Methotrexate-Ebeve Solution, syringe, 1 piece, 0.75 ml, 7.5 mg, for injection
Side effect
According to WHO, adverse effects are classified according to their frequency as follows: very common (≥ .1/10), common (≥ .1/100 to less than 1/10), uncommon (≥ .1/1000 to less 1/100), rare (from ≥ .1/10,000 to less than 1/1000), very rare (less than 1/10,000). frequency unknown - based on available data, it was not possible to determine the frequency of occurrence. From the hematopoietic system: often - suppression of bone marrow function (leukopenia, thrombocytopenia, anemia). infrequently - pancytopenia. very rarely - severe progressive depression of bone marrow function, agranulocytosis. frequency unknown - megaloblastic anemia. From the central nervous system: often - drowsiness, headache, fatigue. infrequently - depression, confusion, mood changes. rarely - when using methotrexate in low doses - transient slight impairment of cognitive functions, unusual sensations in the cranial area. very rarely - pain, myasthenia gravis or paresthesia in the extremities, perversion of taste (metallic taste in the mouth), epileptic seizures, meningism, paralysis, insomnia. From the senses: often - visual impairment. uncommon - eye irritation. rarely - conjunctivitis. From the respiratory system: often - chronic interstitial pneumonitis (symptoms indicating potentially serious damage to the lungs with interstitial pneumonitis: dry, unproductive cough, shortening of breathing, increased body temperature). infrequently - alveolitis, pleural effusion. rarely - pulmonary fibrosis, Pneumocystis pneumonia, bronchial asthma. very rarely - pleural pain and thickening of the pleura (when treated with methotrexate in high doses), acute pulmonary edema. From the digestive system: very often - stomatitis, nausea, inflammation of the mucous membranes, loss of appetite, dyspepsia, anorexia, a significant increase in the activity of liver transaminases. often - diarrhea, ulceration of the oral mucosa. infrequently - enteritis, vomiting, liver cirrhosis, liver fibrosis, liver steatosis. rarely - ulceration of the gastrointestinal mucosa. very rarely - malabsorption syndrome, toxic megacolon. From the urinary system: infrequently - inflammation and ulceration of the bladder, impaired renal function, urinary disorders. rarely - renal failure, oliguria, anuria, electrolyte imbalance. From the skin: often - exanthema, erythema, itching. uncommon - photosensitivity, alopecia, herpes zoster, vasculitis, skin rashes herpetiformis, urticaria. rarely - increased pigmentation. very rarely - Stevens-Johnson syndrome, epidermal necrolysis (Lyell's syndrome). When exposed to ultraviolet radiation, increased psoriatic skin lesions, increased pigmentation of nails, acute paronychia, furunculosis and hidradenitis. From the musculoskeletal system: infrequently - arthralgia, myalgia, osteoporosis. From the cardiovascular system: often - vasculitis, bleeding of various locations. infrequently - effusion into the pericardial cavity. rarely - cardiac tamponade, nosebleeds. From the immune system: very often - decreased resistance to infections, pharyngitis. infrequently - hypogammaglobulinemia. rarely - sepsis. very rarely - anaphylactic reactions, increased number of rheumatoid nodules. From the reproductive system: infrequently - ulceration and inflammation of the vagina. very rarely - loss of libido, impotence, oligospermia, menstrual disorders, vaginal discharge. Other: often - chills, malaise, fever, necrosis. rarely - deterioration of wound healing. With intramuscular injection - a burning sensation or tissue damage (formation of a sterile abscess, destruction of adipose tissue) at the injection site. very rarely - benign, malignant and nonspecific neoplasms (including cysts and polyps), lymphomas, which in some cases regress after discontinuation of methotrexate. frequency unknown - diabetes, other metabolic disorders, sudden death. Adverse reactions with intrathecal methotrexate Acute: chemical arachnoiditis, manifested by headache, back or shoulder pain, stiffness of the muscles in the back of the neck and fever. Subacute: paresis (usually transient), paraplegia, impaired cerebellar function. Chronic: leukoencephalopathy, manifested by irritability, confusion, ataxia, muscle plasticity, sometimes convulsions, dementia, drowsiness, coma, in rare cases with death. When combining radiation therapy to the cranial area and intrathecal administration of methotrexate, the incidence of leukoencephalopathy increases.
