Types of pemphigus
People distinguish between true pemphigus (pemphigus) and other blisters on the skin. The true one is of the following types:
- ordinary, or vulgar - occurs most often. Externally intact and undamaged skin becomes covered with blisters with serous fluid inside, which burst easily and quickly and heal. Localization - the mouth area and the mucous membrane of the lips, as well as the nasolabial triangle. At first glance, harmless bubbles appear more and more often, each time occupying a larger area throughout the body. When they burst, they leave pink eczema in this place. The child should begin receiving adequate therapy between 6 months and 2 years. Otherwise, there is a danger of death;
- vegetative - the course of the disease differs from the usual type only in the consequences on the skin. In this case, instead of eczema, vegetation papillomas of a grayish tint remain. These papillomas are growing;
- leaf-shaped - got its name due to the visual appearance of the crusts formed after the bursting of bubbles. A distinctive feature of this species is the rapid development of pathology. In this case, the count is not in months, but in days. In this case, the skin peels off in whole pieces shaped like leaves;
- erythematous - is a complication after leaf-shaped and has no striking differences from the previous form of pathology;
- seborrheic - originates in the hair on the head and face. Small bubbles quickly become a yellowish crust. The progression of the pathology is slow, affecting the back, abdomen and limbs. After peeling off the crust, weeping eczema remains.
There are other types of pemphigus that are not related to pemphigus:
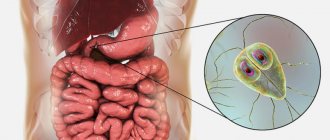
- infectious viral pemphigus in children - develops under the influence of viruses: Coxsackie, enterovirus 71. In this case, the latter option may have the nature of an epidemic. It has specific localization sites - feet and palms, butt and genitals;
- congenital syphilis - occurs when there is intrauterine infection with syphilis. It appears within a couple of days after birth. The blisters burst quickly and leave behind weeping pink eczema.
Untrue types of pathology in medicine refer to the symptoms of pemphigus in children. This course of the disease allows for faster and more correct treatment of pemphigus in children, aimed at eliminating the root cause. The most difficult thing in this pathology is establishing the true cause of the disease.
A rare but severe type of true pemphigus is the paratumor type. It has the most striking symptoms. It occurs against the background of leukemia and lymphoma, and also appears as a harbinger of the development of a malignant tumor.
Epidemic pemphigus of newborns
Signs
The disease develops very quickly.
First, the child develops a fever and becomes restless. Within a few hours, small blisters filled with a clear yellowish liquid form on the baby’s skin in the navel, abdomen, buttocks, arms and legs, chest, back, as well as on the mucous membrane of the mouth, nose and genitals. The skin around the blisters may be slightly red and swollen, or it may be normal. After some time, the bubbles increase in size, their contents become purulent. They open, the contents expire, and an itchy bright red erosion forms in place of the bubble. Pemphigus in newborns is often accompanied by refusal to eat and weight loss.
Description
Epidemic pemphigus of newborns is caused by Staphylococcus aureus. However, some experts believe that streptococci also play a role in the development of this disease. The source of the disease is the medical staff of maternity hospitals and women in labor suffering from pyoderma, furunculosis or hidradenitis. Pemphigus can also be transmitted from child to child through the hands and clothing of medical personnel.
Most often, this disease develops in weakened children, for example, in premature babies, in children with low body weight, in those who have suffered birth trauma, as well as in children whose mothers have suffered severe toxicosis of pregnancy. It is in these newborns that the skin reacts when bacteria penetrate it by forming blisters.
If the course of the disease is favorable, it is cured in 2-4 weeks. If unfavorable, complications are possible - phlegmon, pneumonia, sepsis. Sepsis can cause the death of a child.
A particularly severe form of epidemic pemphigus of newborns is Ritter's exfoliative dermatitis. With this disease, extensive erosions form, and within a few days the entire skin is affected.
Diagnostics
The diagnosis is made based on the clinical picture. Bacteriological culture of the discharge from the vesicles must be done.
The disease is differentiated from congenital epidermolysis, syphilitic pemphigus, and chickenpox.
Treatment
Epidemic pemphigus of newborns is treated with antibiotics and sulfonamides. The blisters are opened, the wounds are treated with an ointment with an antibiotic and aniline dye or a solution of potassium permanganate. Antihistamines are used to relieve itching.
In some cases, corticosteroid ointments are prescribed to relieve inflammation and itching.
If necessary, plasma or blood transfusions are given.
Prevention
To prevent epidemiological pemphigus in newborns, sick children are immediately isolated from healthy ones.
Maternity hospital staff are regularly examined for pyoderma and furunculosis. Those who become ill are removed from working with children.
It is important to thoroughly disinfect the rooms and not neglect wet cleaning and quartz treatment.
Linen in maternity hospitals must be changed frequently and must be sterilized.
© Dr. Peter
Causes of occurrence and development
The pathology begins its development after the development of autoimmune antibodies aggressive to desmoglein proteins. These proteins act as an adhesive base used to connect skin cells. In the process of protein destruction, the skin is destroyed. At this point, bacteria from the environment begin to penetrate the skin layers, causing the formation of blisters.
The factors that trigger the pathological process still remain unclear. Some of them are established by science:
- genetic predisposition to autoimmune processes;
- malfunctions of the central nervous system;
- the presence of viruses, infections or other pathogens in the body - a connection has been identified between infection with endogenous bacteria and the appearance of an autoimmune reaction.
Russian official medicine identifies the following reasons causing an inadequate immune response:
- taking medications of the thiol group - strong antibiotics, immunomodulators and others;
- burns;
- herpes virus types 1, 2 and 8;
- tactile contact with pesticides;
- severe stress or nervous overload.
It is almost impossible to establish the true cause of the disease. In fact, in laboratory conditions only the presence of aggressive antibodies is determined.
Symptoms and signs
The early stages of the disease have virtually no dangerous signs. The child’s health remains normal, and skin changes have not yet appeared. The condition worsens as the area of the affected skin gradually increases.
