What is Down syndrome?
Down syndrome is a genetic disorder in which a random mutation in the 21st pair of chromosomes results in a third copy.
Normally, a healthy person has 23 pairs of chromosomes, each containing an individual set of genes. Any change in their quantity (underdevelopment of one pair, the appearance of a third chromosome in a pair, doubling of a pair) and quality (all kinds of changes within the chromosome itself) leads to irreversible congenital disorders of human development. According to the Downside Up Foundation, about 2,500 thousand children with Down syndrome are born in Russia every year. 85% of families refuse them in the maternity hospital, including on the recommendation of medical personnel.
In the case of Down syndrome, an additional chromosome causes some features in appearance and pathologies of internal organs. The cardiovascular system and gastrointestinal tract are most often affected. The extent of symptoms varies among individuals, but all patients have lifelong mental retardation and developmental delays. Despite this, people with Down syndrome can study, work, play sports, take driver's license tests, act in theater and participate in beauty pageants².
Melanie Segard, who has Down syndrome, talks about the weather on French television. Photo: Franceinfo
In recent decades, there has been an increase in the incidence of Down syndrome. This is due to the increasing age of pregnant women and the negative impact of environmental factors on human health. Between 1979 and 2003, the incidence of Down syndrome in the United States increased by 30%¹.
In Russia, assistance to children and adults with Down syndrome is provided by such projects as “Love Syndrome”, the “Downside Up” Foundation and others. They organize fundraisers, hold thematic meetings, events in support of their wards, and help children with employment.
Correction and treatment of Down syndrome
Curing a chromosomal abnormality is currently impossible, but systematic medical observation and corrective assistance for children with Down syndrome make it possible to achieve success in their development, socialization and acquisition of work skills.
Most patients with Down syndrome have intellectual development disorders - usually mild or moderate mental retardation. The motor development of children with Down syndrome lags behind their peers, and there is also systemic underdevelopment of speech. Our medical center has developed unique schemes of rehabilitation measures for children with Down syndrome, which are aimed at treating mental retardation and delayed speech development.
To stimulate and develop mental functions, we use the method of bioacoustic correction of the brain, physiotherapy, exercise therapy, and transcranial micropolarization.
In combination with training on simulators using biofeedback (BFB).
To develop psycho-speech and communication skills, children with Down syndrome need classes with a neuropsychologist and speech therapist.
Psychological and pedagogical support for families raising “sunny children” plays an important role.
In all cases, children with Down syndrome are classified as children with special educational needs, and therefore require additional help from teachers and social educators, the use of special educational programs, and the creation of a favorable and safe environment.
Risk factors for having a child with Down syndrome
There is no specific reason that in 100% of cases leads to the birth of a child with Down syndrome. However, there are risk factors that increase the likelihood of having such children. These include:
- Mother's age. The risk of conceiving a child with Down syndrome increases in women after 35 years of age, since over the years the eggs tend to divide chromosomes incorrectly. Thus, according to the National Down Syndrome Society (USA), at 35 years of age a woman’s risk of conceiving a sick child is 1:350 cases, 1:100 by the age of 40, and reaches 1:30 at 45 years of age. According to some studies4, paternal age is also a risk factor: in the study group, men over 40 years of age had a 2-fold increase in the likelihood of having a child with Down syndrome. However, this factor has so far been less studied.
- The family already has a child with Down syndrome. The risk in this case increases significantly. When planning a pregnancy, both parents are referred to a genetic counselor, who will prescribe an additional examination, analyze their specific situation and be able to assess the risks more accurately.
- One of the parents is a mosaic or a carrier of the translocation. 7-8% of children with Down syndrome have a translocation or mosaic form of the syndrome. A small proportion of them inherited the translocation from their parents, despite the fact that the father and mother did not have signs and symptoms of Down syndrome.
Publications in the media
Down syndrome (trisomy 21, trisomy G) is a chromosomal disease caused by trisomy in the chromosome. 21, usually due to a violation of chromosome segregation during meiosis of the egg.
The frequency is 1 in 650 live births (the overall frequency in the population is higher, given that over 2/3 of affected fetuses die in utero). The frequency increases with maternal age, which is confirmed by amniocentesis data (especially sharply after 30 years).
Genetic aspects • Trisomy 21: 90-95% of patients have extra chr in all cells. 21 • Unbalanced translocation 21: 5% of patients have long arm chr. 21 is translocated to another chromosome, usually to 14. Among translocation trisomies, 1/2 are new, 1/2 are a consequence of a balanced translocation in one of the parents • Mosaic trisomy 21: 2 or more cell populations are found in 1–5% of patients : usually normal and trisomy 21 (clinical manifestations are usually less pronounced).
Pathomorphology. After 20 years, 100% of patients have plaques characteristic of Alzheimer's disease in the brain.