Methotrexate: the great and the terrible
No, no, today we will not talk about the Great and Terrible Goodwin from the Emerald City) Methotrexate... Whatever is attributed to this drug, as soon as it is not called (dangerous chemotherapy, terrible poison and poison, and these are only the most modest epithets). The fear of methotrexate is sometimes even greater than the fear of rheumatic disease itself. Patients secretly hate him and dream of “getting off” him as quickly as possible, drawing in their imagination terrible pictures of irreparable harm to the body. Meanwhile, methotrexate is one of the main drugs used in rheumatology. So who is he: friend or enemy? To be afraid or to accept without fear? We'll figure it out today...
Among modern medications used to treat rheumatoid arthritis and other rheumatic diseases, methotrexate occupies a special place. Back in the early 80s of the last century, several clinical trials were conducted on the effectiveness of the drug at a dose of 7.5–15 mg/week, and later – up to 25 mg/week in patients with rheumatoid arthritis. The clinical efficacy of the drug and its dose dependence were assessed. Until the early 90s, methotrexate was considered as a reserve drug, treatment with which was started when other basic anti-inflammatory drugs (DMARDs) were ineffective. Currently, methotrexate has received the status of the “gold standard” among DMARDs used to treat rheumatoid arthritis, I think you have heard this phrase more than once. According to preliminary estimates, more than half a million (!) patients use methotrexate for the treatment of rheumatoid arthritis alone. The unique place of methotrexate in the treatment of rheumatoid arthritis is determined by many circumstances.
First, the effectiveness of methotrexate has been confirmed in a large number of open-label, controlled studies and observational studies. It has been shown that when treating with methotrexate, the effectiveness lasts longer and the toxicity is less pronounced than when using other basic drugs. In Russia, methotrexate has been used for the treatment of patients with rheumatoid arthritis, including its early variants, since 1984, the maximum duration of continuous therapy is 28 years (on average 14.8 years) (according to the Research Institute of Rheumatology). According to Australian rheumatologists, 75.4% of patients have been using methotrexate for more than 6 years and 53% for more than 12 years. Preliminary results indicate the pharmacoeconomic advantages of methotrexate over other basic anti-inflammatory drugs. In addition, there are studies that confirm lower mortality with long-term therapy with methotrexate compared to other basic drugs.
The unique place of methotrexate in the treatment of rheumatoid arthritis is determined by the fact that it is currently one of the most effective standard DMARDs and can be prescribed at any stage of arthritis. It is characterized by the highest duration of continuous use and simple dosing. Methorexate therapy is characterized by well-known and controlled (!!!) toxic reactions, as well as a relatively low cost of treatment.
Mechanism of action
The mechanism of action of methotrexate is based on its antifolate properties. The anti-inflammatory activity of relatively low doses of the drug (10–20 mg/week), in contrast to ultra-high doses (100–1000 mg/m2), is realized due to the activity of its derivatives, which can induce the formation of a powerful anti-inflammatory mediator - adenosine. The adenosine-dependent effects of methotrexate include a decrease in the synthesis of pro-inflammatory cytokines interleukin-6, -8, -10, tumor necrosis factor (TNF), etc. These effects allow methotrexate prescribed for the treatment of rheumatic diseases to be considered not as immunosuppressive (suppressive immunity), but more as an anti-inflammatory drug, which is confirmed by clinical practice. Methotrexate has obvious immunomodulatory activity, inhibiting the synthesis of pro-inflammatory substances and stimulating the synthesis of anti-inflammatory substances.
Pharmacological properties
When taken orally, methotrexate, undergoing some changes, enters the liver through the portal vein. After taking methotrexate at a dose of 10–25 mg, drug absorption ranges from 25 to 100% (average 60–70%). The maximum concentration of the drug in the blood is achieved after 2–4 hours. Although taking methotrexate with food slows the achievement of peak concentrations, its absorption and bioavailability are not affected, so the drug can be taken with food. Methotrexate binds to albumin and is excreted primarily by the kidneys (80%) and to a lesser extent by the liver (10–30%). The development of renal failure leads to a slowdown in the release of the drug and increases its toxicity. Methotrexate metabolites (that is, substances formed during the transformation process in the body) are found inside cells for ≥7 days after a single dose, which determines the frequency of taking the drug once a week.