The bubbles themselves have a number of distinctive features - lethargy, easy to open, sagging skin under the liquid inside the bubble. Primary rashes are always localized in the mouth and mucous membranes of the lips. There are no painful sensations. Opened blisters form skin crusts or wet eczema, which take a long time to heal.
Gradually the affected area increases. Infection with bacteria leads to the appearance of suppuration and foci of inflammation, in place of which eczema and large erosions subsequently appear. Another distinctive feature is the lack of healing of the skin at the site of the blister rupture. Gradually, the erosions expand and unite into a single lesion.
All forms of pemphigus have a wave-like manifestation of symptoms. In the absence of a timely response, intoxication syndrome begins - nausea and headaches. Ultimately, the death of the little patient inevitably occurs. Viral pemphigus in children has symptoms similar to the true disease, and there is a pronounced viral infection.
When to see a doctor
Baby rash appears frequently and rarely poses a real threat to the child's life. Basically it becomes a reactive feature to allergens and infections. It is important for parents to know which rashes pose a mortal danger to the child. If signs of such a rash appear, you should seek help from a dermatologist.
The pediatric department of JSC "Medicine" (clinic of academician Roitberg) has been guarding children's health for many years. You can make an appointment with a dermatovenerologist by phone. The clinic has a convenient location, a two-minute walk from the Mayakovskaya metro station, as well as the possibility of placement in a hospital for examination and treatment.
Hereditary pemphigus (epidermolysis bullosa)
The paper outlines the clinical features of the most common types of pemphigus neonatorum (epidermolysis bullosa), diagnostic problems, the basic principles of treatment, potentialities of prevention. Particular emphasis is laid on a diet, care, treatment of complications, and topical therapy. IN AND. Albanova, Pharmaceutical Research and Production Enterprise "Retinoids", Chief Physician of the Diagnostic and Treatment Centre, Doctor of Medical Sciences. Sciences, dermatovenerologist. VI Albanova, MD, dermatovenereologist, Head Physician, RETINOIDS Therapeutical-and-Diagnostic Center, RETINOIDS Pharmaceutical Research and Production Enterprise. N
hereditary epidermolysis bullosa is a group of blistering hereditary skin diseases that includes more than 20 monogenic dermatoses. Since the question of the independence of many of them has not yet been resolved, it is customary to call them forms of hereditary epidermolysis bullosa. Clinically common to all forms is the early onset of the disease, most often from birth or the first days of life, and the occurrence of blisters or erosions on the skin and mucous membranes as a result of minor mechanical trauma (“mechanobullous disease”). The presence or absence of scars after healing provides the basis for dividing all forms into dystrophic and simple. With the introduction of electron microscopy into the diagnosis of hereditary epidermolysis bullosa, all forms began to be divided into 3 groups: simple, borderline and dystrophic epidermolysis bullosa. In simple forms of epidermolysis bullosa, the formation of blisters occurs as a result of cytolysis of basal epithelial cells, which is revealed on electron diffraction patterns in the form of pronounced swelling of their cytoplasm with rupture of the cell membrane. In this case, the intact basement membrane is located at the base of the bladder. In borderline forms, separation of the epidermis from the dermis occurs at the level of the light plate of the basement membrane of the epidermis due to the inferiority of hemidesmosomes and attachment filaments. A dense lamina of basement membrane is located at the base of the blisters. In dystrophic forms, the separation of the epidermis from the dermis occurs below the basement membrane and is associated with the inferiority of the attachment fibrils - the structures connecting the basement membrane with the dermis. To carry out treatment, it is enough to know the main clinical forms. However, issues of prognosis and genetic counseling can only be resolved on the basis of an accurate diagnosis, which is currently only possible in large diagnostic centers with specialists in hereditary skin diseases and electron microscopy of the skin (Central Dermatovenerological Institute of the Ministry of Health of the Russian Federation), as well as using the method immunofluorescence or immunohistochemical mapping. Let us briefly look at the main clinical signs of 6 significantly different nosological forms of hereditary pemphigus.
Simple generalized epidermolysis bullosa
The disease is inherited in an autosomal dominant manner and manifests itself from birth or the first month of life. The first blisters appear on the feet, less often on the hands, subsequent ones - in places of pressure from clothing and shoes, as well as friction (neck, lower back, elbows, knees). With age, the number of rashes decreases, which is apparently due to the ability of patients to avoid mechanical injuries. Exacerbation always occurs in the warm season, although in young children seasonal fluctuations are not always noticeable. Bubbles and erosions appear a short time after the injury (20 - 30 minutes). The blisters have a hemispherical shape, a dense elastic covering, serous or, less often, bloody contents (Fig. 1). A ring of hyperemia appears around the bubble. Subjectively, the appearance of a bubble is accompanied by a burning sensation and pain, especially intense in the first hours after its formation. Emptying the blisters brings relief to the patient and prevents further increase in their size. Healing occurs quickly (2 - 3 days), while the lining of the bladder dries out and peels off. If the covering of the bladder is cut off, the resulting erosion becomes covered with a crust and healing is somewhat delayed. The healing period is accompanied by itching. After healing, slight flaking and pigmentation may occur. The repeated appearance of bubbles in the same place is typical.
Rice. 1. Patient N., 19 years old. Simple generalized epidermolysis bullosa. Fresh hemispherical bubble with serous contents.
All patients have hyperhidrosis of the palms and soles. Gradually, focal hyperkeratosis forms at the sites of pressure and friction on the soles. Changes in the nail plates (yellowish-gray color, thickening, curvature) are observed in all adult patients. Mycoses of the feet are often associated with the underlying disease.
Rice. 2. Patient K., 8 years old. Epidermolysis bullosa herpetiformis simplex. Typical lesions are round in shape with pigmentation in the center and blisters and crusts along the periphery.
In young children, blisters sometimes appear on the oral mucosa, but due to the rapid healing of erosions, they often go unnoticed, and when infected, aphthous stomatitis is diagnosed.