Clinical picture • Newborns and children •• Brachycephaly (100%) •• Mongoloid eye shape (90%) •• Epicanthus (90%) •• Muscular hypotonia (80%) •• Macroglossia (75%) •• Brushfield spots (light spots ["salt and pepper"] of the iris) on the iris (50%) •• Ear abnormalities •• Convergent strabismus •• Wide bridge of the nose •• Small chin •• Short neck •• CHD (up to 30% of children) •• Dermatoglyphics • •• Four-digit palmar fold ••• Absence of plantar curls (pads of the toes) ••• Convergence (up to fusion) of 2–3 flexor folds of the little finger •• Stenosis or atresia of the duodenum •• Absence of the anus •• Hirschsprung's disease in 2– 3% of children •• Delayed psychomotor development (may not appear until 1 year of age) •• Increased susceptibility to infections • Adults. Most manifestations are milder, brachycephaly persists. Patients experience delayed cognitive function (IQ - 40–45), although individuality and communication skills are preserved. After age 35, dementia similar to Alzheimer's disease develops. Most patients are capable of self-care. Some have jobs, although they require guardianship. Some patients exhibit autistic tendencies, and a small percentage of patients are nonverbal. Men are always infertile (no spermatogenesis).
Diagnostics • Study of the chromosome set (karyotype) is always necessary to exclude translocations • Given the frequent combination with leukemia - hematological studies annually • Determination of the level of thyroid hormones (hypo-, hyperthyroidism) is indicated • In children with pyuria and fever of unknown etiology - abdominal ultrasound to detect urinary tract abnormalities • In all children - EchoCG (VSD may not be apparent at birth).
Prenatal diagnosis • Ultrasound: •• Brachycephaly •• Hypotelorism •• Excessive cervical fold (16–29 weeks of gestation) •• Increased anteroposterior size of the nuchal space (10–14 weeks of gestation) •• Moderate ventriculomegaly •• CHD •• Hyperechoic intestine •• Duodenal atresia •• Non-immune hydrops fetalis •• Moderate hydronephrosis •• Shortening of the limbs •• Hypoplasia of the middle phalanx of the little finger • Biochemical parameters of maternal serum •• Decrease in the level of serum AFP less than 50% •• Increase in the level of hCG and unconjugated estriol.
Differential diagnosis. Trisomy 22 and deletion of the short arm of the chr. 9 may clinically resemble Down syndrome, which requires mandatory karyotype testing.
Management tactics • Genetic research and consultation • CVS research.
Surgery. Correction of congenital heart disease.
Complications • Intestinal obstruction (fistulas, intestinal tube abnormalities in 10% of cases) • Thyroid diseases (hypo- and hyperthyroidism in 5–8%) • Leukemia (0.5%) • Alzheimer's disease in older age.
Course and prognosis. The outcome and duration of the disease largely depend on the presence of congenital heart disease. Life expectancy is reduced: 30% die in the first year of life, 50% do not survive beyond the age of 5, and only 8% survive beyond 40 years. In 1/3 of patients, development is within normal limits in the first year of life; subsequently, mild deviations occur (slow development after the first year of life, moderate deviations in speech and cognitive functions). Gastrointestinal complications and heart failure with congenital heart disease can begin suddenly. Hypothyroidism usually appears 6 months after birth; a typical symptom is growth retardation.
Age characteristics. In 1/3 of patients over 35 years of age, clinical manifestations of Alzheimer's disease are observed.
Prevention • Prenatal karyotyping in women at risk • Low levels of AFP in maternal serum at 14–16 weeks of pregnancy (helps identify 1/3 of cases).
ICD-10 • Q90 Down syndrome
Note. The terms “Mongolism” and “Mongoloid idiocy” were previously used to refer to the disease.
Treatment
There is no cure for Down syndrome. Therapy is aimed at pathological conditions caused by the syndrome itself. Surgery is performed for congenital malformations, infectious diseases are treated, ophthalmic pathologies, metabolic disorders, etc. are corrected. All this is carried out with the participation of a group of medical specialists - children with Down syndrome must visit them regularly.
Sunny is the name given to children with Down syndrome. They are kind and smiling. Photos: freepik.com
In 2011, the American Academy of Pediatrics (AAP) for the medical surveillance of children with Down syndrome developed guidelines that describe age-specific routine screening for a child with Down syndrome. Its goal is the early diagnosis of concomitant pathologies:
- Echocardiography: during prenatal consultation or immediately after birth.
- Thyroid testing (thyroid-stimulating hormone (TSH) levels): done at birth, 6 months, 12 months, and then annually.
- Hearing assessment: At birth, then every 6 months until normal hearing is confirmed (around 4 years), then annually thereafter.
- Ophthalmological assessment: by 6 months, then annually until 5 years; then every 2 years until age 13 and every 3 years until age 21.
- Physical development: Height, weight and head circumference are determined at each examination using a Down syndrome growth scale.
- Sleep Study for Obstructive Sleep Apnea: Completed by 4 years of age.
In addition to specialized specialists, the most important role in the life of a special child is played by preventive specialists: speech therapists, physiotherapists, rehabilitation doctors, speech pathologists, massage therapists, etc.
Down syndrome is not a barrier to success
People who have become famous show by their example that even with Down syndrome you can realize yourself in life and achieve success.
- Karren Gaffney. He runs a non-profit organization that deals with the adaptation of children with disabilities into society. Karren's left leg is paralyzed, but she became the first person with Down syndrome to swim the English Channel. She won a gold medal at the Paralympic Games and recently received an honorary doctorate from the University of Portland in Oregon.