Side effects
Side effects that develop during treatment with methotrexate can be divided into three main groups:
1) effects associated with folate deficiency (stomatitis, inhibition of hematopoiesis) can usually be corrected by administering folic or folinic acids and/or discontinuing methotrexate (temporary or permanent). The use of methotrexate without the prescription of folic acid is unacceptable!!!
2) allergic reactions, which sometimes disappear when treatment is interrupted. Harbingers of such reactions can be considered the appearance of an unmotivated dry cough with a rapid change in ambient temperature, for example, when going outside, or, conversely, shortness of breath;
3) reactions associated with the accumulation of active metabolites of the drug (liver damage). According to a meta-analysis of placebo-controlled randomized clinical trials (RCTs), the incidence of adverse reactions during treatment with methotrexate is approximately 22%, and in patients receiving placebo it is 7%.
Gastrointestinal tract
Nausea and vomiting usually appear 1–8 days after taking methotrexate and last 1–3 days, but can occur at any time during treatment. In this case, it is necessary to temporarily discontinue the drug and switch to subcutaneous administration of the drug. For mild nausea on the day of taking the drug and/or the next day, Motilium can be used situationally. Methotrexate may slow the scarring of gastric and duodenal ulcers, especially during concomitant use of nonsteroidal anti-inflammatory drugs (NSAIDs). Ulcerative lesions of the mucous membrane of the upper gastrointestinal tract are a relative contraindication for the use of methotrexate. On the other hand, methotrexate is the most common and accessible drug for the treatment of arthritis, so the detection of ulcerative lesions of the mucous membrane only indicates the need for targeted and thorough antiulcer treatment, and not the exclusion of methotrexate from therapy. Patients are often successfully treated with methotrexate for many years without recurrence of acute gastric ulcers, especially since with the effectiveness of methotrexate, NSAIDs can be discontinued and the source of stress ulcers, such as pain, decreases or disappears.
Liver
The most common side effect during therapy is a temporary increase in the level of aminotransferases (ALAT, AST) and alkaline phosphatase (ALP). As a rule, the concentration of aminotransferases reaches a maximum 4–5 days after taking the drug and persists for 1–2 weeks. A two-fold increase in aminotransferase levels is NOT a reason to discontinue methotrexate, whereas a more significant increase indicates the need to reduce the dose or interrupt treatment. With a multiple increase, in addition to the abolition of methotrexate, hepatoprotectors are usually prescribed. After normalization of aminotransferase levels, therapy is resumed at a lower dose, and subsequently the dose can be increased or left unchanged. Data regarding the likelihood of developing liver cirrhosis during treatment are contradictory. There are reports that liver damage during treatment with methotrexate is more common in patients with psoriasis. Liver changes during morphological examination are detected in only 3–11% of patients receiving methotrexate for more than 2 years, but liver cirrhosis develops very rarely (approximately 1 in 1000 patients). Regular monitoring of aminotransferase levels is considered sufficient as an early and reliable marker of liver damage. In this regard, the complete abstinence of patients from alcohol is of fundamental importance!!! People with psoriasis and psoriatic arthritis are more likely to have more severe liver damage and a higher rate of progression of liver damage than people with rheumatoid arthritis. Risk factors for liver damage during treatment include:
- alcohol consumption,
- lack of folic acid intake,
- total dose of methotrexate and duration of therapy,
- presence of diabetes mellitus,
- obesity,
- elderly age.
In patients with rheumatoid arthritis receiving methotrexate, aminotransferase levels should be monitored at least once every 3 months!
Methotrexate and viral hepatitis
A serious problem is the prescription of methotrexate in the presence of carriage of hepatitis B and/or C viruses. Determination of markers of hepatitis B and C is included in the standards for examining patients before prescribing methotrexate. However, when HBsAg or anti-HCV is detected, further studies to determine viremia and its severity are usually not carried out. Apparently, incomplete examination, as well as the lack of long-term observations, are often the reasons for a calm attitude towards prescribing methotrexate to such patients.