Simple localized epidermolysis bullosa
The disease is characterized by the same symptoms as the previously described form, but the rashes are located exclusively on the hands and feet. The literature describes cases where the first signs of the disease occurred much later than usual - in adults during military service or agricultural work with increased load on the feet. In some patients, the disease begins with widespread rashes, which gradually turn into localized ones, which indicates the genetic commonality of generalized and localized epidermolysis bullosa simplex.
Epidermolysis bullosa herpetiformis simplex
It is inherited in an autosomal dominant manner, but sporadic cases are common. The disease begins at birth or the first week of life. The first rashes are usually located on the hands and feet, they spread quickly, which is accompanied by a disturbance in the child’s general condition (loss of appetite, anxiety, sleep disturbances, and often a rise in temperature). The blisters quickly erode, and areas devoid of epithelium sometimes occupy most of the skin. Secondary infection of erosions and dehydration develop. By 3-6 months of age, the rashes acquire a typical appearance for this form - hemispherical blisters with a tense tire and serous, hemorrhagic or purulent contents, as well as erosions covered with crusts, forming ring-shaped, arched, scalloped foci, in the center of which there is a pigmentation zone ( Fig. 2). Each individual erosion heals quickly, the healing of the entire lesion lasts for 1 - 1.5 months.
Rice. 3. Patient S., 10 years old. Dominant dystrophic epidermolysis bullosa. Blisters and erosions in frequently injured areas, skin atrophy on the legs and knees.
Most often, lesions are located around the mouth and nose, on the hands, feet, and knees, but any area of the skin can be affected.
| Rice. 4. Patient M., 25 days. Recessive dystrophic epidermolysis bullosa. Multiple blisters, erosions, erythematous spots. | Rice. 5. Patient L., 10 years old. Recessive dystrophic epidermolysis bullosa. Erosions, crusts, cicatricial atrophy of the skin. | Rice. 7. Patient K., 6 years old. Recessive dystrophic epidermolysis bullosa. Contractures and syndactyly of the feet and hands, extensive areas of skin atrophy. |
The progression of the pathological process can be observed from several months to a year, after which a gradual improvement occurs - a decrease in the area of skin lesions, a less frequent occurrence of blisters and infected rashes, and normalization of the general condition. From 2 to 3 years of age, patients experience a distinct seasonality of exacerbations - in the summer there are more rashes. Sometimes complete resolution of the rash is observed when the body temperature rises above 38° C during infectious diseases. By the end of the first ten years of life, the occurrence of blisters becomes rare, and in the second it stops.
Rice. 6. Patient Zh., 7 years old. Recessive dystrophic epidermolysis bullosa. Contractures and syndactyly of the hands.
All patients have hyperkeratosis of the feet, which gradually increases with age. After the blistering stops, it sometimes becomes the only symptom of the disease. The oral mucosa is affected in most patients. Epithelization of erosions in the mouth occurs very quickly, leaving no traces. Caries, less often defects of tooth enamel and anomalies in the position of teeth, are present in all patients over 2 years of age. A variety of nail changes are observed in all patients and progress with age. In the first year of life, blisters sometimes appear under the nail plates, which peel off, but always recover. Children's growth and development are appropriate for their age.
Severe borderline epidermolysis bullosa
The disease is the most severe form of hereditary pemphigus, leads to the death of the child in the first weeks or months of life, and is inherited in an autosomal recessive manner. Rashes in the form of flaccid, easily eroded blisters immediately become generalized. Characteristic features are the presence of granulations along the edges of erosions, especially pronounced on the face and nail folds, severe general condition of the child, and severe anemia. Often, epidermal detachment occurs without the formation of a bubble. Healing is slow, with skin atrophy. There are always erosions in the oral cavity. Bubbles can also form in the esophagus, larynx, pylorus, small and rectal intestines, gall bladder, urethra, and kidneys. Patients are sharply retarded in physical development. Death occurs as a result of asphyxia from a detached bladder or dermatogenous sepsis.
Dominant dystrophic epidermolysis bullosa
The disease is inherited in an autosomal dominant manner and begins at birth or the first days of life. In the first months, skin damage is generalized, later blisters usually appear on the same frequently injured areas: hands, feet, knees, elbows, neck. Healing occurs with the formation of an atrophic scar with a clear boundary, slight folding of the skin in the scar area, and pigmentation (Fig. 3). The nail plates are affected in all patients, and only in rare cases are the nails absent; more often they are dystrophic. The growth and development of children is not impaired. At an early age, obstruction of the esophagus may occur, which is expressed in choking, vomiting when eating solid food, drooling, and pain when swallowing. These phenomena are reversible. With age, blisters appear less and less often, and in adults the presence of the disease can only be reminded of dystrophic changes in the nails and barely noticeable scars on the elbows, knees and ankles.
Recessive dystrophic epidermolysis bullosa
The disease is inherited in an autosomal recessive manner, has a severe course, and often leads to death at an early age. The disease always occurs from birth or the first hours of life. Already at birth, the skin of the extremities is often eroded. In the first days of life, the rash spreads, and blisters appear not only as a result of minor skin trauma, pressure and friction, but also spontaneously (Fig. 4). Even large erosions heal relatively quickly (depending on the size in 3 - 10 days), but new ones constantly appear (Fig. 5). Healing occurs with the formation of atrophic scars; contractures and syndactyly gradually develop on the hands and feet (Fig. 6,7). Nail plates are absent from birth or are gradually lost as a result of the formation of subungual blisters. Cicatricial atrophy of the skin of the scalp is manifested by diffuse sparseness of hair and its dystrophic changes. Multiple blisters also appear on the mucous membrane of the oral cavity, esophagus, and rectum. The process of scarring in the mouth leads to limited mobility of the tongue, atrophy of its papillae, fusion of the vestibular folds and microstomia, in the esophagus - to its narrowing, impaired passage of food, in the rectum - to chronic constipation, sharp pain during defecation. The teeth are affected in all patients, caries, tooth enamel defects, and location anomalies predominate. Damage to the mucous membrane of the eyes is often observed in childhood, which is clinically manifested by burning and pain when trying to open the eyes. Epithelization of conjunctival erosions occurs quickly (2 - 4 days). Scarring on the cornea ends with the formation of cloud-like opacities that do not significantly impair vision. The general condition of patients is characterized by weakness, fatigue, and long periods of low-grade fever. Constant painful sensations lead to limited mobility of patients, slower psychomotor and physical development, and social maladjustment. Hypochromic anemia is noted. With age, the ability to heal erosive and ulcerative lesions decreases; some lesions do not heal for several months or even years. On such lesions, as well as on scars, epithelial tumors can form, most often squamous cell carcinoma, resistant to therapy. Among the causes of death in the first year of life, the most common are asphyxia, aspiration pneumonia, dermatogenous sepsis, and at the age of over 30 years - malignant skin tumors.