- Pablo Pineda. Spanish actor, who in 2009 received the “Silver Shell” at the San Sebastian Film Festival for Best Actor in the film “Me Too.” Lives in Malaga, works in the municipality, teaches, has several diplomas: teaching, bachelor of arts and diploma in educational psychology.
- Ronald Jenkins. A young man with Down syndrome, musician and composer. Ronald began playing the piano at the age of four. At the age of 17, he began posting his videos on Youtube under the pseudonym Big Cheez. At the same time, he released his first album, Straight Laced by Fish.
- Paula Sazh. Born in Scotland in 1980. She has starred in several films, plays netball professionally, and became a lawyer. Paula provides legal support to two international foundations: Ann Craft and Mancap.
- Melanie Segard. The girl dreamed of becoming a weather forecaster. A friend advised her to make a short video about herself and post it on social networks. In just a few days, more than 180 thousand people supported her dream, and now the page has over 255 thousand subscribers. A week later, Melanie’s dream came true - she received an offer from two national channels, and now she talks about the weather.
Characteristic signs and symptoms
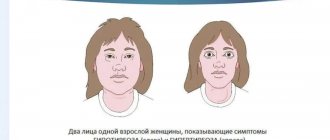
People with Down syndrome may act the same and be similar to each other, but each will have varying degrees of symptoms. Common ones include an intelligence quotient (IQ) ranging from moderate to low, slower speech than other children, and some physical features.
External signs of Down syndrome:
- flattened face, especially the bridge of the nose;
- slanted almond-shaped eyes, epicanthus - a vertical fold of the eyelid at the inner corner of the eye;
- small white spots (Brushfield spots) on the iris;
- a tongue that is often visible from an open mouth;
- short neck;
- small ears;
- one palmar fold instead of two;
- short stature;
- low muscle tone and weak joints.
Figure 1. External signs of people with Down syndrome.
. Image: kavusta / Depositphotos In addition to externally visible features of physical development, various pathologies of internal organs are observed with Down syndrome³.
Heart defects are common: About half of children with Down syndrome have some kind of birth defect. If there is a threat to life, then in the first weeks after birth the baby undergoes cardiac surgery. In addition to heart defects, some children develop developmental anomalies of the gastrointestinal tract: intestines, esophagus, anus. The risk of developing digestive problems such as gastrointestinal obstruction, heartburn (gastroesophageal reflux) or celiac disease increases. Due to malfunctions of the immune system, people with Down syndrome have an increased risk of developing autoimmune and infectious diseases, and some forms of cancer.
Soft tissue and skeletal changes can lead to airway obstruction, which can cause sleep apnea (sleep apnea) in both children and adults.
Also, due to their metabolism and endocrine system, people with Down syndrome are more likely to be obese compared to the general population.
“Monkey fold” on the palm. People with Down syndrome have one transverse palmar crease, rather than the usual two. Photo: Indian journal of human genetics / Open-i (CC BY-NC-SA 2.0)
Complications and prognosis
Complications of Down syndrome include:
- congenital heart defects;
- infectious diseases;
- leukemia;
- early dementia (Alzheimer's disease);
- stopping breathing during sleep;
- obesity.
The life expectancy of people with this pathology is low, about 49-50 years, but recently it has increased: back in the 20th century, such patients lived for about 25 years. They are able to create families, but men cannot have children. As a rule, people with Down syndrome receive secondary education and work.
Diagnosis of Down syndrome
The diagnosis is made on the basis of a characteristic clinical picture - a set of external signs, monitoring the rate of physical and intellectual development of the child, and the presence of pathology of internal organs. Newborns are tested for Down syndrome when indicated - in particular, if external signs indicate it. The diagnosis is confirmed by karyotyping - a study of the child’s chromosomes for the presence of an altered karyotype.
In addition, the functions of internal organs that are often impaired in Down syndrome - the thyroid gland, visual and auditory analyzers - are examined. Possible heart defects and leukemia are identified. For this purpose, the child is prescribed an ultrasound examination of the abdominal organs and heart, consultations with specialist doctors: a pediatric cardiologist, a surgeon, an ophthalmologist, and an orthopedic traumatologist.
During pregnancy, women undergo the following tests: screening - they are mandatory for everyone and special ones, which are prescribed by a doctor according to indications. The examinations are aimed at identifying various diseases and genetic abnormalities in the fetus (including Down syndrome, one of the most common genetic disorders).
Expectant parents at risk should consult a geneticist. Photo: photographee.eu / Depositphotos
Symptoms in newborns
A doctor may suspect Down syndrome immediately after the birth of a child based on characteristic signs. However, an accurate diagnosis is established after determining the karyotype (chromosome set).
“Daunyats”, for the most part, have a flat face with a Mongoloid eye shape and a short, rounded skull (brachycephaly). In the eyes, there is a vertical fold of skin that covers the inner corner of the eye (epicanthus).
There is increased joint mobility and muscle hypotonia, due to which the child’s mouth is slightly open and the tongue is extended.
The back of the head of children is flattened, the neck is shortened with a small head and vertically set ears with attached lobes, and there are dental anomalies.
