for several months and even years, until the cause is eliminated.
At this moment, a person is seized by a feeling of fear. He begins to choke, his legs give way, and he may lose consciousness. The patient becomes pale, begins to rush about, and scream. The sensation in the chest resembles a blow to the rib cage.
An even greater fear is the compensatory break after an extraordinary compression. The patient fears that his heart will stop. It seems to him that he will die, and this cannot be avoided.
If the excitement intensifies, then the symptoms worsen. Atrial fibrillation occurs. It seems that the heart works outside the regime, chaotically, as it pleases. Fortunately, this condition rarely occurs.
Clinical case
A 33-year-old man came to see me with complaints of rapid heartbeat, periodic sensations of “fading” and interruptions in heart function over the past 3 weeks. He does not take any medications on his own. Doesn't smoke, doesn't drink alcohol. A general examination revealed a high heart rate (105 beats per minute) and increased blood pressure - 140/80 mmHg. Art. During the conversation, I noticed the patient’s uncharacteristic irritability and bulging eyes. When questioning about the presence of diseases in relatives, the man noted that his father suffered from Graves' disease. Holter ECG monitoring was prescribed. Sinus tachycardia, atrial extrasystole of the bigeminy type, and a large number of single extraordinary contractions (967) were detected. A referral was issued to an endocrinologist to check the thyroid gland. On the recommendation of a specialist, an ultrasound examination was performed and blood was taken for hormonal tests. The results obtained: diffuse enlargement of the thyroid gland, decreased TSH levels, increased concentrations of free T4, high titers of antibodies to the TSH receptor. Diffuse toxic goiter was confirmed . Mercazolil therapy was prescribed with subsequent monitoring of hormone levels. To slow down the heartbeat and combat extrasystole, beta-blockers (Bisoprolol) are recommended.
Supraventricular extrasystole
Supraventricular extrasystole is one of the types of arrhythmia. In this case, an extraordinary excitation of any part of the heart occurs, caused by the occurrence of a premature impulse in the upper parts of the heart or in the antiventricular node.
The causes of supraventricular extrasystole are varied. Extrasystoles are functional and organic. Functional ones can occur in people with a healthy heart, in particular in children and tall young men. This is a rare single supraventricular extrasystole with the number of contractions less than 30 per hour.
Functional extrasystoles are usually classified as having the following origin: neurogenic; diselectrolyte; dishormonal; toxic; medicinal.
Neurogenic, in turn, are divided into hypoadrenergic, hyperadrenergic and vagal.
Hyperadergic extrasystoles are associated with increased physical and mental work, emotional arousal, drinking alcohol, smoking, and eating spicy foods.
Hypoadergic ones are difficult to recognize. Their existence is confirmed by experimental data and clinical observations.
With vagal extrasystole, interruptions in heart contraction occur after eating and during sleep, that is, in a horizontal position.
Organic supraventricular extrasystoles are caused by heart diseases, including:
- cardiac ischemia;
- heart defects;
- cardiomyopathy;
- myocarditis;
- tricuspid valve prolapse;
- mitral valve prolapse with blood returning to the left atrium;
- minor atrial septal defect;
- expansion of the pulmonary artery trunk;
- atrial dilatation in obesity, diabetes mellitus, chronic alcohol intoxication.
Sinus extrasystole is most often caused by chronic ischemic heart disease. We can talk about the organic nature of supraventricular extrasystole if it develops:
with sinus tachycardia; comes from several foci (polytopic); associated with angina pectoris; extrasystoles more than 30 per hour during ECG monitor recording and more than 5 per minute during examination by a doctor.
Supraventricular extrasystole is one of the types of arrhythmia. In this case, an extraordinary excitation of any part of the heart occurs, caused by the occurrence of a premature impulse in the upper parts of the heart or in the antiventricular node. Etiology and types of supraventricular extrasystoles
The causes of supraventricular extrasystole are varied. Extrasystoles are functional and organic. Functional ones can occur in people with a healthy heart, in particular in children and tall young men. This is a rare single supraventricular extrasystole with the number of contractions less than 30 per hour.
Extrasystoles of the following origin are usually classified as functional:
- neurogenic;
- diselectrolyte;
- dishormonal;
- toxic;
- medicinal.
Enlargement of the thyroid gland and its increased function can often be the cause of supraventricular extrasystole
Neurogenic, in turn, are divided into hypoadrenergic, hyperadrenergic and vagal.
Hyperadergic extrasystoles are associated with increased physical and mental work, emotional arousal, drinking alcohol, smoking, and eating spicy foods.
Hypoadergic ones are difficult to recognize. Their existence is confirmed by experimental data and clinical observations.
With vagal extrasystole, interruptions in heart contraction occur after eating and during sleep, that is, in a horizontal position.
Organic supraventricular extrasystoles are caused by heart diseases, including:
- cardiac ischemia;
- heart defects;
- cardiomyopathy;
- myocarditis;
- tricuspid valve prolapse;
- mitral valve prolapse with blood returning to the left atrium;
- minor atrial septal defect;
- expansion of the pulmonary artery trunk;
- atrial dilatation in obesity, diabetes mellitus, chronic alcohol intoxication.
Sinus extrasystole is most often caused by chronic ischemic heart disease. We can talk about the organic nature of supraventricular extrasystole if it develops:
- with sinus tachycardia;
- comes from several foci (polytopic);
- associated with angina pectoris;
- extrasystoles more than 30 per hour during ECG monitor recording and more than 5 per minute during examination by a doctor.
In addition, supraventricular extrasystole is classified as follows:
- According to the number of ectopic foci: monotopic (one foci), polytopic (several foci).
- By localization: atrial with the source of excitability in the atria and antiventricular - in the septum between the upper and lower parts of the heart.
- By frequency: paired (two extrasystoles in a row), single (less than 5 per minute), multiple (more than 5 per minute), group (several premature contractions in a row).
Often people with supraventricular premature beats have no symptoms. The most characteristic signs:
- Dizziness, feeling of weakness.
- Shortness of breath, lack of air.
- Fear, anxiety, panic, fear of death.
- Interruptions in the work of the heart, a feeling of its revolutions.
- Feeling of heart stopping or freezing.
- After freezing, a push to the chest.