Treatment of hereditary pemphigus
When developing treatment tactics, it should be taken into account that the period of activity of hereditary diseases stretches for many years and it is hardly worth recommending an equally long-term use of even effective drugs. Active therapy is used during exacerbation and the occurrence of complications in short courses, and then is replaced by a longer prescription of restorative and symptomatic drugs. Particular attention is paid to issues of care and nutrition. The main goals of treatment are to prevent the appearance of blisters on the skin and mucous membranes, accelerate the healing of existing rashes, prevent and treat secondary infections, prevent and treat severe complications associated with scarring.
Pathogenetic therapy
It is known that the skin of patients with recessive dystrophic epidermolysis bullosa produces an excessive amount of structurally altered collagenase. In this regard, the use of drugs that inhibit the production or activity of collagenase - diphenin (phenytoin), erythromycin, large doses of vitamin E and retinoids - is pathogenetically justified. Difenin
(used in psychiatry for the treatment of epilepsy) is produced in tablets of 0.1, administered orally twice a day at the rate of 3.5 mg/kg body weight per day in adults and 8 mg/kg in children.
During the first 3 days, 1/3 of the daily dose is prescribed, from the 4th to the 6th day 2/3, from the 7th day - the full dose. If it is necessary to discontinue the drug, reduce its dose in the reverse order. A positive effect in the form of a reduction in the number of blisters, accelerated epithelization of erosions, and increased skin resistance to traumatic influences is noted after 3 - 4 weeks. When treated with diphenin, dizziness, agitation, nausea, vomiting, tremor, lymphadenopathy, and gingival hyperplasia are possible. Erythromycin
is prescribed orally in the usual age-specific dose for 10 to 14 days.
Considering the bacteriostatic effect of the antibiotic, it is better to prescribe it when multiple blistering rashes on the skin are accompanied by secondary infection of erosions. Tocopherol acetate
(vitamin E) is available in capsules of 50 and 100 mg and in an oil solution of 5%, 10% and 30% (50, 100 and 300 mg/ml).
The drug for epidermolysis bullosa gives a positive effect only in doses exceeding 1500 mg per day. Children are prescribed 1/2 - 1/3 of this dose (that is, 500 - 1000 mg per day). The course of treatment is 20 - 40 days. The drug is prescribed in equal parts in the morning and evening during or immediately after meals. For older children who do not have swallowing problems and adults, vitamin E is prescribed in capsules, in other cases - in drops. We have not noted any side effects when using such high doses and have not described them in the literature. From the group of retinoids, tigazone and retinol palmitate
or retinol acetate are used. In addition to the anti-collagenase effect, they have the ability to accelerate epithelization. In this regard, it is better to prescribe them to patients with a significant area of damage, but without secondary infection. Tigazone is available in capsules of 10 and 25 mg, prescribed in a daily dose of 1 mg/kg body weight (in equal parts 3 times a day with meals). If the effect is good (usually on the 3rd - 7th day), after 2 - 3 weeks the daily dose is reduced to 0.3 - 0.5 mg/kg. Long-term use of tigazon is not recommended, since the drug has many side effects: cheilitis, dry skin and mucous membranes, hair loss, biochemical disorders, and in children - growth retardation. Tigazon is embryotoxic and teratogenic and is contraindicated in pregnant women and women planning pregnancy. Before starting treatment, you must make sure that there are no abnormalities in clinical and biochemical blood tests. Retinol palmitate is produced in capsules of 100,000 IU and an oil solution of 100,000 IU/ml, retinol acetate is produced in capsules of 3300, 5000 and 33000 IU and an oil solution of 100,000 and 250,000 IU/ml. Both drugs are used in a daily dose of 5000 IU/kg body weight (equal parts in the morning and evening after meals). Compared to tigazon, the drugs are less toxic, but their positive effect appears at a later date (on the 7th - 10th day). The course of treatment is 1.5 - 2 months. Drugs with anticollagenase activity are not always effective. Most of them are not recommended for long-term use; usually 2-3 courses of treatment are carried out per year. The basis of treatment remains symptomatic therapy.
Symptomatic therapy
General therapy includes the use of broad-spectrum antibiotics for secondary infection of rashes (they are prescribed only when the general condition of the patient is disturbed), antihistamines and sedatives for severe itching, anabolic and restorative agents and enzymes for retarded physical development. In case of anemia, the best effect is obtained by direct blood transfusion, transfusion of red blood cells, plasma, albumin is possible, and an appropriate diet must be prescribed. In complex therapy, it is necessary to prescribe multivitamin preparations. Preference is given to complexes containing microelements. If the oral mucosa is affected, after each meal it is recommended to rinse your mouth with decoctions of chamomile, sage, calendula, St. John's wort, oak bark, and serpentine rhizome. After rinsing, it is good to use sea buckthorn oil, ointment with retinol palmitate, carotoline, solcoseryl, and Kalanchoe juice in the form of applications. Young children are given sea buckthorn oil in drops orally. For spasms of the esophagus with impaired passage of food, bed rest, dry heat on the chest area, antispasmodics, and electrophoresis with peloidin are recommended.