Over the age of 8 years, eye diseases (cataracts, glaucoma) often develop. The bridge of the nose of the “downyat” is also flattened, and there is often a squint and a short nose.
There is one transverse fold in the palm, and the little finger is shortened and curved.
Often such babies are diagnosed with congenital heart and digestive tract defects, symptomatic epilepsy and chest deformation.
Sick children can reach average height, but often their physical development lags behind due to skeletal development disorders.
All patients with this pathology have mental retardation to varying degrees.
Prenatal diagnosis
The general scheme of prenatal diagnosis looks like this:
1. In the first trimester of pregnancy:
- Human chorionic gonadotropin (hCG) is a hormone that is produced by the membrane of the embryo and is involved in maintaining pregnancy.
- Pregnancy-associated plasma protein A (PAPP A). Abnormal levels of hCG and PAPP-A may indicate abnormal fetal development.
- Ultrasound examination - allows you to identify specific ultrasound signs of anomaly in the fetus.
2. In the second trimester of pregnancy:
- Ultrasound diagnostics.
- Alpha fetoprotein (alpha FP) - Low levels may indicate Down syndrome.
- Beta subunit of human chorionic gonadotropin (beta-hCG). An increase in hCG concentration in some cases is associated with a child’s illness.
- Free estriol. Low estriol levels can be a sign of Down syndrome.
The results of ultrasound, PAPP-A, alpha-FP, hCG and estriol, combined with data on the age and heredity of the mother, allow us to calculate the risk of having a child with Down syndrome.
Data from prenatal testing are especially important for women at risk of having children with Down syndrome. If the risk turns out to be very high, the following invasive (involving the skin) studies may be prescribed:
- Amniocentesis is the removal of a sample of amniotic fluid and subsequent examination of the fetal chromosomes.
- Chorionic villus biopsy - obtaining a sample of tissue from the chorion (the outer embryonic membrane surrounding the embryo). It also allows you to detect chromosomal abnormalities.
- Umbilical cord blood collection - a test performed if previous tests have been ineffective.
For women with a predisposition to the disease, genetic counseling is recommended when planning pregnancy.
Down syndrome is detected during pregnancy. Women undergo mandatory prenatal screening. Photo: freepik.com
Down syndrome is a genetic disease that causes mental retardation, delayed physical development, and congenital heart defects. In addition, it is often accompanied by dysfunction of the thyroid gland, impaired hearing, and vision.
Down syndrome is the most common disorder caused by a chromosome abnormality. As the mother ages, the risk of having a child with Down syndrome increases.
The disease has no cure and its severity may vary.
Treatment depends on the manifestations of the disease. Although it is impossible to get rid of the syndrome itself, working with a defectologist from an early age contributes to the development of the child’s mental functions.
Synonyms Russian
Trisomy on chromosome 21, Trisomy G.
English synonyms
Down Syndrome, Down's syndrome, Trisomy 21.
Symptoms
Children with Down syndrome may have specific facial features and head structure:
- small head,
- wide face,
- short neck, excess skin on the back of the neck,
- short and wide nose
- underdeveloped upper jaw,
- light gray spots on the iris of the eyes until the 12th month of life,
- epicanthus - a semilunar skin fold in the inner corner of the upper eyelid - the “third eyelid” - and, as a consequence, a narrow, Mongoloid shape of the eyes,
- small, asymmetrical, low-set ears,
- large tongue without a central groove, often open mouth,
- incorrectly positioned teeth.
The following symptoms are also characteristic of patients with Down syndrome:
- low muscle tone,
- disproportionate physique,
- underdevelopment of sexual characteristics,
- wide short palms with one fold instead of two, the thumb is located low in relation to the other fingers,
- sandal-shaped gap between the first and second toes,
- relatively short, overly flexible fingers.
Children with Down syndrome usually develop more slowly than normal. They begin to sit, crawl and walk about twice as late as typically developing children.
Patients also have a moderate degree of mental retardation.
General information about the disease
Down syndrome is a genetic disorder caused by an abnormality of chromosome 21 that causes mental retardation, heart defects, and developmental disorders.
It is often accompanied by dysfunction of the thyroid gland, hearing and vision impairment.
There are 23 pairs of chromosomes in the human chromosome set. In this case, one chromosome from a pair comes from the mother, one from the father. There are a total of 46 chromosomes in the body.
The cause of Down syndrome is an abnormality of chromosome 21, which is characterized by the presence of additional copies of genetic material on chromosome 21 in the form of trisomy or translocation. The 21st chromosome affects almost all organ systems and is responsible for the traits and developmental features that are impaired in Down syndrome.
- Trisomy 21 involves the presence of a copy of this chromosome. That is, instead of two chromosomes, the 21st pair is represented by three. Thus, in all cells of the body there are three chromosomes of the 21st pair instead of two.
Trisomy accounts for 95% of cases of chromosome 21 abnormality. It occurs when cell division is disrupted during the formation of reproductive cells (sperm and eggs) of the parents. Almost always, the extra chromosome is passed on to a child with Down syndrome from the mother. As the mother's age increases, the risk of having a child with Down syndrome increases. The older the egg, the greater the likelihood of improper cell division.
- The mosaic version of the syndrome occurs when only some cells of the body have an abnormal copy of the 21st chromosome. The “mosaic” of abnormal and normal cells is caused by a violation of cell division after fertilization in the embryo.