Hematopoietic system
Changes in blood parameters during methotrexate therapy are observed relatively rarely (no more than 1–3% of cases). Cases of leukopenia, thrombocytopenia, megaloblastic anemia, and pancytopenia have been described. Pancytopenia (that is, a decrease in all blood counts) is a deadly complication of therapy. The severity of this condition correlates with the dose of the drug, the presence of renal failure, concomitant infection, folic acid deficiency, and the combination of methotrexate with other toxic drugs. Unfortunately, taking folic acid does not prevent the development of pancytopenia. Elderly patients are at greatest risk of developing severe cytopenia. Normalization of hematopoiesis after discontinuation of the drug in most patients occurs within 2 weeks, but in some cases it becomes necessary to prescribe high doses of folate and even a colony-stimulating factor. In addition to cytopenia, that is, a decrease in blood counts, methotrexate in some cases can cause leukocytosis (that is, an increase in the level of white blood cells) without developing an infection.
Infectious complications during methotrexate therapy develop relatively often. These may be recurrent respiratory diseases, purulent bronchitis, and less often - unusually severe fungal and viral infections - nocardiosis, pulmonary aspergillosis and toxoplasmosis, herpes, cryptococcosis, Pneumocystis pneumonia. The development of severe infections is grounds for urgent withdrawal of methotrexate. But fortunately, according to several studies, long-term use of methotrexate is NOT associated with an increased risk of infectious complications.
Teratogenicity
Methotrexate is embryotoxic and has a teratogenic effect. Low doses of methotrexate can lead to the development of defects in the fetus, for example, the so-called “methotrexate syndrome”. Developmental delays and mental impairment have been described in children born to mothers who took the drug during pregnancy. Since even a single dose of methotrexate can cause defects in the fetus, this drug is contraindicated for pregnant women or women planning pregnancy! Methotrexate remains in the cells for a long time, so a washout period of at least 3–6 months is recommended before conception.
The cardiovascular system
An important advantage of methotrexate, which distinguishes it from other basic drugs, is the reduction in the risk of cardiovascular complications, which are the main cause of premature death in patients with rheumatoid arthritis. According to the literature and numerous studies in recent years, in patients with rheumatoid arthritis during treatment with methotrexate, there is a decrease in mortality from cardiovascular complications (up to 70%!!!) compared to patients receiving other DMARDs. It is believed that the beneficial effect of methotrexate on the cardiovascular system may be associated with increased formation of adenosine. However, many patients develop hypercholesterolemia (increased cholesterol levels in the blood), which requires the prescription of statins. Patients with rheumatoid arthritis often experience increased homocysteine concentrations and impaired homocysteine metabolism, regardless of treatment. Hyperhomocysteinemia is considered a risk factor for thrombosis. This indicates the need for long-term studies assessing all possible factors determining the development and progression of cardiovascular system pathology in patients.
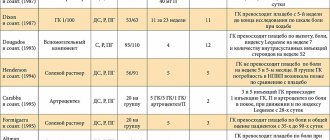
Flu-like syndrome or post-dose reactions
Cases have been described of the appearance 24 hours after taking methotrexate of pain in the joints and muscles, general malaise, sometimes accompanied by fever and lasting from 1 to 4 days. These reactions indicate the need to discontinue treatment and are considered the second most common cause after gastrointestinal symptoms. Some patients experience headache, memory loss, and photophobia. Unfortunately, many patients complain of headaches of varying severity and memory loss. This is another area that requires study and identification of approaches to reduce the incidence of adverse reactions. The currently very limited number of available and effective DMARDs makes it impossible to discontinue methotrexate in many patients with headache and/or complaints of some memory loss. At the same time, the development of a post-dose reaction in all cases requires discontinuation of the drug.
Methotrexate nodulosis
In patients receiving methotrexate, the development of subcutaneous nodules has been described, differing from rheumatoid nodules in smaller size and atypical localization, this is called methotrexate nodulosis (nodulation). Typically, these atypical nodules are localized on the hands. Methotrexate nodulosis can develop in patients who are seronegative for rheumatoid factor (RF) and during the period of remission of arthritis. There is evidence that the administration of hydroxychloroquine in most cases leads to regression of nodulosis.