Skin care and external treatment
For constipation, you should not use laxatives that cause chemical or mechanical irritation of intestinal receptors; the best effect is achieved by diet and the introduction of warm vegetable or petroleum jelly into the rectum in the form of a microenema. The use of corticosteroid drugs, either internally or externally, is not recommended. Without preventing the formation of blisters or promoting healing, they enhance the formation of atrophic scars. Preventive vaccinations are contraindicated only during periods when the child’s general condition is impaired. From the first days of a sick child’s life, one should strive to minimize factors that injure the skin. Diapers should be soft, without seams. When swaddling, pay attention to ensure that the baby’s legs do not touch each other. All underwear is worn with the seams facing out. Clothes should not have elastic bands or ribbons that restrict movement. For the same reason, it is undesirable to use diapers. The child is picked up very carefully, only dressed or wrapped in a diaper, supported from below, avoiding stretching the skin. When a child begins to walk, it is advisable to hem his clothes (on his elbows and knees) with several layers of soft fabric. At home, it is recommended to wear loose clothing and no shoes. Walking shoes should be loose and easy to put on. All persons involved in caring for the child and monitoring his health should be warned about the characteristics of the disease and the inadmissibility of even minor trauma to the skin and mucous membranes (for example, during examination by a pediatrician, otolaryngologist or dentist). Blisters form more easily on dry, atrophic skin with reduced sebum secretion. In this regard, the skin needs to be artificially fattened and hydrated daily so that it becomes soft and elastic and is more resistant to mechanical stress. For this purpose, creams and ointments on a water-emulsion basis (ointment with retinol palmitate, ointment Radevit, 5% ointment with urea) or vegetable oil (except sunflower) are used. The cream used should not be thick. Blisters that form on the skin are emptied daily by pricking both sides with a thick injection needle and removing the fluid either by pressing or suctioning with a syringe. It should be remembered that your own epidermis is the best covering for the wound and most contributes to its healing. However, in most cases, repeated mechanical trauma leads to rupture of the exfoliated epidermis, exposing the erosive surface. It is best to immediately apply a collagen sponge covering (colaspon, algicol, digispon, etc.) to the erosions. If there are no coverings at hand, it is necessary to treat the wound with an antiseptic to avoid infection and apply a sterile bandage with wound-healing agents (ointments with retinol palmitate, Radevit, solcoseryl, Actovegin, Bepanten, panthenol aerosol).
Despite precautions, most erosions become infected and turn into ulcers.
(dermazin, levosin, levomekol, fastin)
are applied to infected areas Aerosol external agents are convenient:
olazol, hypozol, legrazol, levovinisol, etc.
Collagen sponge coatings containing enzymes are used to heal ulcers. In case of extensive damage, general UV irradiation at suberythemal doses has a good effect. Magnetic therapy is prescribed for selected long-term non-healing ulcers. Baths with herbs stimulate healing well, improve well-being and are the most pleasant procedure for patients of any age. For baths, any herbal decoctions with anti-inflammatory and astringent effects are used. For severe itching, add mint or valerian. After a bath, be sure to lubricate the skin with a nourishing cream. In many patients, milia form after healing, especially often on the back of the hands. These rashes resolve on their own over time and do not require treatment. Adult patients should be warned about the possible appearance of unusual rashes on scars and ulcers, which requires immediate contact with a dermatologist. Epithelial tumors in epidermolysis bullosa may be resistant to treatment; treatment should be started as early as possible.
Nutrition
At all periods of a patient’s life, nutrition must compensate for the loss of protein, salts and water associated with the formation of blisters. Breastfeeding is preferable; with the introduction of supplementary feeding and complementary feeding, the amount of protein introduced with food should be increased by 20%. Fruit juices and purees should not be sour. In the morning, it is useful to give the child a little unrefined vegetable oil, which compensates for the lack of polyunsaturated fatty acids and facilitates bowel movements. The diet includes foods rich in coarse plant fiber (cabbage, zucchini, beets, dried fruits). Food that injures the mucous membrane is prohibited (caramel, crackers, dryers, waffles, etc.). Adult patients are warned against drinking alcoholic beverages and spicy foods, which provoke the formation of blisters in the esophagus.
For spasms and narrowing of the esophagus, a mechanically and thermally gentle diet is used, increasing the number of meals.
Prof. S.I. Vozdvizhensky (Moscow Research Institute of Pediatrics and Pediatric Surgery) developed a method of surgical treatment of contractures and syndactyly of the hands in children with epidermolysis bullosa. However, there is a danger of relapse, and therefore a long period of anti-relapse therapy is necessary. Sick children can become disabled, adults are able to work or are disabled groups I - III, depending on the form, severity of the disease and complications. Due to the difficulties of treatment, prevention methods are of particular importance. Genetic counseling is possible after an accurate diagnosis has been established. The risk of developing the disease with dominant forms is 50% for each child. If healthy parents have a child with a recessive form of epidermolysis bullosa, then for each subsequent child the risk of developing the disease is 25%. If a patient with a recessive form wants to have a child, then his risk of developing the disease is negligible. The risk becomes greater (50%) if the second parent is a carrier of the identical recessive gene for epidermolysis bullosa. The risk increases significantly with consanguineous marriages. In case of borderline and recessive dystrophic epidermolysis bullosa, prenatal diagnosis is possible by fetal skin biopsy at 16–18 weeks of pregnancy, followed by electron microscopic examination. Such a study can be carried out at the Center for Maternal and Child Health (Moscow) and in a number of foreign countries. If the fetus has a disease, the pregnancy is terminated.
Literature:
1. Bruckner, Tuderman L. Epidermolysis bullosa hereditary. Hautarzt 1995;46:61-72. 2. Albanova V.I. Clinical characteristics of dominant dystrophic epidermolysis bullosa. Bulletin of dermatol. - 1994;1:48-52. 3. Albanova V.I. Epidermolysis bullosa. In the book “Monogenic dermatoses”. — Yoshkar-Ola. - 1993. P. 104-26. 4. Suvorova K.N., Albanova V.I. Hereditary epidermolysis bullosa. In the book “Children's dermatovenerology. - Kazan. 1996. pp. 69-80.
