Arbidol is an original antiviral drug for the treatment and prevention of influenza and other acute respiratory viral infections.
- Included by experts of the International Society for Influenza and Other ARVIs in the list of antiviral agents for the treatment of influenza (ISIRV)
- Included in the clinical recommendations of the Ministry of Health of the Russian Federation
- Included in the rubric of the World Health Organization (WHO)
Arbidol blocks the early stage of virus reproduction, preventing the virus from entering the cell by blocking the fusion of viruses with the cell membrane. American scientists from the leading scientific center The Scripps Research Institute, La Jolla, (San Diego, California), which employs several Nobel Prize laureates in the field of natural sciences, have confirmed the “point” of binding of the drug Arbidol with the influenza virus. At the end of December 2021, the authoritative international journal PNAS (the second most cited specialized publication in the world) published an article on the results of a study on the mechanism of the antiviral action of the Russian drug Arbidol.1 It was previously demonstrated that the target of action of the original Russian antiviral drug Arbidol is the surface protein of the virus influenza HA (hemagglutinin).2
Arbidol is an original development of Russian scientists with international recognition. The following countries took part in the study of the drug: Russia, USA, Great Britain, Australia, Japan, China, Turkey, Ukraine, Belgium, Czech Republic, France, Italy, Spain, Italy, India, etc. Scientific interest in the umifenovir molecule is growing!
Clinical studies on the drug Arbidol in the treatment of influenza and other acute respiratory viral infections in adults and children, as well as in the treatment of acute intestinal infections of viral etiology in children, included a total of over 23,000 patients,
including more than
6,500 children
.
Leading scientific institutes and medical institutions of Russia took part in the research of the drug Arbidol:
- — Research Institute of Epidemiology and Microbiology named after Pasteur;
- — Research Institute of Virology named after D.I. Ivanovsky;
- — Research Institute of Influenza of the Ministry of Health of the Russian Federation;
- — Research Institute of Epidemiology and Microbiology named after N. F. Gamaleya;
- — Russian National Research Medical University named after N. I. Pirogov;
- — Moscow Research Institute of Epidemiology and Microbiology named after G. N. Gabrichevsky.
The special path of Russian medicines
For several years now, Arbidol has remained one of the best-selling antiviral drugs in Russia.
It is even more popular than means to increase potency. If you believe the instructions for the medicine, in 2012 the citizens of our country bought 5 billion rubles worth of packages of it. Its active ingredient, umifenovir, was synthesized by Soviet pharmacologists from the All-Union Scientific Research Chemical and Pharmaceutical Institute named after. Sergo Ordzhonikidze (now JSC TsKhLS-VNIHFI in Moscow) and several other scientific institutes in 1974. They began selling it as a medicine in 1988. Despite such a venerable age of the drug, its effectiveness was tested only in the USSR and China.
Our country is different from others in many ways. Unfortunately, these meanings are not always positive. In the case of drugs, the fact is that we have little control over which drugs go onto the market. If in the USA the Food and Drug Administration carefully monitors what drugs enter the market, then in our country even experts cannot figure out what rules are used to register drugs. In Russia, unlike other countries, most medications are sold without a prescription. And there are a huge number of drugs whose effectiveness has not been really tested. These drugs include Arbidol.
According to modern rules of drug development, you first need to understand how a molecule of a potential active substance behaves “in a test tube”, with what it reacts and with what it does not. Then you need to test its effect on cell cultures. The next stage is animals. Typically mice and rats are used first, followed by non-human apes such as macaques. Animals are tested to see what maximum dose of a potential drug the body can tolerate, whether it is toxic in small doses, and what side effects it produces.
If a substance passes preclinical trials, clinical trials await it, this time on humans. Healthy volunteers use the potential drug for a period of time to further test it for possible side effects. In addition, the substance is given to hundreds of patients and they see how effectively it copes with the disease compared to a “dummy” placebo. If a potential drug turns out to be effective and safe enough for people, its developers can expect their brainchild to appear in pharmacies. And even after the start of sales of the drug, it continues to be tested in so-called post-marketing studies. People who have taken a new drug can report its effects, both good and bad, to the manufacturer.
In the case of Arbidol, everything happens, essentially, in the reverse order. Although it is the best-selling antiviral drug in the world's largest country, nothing concrete is known about the effectiveness of this drug. On the main page of the website dedicated to Arbidol, it is written in large letters: “The World Health Organization has included Arbidol in the list of drugs that have a direct antiviral effect.”
Under this inscription there is a link to the WHO website, where it supposedly says so. In fact, it turns out that the meaning of the WHO’s action was somewhat different. Umifenovir was assigned a separate code in the international drug classification ATX. This system exists to make it easier to collect information about the use of various drugs. Just because a substance has the code ATX does not mean it has been proven to be effective or safe. In essence, listing a drug in ATX is an acknowledgment that it exists and is used, nothing more.
Well, a search for articles on clinical trials of umifenovir in the largest database of scientific articles on medicine PubMed produces unintelligible results. In fact, in less than 30 years of sales of Arbidol, it was “checked for lice” only twice, and once in China. An article about this was published in Chinese. The second study is currently being conducted in Russia, and its final results are not yet known. About him - a little lower.
But in the last two years, several publications by foreign scientists have appeared, which finally reveal the potential mechanism of action of umifenovir. Generally speaking, it was necessary to start with such research, and not somewhere overseas, but here, because our compatriots developed this drug.
The use of a domestic antiviral drug from the perspective of evidence-based medicine
Perhaps none of the domestic drugs has recently been subjected to such targeted criticism, which appealed to the evidence base for its use in influenza. Many special medical problems began to be discussed in the media. Therefore, it seems advisable to professionally and impartially understand the essence of the problem.
First of all, it is necessary to recall the basics of general and clinical pharmacology, according to which a drug can influence the etiological, pathogenetic and symptomatic components of the disease. Therefore, it is advisable to consider the use of Arbidol for influenza from these positions, adding to them an analysis of the quality of previously conducted clinical studies from the standpoint of evidence-based medicine and an assessment of not only the effectiveness, but also the safety of the drug.
Impact on the etiology of the disease
The causative agent of influenza infection is the influenza virus, which is an enveloped RNA-containing virus with a negative genome. Inside the virion there are 8 RNA segments associated with proteins of the polymerase complex and the nucleocapsid protein. The inner side of the lipid membrane of the virus is lined by the main structural membrane protein M1, and the M2 protein that forms ion channels is immersed in it. Externally, two surface glycoproteins of the influenza virus are immersed in the lipid membrane of the virus - hemagglutinin (HA) and the viral enzyme neuraminidase (NA), which determine the extraordinary variability of the influenza virus [1].
In the reproductive cycle of the influenza virus, which lasts for 6–8 hours in the cells of the upper and lower respiratory tract, early and late stages are distinguished. In the early stages, adsorption of the virus on the cell surface and penetration of the virus into the cell occurs. After HA binds to cellular receptors, the virus enters endosomes, where the lipid membrane of the virus merges with the endosome membranes. In endosomes, a low pH value activates ion channels formed by the M2 protein, the operation of which leads to the release of the viral ribonucleoprotein from the M1 protein covering it, the release of the viral genome and the beginning of transcription. The later stages include primary and secondary transcription, translation and assembly of the virion on the cell surface, leading to the formation of mature viral particles and their further release from the cell.
At these stages of viral reproduction, an important role is played by the influenza virus enzyme neuraminidase, which cleaves the neuraminidase component of the sialic acid of the hemagglutinin receptors of the epithelial cells of the respiratory tract, helping to release newly formed viral particles from the cells and infect them with new cells [1]. According to experts from the Food and Drug Administration, USA, only drugs that have a direct direct effect on virus replication can be called antiviral, i.e., the action of these drugs is directed at a specific virus-specific target in the virus reproduction cycle [2, 3]. The target of action of adamantane-type anti-influenza drugs (amantadine and rimantadine) is the M2 protein of the influenza virus [4, 5]. The function of the viral enzyme neuraminidase is blocked by the anti-influenza drugs oseltamivir and zanamivir [1]. The virus-specific target of Arbidol's action in the viral reproduction cycle is the surface protein of the influenza virus NA.
Arbidol, interacting with NA, leads to a change in its spatial structure, resulting in the inability of the virus to penetrate into cells [6–7]. The most important indicator of the direct antiviral effect of a drug is its ability or the ability of its metabolites to suppress virus reproduction in cells, which is numerically expressed as an inhibitory concentration of 50 (IC50 is the concentration of a drug that inhibits virus replication by 50%). It is important to note that the effectiveness of a drug with detected antiviral activity in cell culture is manifested at the body level only if the order of concentrations that cause suppression of viruses in cell culture is achieved in human blood plasma or in places where the virus multiplies (for example, in the case of influenza infections in the cells of the respiratory tract, lung tissues, etc.) [2, 3]. Pharmacokinetic studies have shown that the concentrations of all recognized etiotropic anti-influenza drugs in the blood are comparable to their concentrations necessary to suppress viral reproduction in cell culture.
Analysis of the data presented in the table allows us to make an unambiguous conclusion that Arbidol meets all standard international requirements for antiviral drugs. It should be especially noted that these data were obtained in various domestic and foreign research centers.
The effect of Arbidol and other drugs for the treatment of influenza on the immune system
Arbidol has an immunomodulatory effect, leading to an increase in the total number of T-lymphocytes and T-helper cells. Normalization of these indicators was observed in patients with an initially reduced number of CD3 and CD4 cells, and in individuals with normal functioning of cellular immunity there were practically no changes in the number of T lymphocytes and T helper cells. At the same time, the use of Arbidol does not lead to a significant decrease in the absolute number of T-suppressor lymphocytes - thus, the stimulating activity of the drug is not associated with inhibition of the function of suppressor cells. In experiments in vitro and in vivo, Arbidol has an activating effect on the phagocytic function of peritoneal macrophages. Thus, the drug increases the phagocytic number (PF) by 123%, the phagocytic index (PI) by 221% and macrophage activity (MPA) by 176%.
This effect is one of the most important mechanisms of the body's defense against infection. It is assumed that the activating stimuli for phagocytic cells were cytokines and, in particular, interferon, the production of which is enhanced under the influence of the drug. The content of natural killer cells, NK cells, also increases, which allows the drug to be characterized as an inducer of natural killer cell activity. Thus, the presence of immunomodulatory activity in Arbidol in relation to various parts of the immune system prevents the occurrence of secondary infections and the development of exacerbations of chronic diseases in patients [60–63].
Oseltamivir and zanamivir do not have immunomodulatory properties. Oseltamivir does not affect the formation of anti-influenza antibodies, including the production of antibodies in response to the administration of an inactivated influenza vaccine. There is evidence that treatment with oseltamivir can significantly reduce the levels of interleukin 6 (IL-6) and TNF-alpha, markers of the inflammatory response to an infectious disease, compared to placebo [64–65].
Ingavirin has a modulating effect on the functional activity of the interferon system: it causes an increase in the interferon content in the blood to the physiological norm, stimulates and normalizes the reduced alpha-interferon-producing ability of blood leukocytes, stimulates the gamma-interferon-producing ability of leukocytes. Causes the generation of cytotoxic lymphocytes and increases the content of NK cells. The anti-inflammatory effect is due to the suppression of the production of key pro-inflammatory cytokines and a decrease in the activity of myeloperoxidase [56].
Impact on the risk of developing the disease and its complications, as well as its clinical symptoms
IN
And
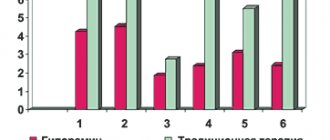
data are presented on the effect of Arbidol and other antiviral drugs on the risk of development and course of ARVI and influenza, as well as their complications in different age groups.
As can be seen from
and, Arbidol is not inferior in its preventive and therapeutic effectiveness to existing antiviral drugs, and often surpasses them.
Clinical studies on Arbidol from the perspective of evidence-based medicine
Currently, there are several levels of research evidence, which are designated by numbers (from 3 to 5–7), and the lower it is, the greater the reliability of the research data. The studies themselves can be divided into three categories according to the level of evidence (maximum category I):
- Category I - this includes well-designed, large, randomized, controlled studies, meta-analysis or systematic reviews;
- Category II - this includes cohort studies and case-control studies;
- Category III - this includes uncontrolled studies and expert consensus.
Practical recommendations for diagnosis and treatment are based both on research results and on extrapolation of these data. Taking this into account, recommendations are divided into several levels, which are usually designated by Latin letters - A, B, C, D, E ().
Level A recommendations are based on the results of studies classified as category I evidence and, therefore, have the highest level of reliability. The reliability of level B recommendations is also quite high - when formulating them, materials from category II studies or extrapolations from studies of category I evidence are used. Level C recommendations are based on uncontrolled studies and expert consensus (category III evidence) or contain extrapolations from category I and II recommendations.
The quality of research publications themselves is currently recommended to be assessed using the Jadad questionnaire, in which the maximum score is 5 points.
It is obvious that for an antiviral drug used for influenza, it is necessary to distinguish two groups of clinical studies assessing its preventive and therapeutic effectiveness.
Research on the preventive effectiveness of Arbidol
Currently, there are 18 domestic publications on the preventive effectiveness of Arbidol during an influenza epidemic. We selected three official reports on clinical trials of the drug for analysis, since it was these studies that became the legal basis for the subsequent use and further study of the drug.
- Clinical study of the preventive effectiveness of the anti-influenza drug Arbidol (Appendix 1). This study is described as a randomized study using identical placebo - +2 points on the Jadad questionnaire.
- Study of the preventive effectiveness of Arbidol during the 1988 influenza epidemic (Appendix 2). This study is described as randomized, double-blind, using identical placebo and indicating the number of patient dropouts from the study groups - +4 points on the Jadad questionnaire.
- Clinical trial in adults as a prophylactic anti-influenza drug of the new chemotherapy drug Arbidol (Appendix 3). This study is described as randomized (random number tables were used), double-blind, using identical placebo - +4 points on the Jadad questionnaire.
IN
The results of assessing the quality of clinical studies conducted according to the most important formal criteria are presented. As can be seen from them, the number of points scored ranged from 64% to 78% of the maximum possible result (an average of 68%). According to the Jadad questionnaire, the average score of the analyzed studies was 3.3 points out of a maximum possible 5 points. Thus, the analysis allows us to make an unambiguous conclusion that, according to most of the evaluated criteria for a high-quality clinical study, work on the preventive activity of Arbidol is at a level significantly above average. It is noteworthy that 2 out of 3 studies on the Jadad questionnaire scored almost the maximum number of points.