- Translocation of the 21st chromosome to other chromosomes (usually to the 15th or 14th). Children have two pairs of chromosomes 21 and additional material from chromosome 21. In this case, part of the 21st chromosome moves to another when chromosome division is disrupted during the formation of sperm and eggs of the parents (about 25% of translocation cases) or at the time of conception (about 75% of cases).
Thus, Down syndrome is caused by a violation of cell division during the development of an egg, sperm or embryo.
Down syndrome is not a hereditary disease, although there is a predisposition to its development. Women with Down syndrome have a 50% chance of giving birth to an affected child, and spontaneous abortion often occurs. Men with Down syndrome are infertile, with the exception of the mosaic variant of the syndrome.
Carriers of a genetic chromosome translocation will also have an increased likelihood of having a child with Down syndrome. If the carrier is the mother, the child with Down syndrome is born in 10-30%, if the carrier is the father - in 5%.
Women who have a child with Down syndrome have a 1% chance of having a second affected child.
Children with Down syndrome may experience the following complications.
- Heart defects. About half of children with Down syndrome are born with heart defects, which may require surgery in early childhood.
- Leukemia (malignant disease of the hematopoietic system). Children with Down syndrome, especially at an early age, are more likely to develop leukemia than other children.
- Infectious diseases. Due to disorders of the body's immune system, children with Down syndrome are more susceptible to infectious diseases.
- Dementia. After age 40, people with Down syndrome have an increased risk of developing dementia.
- Sleep apnea. Children with Down syndrome are predisposed to sleep apnea, a condition in which ventilation to the lungs stops for 20-30 seconds during sleep. In severe cases, apnea can occupy up to 60% of all nighttime sleep. Regular apnea leads to daytime sleepiness, memory impairment, decreased intelligence, decreased performance, and constant fatigue.
- Obesity.
The life expectancy of people with Down syndrome depends on the severity of the manifestations and averages 50 years or more.
Who is at risk?
- Women with Down syndrome (men with Down syndrome are usually infertile).
- Mothers after 30 years. With age, the risk of having a child with Down syndrome increases: by the age of 35 it is 1 in 400, by 45 it is 1 in 35. However, approximately 80% of children with Down syndrome are born to mothers under 35 years of age.
- Fathers over 42 years old.
- Carriers of genetic chromosome translocation. If the mother is the carrier, the risk of having a child with Down syndrome is about 10-30%, if the father is about 5%.
- Parents who already have a child with Down syndrome. The risk of having another child with this condition is approximately 1%.
Diagnostics
The diagnosis is made based on the characteristic clinical picture. Newborns are tested for Down syndrome. Pregnant women are also prescribed tests aimed at identifying Down syndrome in the fetus.
Down syndrome is suspected based on the presence of appearance features characteristic of this disease. The diagnosis is confirmed by karyotyping - examining the child’s chromosomes for abnormalities.
In addition, functions that may be impaired in Down syndrome are examined - thyroid function, visual and auditory analyzers. Possible heart defects and leukemia are identified.
- Thyroid-stimulating hormone (TSH) is a hormone produced by the pituitary gland, a small gland located in the brain. It regulates the functioning of the thyroid gland. When its function is impaired, its level usually changes.
- Thyroxine is a hormone produced by the thyroid gland and affects many types of metabolism in the body. In Down syndrome, its level may be reduced.
- Bone marrow biopsy. Examining a bone marrow sample under a microscope can detect leukemia.
In a fetus, Down syndrome can be suspected based on screening results and ultrasound data. Alpha-fetaprotein testing is recommended for all pregnant women. In addition, examination of pregnant women involves the following tests.
First trimester of pregnancy
- Human chorionic gonadotropin (hCG) is a hormone that is produced by the membrane of the embryo and is involved in maintaining pregnancy.
- Pregnancy-associated plasma protein A (PAPP A). Abnormal levels of hCG and PAPP-A may indicate abnormal fetal development.
Second trimester of pregnancy
- Ultrasound examination - allows to identify fetal development disorders.
- Alpha fetoprotein (alpha FP) – low levels may indicate Down syndrome.
- Beta subunit of human chorionic gonadotropin (beta-hCG). An increase in hCG concentration in some cases is associated with a child’s illness.
- Free estriol. Low estriol levels can be a sign of Down syndrome.
The results of ultrasound, PAPP-A, alpha-FP, hCG and estriol, combined with data on the age and heredity of the mother, allow us to calculate the risk of having a child with Down syndrome.
These studies are especially important for women at risk of having children with this disease.
If the risk is found to be very high, the following studies may be carried out.
- Amniocentesis is the removal of a sample of amniotic fluid and subsequent examination of the fetal chromosomes.
- Chorionic villus biopsy - obtaining a sample of tissue from the chorion (the outer embryonic membrane surrounding the embryo). Allows you to identify chromosomal abnormalities.
- Umbilical cord blood collection - allows you to identify chromosomal abnormalities. The test is carried out if previous studies have been ineffective.
For women with a predisposition to the disease, genetic counseling is recommended when planning pregnancy.