Prevention and prognosis
Medicine has not proposed any specific measures to prevent pemphigus due to the fact that the true causes of its occurrence have not been established. A set of preventive measures is aimed at strengthening the health of a little person:
- formation of strong immunity;
- hardening and walking in the fresh air from the moment of birth;
- proper nutrition;
- avoidance of excessive use of drugs and medications.
Forecasts depend on the speed of contacting a doctor - for symptoms of pemphigus in children, treatment should begin as early as possible. Therefore, you should not self-medicate under any circumstances. In order not to miss the appearance of signs of pathology, it is necessary to examine any skin problems with a dermatologist.
The prognosis of true pemphigus is a priori conditionally unfavorable. Even with adequate and timely treatment, the likelihood of death cannot be eliminated. Any form of pathology is considered chronic.
At the same time, the introduction of hormonal drugs into therapy made it possible to reduce the mortality rate from 65% to 7%. The disease requires constant maintenance therapy. Otherwise, 91% of cases experience acute exacerbations and sudden progression, and consequently an increase in the likelihood of death.
Diagnostics
This pathology is rare, and pediatricians, as a rule, cannot determine it accurately. Therefore, the primary stage of diagnosis is the distinction between pemphigus and other dermatological diseases that are accompanied by rashes of blisters and blisters.
Differential diagnosis is carried out using a special method - Nikolsky's test. The essence of the test is to rub the skin near the bubble and on a distant area of the skin, as well as pressing the fingertip on the bubble. A positive result is considered to be the presence of signs of skin separation:
- spreading of serous fluid into adjacent layers of skin when pressed;
- slight peeling of the skin in the form of a ribbon when you gently pull the skin over the bubble - similar to a sunburn;
- friction on a healthy area shows the mixing of the upper layers of the epidermis.
One of the most informative diagnostic methods is a blood test for the presence of aggressive antibodies to the desmoglein protein. If these antibodies are present, a diagnosis of pemphigus is made.
Additionally, the following may be assigned:
- cytological studies of serous fluid samples from the bottom of the erosion or from the bladder;
- general blood and urine analysis;
- chest x-ray;
- consultations with related doctors - nephrologist, cardiologist, infectious disease specialist.
Treatment
How to treat pemphigus in a child? The main drugs today are hormones from the group of glucosteroids. In this case, systemic therapy is carried out without age restrictions.
Treatment of pemphigus has several main directions:
- preventing the appearance of new blisters and erosions;
- healing of affected areas of the skin.
Glucosteroids are administered in increased dosages. Due to this technique, the intensity of the formation of new foci decreases and the restoration process begins in existing erosions. This process takes about 2 weeks. Subsequently, the patient is transferred to maintenance hormonal therapy. The drug does not change, but the dosage is significantly reduced.
Viral pemphigus in children treatment is aimed at suppressing the virus. Pemphigus vulgaris requires the administration of a larger volume of drugs than foliaceus. The transition to maintenance therapy is carried out gradually. Moreover, the vast majority of patients are forced to take daily injections of maintenance doses of glucosteroid drugs throughout their lives.
Children should take hormonal medications simultaneously with calcium and vitamin D. The effectiveness of treatment increases due to the use of immunosuppressive drugs from the first days of treatment. These drugs have a depressing effect on the activity of the body's immune system.
Early stages of treatment often involve the use of procedures aimed at clearing the blood of aggressive antibodies. Such procedures include hemodialysis and plasmapheresis. The skin must be treated with antiseptics and special ointments to reduce the risk of infection.
Treatment of pathology is daily and lifelong. Sometimes there may be breaks between relapses of the disease.
Baby care
The diagnosis of pemphigus requires special, attentive and daily care for the child. The organization of a baby’s life directly affects his life expectancy. The initial stage of treatment takes place within the walls of the hospital. After discharge, the child should receive all necessary medications in the prescribed volume and time of administration. Parents must learn how to give injections, because the daily services of a hired nurse will negatively affect the family budget.
Every day your child needs to treat blisters and eczema on the skin. Processing is carried out using aniline dyes. This group of agents has the widest spectrum of action on various microbes, including staphylococcus. Erosion and crusts formed are treated with corticosteroid-based ointments.
The presence of infectious signs in the form of pus, inflammation, swelling means the start of using antibiotic ointments. Large affected areas require the use of sterile dressings to help avoid further injury. Dressings are changed at least 2 times a day. For small affected areas, the relevance of bandages is associated with the child’s high motor activity.
The appearance of pain requires taking painkillers and consulting a specialist. The presence of damaged areas in the oral cavity is associated with mandatory rinsing of the mouth with antiseptic agents. A useful and effective means of care is taking baths with antiseptic agents. It is mandatory to take vitamin and mineral complexes consisting of vitamin E, calcium, magnesium and folic acid.
The diet also requires enrichment with vitamins and minerals. Meals are provided on a fractional and frequent basis, at least 6 times a day. This diet plan is especially important when the esophagus and mucous membranes in the mouth are affected. Diet therapy is based on the complete exclusion of salt and increasing the amount of protein. Registration at a dispensary and systematic visits to a dermatologist are required - at least twice a year and urgently in case of relapse. The use of immunosuppressive therapy imposes restrictions on vaccinations.
General notes on therapy
- For superficial forms of pyoderma, the use of topical antiseptics, aniline dyes, and external antibacterial drugs is recommended.
- Systemic antibacterial agents are prescribed for widespread, deep, chronic, recurrent pyoderma, in the absence of effect from external therapy, the presence of general phenomena (fever, malaise) and regional complications (lymphadenitis, lymphangitis), localization of deep pyoderma on the face.
- Glucocorticosteroids for systemic use are prescribed for high activity of the pathological process, for chronic ulcerative-vegetative and gangrenous pyoderma.
- Systemic retinoids are prescribed for keloid acne, abscess folliculitis and scalp perifolliculitis.
- Immunobiological agents are prescribed in cases of recurrent, persistent forms of pyoderma.