The studies themselves on the preventive effectiveness of Arbidol belong to category I studies with a level not lower than 1b.
Research on the therapeutic effectiveness of Arbidol
Currently, there are 17 domestic and 3 foreign publications on the therapeutic effectiveness of Arbidol for ARVI and influenza. We selected 2 publications about a clinical trial of a drug for influenza for the study.
- Efficacy and safety of using the drug Arbidol for influenza (Appendix 4). This study is described as randomized (random number tables were used), double-blind - +3 points on the Jadad questionnaire.
- Multi-purpose, randomized, double-blind, parallel clinical trial of the therapeutic efficacy of the drug Arbidol (Appendix 5). This study is described as randomized (random number tables were used), double-blind - +3 points on the Jadad questionnaire.
IN
The results of assessing the quality of clinical studies conducted according to the most important formal criteria are presented. As can be seen from them, the number of points scored ranged from 71% to 78% of the maximum possible result (an average of 5%). According to the Jadad questionnaire, the average score of the analyzed studies was 3 points out of a maximum possible 5 points. Thus, the analysis allows us to make an unambiguous conclusion that, according to most of the evaluated criteria for a high-quality clinical study, work on the therapeutic effectiveness of Arbidol is also at a level significantly above average.
The studies themselves on the therapeutic effectiveness of Arbidol belong to category I studies with a level not lower than 1b.
Safety of prevention and therapy with Arbidol
One of the most important criteria for the widespread use of a drug in the population is not only its preventive and therapeutic effectiveness, but also the safety of use.
To the studies analyzed above, it is necessary to add the results of two more double-blind studies of Arbidol performed in China (Appendix 4 and 5).
As can be seen from the presented data, Arbidol has a minimal number of side effects, which increases patient adherence to therapy, and makes it possible for doctors to prescribe the drug to the population.
The discussion of the results
The widespread use in Russia and inclusion in the list of vital drugs of the original domestic etiotropic antiviral drug Arbidol, intended for the treatment and prevention of influenza A and B, as well as other acute respiratory viral infections, is based on convincing data that meets the requirements of evidence-based medicine. The antiviral activity and mechanism of virus-specific action of Arbidol have been convincingly proven in numerous preclinical studies performed not only in leading scientific centers in Russia, but also in the USA, Great Britain, Australia, France, China and other countries. More than 12,400 and 1,400 individuals, respectively, participated in clinical studies on the preventive and therapeutic effectiveness of Arbidol.
An analysis of publications on the use of Arbidol allows us to conclude that the drug is currently well studied, has a reasonably high degree of evidence of use, and in the future there is no need to prove the previously proven high effectiveness and safety of use.
Literature
- Laver WG, Bischofberger N., Webster RG Disarming Flu Viruses // Scientific American. 1999. V. 280. P. 78–87.
- FDA. Antiviral Drug Advisory Committee. Gaithersburg: Center for Drug Evaluation and Research. 2002. P. 1–266.
- Hayden F. WHO Guidelines on the Use of Vaccines and Antivirals during Influenza. Annex 5-Considerations for the Use of Antivirals during an Influenza pandemic, Geneva, 2–4 October, 2002.
- Hay A. Amantadine and Rimantadine-Mechanisms. In book: Antiviral Drug Resistance, D. Richman (ed), John Willey and Sons Ltd, UK (1996), 44–58.
- Belshe, Burk B., Newman F. et al. Drug resistance and mechanism of action amantadine on influenza A viruses // J. Inf. Dis. 1989. 159. 430–435.
- Boriskin Y., Leneva I., Pecheur E. et al. Arbidol: a broad-spectrum antiviral compound that bloks viral fusion // Current Med. Chem. 2008. Vol. 15. P. 997–1005 (Review Invited, English).
- Leneva IA, Russell RJ, Boriskin YS et al. Characteristics of arbidol-resistant mutants of influenza virus: implications for the mechanism of anti-influenza action of arbidol // Antiviral Res. 2009. Vol. 81. R. 132–140.
- Leneva I. A., Fedyakina I. T., Guskova T. A., Glushkov R. G. Sensitivity of various strains of influenza virus to arbidol. Study of the effect of arbidol on the reproduction of influenza A virus in combination with various antiviral drugs // Therapeutic archive. 2005, No. 8.P.84–88
- Fedyakina I. T., Leneva I. A., Yamnikova S. S. et al. Sensitivity of influenza A/H5 viruses isolated from wild birds in Russia to arbidol in MDCK cell culture // Questions of Virology. 2005. No. 6. P. 22–25
- Burtseva E., Shevchenko E., Belyakova N. et al. Monitoring the sensitivity of epidemic strains of influenza viruses isolated in Russia to etiotropic drugs // Questions of Virology. 2009. 54 (5): 24–87.
- Burtseva E. I., Shevchenko E. S., Leneva I. A. et al. Sensitivity to rimantadine and Arbidol of influenza viruses that caused epidemic increases in incidence in Russia in the 2004–2005 season // Questions of Virology. 2007. No. 2. pp. 24–29.
- Lvov D.K., Burtseva E.I., Prilipov A.G. et al. Isolation on May 24, 2009 and depositing in the State Collection of Viruses (GKV N 2452 dated May 24, 2009) of the first strain A/Moscow/01/2009 (H1N1 ) swl, similar to swine virus A (H1 N1) from the first patient identified on May 21, 2009 in Moscow // Questions of Virology. 2009. T. 54, No. 6. P. 10–14.
- Romanovskaya A. A., Durymanov A. M., Sharshov K. A. et al. Study of the sensitivity of influenza A (H1N1) viruses that caused illness in April-May 2009 to antiviral drugs in MDCK cell culture // Antibiotics and Chemotherapy . 2009. T. 54, No. 5–6. pp. 41–47.
- Shi L., Xiong H., He J. et al. Antiviral activity of arbidol against influenza A virus, respiratory syncytial virus, rhinovirus, coxsackie virus and adenovirus in vitro and in vivo // Arch. Virol. 2007. Vol. 152. P. 1447.
- Leneva I. A., Fedyakina I. T., Eropkin M. Yu., Gudova N. V., Romanovskaya A. A., Danilenko D. M., Vinogradova S. M., Lepeshkin A. Yu., Shestopalov A. M. Study of the antiviral activity of domestic anti-influenza chemotherapy drugs in cell culture and in animal models // Questions of Virology. 2010.
For the rest of the bibliography, please contact the editor.
V. I. Petrov *, Doctor of Medical Sciences, Professor, Academician of the Russian Academy of Medical Sciences S. V. Nedogoda *, Doctor of Medical Sciences, Professor I. A. Leneva **, Doctor of Biological Sciences
*Volgograd Medical University , Volgograd **TsKhLS VNIHFI , Moscow
Contact information for authors for correspondence
Appendix 4
Efficacy and safety of arbidol in the treatment of influenza
Wang MZ, Cai BQ, Li LY, Lin JT, Su N., Yu HX, Gao H., Zhao JZ, Liu L.
Efficacy and safety of arbidol in treatment of naturally acquired influenza.
Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2004 Jun; 26(3):289–293.
Objective: to evaluate the effectiveness and safety of arbidol hydrochloride in the treatment of influenza virus.
Methods: Conducting a double-blind, parallel clinical trial. Registration of participants.
Inclusion criteria: age - from 18 to 65 years, with flu symptoms, presented in the first 36 hours from the onset of the disease, with a temperature of 37.8 degrees or higher; epidemic rise in the incidence of influenza. The subjects were randomly divided into 2 groups, one group was prescribed Arbidol (200 mg 3 times a day for 5 days), the other group was prescribed placebo.
Results: The study included 232 subjects who were prescribed appropriate treatment and followed up. All subjects voluntarily took part in the drug study (113 people in the Arbidol group; 109 people in the placebo group). For various reasons, 22 subjects (9.3%) were unable to continue participation in the study. 210 subjects completed the study and were designated the RR group (102 people in the Arbidol group and 108 people in the placebo group).
Laboratory-confirmed influenza was present in 125 subjects who were assigned to the PPi group (59 people in the Arbidol group and 66 people in the placebo group). In the PPi group, general improvement in the condition of patients taking Arbidol occurred faster than in the placebo group. The average duration of illness in patients taking Arbidol was 72 hours (95% confidence interval 66.00–78.00 hours), and in the placebo group - 96 hours (95% confidence interval 87.46–104 ,54 hours). The average area under the curve of the severity of influenza symptoms versus the time of illness was significantly greater in the Arbidol group than in the placebo group. The mean area under the curve (symptom severity/time) was 780.00 and 684.00, respectively. Side effects were similar in both the Arbidol group and the placebo group. The main side effects are gastrointestinal upset and increased transaminases.
Conclusion: Arbidol is an effective and safe drug for the treatment of influenza at an early stage of the disease.
Appendix 5
Multicenter randomized, double-blind, parallel clinical trial of the therapeutic efficacy of arbidol hydrochloride tablets
LIU Hong-bo, QU Wen-xiu, LI Sheng-qi.
Multicenter randomized double blind parallel clinical trial of arbidol hydrochloride tablet.
The Chinese Journal of Clinical Pharmacology, 2006, 06.
Objective: to study the effectiveness and safety of arbidol hydrochloride tablets in the treatment of influenza.
methods : A double-blind parallel clinical study was conducted. The subjects were randomly divided into 2 groups: experimental (108 cases of disease) and control (105 cases), the patients of which took Arbidol or ribavirin tablets, 200 mg 3 times a day for 6 days.
Results : the clinical efficacy rate in the groups using Arbidol and ribovirin was 91.67% and 84.47%, respectively (PP analysis results, P > 0.05), and the recovery rate was 82.41% and 74.76% respectively. The percentage of adverse events was 7.62% and 5.71% in the experimental and control groups. The results of both groups were not significantly different (P > 0.05).
Conclusion: Arbidol is an effective and easily tolerated drug for the treatment of influenza at an early stage of the disease.
Lost Resolution
Not long ago, Russian-language media and social networks were making noise about the Memorandum on the pseudoscience of homeopathy, which was developed by the Commission for Combating Pseudoscience and Falsification of Scientific Research under the Presidium of the Russian Academy of Sciences. Its authors ask the Ministry of Health to “reconsider, in the light of current scientific data, decisions taken more than 20 years ago without sufficient grounds to introduce homeopathy into the Russian healthcare system” and “to withdraw homeopathic medicines from medical use in state and municipal medical institutions.” Facebook disputes revealed many hidden lovers of homeopathy and quarreled many good friends.
However, few people remember that ten years ago, in March 2007, a similar document was drawn up at the Academy of Medical Sciences (RAMS). The resolution of the meeting of the Presidium of the Formulary Committee of the Russian Academy of Medical Sciences dated March 16, 2007 stated: “The Formulary Committee of the Russian Academy of Medical Sciences, supporting the need for emergency measures taken by the Government of the Russian Federation to normalize the situation with drug supply to the population of the country, and realizing its involvement in the problem of drug supply, proposes:
“Take Arbidol and stay at home”: Pharmacists were optimized, and then there’s an epidemic
Many things have not passed the coronavirus test in Russia. Adequacy of officials. Social orientation of business. Optimized medicine. It turned out that the cheerful reports about “breakthroughs” and “optimization” are a fool’s errand: there is a shortage of protective equipment, equipment, specialists and hospital beds. But the country began to gradually cope with all this force majeure - primarily due to the heroism of doctors, and also because they did not have time to fully optimize medicine and while the state has somewhere to direct its resources to urgently mobilize the country’s medical capabilities. That is, to the question “how to treat?” answers are sought and found. But with the answer to the question “how to treat?” everything is much worse. Effective managers optimized pharmaceuticals much more effectively.
Russian panacea or dummy?
“Take Arbidol and don’t go anywhere,” was the recommendation heard from doctors by many of those who came to see us in the last month due to signs of a cold and fears that they had “caught corona.” What else could the doctors say?
For many years, if not decades, we have had the same answer to all acute respiratory viral infections and acute respiratory infections. It was announced back in March by the Moscow Department of Health, in a manual with recommendations for the treatment and prevention of coronavirus infection COVID-19.
The document notes that for the drug prevention of COVID-19 in adults, intranasal administration of recombinant interferon alpha-2b is possible. Among the immunotropic drugs that have an antiviral effect, anaferon, ergoferon, and kagocel are recommended.
Well, our main fighter against the virus was and remains “His Majesty Arbidol.”
At the same time, for a decade now we have been in full swing about the fact that this drug is useless, but it is being lobbied at the highest level so that the manufacturer receives government orders. Numerous rumors have long been circulating in the media and in the “expert community” about the alleged personal involvement of the former Minister of Health and Social Development (and now Deputy Prime Minister) Tatyana Golikova in the promotion of Arbidol: it was alleged that Tatyana Golikova and her husband, former Deputy Prime Minister Viktor Khristenko, allegedly would have some relation to the manufacturing company. Evil journalists even gave Golikova the unkind nickname “Madame Arbidol.”
Sales of Tamiflu in 2009 increased by... 1000%! Over the nine months of the year, Russians bought $6.1 million worth of imported medicine. Photo: Alexey Smyshlyaev/Shutterstock
It’s worth dotting all the i’s. No, this is not a “dummy”, not homeopathy. This is a drug developed almost half a century ago at the Moscow All-Union Scientific Research Chemical and Pharmaceutical Institute named after. Sergo Ordzhonikidze (now JSC TsKhLS-VNIHFI) and at the Obninsk Research Institute of Medical Radiology of the USSR Academy of Medical Sciences (now the Medical Radiological Research Center of the Russian Academy of Medical Sciences).
In 1974, the creators of the drug received copyright certificate No. 1685933, in which the chemical compound “1-methyl-2-phenylthiomethyl-3-carbethoxy-4-dimethylaminomethyl-5-hydroxy-6-bromoindole hydrochloride” was named “arbidol”. The drug inhibits the hemagglutinin protein, which determines the ability of viruses to attach to the donor cell.
Few people pay attention to what the instructions say about the effectiveness of the drug in vitro, that is, in laboratory conditions. But its effectiveness in vivo, on living beings, has not been proven.
So many copies have already been broken around the effectiveness of arbidol that trying to outline the history of the discussion is a hopeless task. One fact is important: arbidol was made in our country as drug No. 1, has powerful government support and at the same time very aggressive marketing from, and now OTCPharm, - this is a product that the company promotes in every possible way. Based, among other things, on the experience of foreign colleagues.