Treatment
Down syndrome cannot be cured, so therapy is aimed at specific manifestations of the disease.
If necessary, surgical operations are performed to treat heart defects, anomalies of the gastrointestinal tract, examination by a neurologist, cardiologist, ophthalmologist, defectologist, speech therapist, pediatrician, etc.
Early treatment will maximize the abilities of children with Down syndrome and improve their quality of life. Immediately after birth, it is extremely important to develop the child’s motor, cognitive sphere, and his mental functions. There are special preschool and school institutions where a program has been developed for children with the appropriate level of intelligence.
Prevention
Prevention of the birth of children with Down syndrome has not been developed. People who are at risk of having a child with this disease are recommended to undergo genetic testing when planning a pregnancy.
Recommended tests
- Free beta subunit of human chorionic gonadotropin (beta-hCG free)
- Pregnancy-associated plasma protein A (PAPP A)
- Alpha fetoprotein (alpha FP)
- Free estriol
- Thyroid-stimulating hormone (TSH)
- Free thyroxine (free T4)
- Total thyroxine (T4)
Literature
- Dan L. Longo, Dennis L. Kasper, J. Larry Jameson, Anthony S. Fauci, Harrison's principles of internal medicine (18th ed.). New York: McGraw-Hill Medical Publishing Division, 2011.
Causes of Down syndrome development
Normally, human cells contain 23 pairs of chromosomes. One chromosome of the pair belongs to the father, the other to the mother. Down syndrome occurs when the 21st pair of chromosomes gets three instead of two. The additional genetic material is responsible for the child's characteristics and developmental problems. There are three genetic variations in the formation of the syndrome.
The classic version of Down syndrome is trisomy 21, where each cell in the body has three copies of chromosome 21 instead of the usual two.
Figure 2. Karyotype of a person with Down syndrome. Wikipedia (Public Domain)
There are other options. In some cases, the syndrome occurs when part of chromosome 21 attaches to another chromosome during the formation of eggs and sperm in a parent or very early in the development of the fetus. The person then has two normal copies and an extra piece of chromosome 21 attached to another chromosome. The result is the same three copies of genetic material. This form is called translocation.
A small percentage of people with Down syndrome (1-2%) have an extra copy of chromosome 21 in only a portion of the body's cells. This is called mosaic Down syndrome.
Video 1. Causes, symptoms and diagnosis of Down syndrome.
Classification
According to the mechanism of development of Down syndrome, there are three forms:
- Trisomy on chromosome 21.
- Translocation form of Down syndrome.
- Mosaic form of Down syndrome.
The first form accounts for about 95% of cases of the disease and up to 5% for the other two.
Prognosis for people with Down syndrome
The life expectancy of people with Down syndrome has increased significantly. Thus, in 1960, a child with Down syndrome often did not live to see his 10th birthday. Today, the life expectancy of people with this disease is 50-60 years.
Video 2. People with Down syndrome answer questions, talk about the attitude of others towards them, about family, love, their dreams and plans for the future.
Educational and socialization opportunities for individuals with Down syndrome vary. They largely depend on the child’s intellectual abilities and on the efforts made by parents and teachers. In almost all cases, children with Down syndrome manage to acquire the household and communication skills necessary in everyday life. There are patients who have achieved success in the fields of art, acting, sports, and also in higher education. Adults with Down syndrome can lead an independent life, master simple professions, and have their own family.
The support of experienced professionals (doctors, rehabilitation therapists, psychologists, social educators) and the understanding of family and friends are crucial for people with Down syndrome. In many countries, there are communities of patients where parents of such children and the children themselves, as well as adults with Down syndrome, can receive support, discuss pressing problems, and share their successes.
Down syndrome – a sentence or hope?
Down syndrome is the most common genetic abnormality caused by trisomy 21 pairs of chromosomes. According to statistics, approximately 1 in 700 children are born with Down syndrome. This ratio is the same in different countries, climate zones, and social strata. It does not depend on the parents’ lifestyle, their health, bad habits, nutrition, wealth, education, skin color or nationality. The likelihood of having such a child increases with the age of the mother, but since younger mothers give birth more often, all age categories are equally represented among parents of children with Down syndrome.
This syndrome was described by John Langdon Down in 1866 as a mental retardation associated with a number of characteristic external signs. And in 1959, Jerome Lejeune revealed its genetic nature.
By 1964, three main types of chromosomal abnormalities in Down syndrome became known:
- Standard trisomy (94%) - tripling of chromosome 21 is present in all cells and occurs as a result of a violation of the process of meiosis.
- The mosaic form (2%) is caused by disturbances in the mitosis process in one of the cells at the blastula or gastrula stage; tripling of chromosome 21 is present only in the derivatives of this cell. In these forms, the parents have a normal genotype.
- Translocation form (4%) - the arm of one 21st chromosome is attached to another chromosome and during meiosis moves into the resulting cell along with it. Before the birth of their next child, parents must undergo genetic testing.