- The regimen of a patient with pyoderma involves rational skin care both in the lesion and outside it. In case of a disseminated process, frequent water procedures and hair removal by shaving are not recommended. It is recommended to cut the hair in the area where pyodermic elements are located.
- In case of long-term infectious and inflammatory processes, as well as in case of multiple rashes, certain attention should be paid to diet: nutrition should be complete, rich in vitamins, the amount of salt and carbohydrates is sharply limited, and alcohol is completely excluded.
indications for hospitalization
- diseases associated with the action of toxin-produced strains of staphylococcus and streptococcus;
- widespread rashes accompanied by a violation of the general condition.
requirements for treatment results
- resolution of pathological skin elements;
- epithelization, scarring of ulcers;
- reducing the frequency of disease relapses in chronic forms of pyoderma.
prevention
- Primary prevention of pyoderma consists of timely antiseptic treatment of microtraumas, cracks, and wound surfaces. It is necessary to treat identified common diseases against which pustular skin lesions may develop (diabetes mellitus, diseases of the digestive tract, respiratory system, etc.).
- Secondary prevention of pyoderma includes periodic medical examinations and, if necessary, anti-relapse therapy (general UV irradiation, skin care, sanitation of focal infection).
External therapy
1. Antiseptic preparations for external use:
- solution of brilliant green, alcohol 1% externally to the area of rash 2-3 times a day for 7-14 days, or
- fucorcin, alcohol solution applied externally to the area of rash 2-3 times a day for 7-14 days, or
- methylene blue, aqueous solution 1% externally to the area of rash 2-3 times a day for 7-14 days, or
- potassium permanganate, aqueous solution 0.01-0.1% externally to the area of rash 2-3 times a day for 7-14 days, or
- hydrogen peroxide solution 1-3% externally on the rash area 2-3 times a day for 7-14 days, or
- chlorhexidine, alcohol solution 0.5%, aqueous solution 0.05-1% externally to the area of rash 2-3 times a day for 7-14 days, or
- povidone-iodine, 10% solution applied externally to the area of the rash 2-3 times a day for 7-14 days.
2. Antibacterial drugs for external use:
- neomycin sulfate (5000 IU/5 mg) + bacitracin zinc (250 IU) externally to the area of rash 2-3 times a day for 7-14 days, or
- gentamicin sulfate, ointment or cream 0.1% (d) externally to the area of rash 3-4 times a day for 7-14 days, or
- fusidic acid, cream or ointment 2% externally to the area of rash 3-4 times a day for 7-14 days, or
- mupirocin, 2% ointment applied topically to the area of rash 2-3 times a day for 7-14 days, or
- erythromycin, ointment (10,000 units/g) externally to the area of rash 2-3 times a day for 7-14 days, or
- lincomycin hydrochloride, 2% ointment applied externally to the area of rash 2-3 times a day for 7-14 days, or
- silver sulfathiazole, 1% cream applied externally to the area of rash 1-2 times a day for 7-10 days for 7-14 days.
3. Glucocorticosteroid topical agents combined with antibacterial drugs:
Prescribed in the case of an acute inflammatory process accompanied by erythema, swelling, itching, and more often in the presence of itchy dermatoses complicated by secondary pyoderma:
- tetracycline hydrochloride + triamcinolone acetonide, aerosol applied externally to the area of rash 2-4 times a day for 5-10 days, or
- hydrocortisone acetate + oxytetracycline hydrochloride, ointment, aerosol applied externally to the area of the rash 1-3 times a day for 5-10 days, or
- fusidic acid + betamethasone, cream applied externally to the rash area 2-3 times a day for 7-14 days, or
- fusidic acid + hydrocortisone, cream applied externally to the rash area 3 times a day for 7-14 days, or
- betamethasone valerate + gentamicin sulfate, cream, ointment (B) externally to the area of rash 1-2 times a day for 7-14 days;
- betamethasone dipropionate + gentamicin sulfate, cream, ointment (B) externally to the area of the rash 2 times a day for 7-14 days.
Systemic therapy
1. Antibacterial drugs of the penicillin group:
- benzylpenicillin sodium salt: children - 25,000-50,000 units per kg of body weight per day intramuscularly, adults - 2,000,000-12,000,000 units per day intramuscularly. The drug is administered every 4-6 hours for 7-10 days, or
- amoxicillin trihydrate: children under 2 years of age - 20 mg per kg of body weight per day orally, children aged 2 to 5 years - 125 mg 3 times a day orally, children aged 5 to 10 years - 250 mg 3 times per day orally, for children over 10 years of age and adults - 500 mg 3 times a day orally. The course of treatment is 7-10 days, or
- amoxicillin: children under 3 years of age - 30 mg per kg of body weight per day in 2-3 doses orally, children aged 3 to 10 years - 375 mg 2 times a day orally, children over 10 years of age and adults -500 -750 mg 2 times a day orally. The course of treatment is 7-10 days, or
- amoxicillin trihydrate + clavulanic acid: children aged 3 months to 1 year - 2.5 ml of suspension 3 times a day orally, children aged 1 to 7 years - 5 ml of suspension 3 times a day orally, children aged from 7 to 14 years old - 10 ml of suspension or 5 ml of suspension forte 3 times a day orally, children over 14 years of age and adults - 1 tablet (250 + 125 mg) 3 times a day or 1 tablet (500 + 125 mg) ) 2 times a day orally. The course of treatment is 7-10 days.