The epidemic opens wallets
In 2009, the world was frightened by swine flu. WHO declared a pandemic threat, raising it to the maximum level 6. Previously, a threat of this magnitude was declared in 1968, when humanity was engulfed by the Hong Kong strain of influenza. But then about a million people died, and about 150 thousand died from pork.
European media have accused the World Health Organization of exaggerating the danger of swine flu. Scientists and journalists suspected the organization's leading experts of acting in the interests of pharmaceutical companies.
Intentionally or not, but then, indeed, it was heard from all angles that the only effective drugs for swine flu were the manufactured Tamiflu and British Relenza.
The commercial effect was immediate: Tamiflu sales grew from $600 million in 2008 to $2.6 billion in 2009. More than four times the growth. Governments have allocated billions of dollars to purchase antiviral drugs.
This also affected Russia. Sales of Tamiflu in 2009 increased by... 1000%! Over the nine months of the year, Russians bought $6.1 million worth of imported medicine. In October alone, when the seasonal and swine flu epidemic began in almost all regions of Russia, pharmacies sold $3 million worth of Tamiflu. Maybe they would have sold more, but many people couldn’t afford the foreign drug.
Manufacturers and lobbyists of arbidol also “saw the moment.” During the 2009-2010 swine flu season, government officials, in particular Tatyana Golikova (then head of the Ministry of Health and Social Development) and Gennady Onishchenko (former chief sanitary doctor of the Russian Federation), personally monitored the availability of the drug in pharmacies.
At the end of 2009, Arbidol was included by the Russian government in the state list of vital drugs (first as an immunostimulant, then as an antiviral drug).
As a result, arbidol showed a 120% increase in sales against swine flu.
10 years have passed, and now there is a new problem - COVID-19. And here the marketing of arbidol went on the attack ahead of the curve.
Already at the end of January, radio advertising positioned arbidol as a remedy against coronavirus. Posts began to appear on social networks saying that Chinese tourists were sweeping the drug off pharmacy shelves. Later, a video about Italians who admired the drug purchased at the airport gained fame.
The media also actively circulated the news that China had officially recognized arbidol as a medicine against the new coronavirus. This was allegedly stated by the Chinese Ambassador to Russia Zhang Hanhui. But later it turned out that the diplomat was misunderstood. He only meant that the drug was one of 30 drugs that were tested for effectiveness against coronavirus.
The Federal Antimonopoly Service became interested in the situation, and on March 16, it made a decision to recognize the advertising of Arbidol as improper, violating Part 6 of Article 24 of the Federal Law “On Advertising.” However, FAS could not call the advertisement unreliable.
Probably, they have not yet seen the publications of Chinese doctors who stated that testing arbidol (as well as other drugs) on patients with corona did not give any outstanding results.
But all these “showdowns” are no longer interesting at all. The result has been achieved: with the beginning of the coronavirus epidemic in Russia, sales of arbidol from February 1 to February 20 jumped by 11% compared to the same period last year. In Moscow alone, sales increased by 31%. Since January 26, sales have increased per day by more than a third.
According to the research company DSM Group, at the end of March, the top 3 brands by value of pharmacy sales in Russia consisted of such drugs as Miramistin (it was swept away to wipe hands and everything else), Arbidol and Ingavirin. At the same time, in terms of growth in rubles, Arbidol became the undisputed leader - 389% growth. Arbidol is given to patients in clinics and prescribed to those who are sick at home.
Impocel and other pherons
As for the above-mentioned kagocel, interferon and other immunomodulators, their effectiveness is even more questionable.
According to Alexander Hadjidis, chief clinical pharmacologist of St. Petersburg, we do not have immunomodulatory drugs for the treatment of ARVI with proven effectiveness, as in the rest of the world.
In an interview with the Internet portal “Doctor Peter”, he recalled that some immunostimulating drugs “for the treatment of ARVI” until recently had a completely different purpose. Thus, Kagocel (international nonproprietary name, INN, gossypol) was used for a long time as a contraceptive drug, causing a disorder of spermatogenesis, and then suddenly became an immunomodulator. In the late 1990s, a WHO study group on methods of regulating male fertility concluded that the risks of its use outweighed the benefits and its use in its pure form as a contraceptive was prohibited. Simply put, the use of gossypol, and now kagocel, led to male infertility.
Ingavirin, which the Ministry of Health recommended for the treatment of influenza, experienced approximately the same metamorphosis. Its active ingredient is called vitaglutam (pentanedioic acid imidazolylethanamide). As Alexander Hadjidis said, the drug “Dicarbamin” was first created on its basis; it was used in chemotherapy regimens for cancer patients to stimulate hematopoiesis. In 2014, it was excluded from the register of medicines of the Russian Federation at the request of the manufacturer. But there remained another drug with the same active ingredient - Ingavirin, registered in 2008 as an antiviral drug for the treatment and prevention of influenza and ARVI. In scientific journals you can find a description: “The pharmacokinetics of the drug vitaglutam in humans has not been studied. The instructions for use provide only data obtained in experiments on animals using a radioactive label, from which it is impossible to reliably judge the pharmacokinetics of the drug in the human body. Due to insufficient information about the safety of the drug, its use should be considered with great caution, especially in patients at high risk of developing complications of influenza.”
As Hadjidis noted, the only officially confirmed domestic antiviral drug, Soviet remantadine, has long lost its effectiveness: viruses have become insensitive to it.
Generics instead of innovations
Estimates of what is going on in our pharmaceutical industry and science vary greatly. On the one hand, one cannot help but admit that after the total collapse that occurred in the 1990s, the industry has partially revived. The largest international pharmaceutical companies, domestic enterprises and research centers operate in Russia. Moreover, pharmacy is one of the most dynamically developing sectors of the economy.
But the direction in which pharmaceuticals is developing is causing great concern.
As, for example, Ekaterina Nezhnikova and Maxim Maksimchuk, researchers at the Russian Peoples' Friendship University, noted last year, in recent years the pharmaceutical industry has continued to reorient production toward generics.
Let us remind you that generics are medicines that are identical to the original ones in composition and therapeutic properties, but do not have patent protection and the name of the original drug.
Their production has its advantages - they are cheaper than the originals and, therefore, more accessible to people. Although at the same time, patients with average and high incomes usually do not trust such “replicas”.
One of the main disadvantages is that this vector of industry development kills innovation. Companies produce ready-made drugs without investing in the development of new drugs, their clinical trials, or licensing fees, as a result of which the innovative activity of enterprises decreases. As noted, the problem is aggravated by the difficulty of obtaining funding for the development of new drugs: the main source of funding for innovation in Russian industry is the own funds of pharmacologists.
“Instead of generating scientific knowledge and forming business ideas based on it, companies reproduce “foreign” medicines,” the scientists state.
Among other problems, experts noted the high share of counterfeit products on the market (up to 10%), the promotion of biologically active additives (BAA) under the guise of medicines by unscrupulous participants in the pharmaceutical market, dependence on imported substances and the inability to meet market needs due to the lack of competitiveness of domestic pharmaceutical companies.
There are hopes of getting something really effective from Russian pharmaceuticals, something of our own, domestic. Photo: Andrey Nikerichev / AGN “Moscow”
By the way, regarding imports. Our medicines are still mostly imported from abroad. Import substitution has actually failed. In January of this year, proposals from the Ministry of Industry and Trade to change plans in this area became known. The ministry proposed reducing the share of domestic medical products on the Russian market: in 2021 from 40% to 25%, and in 2024 from 45% to 30%. It is also proposed this year to reduce the target for the share of domestic drugs from 50% to 32.9% in monetary terms.
In the state program “Development of the Medical and Pharmaceutical Industry” of 2014, prepared by the Ministry of Industry and Trade, it was planned to increase the share of domestic drugs in consumption to 50% by 2021. This would allow us to say that the Russian drug market is mature, does not depend heavily on imports, and the domestic drugs that circulate on it are comparable to imported ones in terms of safety and effectiveness profile.
However, the goals were not achieved. Over the nine months of 2021, the share of Russian medicines on the market was 30.5% in monetary terms instead of the target 46%, and of medical products – 22.74% instead of the target 36%.
At the same time, domestic manufacturers are increasing sales of drugs abroad. In the first nine months of 2021, sales of Russian medicines abroad amounted to 400 million packages, or 20 billion rubles, which in monetary terms is 23.5 % more than the same figure for the previous year. They sell mainly to neighboring countries and third countries - for example, to Nigeria.
As explained, the pharmaceutical market is growing on government orders, but the money is spent on imported drugs that have no analogues in Russia.
In February, the Accounts Chamber noted the lowest level of execution of budget expenditures in 10 years. The most failed program was the “Development of the Pharmaceutical and Medical Industry for 2013-2020” (62.9 percent completed).
This program was soon closed ahead of schedule, and plans began to be made until 2030. And the problems are only multiplying.
According to Doctor of Pharmaceutical Sciences Tatyana Orlovskaya and a number of other experts, the main problem of the industry is personnel. Pharma 2020 was aimed at creating new drug manufacturers, but this requires qualified specialists, but they are not there. Yes, there are specialized universities and faculties, but the level of their graduates is that of a pharmacist in a pharmacy. During the implementation of Pharma 2020, no attention was paid to this. There were plans to develop our own medicines, but the standards in the pharmacy specialty remained the same, focused primarily on banal sales.
According to Orlovskaya, the “total destruction of pharmaceutical education” is certainly beneficial to large foreign corporations - Western, Indian, Chinese, which have more than once been caught “working with doctors” in Russia and are most afraid of giving up the enviable Russian market to Russian manufacturers. That is why there are no longer state pharmaceutical universities in Russia - this is unprofitable for the world giants.
What are we left with in the face of an epidemic? With nothing? Or is there still hope that our scientists are able to create real medicines?
The epidemic is like a new chance
Now the whole world is catching news from the United States, where coronavirus patients are being treated with the drug Remdesivir. Developed as a treatment for the Ebola virus, it appears to be effective against COVID-19. Although there is no exact data, there is no definitive understanding of the side effects. But America is in a hurry - they need to turn the situation around with the pandemic, pull the economy out of recession, and re-elect Donald Trump.
Meanwhile, in Russia, as it turns out, despite everything, work is underway on new drugs. Moreover, in the wake of the epidemic, this work has been accelerated.
At the end of April, by decision of the Siberian Branch of the Russian Academy of Sciences, the Center of Competence for Combating Particularly Dangerous Infections was organized within its framework. ().
This will be a specialized center for the creation of innovative medicines covering the full product life cycle - from the laboratory to the industrial stage. The main task is the speedy transfer of the latest anti-infective drugs to the healthcare system.
“Today, the center’s first steps are certainly related to the coronavirus pandemic,” emphasized its director Nariman Salakhutdinov. “But as a stably operating structure, it must be aimed at future threats, at new infections - many of these arise even during the course of one human life, COVID-19 is not the first and not the last. This requires equally stable government funding, and a lot of it: we are not talking about the most low-budget branch of scientific knowledge. We need, for example, large numbers of laboratory animals and extensive chemical libraries - not paper ones, but collections of compounds."
Now the whole world is catching news from the United States, where coronavirus patients are being treated with the drug Remdesivir. Developed as a treatment for the Ebola virus, it appears to be effective against COVID-19. Photo: US Navy/Globallookpress
He also recalled the first promising developments: a complex has already been created to combat the causative agent of infectious hemorrhagic fever with renal syndrome (HFRS), which appeared in the Far East and the Urals. There was no cure for this disease. Permission was also received for clinical trials of a new anti-flu drug, camphecin. It was invented and synthesized in 2017.
And finally, we can recall that on April 28, the Russian Direct Investment Fund (RDIF), the sovereign wealth fund of the Russian Federation, and the group announced the start of a clinical trial of the drug Favipiravir in patients hospitalized with COVID-19. The studies will take place in 17 centers throughout Russia with the participation of 330 patients with confirmed coronavirus infection.
In a word, there is hope to get something really effective from Russian pharmaceuticals, something of our own, domestic.
After all, in any story there is never completely black and completely white. Someone is making millions, someone is trying to cover up the traces of their negligence and many years of work to collapse the domestic healthcare system. Someone is spreading lies and panic.
But at the same time, against the backdrop of the epidemic, it became clear that Russia has something to be proud of. There is something that other countries look at with envy.
Despite everything, we have maintained what is probably the best system of sanitary and epidemiological control in the world.
We have an industry capable, for example, of producing such ventilators, about which an Italian doctor from Bergamo will say in an interview with the British Guardian: “All the equipment here consists of artificial lung ventilation devices (ventilators) supplied by the Russian military. These are devices that are not available in the West. We have evaluated them and used them, they are of the highest quality. They are extremely useful in intensive care.”
We have doctors and nurses who, forgetting everything that was done to them in recent years, will simply do their duty. Those who have been living isolated from their families, loved ones and relatives for weeks or already months. Those who face infection every day, knowing that no one is immune, that tomorrow their test may be positive, and in a week or two they themselves will need a ventilator. They know this and do their job.
Let us believe that science has survived in our country and, in spite of everything, will still surprise both the country and humanity.
Will the ARBITRATOR judge?
Let’s decipher what the words “multicenter, double-blind, placebo-controlled study” mean. By "multiple-double-blind study" it is assumed that no one knows who is being given the real drug - neither patients nor doctors. After all, otherwise everyone will think that the drug being studied will be more effective than the “dummy” drug, but in reality this does not always happen.
So, a clinical trial of the effectiveness of Arbidol with the ambiguous name ARBITR began in 2011. Information about it is even available in the American registry of clinical trials on the website clinicaltrials.gov. True, it has not been updated since 2013. There is more data on the Russian website of the register of medicines. It states that the ARBITRATOR is still ongoing and will only end on June 30, 2017. Accordingly, it will be necessary to wait about another year until the research results are processed and reports and scientific articles are published on them. Then it will be possible to understand whether Arbidol is as effective as the manufacturers write about it.
But, generally speaking, the preliminary results of the ARBITER are already known. They were published in 2015 in the journal Therapeutic Archives. In total, 293 patients with influenza managed to participate in it, but the data from clinical trials was not analyzed for all, but only for 119. Of these, only 45 were confirmed to be infected with the influenza virus by laboratory tests, and for the remaining 74, the conclusion was made based on symptoms. So in their case it might not have been the flu at all, but some abstract ARVI.