Methotrexate for psoriatic arthritis
Methotrexate has been used to treat psoriatic arthritis since 1964. Compared with other basic drugs, methotrexate is well tolerated in this disease, and the frequency of treatment interruptions is lower than with other drugs. However, 10–30% of patients experience side effects that require discontinuation of the drug. Liver damage develops 3 times more often than when treating patients with rheumatoid arthritis with methotrexate. Methotrexate has long been used to treat severe forms of psoriasis and psoriatic arthritis. Currently, the dose of methotrexate is usually 20–30 mg/week, with a maintenance dose of 10–15 mg/week. Typically, the indications for prescribing methotrexate for psoriasis and psoriatic arthritis are as follows:
- malignant form of psoriatic arthritis;
- rapidly progressing course of the disease;
- high laboratory activity;
- development of severe skin variants of psoriasis (exudative, pustular, erythrodermic);
- low effectiveness or poor tolerability of NSAIDs and glucocorticoids;
- ineffectiveness of other DMARDs.
Still's disease in adults
Positive results were obtained from the use of methotrexate at a dose of up to 20 mg/week: improvement and development of remission of the disease, a significant reduction in the dose of hormonal drugs, positive dynamics of laboratory parameters.
Dermatomyositis/polymyositis
The effectiveness of methotrexate in the treatment of these diseases does not depend on the route of administration (oral or intravenous) and is 50–75%. Methotrexate is often used in combination with glucocorticoids. Therapy begins with a small dose (7.5–10 mg/week), which is increased to 25–30 mg/week. If oral methotrexate is poorly tolerated, an intravenous route of administration is prescribed. Other methods (subcutaneous, intramuscular) are unacceptable in these cases. The dose of the drug is reduced gradually under careful monitoring of clinical manifestations and CPK levels.
Polymyalgia rheumatica and giant cell arteritis
In elderly patients suffering from these diseases, in the treatment of which glucocorticoids are used, the administration of methotrexate in doses of 10–12.5 mg/week has been considered in a number of studies as an opportunity to more quickly reduce the dose of hormones and maintain remission.
Subcutaneous use of methotrexate
In clinical practice, methotrexate is most often used orally, but recently there has been a trend toward more widespread subcutaneous administration of the drug, especially at doses ≥20 mg/week. The theoretical rationale for subcutaneous methotrexate is the wide variability in its oral availability (20–80%), whereas the availability of subcutaneous methotrexate is much higher and more consistent. According to a number of authors, switching patients from parenteral to oral methotrexate led to an increase in the clinical activity of the disease in 49–71% of cases and the development of undesirable side effects (nausea, increased aminotransferase levels). When parenteral administration of methotrexate was resumed, the majority of patients experienced normalization of such disorders. RK Moitra et al. analyzed the results of parenteral use of methotrexate in 102 patients who had previously taken it orally for 3–135 months, and noted an increase in clinical effect and a decrease in ESR in approximately half of the patients. In 2010, methotrexate appeared in Russia in prefilled syringes for subcutaneous administration (Metoject), which opened up new opportunities for optimizing the treatment of rheumatoid arthritis.
In conclusion, I would like to highlight the following points:
- From the standpoint of evidence-based medicine, methotrexate is a DMARD that can be used in various types and durations of rheumatoid arthritis, in patients with undifferentiated arthritis, in early rheumatoid arthritis to achieve (induce) remission, in various rheumatic diseases.
- The sufficiently high effectiveness of the drug, the possibility of dose adjustment and the low frequency of intolerance reactions allow therapy to be carried out continuously for many years.
- The dose of methotrexate should be individualized, and therapy should be aimed at suppressing the activity and progression of the disease. Treatment should begin with a dose of 10-15 mg/week and increase by 5 mg every 2-4 weeks up to 25-30 mg/week depending on effectiveness and tolerability.
- Before prescribing methotrexate, risk factors for severe adverse reactions, including alcohol consumption, should be assessed.
- Treatment with methotrexate should be interrupted at least 3-6 months before the planned pregnancy.
- And, perhaps, the most important thing: the success and safety of methotrexate therapy, as with the use of other drugs, depend on the partnership between the doctor and the patient. If you have any doubts or questions, you can always contact your doctor, I won’t get tired of repeating this!!! If you believe in the success of treatment, you will definitely achieve it!