A presumptive diagnosis, as a rule, is made immediately after the birth of a child based on a number of external signs: “flat” face (90%), brachycephaly (81%), skin fold on the neck in newborns (81%), anti-Mongoloid eye shape (80%), epicanthus (80%), joint hypermobility (80%), muscle hypotonia (80%), short limbs (70%), arched palate (58%), etc. Transverse palmar fold, considered a universal sign of Down syndrome, occurs in 45% of cases, and Brushfield spots (pigmented spots along the edge of the iris) in 19% of cases. Usually, a newborn with Down syndrome has some of the known signs, sometimes some signs are also found in ordinary children. The final diagnosis is made after receiving the results of the karyotype analysis.
Down syndrome is often accompanied by somatic diseases.
Many children are often born with signs of morphofunctional immaturity. Congenital heart defects occur in 40–60% of cases. A common disorder is sleep apnea (up to 50%), which occurs due to the structural features of the nasopharynx, and obstruction of the oropharynx by the root of the tongue. Acquired forms of hypothyroidism can account for up to 35% and require special attention, since the clinical signs of hypothyroidism are masked by manifestations of Down syndrome. Pathology of the musculoskeletal system (including muscle hypotonia and hyperelasticity of ligaments) is present in almost all children. Ophthalmological problems occur in 45%, hearing loss in 38–78%, and gastrointestinal abnormalities in 12% of cases.
Developing prenatal diagnostics make it possible to better diagnose Down syndrome and become more accessible to women in Russia. However, this method does not help resolve the question of whether the family is ready to raise a child with Down syndrome, but only postpones it to the period before the birth of the child. More and more families are turning to our Center in which the parents knew about Down syndrome before the birth of the child and decided to continue the pregnancy.
For many years, Down syndrome was considered a medical problem, as reflected by its old name "Down disease", and since this chromosomal abnormality cannot be cured, such patients were usually institutionalized from birth, where they were given general care . Comorbidities were also considered part of the syndrome and often went untreated. Children with Down syndrome in such conditions demonstrated a low level of psychophysical development with an average life expectancy of about 10 years.
The situation began to change about 50 years ago. Against the backdrop of the humanization of society in developed countries, it was recognized that the conditions of keeping people in closed institutions are not satisfactory, their rights are often violated, and long-term stay in inpatient conditions has an adverse effect on their condition. In addition, keeping people with intellectual disabilities in hospitals required unjustified financial costs. At the same time, psychological and educational research has shown the importance of emotional attachment to an adult and a stimulating environment for the development of a child. Parents of patients with developmental disabilities also advocated for the right of their children to live at home and receive all the care they need in the community. These requirements have found wide support among pediatricians. All this led to the beginning of the process of deinstitutionalization, that is, the dissolution of the boarding school system and the creation of local help services. These changes are reflected in UN documents defining the rights of children with developmental disabilities to life in a family, education and integration into society.
In Russia, the majority of children with Down syndrome continued to be in government institutions and only about 10% of children were raised at home. Attitudes towards people with Down syndrome have begun to change since the early 90s. Parent associations and public organizations played a big role in this. In 1997, a charitable foundation was created in Moscow, the purpose of which is to improve the quality of life of children with Down syndrome in Russia. In 1998, on the basis of this organization, an Early Help Center was opened, providing free psychological and pedagogical assistance to children from birth to 8 years. Until this time, families raising their children at home found it difficult to find professional support, and the developmental level of such children was not studied. All examinations of the level of development of children with Down syndrome were carried out in boarding schools, where for many children the factor of deprivation, that is, lack of parental love and care, turns out to be almost the leading factor in the genesis of their disorders. On the other hand, the development of a system of assistance to children living in families has made it possible to achieve good results in their rehabilitation and changed the idea of their capabilities. The data below is borrowed from foreign literature and confirmed by the experience of the Early Help Center (
.).
Thus, children with Down syndrome go through the same stages of development as ordinary children, and with special education, although somewhat later, they master the same skills.
Today, more than 1,000 families from Moscow and Russian regions receive information support, they are regularly treated and provided with advisory assistance. Such programs are becoming increasingly widespread in our country and neighboring countries.
The modern approach to teaching children with Down syndrome is based on a family-centered model of early assistance, which includes psychological and pedagogical support for parents and is focused on helping parents in raising their children. Much attention is paid to the development of young children (from 0 to 3 years), the prevention of secondary disorders that arise due to concomitant diseases or uneven development of the child. From the first weeks, teachers’ attention is focused on the interaction of parents with the child, motor development, cognitive processes, and the development of communication. From the age of 1.5 years, children begin to attend group classes aimed at socialization and preparation for kindergarten. By age 3, children typically enter kindergarten while continuing to receive additional special education activities. More and more kindergartens are organizing integrative groups, where children with Down syndrome are together with ordinary peers, and celebrate their positive influence on each other. By the age of 8, children enter schools selected according to their level of development. The majority of children study in specialized schools, but there are isolated examples of children with Down syndrome being taught in general education schools.
Of course, only interdepartmental interaction, including health, social protection and education authorities, makes it possible to comprehensively solve the problems of a child with developmental disorders and his family.
Since 2002, active work has been carried out aimed at preventing social orphanhood of children with Down syndrome, as well as changing attitudes towards this category of children in the professional medical environment and in the public consciousness.