The results seem to be quite good: “60 hours after the start of therapy, resolution of all symptoms of laboratory-confirmed influenza was observed in 23.8 percent of patients receiving umifenovir therapy, which was 5.7 times higher than the same figure in the placebo group, which was 4.2% (p<0.05). A significant effect of umifenovir on the rate of elimination of the influenza virus was established, which, in particular, was manifested by a decrease in the number of patients in whom detection of viral RNA persisted for the fourth day or more (25% in the main group versus 53% of patients in the control group; p<0.05 )".
In general, if you take umifenovir, the time of illness seems to decrease. But these are only preliminary results; there should have been at least twice as many subjects. And professional doctors have questions about the research methodology. And the cherry on the cake: most of the authors of ARBITR are employees of companies that produce Arbidol and its analogues. And this gives reason to doubt his impartiality.
How effective is the drug "Arbidol"?
" Arbidol " is the trade name of the drug umifenovir. One of the best-selling medicines in Russia for colds, on the market since 1974. Widely used for viral infections in children and adults.
What is written in the instructions for the drug?
Antiviral agent. It specifically suppresses in vitro ( that is, not in humans, but in a test tube! ) influenza A and B viruses, as well as other viruses that cause acute respiratory viral infections (coronavirus, rhinovirus, adenovirus, respiratory syncytial virus and parainfluenza virus).
Please note - coronavirus is already in the instructions!
How does Arbidol work?
The instructions indicate that Arbidol prevents the fusion of the virus shell with the cell membrane of the body. The drug stimulates the activity of interferon (in a study on mice - after 16 hours), as well as other immune reactions.
It is also written that, according to research, the drug is effective against influenza and ARVI in adult patients in the acute period of the disease. Does not have any negative effects on the human body in recommended doses ( this is very good! ).
When does the manufacturer recommend using Arbidol?
- prevention and treatment of influenza A and B, other acute respiratory viral infections in children over 2 years of age and adults;
- complex therapy of acute intestinal infections of rotavirus etiology in children over 2 years of age ( no serious clinical studies have been published on this recommendation ).
The evidence base for the clinical use of Arbidol is insufficient, despite the instructions for the drug. There are no high-quality studies on the effectiveness of the drug for specific diseases in humans. Therefore, Arbidol is not included in the recommendations of international organizations (in particular, WHO) for the treatment of influenza.
And for other acute respiratory viral infections, antiviral drugs are not used at all in the world.
An attempt to find information on Arbidol in the Cochrane Library (this is basic information on evidence-based medicine) led to a page indicating the article: “Arbidol for preventing and treating influenza in adults and children / Liang Huang, Lingli Zhang, Yantao Liu, Rong Luo, Linan Zeng, Irina Telegina, Vasiliy V Vlassov / Cochrane Systematic Review - Intervention - Protocol Version published: 03 February 2021 /, but on this page it is written that this Article has been withdrawn from the library, without specifying the reasons.
Arbidol is also mentioned in the list of antiviral drugs for the treatment of influenza by the International Society for Influenza and Other ARVI (isirv-AVG), indicating that its clinical effectiveness has not been established .
Are there any serious studies on umifenovir?
In 2012, a multicenter, double-blind, randomized, placebo-controlled trial, ARBITR, funded by the manufacturer, was launched in Russia (registered with the Ministry of Health of the Russian Federation in 2011 under the number RCT No. 375 and on the website clinicaltrials.gov). The study was supposed to be completed in 2015, but the results have not yet been published.
However, an article about this study was published in the journal “Therapeutic Archive” [N.Yu. Pshenichnaya, V.A. Bulgakova, N.I. Lvov et al. / Clinical effectiveness of umifenovir for influenza and ARVI (ARBITR study) // Therapeutic archive. - 2021. - No. 3. - P. 56-63]. The authors report the effectiveness of umifenovir in adult patients with influenza during the acute period of the disease in the form of a reduction in the duration of all symptoms of the disease, a reduction in the severity of the manifestations of the disease and a reduction in the period of virus elimination. This study is flawed: endpoints were not defined, sample size was not justified, and there were design and statistical flaws.
A scientific review of antiviral drugs is available (Meeting Report Prevention and treatment of respiratory viral infections: Presentations on antivirals, traditional therapies and host-directed interventions at the 5th ISIRV Antiviral Group conference. Antiviral Research. 2021 Jan;149:118-142. doi:10.1016 /j.antiviral.2017.11.013), which presents the results of studies of umifenovir. The study was conducted on mice; the ability of the drug to inhibit the reproduction of influenza A and B viruses at a dose of 60 mg/kg and increased survival (50% compared to 0% in the placebo group, Leneva et al., 2016) were noted. Of the minuses, the difficulty of complying with the treatment regimen (4 times a day) was noted and a wish was expressed for the development of long-acting drugs.
Another study on mice (2008), which was sponsored by the manufacturer of Ingavirin, showed the low effectiveness of Arbidol in comparison with the study Ingavirin [S.Ya. Loginova, S.V. Borisevich, V.A. Maksimov et al. / Study of the therapeutic effectiveness of the new domestic drug Ingavirin® against the causative agent of influenza A (H3N2) // Antibiotics and chemotherapy: journal. - 2008. - No. 53. - P. 7-8]. Manufacturer wars, however!
Since the early 2010s, individual studies on umifenovir in vitro or in animals have been published by European researchers:
- Article in the Journal of the American Society of Microbiology : “Arbidol inhibits in vitro infection of mammalian cells with Ebola virus, Tacaribe arenavir, and human herpes virus type 8. Suppression of hepatitis B virus and poliovirus by arbidol has been confirmed. Arbidol inhibits infection when added before or simultaneously with viral infection ( at the level of viral entry into host cells ) and is less effective when added 24 hours after infection [Pécheur EI, Borisevich V, Halfmann P, Morrey JD, Smee DF, Prichard M, Mire CE, Kawaoka Y, Geisbert TW, Polyak SJ. 2021. The synthetic antiviral drug arbidol inhibits globally prevalent pathogenic viruses. J Virol 90:3086–3092. doi:10.1128/JVI.02077-15].
That is, the drug works in laboratory conditions at the stage when the virus enters the body, and not later.
- Articles on laboratory research of Arbidol for infection caused by the Chikungunya virus : Arbidol inhibits infection in fibroblasts of lung tissue (Delogu et al., 2011), two analogues of Arbidol have been created that more selectively suppress the virus in vitro [A. Di Mola, A. Peduto, A. La Gatta et al. / Structure-activity relationship study of arbidol derivatives as inhibitors of chikungunya virus replication // Bioorganic & medical chemistry. — 2014. — Vol. 22, no. 21. -P. 6014−6025. doi:10.1016/j.bmc.2014.09.013. PMID 25282648].
- Arbidol interferes with the replication cycle at the stage of cell adsorption, can be included in cell membranes and prevents the virus from merging with the endosomal membrane (Blaising et al., 2014) [Abdelnabi, R. Towards antivirals against chikungunya virus / R. Abdelnabi, J. Neyts, L Delang // Antiviral Research. — 2015. — Vol. 121. -P. 59−68. - doi:10.1016/j.antiviral.2015.06.017. - PMID 26119058].
It turns out that even with this viral infection in the laboratory, Arbidol works at the level of virus penetration into the cell.
- A study published in the Journal of the Society of Microbiologists of Great Britain: the antiviral effect of Arbidol and its derivatives was studied in vitro at different stages of replication of the herpes simplex virus type 1 - the ability of the studied drugs to reduce the viral load and improve the antiviral response was shown. There was no significant difference in virus infectivity when Arbidol was added after the virus. Arbidol analogs were more active and significantly reduced virus-induced cytokine expression - it is assumed that these analogs may be promising for HSV1.
Again, the effect of the drug is laboratory confirmed, but early and less effective than similar compounds.
- German laboratory study of Arbidol and other antiviral drugs for infection caused by the Crimean-Congo hemorrhagic fever virus (in mice): Arbidol, along with other drugs, suppressed viral replication in vitro, but was not effective in animal studies [L. Oestereich, T. Rieger, M. Neumann et al. / Evaluation of antiviral efficacy of ribavirin, arbidol, and T-705 (favipiravir) in a mouse model for Crimean-Congo hemorrhagic fever // PLOS neglected tropical diseases. — 2014. -Vol. 8, no. 5. - P. e2804. doi:10.1371/journal.pntd.0002804. PMID24786461. PMC 4006714].
To summarize, we can say that Arbidol has a proven laboratory effect - it prevents the virus from entering the cell and blocks inflammation. But: this is only when it is introduced simultaneously with the virus and only in a test tube. Whether the desired effect exists in sick people has not been proven.
And of course about the SARS - CoV -2!
In China, a clinical study was conducted according to the standards of evidence-based medicine, which demonstrated the absence of a therapeutic effect of Arbidol against COVID-19 [Li, et al. // Efficacy and safety of lopinavir/ritonavir or arbidol in adult patients with mild/moderate COVID-19: an exploratory randomized controlled trial. // Med, Journal pre-proof, 17 April 2020; DOI: 10.1016/j.medj.2020.04.001].
However, in Russia, umifenovir is included in the “Temporary guidelines of the Ministry of Health for the prevention, diagnosis and treatment of new coronavirus infection (COVID-19)” dated April 28, 2020 as a possible treatment for mild forms of COVID-19 in combination with the nasal form recombinant interferon alpha. However, the same document reports that there is no evidence of its effectiveness and safety, and that the drug is in clinical trials.
In short, the effectiveness of umifenavir in the treatment of coronavirus remains to be tested in the future.
Is it worth being treated with Arbidol?
The answer to this question is still open. It is worth saying that the drug molecule is interesting and has research potential; the manufacturer needs to carry out properly organized studies on sick people. However, understanding the commercial success of Arbidol, it is unlikely that such studies will be carried out in the near future.
So everyone decides for themselves:
- The doctor needs to decide whether he will follow the clinical recommendations of the Ministry of Health and use this drug in the treatment of influenza (Arbidol is listed third in these recommendations, after Tamiflu and Relenza)
- For the patient – is it worth using this drug...
Be healthy!
Clinical studies of the effectiveness of Arbidol for the treatment and prevention of influenza and ARVI
Leneva I.A., Guskova T.A.
Influenza is a disease that, according to the World Health Organization (WHO), affects up to 100 million people worldwide every year. Mortality from influenza during epidemics in different age groups ranges from tens to hundreds of cases, and during a pandemic the rate can reach 1000 cases per 100 thousand population. In Russia, influenza and ARVI annually account for up to 90% of all registered infectious morbidity. WHO, in addition to vaccination, as the main strategy to combat influenza infection, recommends the use of etiotropic anti-influenza chemotherapy drugs [1,2]. Currently, several such drugs are used in the world. The first generation includes drugs of the adamantane series: amantadine and rimantadine, used in the USA and the West. The use of adamantane-type drugs is limited by the lack of activity against the influenza B virus. Second-generation drugs include neuraminidase inhibitors: zanamivir, used in aerosol form, and oseltamivir, used in the form of capsules or suspensions for children. Neuraminidase inhibitors are effective against both influenza A and B viruses.
In Russia, the original domestic drug Arbidol, created jointly by scientists from the Center for the Chemistry of Medicines (TsKhLS-VNIHFI, Moscow), the Institute of Medical Radiobiology of the Russian Academy of Medical Sciences (Obninsk) and the Research Institute of Epidemiology and Microbiology named after. Pasteur (St. Petersburg). Arbidol is administered orally in the form of tablets (50 mg) and capsules (100 mg). The drug has a systemic effect, is quickly absorbed and distributed to organs and tissues. The maximum concentration in blood plasma when taking Arbidol at a dose of 100 mg is achieved after 1.5 hours. Metabolism of Arbidol occurs in the liver. The half-life is 17-21 hours. The bioavailability of the drug is about 40% and does not depend on food intake [3,4].
Preclinical studies
Preclinical studies have shown that Arbidol inhibits the reproduction of influenza A and B viruses in cell culture and protects against the death of mice infected with influenza virus [3,4]. The antiviral activity of Arbidol has been convincingly proven in numerous preclinical studies performed in leading scientific centers in Russia, the USA, Great Britain, Australia, France, China and other countries [5,21-23]. A study of the mechanism of action of Arbidol showed that it acts in the early stages of viral reproduction and inhibits the fusion of the viral lipid membrane with intracellular membranes, preventing the virus from penetrating into the cell. Arbidol's mechanism of action differs from the currently used anti-influenza drugs: amantadine and rimantadine, which are blockers of ion channels formed by the M2 protein of the influenza virus, and neuraminidase (NA) inhibitors of the influenza virus - zanamivir and oseltamivir [5,6].
Experimental studies have shown that the effectiveness of Arbidol is due, in addition to the specific effect on viral reproduction, to interferon-inducing, immunomodulatory and antioxidant activity [3,4,7]. Toxicological studies revealed that the drug has low toxicity; phase I clinical trials of Arbidol showed its good tolerability in humans [3,4].
Studies in adults
Further clinical study of the effectiveness and safety of Arbidol as a treatment for influenza was carried out in the clinical department of the Research Institute of Virology named after. Ivanovsky (Moscow), Leningrad Research Institute of Epidemiology and Microbiology named after. Pasteur, All-Russian Research Institute of Influenza, Ministry of Health of the USSR (Leningrad) - in 1983-1984. The study involved 433 patients with moderate influenza who were in hospital or on outpatient treatment, of which 293 received Arbidol (200 mg 3 times a day for 3-5 days), 59 people received rimantadine, 68 received placebo and 24 received placebo and symptomatic therapy. The main criteria for assessing the therapeutic effectiveness of Arbidol were the timing of the reverse development of clinical syndromes and symptoms when compared in the main and control groups of patients. At the same time, the possibility of adverse reactions was taken into account. The results of clinical trials showed the therapeutic effectiveness of Arbidol in the treatment of patients with influenza A (H3N2) and B. The use of Arbidol at a dose of 200 mg 3 times a day for 3 days led to a reduction in the average duration of the disease by 1.7-2.65 days, the time of manifestation symptoms such as fever, intoxication, catarrhal phenomena, for 1.3-2.3 days. With the identical therapeutic efficacy of Arbidol and rimantadine for influenza A revealed in trials, Arbidol had a number of advantages over the latter. Thus, it was noted that there were no complications in patients with concomitant chronic diseases when using Arbidol, while in groups of patients treated with rimantadine, such complications were observed in 5.4% of cases. In the group of patients receiving symptomatic treatment, complications were observed even more often and amounted to 16.7%. Remantadine is known to be inactive against the influenza B virus. At the same time, a clinical study of Arbidol during the epidemic outbreak of influenza caused by the influenza B virus in January-March 1984 showed that treatment with Arbidol in 52 patients with a serologically confirmed diagnosis of influenza B, reduced the main symptoms of the disease and shortened the average duration of the disease by 2.65 days.