2. Antibacterial drugs of the cephalosporin group:
- cephalexin: children weighing less than 40 kg - 25-50 mg per kg body weight per day orally, adults and children over 10 years of age - 250 - 500 mg orally 4 times a day. The course of treatment is 7-14 days, or
- cefazolin: children - 20-40 mg per kg of body weight per day intramuscularly or intravenously, adults - 1 g per day intramuscularly or intravenously. The frequency of administration is 2-4 times a day. The course of treatment is 7-10 days, or
- cefaclor: children under 6 years of age - 30 mg per kg of body weight per day orally in 3 divided doses, children aged 6 to 10 years - 250 mg orally 3 times a day, children over 10 years of age and adults - 500 mg orally 3 times a day. The course of treatment is 7-10 days, or
- cefuroxime: children - 125-250 mg orally 2 times a day, adults - 250-500 mg orally 2 times a day. For parenteral administration: children under 3 months of age - 30 mg per kg of body weight (daily dose) 2-3 times a day, children over 3 months of age - 60 mg per kg of body weight (daily dose) 3-4 times a day , adults - 750 mg-1.5 g 3 times a day. The course of treatment is 7-10 days, or
- cefotaxime: children weighing less than 50 kg - 50-100 mg per kg body weight per day intravenously or intramuscularly with an administration interval of 6-8 hours, children weighing more than 50 kg and adults - 2.0-6.0 g per day day intravenously or intramuscularly with an administration interval of 8-12 hours. The course of treatment is 5-10 days, or
- Ceftriaxone: children under 12 years of age - 50-75 mg per kg of body weight 1 time per day intramuscularly, children over 12 years of age and adults - 1.0-2.0 g 1 time per day intramuscularly. The course of treatment is 7-10 days.
3. Antibacterial drugs of the macrolide group:
- erythromycin: children under 3 months of age - 20-40 mg per kg of body weight per day, children aged from 3 months to 18 years - 30-50 mg per kg of body weight per day, adults - 1.0-4.0 g orally per day in 4 doses. The course of treatment is 5-14 days, or
- azithromycin: children - 10 mg per kg body weight 1 time per day orally for 3 days, adults - 500 mg orally 1 time per day for 3 days, or
- Clarithromycin: children - 7.5 mg per kg body weight per day orally, adults - 500-1000 mg per day orally. The frequency of administration is 2 times a day. The course of treatment is 7-10 days.
4. Antibacterial drugs of the tetracycline group:
doxycycline: for children over 12 years of age and/or with body weight less than 50 kg - 4 mg per kg of body weight once a day on the 1st day, 2 mg per kg of body weight once a day on subsequent days; children over 12 years of age and/or weighing more than 50 kg and adults - 100 mg orally 2 times a day for 10-14 days.
5. Antibacterial drugs of the fluoroquinolone group:
- ciprofloxacin 250-500 mg 2 times a day orally for 5-15 days, or
- Levofloxacin: 250-500 mg orally 1-2 times a day for 7-14 days, or
- ofloxacin: 200-400 mg orally 2 times a day for 7-10 days.
6. Antibacterial drugs of the lincosamide group:
clindamycin: children - 3-6 mg per kg body weight orally 4 times a day, adults 150-450 mg orally 4 times a day; when administered parenterally to children, 15-40 mg per kg of body weight per day, to adults - 600 mg-2.7 g per day, frequency of administration 3-4 times per day. The course of treatment is 10 days.
7. Antibacterial sulfonamide drugs:
sulfamethoxazole + trimethoprim: children aged 3 to 5 years - 240 mg orally 2 times a day; children aged 6 to 12 years - 480 mg orally 2 times a day; adults and children over 12 years of age -960 mg orally 2 times a day. The course of treatment is from 5 to 14 days.
8. Glucocorticosteroid drugs for systemic use (for ulcerative, ulcerative-vegetative pyoderma):
- prednisolone 25-30 mg per day intramuscularly for 5-7 days with a gradual dose reduction until discontinuation, or
- dexamethasone phosphate 4 mg (1 ml) 4-6 mg per day intramuscularly for 5-7 days with a gradual dose reduction until discontinuation, or
- betamethasone disodium phosphate + betamethasone dipropionate 1-2 ml intramuscularly once, if necessary, repeat the administration after 10 days.
9. Systemic retinoids: isotretinoin 0.5-1.0 mg per kg body weight per day orally for 3-4 months.
10. Immunobiological agents:
- purified liquid staphylococcal toxoid in 1 ml 12 ± 2 EU of staphylococcal toxoid: in increasing doses: 0.1,0.3,0.5,0.7,0.9,1.2 and 1.5 ml subcutaneously with an interval of 2 days; per course of treatment - 7 injections. The drug is not used simultaneously with treatment with serum antistaphylococcal drugs (immunoglobulin plasma) or
- staphylococcal medicinal liquid vaccine (staphylococcal antifagin), 1 ml: children aged 6 months to 7 years - 0.1 ml subcutaneously daily; for children over 7 years of age, the initial dose is 0.2 ml subcutaneously, then increase the dose by 0.1 ml daily for 8 days. Repeated course of treatment after 10-15 days in case of extensive skin lesions with relapses, or
- human antistaphylococcal immunoglobulin liquid, 100 IU: for mild forms of pyoderma 100 IU per day intramuscularly, for generalized infection 5 IU per kg of body weight per day intramuscularly, course of treatment - 3-5 injections daily or every other day.
In the treatment of diseases of staphylococcal etiology, accompanied by bacteremia and sepsis, the following is used:
- human anti-staphylococcal immunoglobulin for intravenous administration, 10.25 and 50 ml in bottles, in 1 ml at least 20 IU: for children -5-7 IU per kg of body weight, no more than 25 IU (single dose) intravenously drip at a rate of 8-10 drops per 1 min. The course consists of 10 infusions, which are carried out every 24-72 hours. Adults - 5-7 IU per kg of body weight (single dose) intravenously at a rate of no more than 40 drops per minute. The course consists of 10 infusions, which are carried out every 24-72 hours. The drug is compatible with other drugs or
- - normal human immunoglobulin for intravenous administration, 10, 25 and 50 ml in vials. Children: 3-4 ml per kg of body weight, no more than 25 IU (single dose) intravenously at a rate of 8-10 drops per minute for 3-5 days. Adults: 25-50 ml intravenously at a rate of no more than 40 drops per minute every 1-3 days, the course of treatment is 3-10 infusions. The drug is compatible with other drugs.
Non-drug therapy
UHF therapy - used for deep forms of pyoderma. The course of treatment is 5-10 procedures.