The main components of the program are:
- Providing doctors in maternity hospitals with up-to-date knowledge about the developmental characteristics of children with Down syndrome living in families, the possibilities of pedagogical assistance for such children, and tactics for communicating the diagnosis. Information about the program and printed materials about Down syndrome are provided free of charge to maternity care facilities.
- Providing crisis psychological assistance and social support to parents who are at the stage of making a decision about the fate of the child.
- Inclusion of the family in the early assistance service literally from the first days of the child’s life, psychological and pedagogical support in the preschool period and upon admission to school.
The result of the implementation of this program is a steady increase in the number of children with Down syndrome raised in families. Thus, in 2002 in Moscow, approximately 15% of children remained in families, the same as the Russian average, and after 4 years of the program - in 2006 - 50% of children.
Let's talk about this project in more detail.
Many parents remember the words they heard in the maternity hospital for many years. Because Down syndrome is diagnosed immediately after a child is born, parents learn the diagnosis before their relationship with the child has formed, and often even before they see the child for the first time. The way in which the diagnosis is communicated greatly influences the subsequent development of the parent-child relationship and the acceptance of the child, even if the child remains in the family.
The message about Down syndrome destroys the image of the child that parents dreamed of during pregnancy, their plans and ideas about themselves as parents. The significance of this loss determines the intensity and duration of the experience. This process has several phases and ultimately aims to reorganize life in accordance with the new situation.
The first phase (shock) can be described with the words: “This cannot be, this is not happening to me.” It can last from a few minutes to several days. Then comes the reaction phase, which manifests itself in feelings of anger, conflict, distrust, and the search for someone to blame. These feelings often fall on those who happen to be nearby and report the diagnosis. It is important to understand that such behavior is a normal manifestation of this stage of grief, and to try to emotionally support the parents. This phase can last from several days to several weeks.
At the next stage, the adaptive phase begins. Parents gradually accept the fact that their child has Down syndrome, their anxiety noticeably decreases, and they begin to think about immediate needs. This phase can last up to a year. After this, the orientation or reorganization phase begins, when the family masters the role of parents of an unusual child, takes a constructive approach to solving their problems, seeks help from the appropriate services, makes plans for the future, and establishes new relationships.
Unfortunately, parents usually have to make a decision about the fate of the child while he is in the maternity hospital, that is, within the first few days after his birth. At this time, they are in a shock or reactive phase, and in this state it is almost impossible to make an informed decision. The ability to delay a choice gives them the time they need to adapt. The Early Help Center has recorded about 30 cases in which parents took their child home several days or months after abandonment.
The doctor in the maternity hospital who reports the diagnosis is also under stress caused by the failure of the newborn to meet his expectations, the need to convey unpleasant news, the expected reaction, etc. In addition, he turns out to be the only person to whom parents can turn, and he has to answer the question: “What does this mean?”, presenting pedagogical information about the development and socialization of the child, and also provide psychological support to the mother, answering the question: “What to do now?”
Without sufficient psychological preparation, doctors often act at the expense of their mental strength, “trying the situation on themselves.” Often it is difficult for a doctor to determine the boundaries of his responsibility, and he, sincerely wanting to help parents, advises them to abandon the child, based on their own ideas and their psychological resources. In this case, it turns out that the doctor advises to abandon a child who is not his own, and the parents have to abandon their own.
The mother's reaction, confusion, tears, and aggressive behavior also cause a desire to help her, and she is often prescribed medications that reduce the intensity of grief, but slow down its experience.
Understanding the limits of one’s capabilities and responsibilities, and the opportunity to invite a psychologist, teacher or representative of the parent association make the task facing them easier for doctors.
Let's take a closer look at what is important to do in the maternity hospital:
- congratulate the parents on the birth of a child, list the usual positive things in such cases: gender, height, weight, etc.;
- talk about his problems, examination plan and necessary medical measures;
- bring the baby to the mother, try to maintain breastfeeding, since this is extremely important for the child’s health, improving his contact with the mother and the development of speech in the future;
- provide parents with general information about Down syndrome, avoiding predictions, since the development of a newborn child cannot be predicted;
- support any decision of the parents about the future fate of the child;
- It is not permissible to agitate parents to make this or that decision, since we do not fully understand the circumstances of the life of this particular family and cannot share with them the responsibility for the jointly made decision;
- By kindly questioning parents about their decision, we bring them back to their feelings, their life circumstances, and their own motivations and responsibilities. This leads to the fact that they make a more natural decision - not to abandon the child and subsequently take a more active parental position;
- give time to make a decision about the fate of the child, since the condition of the parents after reporting the diagnosis often does not allow them to make an informed choice. Arrange, if necessary, a meeting with other family members or a psychologist;
- provide information about organizations where the family can receive support in the future. If the child still has medical problems, he should be sent to a medical institution; if he has developmental problems, he should be sent to a psychological or pedagogical institution. These could be educational services, parent mutual support groups, social services, etc. The best option, of course, is the early intervention service, since the family-centered model of early intervention allows parents to receive psychological support when contacting about the child's development.
Starting work with the family at the stage of the maternity hospital, including the family in the early intervention service, with the subsequent transition of the child to kindergarten, school and employment projects for adults, ensures the development, training and socialization of children, and also gives their parents the opportunity to work and lead a normal life life.
T. P. Medvedeva , Moscow