Three institutions participated in a clinical comparative double-blind placebo-controlled study of the preventive effectiveness of Arbidol: the Influenza Research Institute, the USSR Ministry of Health (Leningrad), the Leningrad Research Institute of Epidemiology and Microbiology named after. Pasteur and Research Institute of Virology named after. Ivanovsky (Moscow). These trials covered a total of 7646 people in organized adult groups and industrial enterprises, of which 4695 people received Arbidol, 111 received rimantadine and 2840 received placebo. According to the study design, each drug was assigned a corresponding code, which was revealed after completion of statistical processing.
During the study of the preventive effectiveness of Arbidol (from 1986 to 1990), influenza epidemics associated with the circulation of influenza A viruses (H3N2, H1N1) and influenza B viruses were noted, as well as outbreaks of mixed respiratory diseases caused by influenza, parainfluenza and adenoviruses. Assessment of preventive effectiveness in all medical institutions was carried out by comparing the incidence of influenza and ARVI in the experimental and control groups with the subsequent calculation of effectiveness indices (IE - the ratio of the number of cases per 100 people taking placebo to the number of cases per 100 people taking the drug) for the period taking medications and for 4-5 months after taking preventive courses. Data from clinical studies also showed good tolerability of Arbidol by adults when used daily at a dose of 200 mg for 10-20 days. No adverse events were noted.
During the period of a mixed epidemic outbreak of influenza A (H3N2) and B in organized groups, Arbidol had a preventive effect, which depended on the regimen of the drug. The IE for the preventive action of Arbidol compared to placebo averaged 2.0-3.0. The highest IE, equal to 3.12, was observed when using Arbidol 100 mg 2 times a week. Taking Arbidol (200 mg for 16-18 or 10-14 days) in the same groups during epidemic outbreaks of influenza caused by influenza A viruses H3N2 and H1N1 led to a decrease in the incidence of IE from 1.3 to 3.8. The prophylactic course in these studies was most effective in individuals who were not vaccinated against influenza (IE = 2.5) compared with those previously vaccinated (IE = 1.3). Clinical trials of the preventive action of Arbidol revealed the duration of its protective effect. After completing the course of prophylactic administration of Arbidol, no increase in the number of cases was observed, while discontinuation of the use of rimantadine, which was used in the trials as a comparison drug, led to a sharp increase in the incidence of influenza. 10 days after the end of the prophylactic use of the Arbidol course, its IE was 5.16, while for rimantadine it did not exceed 1.0. The fact of prolongation of the preventive effect of Arbidol was established for 4-5 months after carrying out preventive courses, when a decrease in the incidence of acute respiratory infections was noted by 1.4-3.6 times, depending on the study groups.
When Arbidol was taken orally at a dose of 200 mg once a day for 5 days in 240 patients in 128 family foci of infection during an epidemic outbreak of influenza A, the IE was 6.7, while with influenza B the number of cases decreased by 86.3 % with an efficiency index of 7.5.
Based on the results of many years of clinical studies of therapeutic and prophylactic effectiveness, Arbidol was approved for use in medical practice in adults as a therapeutic and prophylactic agent for influenza A and B and ARVI in 1990, and in children in 1995.
Data obtained from registrational clinical studies have also been confirmed in extensive post-marketing studies and clinical surveillance programs
In the program of clinical observation of the use of Arbidol in organized groups, carried out within the framework of registered indications of the State Center for Sanitary Epidemiology of the Ministry of Defense of the Russian Federation, in Moscow and the Moscow region. 800 patients participated. When taking Arbidol for medicinal purposes (200 mg 3 times a day for 3 days), the duration of fever, malaise, chills, headache in patients of the experimental group who received Arbidol for treatment was reduced by 1.3-1.8 times compared with control group, the length of stay at the medical center was reduced by 1.4 times. When taking Arbidol (200 mg 2 times a week for 3 weeks), a lower incidence rate was noted in the group taking the drug compared to the control group. The IE for using Arbidol was 1.33, and the protection rate was 25%. Prophylactic use of Arbidol reduced the number of complicated cases by 1.66 times. When taking Arbidol for therapeutic and prophylactic purposes (200 mg 2 times a week for 3 weeks, then in case of illness - 0.2 g 3 times a day for 3 days), the duration of intoxication symptoms in sick individuals was reduced by 1. 8-3 times, compared with the control group, the length of stay at the medical center was reduced by 1.6 times [12].
In another study conducted by the Department of Health of Zelenograd in the autumn-winter period of 2001-2002, among 2055 patients, prophylactic use of Arbidol (200 mg 2 times a week for 3 weeks) led to a significant decrease in the incidence of influenza and ARVI in individuals treated with the drug compared to the control group. The IE in the group receiving Arbidol was 3.2, with a corresponding protection rate of 68.7%. Serological studies confirmed the preventive effectiveness of Arbidol against other respiratory viruses (adenoviruses, respiratory syncytial virus, parainfluenza viruses type 1 and 3) circulating during the study period [13].
Of particular interest are studies of the effectiveness of Arbidol in people of the so-called risk group, which includes the working population with varying degrees of exposure to harmful production factors (workers of factories, factories, plants), leading to disorders in the immune system. A study conducted during the seasonal rise in the incidence of influenza and ARVI in 2004-2005. among such a group of workers and employees of the Novo-Lipetsk Metallurgical Plant (593 people), showed that the preventive use of Arbidol led to a 2.2-3-fold reduction in incidence compared to the control group. The combined use of Arbidol (200 g 2 times a week for 3 weeks) together with the influenza vaccine Influvac (Arbidol was taken before and after vaccination) reduces the incidence of the disease by 3-2.5 times, leading to an increase in the frequency of seroconversions and an increase in titers of specific antibodies to viruses influenza, including at the protective level [14].
Research in children
Children belong to the highest risk group for the incidence of influenza and ARVI; their annual incidence of influenza is 1.5-3 times higher than in adults. They are the main group in which influenza spreads, and schoolchildren are most often the primary sources of influenza infection in families. In the category of so-called frequently ill children, who suffer several episodes of ARVI during the year, complications are the most dangerous. Among them, ENT pathology prevails; complications such as bronchitis, pneumonia, sinusitis, tonsillitis, and acute otitis media are registered in every third child with influenza and ARVI [8,9]. The use of the only anti-influenza drug rimantadine in Russia at the beginning of the 90s of the 20th century in children, in addition to the lack of activity against the influenza B virus, was limited by the presence of side effects and the rapid emergence of resistance to it. These circumstances, as well as the safety and effectiveness of Arbidol in adults proven in clinical studies, served as the basis for the creation of a pediatric dosage form of the drug.
Clinical trials of the preventive and therapeutic effectiveness of the pediatric form of Arbidol were carried out in 4 institutions: Research Institute of Influenza, Leningrad Research Institute of Epidemiology and Microbiology named after. Pasteur, Laboratory of Etiology and Epidemiology of Influenza Research Institute of Virology named after. Ivanovsky RAMS and in the Department of Clinical Virology of the Research Institute of Virology named after. Ivanovsky RAMS. The trials involved 923 children aged 6 months to 14 years, of whom 479 received Arbidol and 444 received placebo. All trials conducted were randomized, placebo-controlled, and a clinical study at the Leningrad Research Institute of Epidemiology and Microbiology named after. Pasteur (155 children) was also double blind.
In studies of the therapeutic effectiveness of Arbidol in children conducted by the Influenza Research Institute and in the clinical department of the Virology Research Institute named after. Ivanovsky (158 and 120 children, respectively), for influenza caused by various serotypes of the virus, as well as when they are combined with ARVI pathogens of non-influenza etiology, the effectiveness of a 5-day course of Arbidol (10 mg/kg in 4 doses) averaged 84.8% . There was a significant reduction in the febrile period and the period of intoxication, the duration of symptoms of laryngotracheitis and catarrhal phenomena. The therapeutic effectiveness of Arbidol was most pronounced when administered early (the first two days of infection). A reduction in the period of viral antigen release from the nasopharynx was observed. It was noted that in children receiving Arbidol at a dose of 50 mg 3 times a day for 5 days, in no case was nosocomial superinfection observed, while in the placebo group reinfection was detected in 2 patients.
Randomized placebo-controlled trials of the preventive effectiveness of Arbidol in children were conducted during 3 epidemic seasons (1993, 1994, 1995) during the rise in the incidence of influenza and ARVI (490 children aged 3 to 7 years).
In a double-blind, placebo-controlled clinical study at the Leningrad Research Institute of Epidemiology and Microbiology. Pasteur (155 children) showed that use of the drug at a dose of 50 mg 2 times a week for 3 weeks 2 weeks before the peak incidence of influenza B led to a reduction in incidence by 1.2-4.4 times, depending on the age group.
In studies conducted by the Research Institute of Virology. Ivanovsky with the participation of 335 children aged 6-15 years, it was shown that when using Arbidol at a dose of 50 mg 3 times a week for 5 weeks, the total incidence, regardless of the etiology of ARVI, IE ranged from 2.05 to 2.22, and efficiency ratio from 51.3 to 55%. Taking Arbidol prevented the development of severe forms of the disease and reduced the incidence of complications and exacerbations of chronic diseases. In children 3-4 years of age, no complications were noted; in the control group they amounted to 5%. In the group of children 5-6 years old who received Arbidol, complications occurred in 9% of cases, in the control group of children who received placebo, complicated forms of ARVI were observed in 30% of cases (trial reports 10, 11).
In a clinical study conducted by the Research Institute of Virology. Ivanovsky, Russian State Medical University, Scientific Center for Children's Diseases of the Russian Academy of Medical Sciences, Morozov Children's Clinical Hospital (Moscow) with the participation of 500 children showed that when treated with Arbidol, there was a reduction in the duration of uncomplicated respiratory infections by 2.7-4.7 days, depending on the groups of children participating in the study . In addition, milder infections were observed, as well as a reduced risk of complications. When carrying out a full preventive course of treatment with Arbidol, the number of children suffering from influenza and ARVI was recorded 1.4 times less, and the frequency of episodes was 1.86 times less in comparison with the same indicators in the control group. Among children taking Arbidol, acute respiratory infections were recorded 1.7 times less frequently during 3 months of observation. In the group of children suffering from chronic diseases of the respiratory tract, the number of cases among those taking Arbidol was 3.7 times less than in the control group, and the number of complications (acute bronchitis, pneumonia, otitis media) was 4 times less than in the control group [15 ].
Similar results were obtained at the National Medical University in Kyiv (Ukraine). The study involved 156 children aged 6 to 12 years. Taking Arbidol for 4 weeks by children aged 6 to 12 years, 100 mg once every 3 days, and children over 12 years old, 200 mg once every 3 days, helped reduce the incidence of influenza and ARVI by 2.6 times. The drug prevented the development of severe forms of the disease, as well as the development of complications. The duration of symptoms of influenza infection was reduced by an average of 1.1-3.6 days [16].
The purpose of another clinical study conducted by the Research Institute of Virology named after. Ivanovsky in January 2004 at the Infectious Diseases Clinical Hospital No. 1 (Moscow) among 90 children aged 2 to 6 years, the effectiveness of Arbidol was assessed for ARVI of various etiologies. These studies showed that during the period of morbidity caused mainly by the parainfluenza virus and respiratory syncytial virus and occurring with obstructive laryngitis or broncho-obstructive syndrome, the use of Arbidol led to a reduction in the duration of the period of intoxication and catarrhal phenomena, more rapid relief of croup syndrome and broncho-obstructive syndrome . No cases of reinfection were identified [17].
Resistance
Studies of clinical isolates have shown that the percentage of influenza A virus strains resistant to adamantane-type drugs has increased enormously in the world over the past 2-3 years, reaching 90% in some countries, for example, China and the USA. The high incidence of resistance to amantadine and rimantadine has led to a ban in the United States since the last epidemic season on the use of these drugs for the treatment and prevention of influenza A. Until recently, it was believed that the incidence of resistant strains when taking the neuraminidase inhibitor oseltamivir was 1.3% in adults and 8.6% in children. However, a complete surprise was the increase in oseltamivir-resistant viruses among circulating subtype A H1N1 viruses detected since the beginning of 2008, and these viruses were isolated from people who did not take the drug. The largest number of such strains in Europe were isolated in Norway (64%) and France (39%), in the USA (9%), in Hong Kong and Australia. In Russia, since February 2008, among the circulating strains of influenza A H1N1 virus, 40-50% resistant to oseltamivir were also found.
Mutants resistant to Arbidol have so far been obtained only in experiments through multiple (about 20) passages in cell culture in the presence of increasing concentrations of Arbidol [6]. Despite the widespread use of Arbidol, studies of over 160 clinical isolates isolated in Russia during the epidemic season of 2000-2005 did not reveal a single strain resistant to Arbidol [20]. High sensitivity to Arbidol was also shown for all isolates of influenza viruses that caused epidemic increases in incidence in 2005-2008, including rimantadine- and oseltamivir-resistant strains of influenza A virus. In addition, in a clinical study involving 39 patients infected with influenza A viruses and B, the formation of resistance to Arbidol was not detected during a 5-day course of treatment with the drug (Leneva I.A., Burtseva E.I., personal communication).
Thus, many years of clinical registration and subsequent post-registration studies of Arbidol, covering about 14 thousand patients, as well as more than 15 years of experience in the widespread use of the drug in medical practice as a therapeutic and prophylactic agent for influenza and ARVI in adults and children have shown its high effectiveness and good tolerability. The use of Arbidol for the treatment of influenza infection and ARVI leads to a reduction in the average duration of the disease by an average of 1.7-2.65 days, a decrease in symptoms of the disease, prevention of the development of post-influenza complications and a decrease in the frequency of exacerbations of chronic diseases. When preventing influenza infection, the use of Arbidol increases the body's resistance to viral infections, ensuring a reduction in morbidity in unfavorable epidemiological conditions. All studies conducted showed good tolerability of the drug. Given the identical therapeutic efficacy of Arbidol and rimantadine for influenza A, Arbidol has a number of advantages, expressed in a wider spectrum of action, currently unknown resistance to the drug and a high level of safety in various schemes of its use in adults and children.
References 1. Hayden F. WHO Guidelines on the Use of Vaccines and Antivirals during Influenza. Annex 5-Considerations for the Use of Antivirals during an Influenza pandemic, Geneva, 2-4 October, 2002. 2. Influenza and other respiratory viral infections: epidemiology, prevention, diagnosis and therapy / Ed. O.I. Kiseleva, I.G. Marinich, A.A. Sominina. St. Petersburg, 2003.245p. 3. Glushkov, RG 1992. Arbidol. Drug of the Future 17:1079–1081. 4. Guskova T.A. and Glushkov R.G. Arbidol-immunomodulator, interferon inducer, antioxidant.// Moscow, Timotek, 1999.- 93 p. 5. Glushkov R.G., Fadeeva N.I., Leneva I.A. and others. Molecular biological features of the action of the new antiviral drug Arbidol // Chemical and Pharmaceutical Journal. - 1992. - 2. - 8-15 6. Leneva I., Hay A. The mechanism of action of arbidol against influenza virus - selection and characterization of arbidol-resistant mutants 2002 12th International Congress of Virology, Paris, Abs.1077 7. Kubar O.I., Stepanova L.A. , Safonova L.S., Rozaeva N.R. Clinical application of the immunomodulatory properties of Arbidol in ARVI.-IV Russian National Congress “Man and Medicine”, 1997; 269 8. Acute respiratory diseases in children: treatment and prevention / Scientific and practical program of the Union of Pediatricians of Russia.-M.: International Foundation for Mother and Child Health. 2002.-69s. 9. Uchaikin V.F.. Guide to infectious diseases in children. - Geotar Medicine, 1998. - 700 p. 10. Drinevsky V.P. Osidak L.V. Natsina V.K. and others. Chemotherapy in the treatment of influenza and other respiratory viral infections // Antibiotics and chemotherapy .- 1998.- 9.- P.29-34. eleven . Belyaev A.L., Burtseva E.I., Slepushkin A.N. and others. Arbidol is a new drug for the prevention of influenza and acute respiratory viral infections in children // Bulletin of the Russian Academy of Medical Sciences. - 1996. - 3. - P. 34-37. 12. Shumilov V.I., Shuster A.M., Lobastov et al. The effectiveness of Arbidol in the prevention and treatment of acute respiratory infections. //Military medical journal.- 2002. -T.9.-S. 51-53. 13. Selkova E.P., Semenenko T.A., Gotvyanskaya T.P. and others. Preventive and therapeutic effectiveness of Arbidol. // Epidemiology and vaccination.-2005.- 4.-P.17-24. 14. Semenenko T.A., Selkova E.P., Gotvyanskaya T.P. and others. Indicators of immune status during specific and nonspecific prevention in the elderly.// JMEI.-2006.-P.24-29 15. Uchaikin V.F., Kharlamova S.G., Cheshik S.G. and others. The use of Arbidol and amixin as etiotropic therapy for influenza and ARVI in children // Pediatrics.-2004.-5.- P.73-77. 16. Kramarev S.A., Palatnaya L.A. , Litus V.I. Experience of using Arbidol in the treatment and prevention of influenza and ARVI in children in Ukraine // RMZh.-2003.-21.-P.1050-1051. 17. Cheshik S.G., Vartanyan R.V. The effectiveness of Arbidol therapy for acute respiratory viral infections in young children //New drugs.-2005.-11.-P.37-44. 18. Bright R., Medina M., Xu X., et al. Incidence of adamantine resistance among influenza A (H3N2) viruses isolated worldwide from 1994 to 2005: a cause fro concern.// Lancet.-2005.- 19. Lackenby, A., Hungnes O., Dudman SG, Meijer A., Paget WJ, Hay AJ, Zambon MC, 2008. Emergence of resistance to oseltamivir among influenza A(H1N1) viruses in Europe // Euro. Surveill.-13-R.5. 20.Burtseva E.I. Shevchenko E.S. Leneva I.A. and others. Sensitivity to remantadine and Arbidol of influenza viruses that caused epidemic increases in incidence in Russia in the 2004-2005 season // Questions of Virology. - 2007. - 2. - P. 24-29 21. Shi L, Xiong H, He J, Deng H, Li Q, Zhong Q, Hou W, Cheng L, Xiao H, Yang Z. Antiviral activity of arbidol against influenza A virus, respiratory syncytial virus, rhinovirus, coxsackie virus and adenovirus in vitro and in vivo // Arch Virol. -2007.- May, 22. Boriskin Y., Leneva I., Pecheur E., Polyak S. Arbidol: a broad-spectrum antiviral compound that blocks viral fusion// Current Med. Chem.- 2008.-15.-Р.997-1005 Review Invited (English) 23. Brooks, MJ; Sasadeusz, J. J.; Tannock, GA // Curr. Opin. Pulmonary Med.- 2004.- 10.- R. 197.
Antiviral “Arbidol” is again tested for effectiveness after 20 years
How common medications become dangerous
announced clinical trials of Arbidol. The drug was approved by the Ministry of Health for medical use back in 1988 as an antiviral agent, and since 1992 it has appeared on the pharmaceutical market. Today it occupies one of the leading places in sales. However, the manufacturer is again going to test the drug for effectiveness, as well as for “the emergence of drug-resistant influenza virus strains.”
In general, such studies are not surprising and even commendable, says chief clinical pharmacologist, Professor Alexander Hadjidis. After all, it is not uncommon for the dangers of drugs to be discovered decades after the start of their active use. This happened with acytylsalicylic acid (aspirin), the effect of ulcer formation from the use of which was discovered only forty years after the start of its production. The side effects of the sleeping pill Thalidomide turned out to be even more terrible - it was even prescribed to pregnant women. And only many years later it became clear that the medicine leads to congenital physical deformities of the fetus.
Moreover, this is not only due to the fault of the manufacturer, who did not study the medicine well enough. The fact is that about five million xenobiotics are known - substances foreign to the body that have side effects on it, but the influence of only a few thousand of them has been studied. That's why more drug research is welcome.
Positive effect of notoriety
However, “Arbidol” can be called a unique drug, not in the sense of its therapeutic effect, but because of the notoriety that accompanies it throughout the years. Some doctors believe that Arbidol does not have an antiviral effect, others are inclined to believe that it works as an immunostimulant. Only Professor Oleg Kiselev, director of the Influenza Institute, where the first tests of the drug were carried out, calls the medicine the first means of preventing and treating influenza and ARVI. Although the results of these studies remained unknown to the medical community. And the manufacturer’s attempts to enter the international market were unsuccessful - the drug was not recognized abroad. The World Health Organization considered it unpromising, and the US Food and Drug Administration (FDA) refused to register Arbidol as a drug.
But this did not stop Russian officials from including the medicine in the list of vital drugs. It is not surprising that there were rumors around the drug about lobbying by the ministry itself. And the manufacturing company even sued the president of the Society of Evidence-Based Medicine, Professor Vlasov, who, like many scientists, called the evidence base of Arbidol insufficient. In 2007, the Formulary Committee at the Russian Academy of Medical Sciences called Arbidol an obsolete drug with unproven effectiveness and demanded that it be immediately removed from the list of medicines used to provide medicine to citizens.
He who produces is the one who checks
Will new drug trials shed light on its true effectiveness and safety? According to the medical director of Pharmstandard OJSC, the studies will be conducted in a double-blind, randomized and placebo-controlled manner (RCT). The good thing about this method is that neither the patient nor the researcher knows anything about each other, and until the end of the experiment it is not known which of the patients receives a placebo and which receives the real drug. This makes the research more objective, although it does not exclude the possibility of manipulating the results. Simply put, it is beneficial for a manufacturer interested in selling a drug to show off the product and hide the negative aspects.
“The problem is that, according to the Law on the Circulation of Medicines, clinical trials in our country are carried out by the developers themselves, unlike in the European Union countries, where independent organizations also have the right to do this,” says the chief clinical pharmacologist.
Two years ago, the Formulary Committee at the Russian Academy of Medical Sciences approached the State Duma with a proposal to allow independent experts to conduct clinical trials, and not just drug manufacturers interested in a positive result. But the deputies refused.
The location of the drug trial is still unknown
So, the test results again fall on the conscience of the manufacturers. It is worth noting that clinical studies of Arbidol have already been conducted about ten times, one of them even in China. But, according to Alexander Hadjidis, so far they have been very unconvincing. And it was never possible to prove the effectiveness of the drug. It seems that this time the company has set high goals for itself - to enter the world market with Arbidol. The medical director of Pharmstandard is confident that “new studies will provide additional evidence of the effectiveness and safety of the drug, which will be accepted by experts of the highest level, both in Russia and abroad.”
To confirm their intentions, the manufacturers named the names of famous scientists under whose watchful eye clinical trials will take place. This is the director of the Influenza Research Institute, academician of the Russian Academy of Medical Sciences, Professor Oleg Kiselev and the chief infectious disease specialist of the Northwestern Federal District, professor of the Department of Infectious Diseases of the Northwestern State Medical University. Mechnikova Tamara Sologub.
To find out more, "Doctor Peter" tried to contact experts. However, the Influenza Research Institute refused to give any comments without the consent of the head of the institute, who is away. Tamara Sologub said that she does not personally take part in the Arbidol trials and said that the quality of their conduct is the responsibility of the chief investigator, who is approved by the company and the Ministry of Health and works in the institution where the trials are conducted.
— This is a competent specialist with experience in clinical and research activities.
According to Tamara Sologub, the research will take place in 18 specially accredited centers with experience in such tests, located in 9 cities of the country. In St. Petersburg, this could be the Institute of Influenza and the Hospital named after. Botkin - institutions where adult patients with influenza are admitted. The studies will involve 840 people and will take place over two seasons of influenza epidemics.
Therefore, to begin testing, an outbreak of influenza incidence is necessary, but so far the epidemiological threshold has not been exceeded.
Nina Bashkirova, photo nakanune.ru
© DoctorPeter
Experience of using Arbidol in clinical practice
In Russia, about 30 million cases of ARVI are registered annually, and the total economic damage reaches 40 billion rubles. At the same time, each sick person spends 450–3000 rubles on necessary medications. Not only the medical, but also the socio-economic significance of this issue is obvious. Such a high incidence and ineffectiveness of control methods are due to the polyetiology and mixed nature of infections (there are more than 300 viruses of 7 families), the speed and ease of transmission of pathogens (airborne), the high contagiousness of viruses and the sensitivity of the macroorganism to infection, the year-round high background of ARVI, the variability of antigenic properties of viruses (especially influenza A viruses, leading to partial or complete changes in group and strain determinants), the narrow specificity of the action of most drugs. There are a huge number of drugs for pathogenetic and symptomatic treatment of ARVI (antipyretic, antitussive, expectorant, anti-inflammatory, antihistamine, broad-spectrum antibiotics for post-influenza bacterial complications, as well as homeopathic and immunomodulatory, etc.). The role of immunoprophylaxis against influenza remains. Russia has accumulated extensive experience in the use of both live and inactivated influenza vaccines. However, the effectiveness of vaccine prevention depends on a large number of factors, and coverage of the entire epidemically significant percentage of the population with preventive vaccinations is impossible. In this regard, the Ministry of Health of the Russian Federation revised the tactics of influenza vaccine prevention (Orders of the Ministry of Health of the Russian Federation No. 101/46 of April 9, 1995 and No. 25 of January 27, 1998). Vaccination against influenza is primarily recommended for persons in the “increased risk of infection” group: (children, medical personnel, military personnel, workers in the sphere of consumer services, transport, educational institutions, etc.), as well as groups “increased risk of developing adverse consequences of an influenza infection.” (persons over 60–65 years old, suffering from certain chronic diseases, frequently ill children of preschool age and school age). It must be remembered that specific immunoprophylaxis has some disadvantages. Thus, vaccines, affecting humoral immunity, are effective only against a specific strain of the influenza virus. The production of specific antibodies begins 2 weeks after vaccination, and therefore, the use of vaccines is advisable only for the prevention of influenza and only before the outbreak of an epidemic. The protective antibody titer lasts up to 3 months, which requires revaccination every year. With specific immunoprophylaxis, an immunosuppressive period is observed (from 10 to 15 days), there are contraindications for it, and allergic reactions occur in 40% of cases. In addition, despite the increase in the incidence of acute respiratory viral infections over the past decade, there has been no increase in the incidence of influenza, as a result of which the latter accounts for about 10% in the structure of acute respiratory viral infections. The main percentage falls on respiratory infections of non-influenza etiology. Currently, for the prevention and treatment of acute respiratory viral infections, priority is given to etiotropic chemotherapy drugs that act directly on the infectious agent. Chemotherapeutic agents are represented by M2 channel blockers (amantadine, rimantadine) and neurominidase inhibitors (zanamivir, oseltamivir), as well as a synthetic drug of the class of abnormal nucleosides ribavirin. But these groups of drugs have their drawbacks. Thus, M2 channel blockers are not active against the influenza B virus; their use is accompanied by serious side effects and the rapid emergence and spread of strains resistant to them; neurominidase inhibitors are expensive and also cause side effects; Ribavirin is active only against respiratory syncytial virus. There was an obvious need to develop new tools that would not have these disadvantages. The Center for the Chemistry of Medicines - the All-Russian Research Chemical and Pharmaceutical Institute - has created a new drug - Arbidol, which reduces the risk of influenza and other acute respiratory viral infections during an epidemic by 7.5 times. The use of Arbidol is approved as a preventive and therapeutic agent for children and adults with influenza (including bird flu) and ARVI, including those complicated by bronchitis and pneumonia; in the complex treatment of pneumonia, chronic bronchitis, recurrent herpes infection; for the prevention of postoperative complications and normalization of the immune status in patients who have undergone surgical interventions; for the treatment of acute rotavirus intestinal infections in children over 2 years of age and severe acute respiratory syndrome. Arbidol's chemical structure is ethyl ester 6 - bromine - 5 - hydroxy - 1 - methyl - 4 - dimethylaminomethyl - 2 - phenylthiomethyl - indole - 3 - carboxylic acid hydrochloride. The mechanism of action of Arbidol consists of suppressing the reproduction of the influenza virus, influencing the synthesis of interferon (IFN), increasing the number of T lymphocytes and the functional activity of macrophages, as well as an antioxidant effect. Let us consider these mechanisms in more detail. In order to identify the stage of viral reproduction that is inhibited by Arbidol, a special study was conducted [1]. In the course of studying the effect on influenza virus endocytosis, it was revealed that this drug inhibits the process of fusion of the lipid viral envelope with endosome membranes at pH 7.4, leading to the release of the viral genome and the beginning of transcription. Thus, Arbidol acts in the early stages of viral reproduction. To determine the mechanism of inhibition and prove the virus-specific action of Arbidol, the approach of obtaining and studying mutants resistant to this drug was used. Unlike amantadine and rimantadine, to which resistant strains are formed after 1–2, maximum 3 passages of the virus, mutants resistant to Arbidol were obtained only after 15 passages (in the latter, the mutations were localized in the gene encoding hemagglutinin). [2] Based on the results of a study of mutants, it was concluded that Arbidol interacts with the NA of the influenza virus, increasing its stability to conformational changes induced by low pH and that is why it inhibits the process of fusion of the virus envelope with endosome membranes. The virus-specific properties of Arbidol were confirmed by the National Institute for Medical Research (London, UK) in 2004. The advantage of Arbidol is the lack of strain specificity. In cell cultures, it suppresses the reproduction of influenza A virus by 80%, influenza B virus by 60%, and influenza C virus by 20%. Unlike rimantandine, this drug suppresses the reproduction of rimantandine-sensitive and rimantandine-resistant strains of the virus. Arbidol also has an effect on the avian influenza virus (which was studied on the A/Hong Kong virus in cell culture in the Department of Virology at St. Jude Children's Hospital, USA), but less strongly than on the reproduction of human strains of the influenza virus. The effect of Arbidol on the synthesis of IFN has been shown in vitro in cell culture and when taking the drug by volunteers. IFN synthesis increased, starting from taking 1 tablet (40–80 IU/ml in 61.5% of volunteers) to 3 tablets (1600 IU/ml in 100%). However, there was no further increase in IFN levels when taking Arbidol; on the contrary, it decreased. A rapid increase in IFN synthesis can have a preventive effect when taking Arbidol before the onset of influenza [3,4]. The immunomodulatory activity of the drug, as well as the evaluation of the effectiveness of its use, were studied in clinical trials conducted in 13 institutions in St. Petersburg, Moscow and the Moscow region. The relevance and importance of these studies is also determined by the specifics of the selected populations, namely risk populations, which include medical workers, military personnel and children. The study of the effect of Arbidol on immune status was carried out on a limited contingent of medical workers (Central Clinical Hospital No. 1 in Zelenograd), who are not only the group most at risk of infection, but also a source of infection for patients. Arbidol in the form of tablets of 0.2 g was used for prophylactic purposes per os 2 times a week for three weeks. Using a random sampling method, 2 groups of 38 people each, equal in all respects, were formed: the experimental group received Arbidol, and the control group received placebo according to the same scheme. The studies were carried out over time: before the start of therapy, after 7 and 21 days from the start of the drug. Patients of both groups were examined according to a single scheme, which included determination of parameters reflecting the functioning of the main components of the immune system (cellular, humoral and phagocytic). In order to assess the effect of Arbidol on indicators of specific immunity, a serological study of blood serum samples was carried out. Using a randomized method, 2 groups were formed: an experienced group (96 people) received Arbidol; the control group (107 people) received placebo. Blood sera were examined by enzyme-linked immunosorbent assay (ELISA) for the presence of specific antibodies to influenza A (H1N1 and H3N2) and B viruses, respiratory syncytial (RS) virus, adenovirus and parainfluenza viruses types 1 and 3. According to research results, it was revealed that Arbidol has an immunomodulatory effect, leading to an increase in the total number of T-lymphocytes and T-helper cells (determined using monoclonal antibodies to lymphocyte antigens). Moreover, normalization of these indicators was observed in patients with an initially reduced number of CD3 and CD4 cells, and in medical workers with normal functioning of cellular immunity there were practically no changes in the number of T-lymphocytes and T-helper cells. The use of Arbidol does not lead to a significant decrease in the absolute number of T-suppressor lymphocytes, which means that the stimulating activity of the drug is not associated with inhibition of the function of suppressor cells. An important property of Arbidol is its positive effect on phagocytosis (the total number of macrophages with absorbed bacteria and the phagocytic number increases). It is assumed that the activating stimuli for phagocytic cells were cytokines and, in particular, interferon, the production of which is enhanced under the influence of Arbidol. An increase in the content of NK cells was also noted in individuals in the experimental group, which allows the drug to be characterized as an inducer of natural killer cell activity. During the research, it was not possible to establish a significant effect of Arbidol on the content of B-lymphocytes and the levels of immunoglobulins of the main classes. The lack of immunosuppressive effect of the drug on the production of specific antibodies to respiratory viruses was confirmed by ELISA results. The study of the epidemiological effectiveness of Arbidol was carried out in the autumn-winter period of 2001-2002. on a contingent of 2055 people. For prophylactic purposes, 940 people received the drug (experimental group), 1115 people received placebo (control group). The results of serological studies revealed a wide range of pathogens circulating at that time. The largest share of the incidence of ARVI in both groups was due to adenovirus (22.3±3.3% in the experimental and 19.5±1.8% in the control groups) and RS virus (15.0±2.1% and 15 .8±2.2% respectively). And according to the results of the study for the presence of antibodies (characterizing the infection of the subjects), it was shown that in 43.7±5.1% (in the experimental group) and 52.2±5.4% of cases (in the control group) antibody titers to two and more infectious agents. The proportion of individual pathogens entering the association was different and depended on the intensity of their circulation during the examination period. The most common “partners” in the formation of mixed infections in both groups were parainfluenza viruses type 1 and adenoviruses. Epidemiological tests have shown that the use of Arbidol led to a significant decrease in the incidence of influenza and ARVI in individuals in the experimental group compared to the control group. Thus, in the experimental group, 77 people fell ill (which amounted to 8.2±0.7%) compared to 292 in the control group (26.2±1.3%). The high preventive activity of Arbidol against viruses that cause ARVI is confirmed by an effectiveness index of 3.2 with a corresponding protection index of 68.7%. According to the Influenza Research Institute of the Russian Academy of Medical Sciences, the preventive effect of Arbidol may be even higher: the use of the drug among workers at an industrial enterprise in Severodvinsk during an epidemic of influenza type A led to a 3.8-fold decrease in incidence. Among persons who were in contact with patients with influenza during epidemic outbreaks of influenza A and B, the effectiveness index of Arbidol was 6.7 in relation to placebo and 4.5 in relation to rimantadine, with corresponding protection rates of 85.1 and 77.8%. Undoubtedly, the results of studies of the effectiveness of Arbidol in the prevention and treatment of influenza and ARVI in groups of “increased risk of infection” are important. Thus, in military collectives, especially in newly formed units, training centers, units of peacekeeping forces, etc., their renewal serves as a trigger for intensifying the epidemic process. The issue of the lack of effectiveness of vaccination has already been discussed. The need for economic analysis is also obvious, primarily to identify the feasibility of financing certain preventive measures on a large scale. During the seasonal rise in the incidence of influenza and other acute respiratory viral infections, specialists from the 736 Center for Sanitary and Epidemiological Surveillance of the Ministry of Defense of the Russian Federation conducted a study at the military training center in order to compare the results and costs of using Aribidol in military personnel during the formation of military teams. According to the Center for Ecology and Epidemiology of Influenza, Research Institute of Virology, Academy of Medical Sciences of the Russian Federation, the incidence was associated with the circulation of type A2 (H3N2) and predominantly B viruses. The study included 800 military personnel (400 in the study group who received Arbidol for prophylactic purposes, and 400 in the comparison group without drug prophylaxis). For preventive purposes, Arbidol was prescribed 0.2 g twice a week for three weeks. The morbidity of military personnel with a primary diagnosis of ARVI, both with complications (acute bronchitis, acute pneumonia) and without complications, was analyzed. The incidence rate among individuals taking Arbidol was 270±22, and in the control group – 360±24 (p<0.05). The use of Arbidol contributed to a reduction in the incidence rate by 1.33 times compared to the control group. Prophylactic use of Arbidol reduced the number of complicated cases compared to control by 1.66 times. It was found that the number of latent forms of ARVI was also 1.3 times less. To study the effect of the drug for medicinal purposes in the event of uncomplicated forms of influenza and other acute respiratory viral infections, the drug was prescribed at a dose of 0.2 g 3 times a day for 3 days. As a result, the duration of fever and other manifestations of intoxication syndrome (malaise, chills, headache, etc.) in the group of military personnel who received Arbidol for the treatment of ARVI was reduced by 1.3–1.8 times compared with persons who did not receive Arbidol for either prevention or treatment; the length of stay at the medical center was reduced by 1.4 times. The subjects who received Arbidol had no adverse or adverse reactions. The analysis showed the economic feasibility of using Arbidol by reducing the cost of treating both uncomplicated and complicated forms of respiratory infections. Another group at “increased risk of infection” are children. The share of ARVI together with influenza is at least 70% in the structure of all pathologies in children. In most epidemics, the highest incidence rate is observed in preschoolers 3–6 years old and schoolchildren 7–14 years old. It is necessary to pay special attention to the group of “frequently ill children”, since frequent respiratory diseases can cause disruption of basic adaptation mechanisms, lead to significant impairments in the functional state of the body and contribute to the development of chronic pathology. The group of “frequently ill children” is very heterogeneous in terms of the composition of patients. According to Albinsky V.M., Baranov A.A. (1986), in this group, upper respiratory tract diseases account for 82%, and the frequency of respiratory infections is especially high. A study was conducted to evaluate the effectiveness of Arbidol during the period of epidemic rise in the incidence of influenza and other acute respiratory viral infections (November 2001 - February 2002) among children over 6 years of age. As a result of the analysis of the main indicator of the preventive effectiveness of the drug (the number of episodes of respiratory infections over 3 months of observation per child), it was found that the most pronounced effect was obtained in children who suffer from uncomplicated forms of ARVI less than or more than 5 times a year, or complicated forms less than 3 times a year (the efficiency index compared to the control in these groups was about 2). Among children with chronic pathology of the respiratory tract, there was a significant decrease in the frequency of episodes of acute respiratory diseases (0.25±0.08 in the experimental group and 0.42±0.03 in the control group, p<0.05). On average, expenses per child can be reduced by 1.2 times due to cost optimization: increasing costs for prevention through the use of Arbidol and reducing total costs due to other components (provision of outpatient care, hospitalization, medications used for treatment ARVI, etc.). Thus, these studies clinically substantiate the feasibility and advantages of using Arbidol for therapeutic and prophylactic purposes and from the point of view of pharmacoeconomics.
References 1. Leneva I., Hay A. The mechanism of action of arbidol against influenza virus–selection and characterization of arbidol–resistant mutants. 2002, 12th Intern. Congress of Virology, Paris, abst. 1077. 2. Belshe, B. Burk, F. Newman et al. Drug resistance and mechanism of action amantadine on influenza A viruses. J. Inf. Dis., 1989, 159, 430–435. 3. Guskova TA, Nikolaeva IS, Zacharova NG Experimental and clinical study of arbidol, an antiviral drug. 9th Mediterranean Congress of Chemotherapy, 1994, abs. 82. 4. Glushkov R.G., Guskova T.A., Krylova L.Yu., Nikolaeva I.S. Mechanisms of the immunomodulatory action of arbidol. Bulletin of the Russian Academy of Medical Sciences, 1999, No. 3, pp. 36–40. 5. Chuvirov G.N.; Markova T.P., “Antiviral drug – arbidol.” 6. Glushkov R.G., Fadeeva N.I., Leneva I.A. and others. Molecular biological features of the action of arbidol, a new antiviral drug. Chemical and Pharmaceutical Journal, 1994, No. 2, pp. 5–8. 7. Hayden F. WHO Guidelines on the use of vaccines and antivirals during Influenza. Annex 5–Considerations for the use of antivirals during an Influenza pandemic, Geneva, 2–4 October, 2002. 8. Shumilov V.I., Shuster A.M., Lobastov S.P. and others. The effectiveness of arbidol in the prevention and treatment of acute respiratory viral infections in military personnel. Military Medical Journal, 2001, v. 323, no. 3, pp. 51–53. 9. Belyaev A.L., Burtseva E.I., Slepushkin A.N. and others. Arbidol is a new drug for the prevention of influenza and acute respiratory infections in children. Bulletin of the Russian Academy of Medical Sciences, 1996, No. 6, pp. 34–37. 10. Albitsky V.Yu., Baranov A.A. Frequently ill children. Clinical and social aspects: Ways of recovery. – Saratov, 1986. 11. Korovina N.A., Cheburkin A.V., Zaplatnikov A.L., Zakharova I.N. Immunocorrective therapy for frequently and long-term ill children. M., 1998.–44 p. 12. Order of the Minister of Health of the Russian Federation dated December 22, 1998. Appendix No. 1. – Industry classifier. – “Simple medical services.” 13. L.Kaiser, R.Couch, G.Galasso et al.. First International Symposium on influenza and other respiratory viruses: summary and overview. Kapalua, Maui, Hawaii, December 4–6, 1998. Antiviral Research, 1999, 42, 149–176. 14. Bektimirov T.A. Recommendations from WHO and international forums on tactics to combat influenza in connection with a possible pandemic. Bulletin “Vaccination”, 2003, 3 (27), 1–5.
Influenza (code J 11.1 according to ICD10) is the only disease among acute respiratory viral infections (ARVI) that is registered based on etiology. At the same time, the possibility of making a diagnosis of “influenza” based only on clinical data without laboratory verification exists only during the epidemic rise of this disease in the region. If there are typical symptoms of infection and it is not possible to determine its etiology, the diagnosis of “influenza-like illness”, proposed by WHO along with the terms ARI (acute respiratory infection) and SARI (severe ARI) is valid for a more accurate and quicker ability to monitor the dynamics of the development of an influenza epidemic (pandemic). in the world [1].
Influenza is caused by RNA viruses belonging to the Orthomyxoviridae family, genus Influenza virus, which includes influenza viruses types A, B and C [2]. Influenza A viruses cause diseases in humans, birds, wild and domestic mammals, but their main natural reservoir is waterfowl. Type B influenza viruses have been isolated only from humans, and type C viruses have been isolated from humans and pigs. The main reason for the occurrence of epidemics and pandemics is a change in the nucleotide sequence in the genes encoding the surface antigens of influenza viruses types A and B - hemagglutinin (HA) and neuraminidase (NA), which determine the specificity of viruses.
There are two types of antigenic variability of viruses:
- drift – point mutations in a gene associated with evolution and immunoselection pressure within a subtype, allowing a new antigenic variant of the virus to escape population immunity, causing annual increases in incidence;
- shift (only for influenza A viruses) - a change in HA and/or NA as a result of reassortment (exchange of genome fragments between different viruses during co-infection of a sensitive host) or the resumption of circulation of an extinct strain after long-term persistence in the host’s body. The lack of specific immunity to shift variants of influenza A virus leads to the rapid spread of infection throughout the world with an increase in the number of severe forms of the disease and deaths, as was predicted during the influenza pandemic in 2009 [3]. The virus that caused the pandemic had a unique, previously undescribed genome composition: 2 genes (NA and M) from the avian influenza virus, 5 genes (NA, NP, NS, PB2, RA) from the swine influenza viruses, and 1 gene (PB1) from the human influenza virus. The ability of influenza viruses to undergo antigenic variability determines the high susceptibility of the population and the main epidemiological features of this infection: widespread distribution, short intervals between epidemics (1–2 years for influenza A and 2–4 for influenza B), involvement of all age groups of the population in the epidemic process .
Influenza virus type C, which has only one surface antigen, the glycoprotein HA-esterase, is characterized by significantly greater stability of antigenic and other properties, as well as lower reproductive activity in cellular systems. The virus usually affects newborns and young children, causing lasting immunity. It has been established that antibodies to the influenza virus type C, which is associated with less than 1% of acute respiratory infections, are present in people of all age groups, with the exception of children in the first months of life.
The source of infection for influenza is mainly sick people in the acute period of the disease, including those with a mild or asymptomatic form, less often - convalescents who secrete the virus within two weeks from the onset of the disease, sometimes (in people with physiological [small children] or pathological [with chronic infections] immune deficiency until the 22–25th day for influenza A and until the 30th day for influenza B).
Humans can be infected with animal or avian influenza viruses. Currently, the highly pathogenic avian influenza A (H5N1) virus has spread widely in the countries of Southeast Asia and, in addition to devastating epizootics among wild and domestic birds, often causes an extremely severe form of the disease with a mortality rate of up to 50–60% in humans, but at the same time, fortunately, the absence of human-to-human transmission of the pathogen has limited its pandemic spread [4]. In 2003, an outbreak of influenza A (H7N7) was reported among birds in the Netherlands, followed by the development of infection in 86 poultry farm workers, one of whom died, and in 3 cases transmission of the virus through family contact was recorded [5]. In March 2013, cases of severe influenza with high mortality (out of 131 cases, 36 died) caused by the avian influenza A virus (H7N9), which is more transmissible from animal to human than the A virus (H5N1), were reported in several provinces of China [6]. According to the CDC (Centers for Disease Control and Prevention), in the fall of 2012, influenza diseases caused by a new strain of swine flu A H3N2v, first discovered in July 2011, including in its structure the M protein gene of the influenza virus, were reported in 13 US states H1N1pdm09 [7]. All sick people (307 people, mostly children) had contact with animals. Symptoms of the disease were characteristic of seasonal influenza (fever, cough, pharyngitis, rhinorrhea, myalgia and headache), but 1 death was also recorded. In isolated cases, transmission of the virus from person to person has been confirmed.
The pathogenesis of influenza is composed of a complex of processes that develop simultaneously or sequentially one after another at all stages of the reproduction of pathogens and their subsequent spread throughout the body, the main of which are (see figure):
1. Adsorption and introduction of influenza viruses into the epithelial cells of the respiratory tract (entry gate of infection), provided that they contain specific cellular receptors represented for the influenza virus by sialic acids of glycoproteins [8]. The reproduction of new virions is accompanied by a cytopathic (in relation to cells) effect, their destruction and rejection along with newly formed viruses. Immune defense reactions (early protective inflammatory response) are immediately activated, with the help of which the body tries to free itself from viruses. The leading role of immune reactions at the initial stage, along with secretory immunity factors, belongs to phagocytosis, carried out by cells of the mononuclear macrophage system (macrophages, polymorphonuclear leukocytes, monocytes, plasma and other cells, the chemotaxis of which increases in the lesion) [9]. An increase in the phagocytic activity of these cells is accompanied by a restructuring of their metabolism (increased ionic permeability of the cell membrane), increased glucose oxidation and hyperproduction of the generation of free radicals that have microbicidal, cytotoxic and proteolytic effects [10, 11]. At the same time, the processes of lipid peroxidation intensify with the release of a large amount of free energy necessary for the destruction of pathogens and the implementation of a full immune response. The complement system is activated, and the secretion of cytokines increases.
2. Penetration of pathogens, products of oxidative metabolic processes and destroyed epithelial cells into the bloodstream (viremia, toxinemia) with the development of vasopathy (systemic toxic or toxic-allergic reactions). The role of nitric oxide (NO), which is constantly formed in the endothelial cells of blood vessels and plays a key role in regulating their tone, while contributing to the inactivation of viruses, is also important. It has been shown that overproduction of NO is a sign of a rapid infection, and a deficiency in its formation is one of the reasons for the intracellular persistence of pathogens [12].
In case of severe infection, the possibility of reproduction of influenza viruses in endothelial cells of blood vessels with the development of endotheliosis (alternative inflammatory reaction) in the form of cellular necrosis and apoptosis, increased capillary permeability, and in the most critical cases – circulatory disorders has been proven [13, 14]. There is an imbalance between the processes of fibrinolysis, coagulation and anticoagulation, which results in the activation of blood clot formation processes [15]. It is possible to develop hemorrhagic capillary toxicosis, microthromboembolism, which in the form of congestive congestion of the brain and minor hemorrhages in the epicardium, pleura, lungs and other organs, accompanied by profound hemodynamic disorders, are a constant finding in the pathological examination of those who died from influenza in the first days of the disease. In this case, destructive and inflammatory changes are absent or mildly expressed [16].
3. Formation of an inflammatory focus with a dominant localization for the pathogen in the organs of the upper or lower parts of the respiratory tract. Mostly these are rhinitis, pharyngitis, tracheitis, laryngitis, bronchitis, as well as their combinations. One of the most severe variants of this process, which develops primarily with influenza caused by a new (pandemic) pathogen, is the development of massive pneumonia with acute respiratory distress syndrome (ARDS) and pulmonary edema [17].
4. Outcome: recovery, development of complications, death.
These stages correspond to clinical manifestations characteristic of influenza, the first of which usually appear after the end of the initial stages of pathogen reproduction, i.e., when they penetrate into the bloodstream (the second phase of the infectious process, which begins during the incubation period and persists throughout period of severe intoxication).
Influenza, including that caused by the new virus A (H1N1)pdm, usually begins against the background of complete health or after a short (1–2 hours) prodromal period with a characteristic predominance of the general intoxication syndrome over the symptoms of damage to the respiratory tract (Table 1) [ 18]. Body temperature already in the first hours reaches its maximum level (38.5–40.0 °C) with the simultaneous appearance of other symptoms of intoxication of varying severity: chills (muscle tremors), headache, dizziness, malaise, muscle pain, abdominal pain, joints, eyeballs, nausea, vomiting, sleep disturbances, sometimes hallucinations, delirium. The severity of this syndrome determines the severity of the disease, which can vary from mild to hypertoxic. In some cases, an increase in body temperature, mainly in the form of hyperthermia, may be the only manifestation of the disease. One of the first signs of the disease may be episodes of febrile seizures, which are most typical for children with congenital or acquired pathology of the nervous system.
In severe forms of influenza, the infectious process rapidly progresses with the development of an encephalic or meningoencephalic reaction (hyperthermia, delirium, cerebral disorders with convulsions, confusion or loss of consciousness, meningeal symptoms) and hemorrhagic syndrome (punctate or petechial rash, most often on the skin of the face, neck, chest and upper extremities; hemorrhages in the mucous membrane of the oral cavity, posterior wall of the pharynx, conjunctiva; nasal and uterine bleeding, microhematuria, blood in sputum and stool).
Hypertoxic forms of influenza are characterized by a lightning-fast onset and the development of various types of toxicosis: neurotoxicosis, infectious-toxic shock; Gasser syndrome (hemolytic-uremic with the development of DN and acute renal failure), Waterhouse-Friderichsen (acute adrenal insufficiency, adrenal hemorrhagic syndrome), Rey (toxic encephalopathy with fatty degeneration of internal organs, primarily the liver with the development of acute liver failure), Kisha (acute coronary insufficiency) and hemorrhagic syndrome (stage III DIC - hemocoagulation shock) with the appearance of edema and extensive hemorrhages in various organs (lungs, intestines, adrenal glands, brain), the development of ARDS, often against the background of leukemia and lymphopenia.
The maximum number of severe and complicated forms of the disease is observed mainly with influenza, caused by a new or significantly changed version of the virus. At the same time, influenza caused by the type A virus H1N1pdm09 had clinical symptoms typical of seasonal influenza: in the majority of patients, moderate intoxication was recorded against the background of elevated body temperature (≥ 37.5 ° C) (headache, myalgia, chills, adynamia, malaise ). Of the catarrhal symptoms, all patients suffered from a dry cough, as well as symptoms of tracheitis, nasopharyngitis, and laryngitis [19]. A characteristic feature of pandemic influenza A H1N1pdm09 was the frequent development of hemorrhagic syndrome (in adult patients with pneumonia, mainly in the form of hemoptysis (34.1–14.5 versus 13.1% of cases with seasonal influenza), and in children - nosebleeds (14.5 -7.1% versus 0 cases with seasonal influenza) In addition, as with influenza caused by avian H5N1 virus A, diarrhea and vomiting were recorded in 25–30% of cases.
The severity, duration and outcome of the disease also depend on the development of complications caused by both the impact of the virus and the addition of bacterial flora. The leading place belongs to acute pneumonia, which develops both at the onset of the disease and during the peak period with approximately the same frequency (in 5–8% of cases among those observed on an outpatient basis and in 12.3–18.5% of cases among hospitalized patients), most often with influenza caused by a new virus, which was observed mainly in adults during the 2009 pandemic (Table 2).
Among children, the development of stenosing laryngotracheitis predominated. An important influence on the nature of the course of influenza and the development of complications is exerted by the premorbid background, when aggravated by it (chronic cardiovascular, pulmonary and cerebral diseases, metabolic syndrome, etc.), as in pregnant women, a large number of severe and complicated forms of diseases are recorded, which was also observed during the 2009 pandemic. However, if with seasonal influenza a severe form developed only among patients with a complicated premorbid background, then with pandemic influenza - in a third of cases against a background of complete health, while in 50% of cases these patients required treatment in intensive care unit. The main principle of influenza therapy is early initiation immediately upon the appearance of the first symptoms of the disease, taking into account the severity, severity and localization of the process, the presence of complications, age and premorbid background of the patient (Table 3). Main groups of drugs:
- Etiotropic antiviral drugs – inactivate the pathogen, preventing its penetration into target cells and their subsequent reproduction;
- Interferons and their inducers are drugs that assist immunocompetent structures in inactivating pathogens;
- Syndromic, pathogenetically determined - aimed at preventing the occurrence and restoring an imbalance of adaptive and regulatory mechanisms, as well as dysfunction of individual organs;
- Immunorehabilitation – promoting the restoration of impaired immunity (or its individual components) in case of a complicated course of the disease or in persons with an unfavorable premorbid background.
Currently, there are few drugs with specific antiviral activity against influenza. These are ion channel blockers: Remantadine and its polymer derivative Orvirem; neuraminidase inhibitors - Tamiflu (oseltamivir), Relenza (zanamivir) and Peramivir; fusion inhibitor Arbidol; blocker of assembly of early viral proteins Ingavirin.
Unfortunately, in recent years, influenza viruses type A and B, including avian influenza A viruses H5N1 and H7N9, as well as influenza A virus H1N1pdm09, have shown resistance to Remantadine [5, 6], which, according to our data, remains and in 2013 (Table 4).
The sensitivity of all the studied viruses to neuraminidase inhibitors remains the same, including Tamiflu (oseltamivir), which has been successfully used for all etiological variants of influenza in patients older than one year and pregnant women, including during the A H1N1pdm09 pandemic.
It is worth noting the clinically proven effectiveness of the use of three chemotherapy drugs for pandemic influenza in children: oseltamivir, zanamivir and Arbidol (Table 5).
In practice, it was shown that there were no statistically significant differences in the duration of the main symptoms of the disease in patients receiving one or another chemotherapy drug, except for the duration of nasal discharge, which stopped faster with zanamivir. But in general, the inclusion of any of these drugs in influenza therapy turned out to be statistically significantly more effective than the use of basic (pathogenetic) therapy alone.
At the same time, it has been shown that if the use of oseltamivir is successful only for influenza, Arbidol can be used in the treatment of both influenza and ARVI of other etiologies [20, 21]. In addition, this drug was successfully used as a means of emergency prevention of influenza in families, including pregnant women who had contact with patients, preventing the development of severe forms of the disease in them [22–24].
In 2009, the Pharmaceutical Committee of the Russian Federation issued permission for the use by persons over 18 years of age of the antiviral drug Ingavirin (imidazolylethanamidepentanedioic acid), a blocker of the assembly of early viral proteins. Its activity has been proven against all influenza viruses, including A H1N1pdm09 [25].
Despite the positive results of using the listed chemotherapy drugs, they have age restrictions and there is no permission for their use in the treatment of influenza in children of the first year of life, for whom only the use of interferon alpha drugs is mainly possible. The rest of the therapy is syndromic, primarily detoxification, depending on the severity of intoxication, with the prescription of antioxidants, antipyretics, proteolysis inhibitors, agents for the treatment of lesions of the nasopharynx and other parts of the respiratory tract (upper and lower).
Thus, there should be no uncertainty complex. The start of therapy for influenza, as with any other infectious disease, should be early, taking into account the severity of the first symptoms. In this case, it is necessary to correctly assess the complaints of the patient or his parents, the general condition of the patient and all the identified symptoms of the disease. It is imperative to take into account the epidemic situation in the region and community where the patient was, his age and premorbid background, as well as the compatibility and individual tolerance of the prescribed drugs, the first of which should be etiotropic chemotherapy drugs or interferon drugs in children of the first year of life.