pharmachologic effect
Tiotropium-native is a long-acting m-anticholinergic blocker.
It has equal affinity for various muscarinic receptor subtypes from M1 to M5. The result of inhibition of M3 receptors in the airways is smooth muscle relaxation. The bronchodilator (bronchodilator) effect lasts for at least 24 hours and depends on the dose of tiotropium bromide. The significant duration of action is probably due to the very slow dissociation of tiotropium bromide from M3 receptors compared to ipratropium bromide. When administered by inhalation, tiotropium bromide as an N-quaternary anticholinergic agent has a local selective effect, while in therapeutic doses it does not cause systemic m-anticholinergic adverse reactions. Dissociation of tiotropium bromide from M2 receptors occurs faster than from M3. High affinity for receptors and slow dissociation cause a pronounced and long-lasting bronchodilator effect in patients with chronic obstructive pulmonary disease (COPD). Bronchodilation after inhalation of tiotropium bromide is a consequence of a local rather than a systemic effect.
Tiotropium bromide significantly increases lung function (forced expiratory volume in 1 second - FEV1 and forced vital capacity - FVC) 30 minutes after a single dose over 24 hours. Pharmacodynamic equilibrium is achieved during the first week, and a pronounced bronchodilator effect is observed on the third day.
Tiotropium bromide significantly increases morning and evening peak expiratory flow rates (PEF). The use of tiotropium bromide for a year does not cause a decrease in effectiveness in relation to bronchodilation.
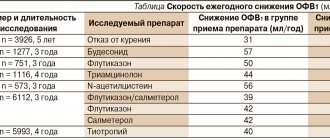
Tiotropium bromide significantly reduces shortness of breath throughout the entire treatment period, significantly improves exercise tolerance, significantly reduces the number of exacerbations of COPD and increases the time until the first exacerbation, and also significantly reduces the number of hospitalizations associated with exacerbation of COPD and increases the time until the first hospitalization . Tiotropium bromide results in a sustained improvement in FEV1 after four years of use, with no change in the rate of annual decline in FEV1.
There is evidence of a 16% reduction in the risk of death during treatment with tiotropium bromide, as well as evidence of an increase in time to first exacerbation with a 17% reduction in the risk of exacerbations when using tiotropium bromide compared to taking salmeterol.
Also, taking tiotropium bromide increases the time until the onset of the first severe (requiring hospitalization) exacerbation, and reduces the annual number of moderate or severe (requiring hospitalization) exacerbations.
Tiotropium-native, 30 pcs., 18 mcg, capsules with powder for inhalation
Tiotropium bromide is a quaternary ammonium compound, sparingly soluble in water.
Tiotropium bromide has linear pharmacokinetics within therapeutic limits after intravenous administration and dry powder inhalation.
When administered by inhalation, the absolute bioavailability of tiotropium bromide is 19.5%, which indicates the high bioavailability of the drug fraction reaching the lungs. Cmax in blood plasma is reached 5 minutes after inhalation. Tiotropium bromide is poorly absorbed from the gastrointestinal tract. For the same reason, food intake does not affect the absorption of tiotropium. When taking tiotropium bromide orally in solution form, the absolute bioavailability was 2-3%.
Plasma protein binding - 72%. Vd - 32 l/kg. At steady state, C max in blood plasma in patients with COPD is 17-19 pg/ml 5 minutes after inhalation of powder at a dose of 18 mcg and decreases rapidly. Css in blood plasma was 3-4 pg/ml.
Does not penetrate the BBB.
The degree of biotransformation is insignificant. Tiotropium bromide is broken down nonenzymatically to alcohol N-methylscopine and dithienylglycolic acid, which do not bind to muscarinic receptors.
Metabolic disturbances are possible when using inhibitors of CYP2D6 and 3A4 isoenzymes (quinidine, ketoconazole, gestodene). Thus, the isoenzymes CYP2D6 and 3A4 are included in the metabolism of the drug. Tiotropium bromide, even at supratherapeutic concentrations, does not inhibit cytochrome P450 isoenzymes 1A1, 1A2, 2B6, 2C9, 2C19, 2D6, 2E1 or 3A4 in human liver microsomes.
After inhalation administration, terminal T1/2 is 5-6 days. The total clearance when administered intravenously to healthy young volunteers is 880 ml/min, with an individual variability of 22%. Tiotropium bromide after intravenous administration is excreted mainly in the urine unchanged - 74%. After inhalation of the powder, renal excretion is 14%, the rest, not absorbed in the intestine, is excreted in the feces. The renal clearance of tiotropium bromide exceeds the CC, indicating tubular secretion of the drug. After long-term administration of the drug once a day in patients with COPD, the equilibrium state of pharmacokinetic parameters is achieved after 2-3 weeks, with no further cumulation observed.
In elderly patients, there is a decrease in the renal clearance of tiotropium bromide (326 ml/min in patients with COPD under 58 years of age, up to 163 ml/min in patients with COPD over 70 years of age), which is apparently due to a decrease in renal function with age. After inhalation, urinary excretion of tiotropium bromide is reduced from 14% (young healthy volunteers) to 7% (patients with COPD), but in elderly patients with COPD there was no significant change in plasma concentrations when inter- and intra-individual variability was taken into account (after inhalation of powder increases AUC0-4 by 43%).
If renal function is impaired after inhalation and intravenous administration, the concentration of the drug in the blood plasma increases and renal clearance decreases. With mild renal impairment (creatinine clearance 50-80 ml/min), often observed in elderly patients, the increase in the concentration of tiotropium bromide in the blood plasma is insignificant (after intravenous administration, an increase in AUC0-4 by 39%). In patients with COPD with moderate or severe decrease in renal function (creatinine clearance <50 ml/min), after intravenous administration of ipratropium bromide, a double increase in its plasma concentration was observed (82% increase in AUC0-4), compared with plasma concentrations blood, determined after inhalation administration of dry powder.
Directions for use and doses
Tiotropium native is prescribed in the form of inhalations, one capsule per day at the same time, using the Inhaler CDM® inhaler.
The drug should not be swallowed.
Tiotropium native should be used no more than once a day.
Elderly and older patients and patients with impaired renal or liver function can take Tiotropium-native in recommended doses. However, careful monitoring is necessary for patients with moderate or severe renal impairment receiving Tiotropium native in combination with other drugs excreted mainly by the kidneys.
special instructions
Tiotropium native as a bronchodilator used once daily for maintenance treatment is not intended for initial therapy in acute bronchospasm attacks, i.e. in urgent cases.
After inhalation of the drug Tiotropium-native, immediate hypersensitivity reactions may develop. Like other inhaled drugs, Tiotropium native can cause paradoxical bronchospasm.
Patients should be familiar with the rules for using Tiotropium-native capsules using an inhaler.
Do not allow the powder to get into your eyes. Eye pain or discomfort, blurred vision, visual halos in combination with eye redness, conjunctival congestion and corneal edema may indicate an acute attack of angle-closure glaucoma. If any combination of these symptoms develops, you should contact your doctor immediately. The use of drugs that cause miosis is not an effective treatment in this case.
Tiotropium native should not be used more than once daily.
Tiotropium-native capsules should only be used with the Inhaler CDM® inhaler.
The use of Tiotropium-native does not affect the results of doping tests in athletes.
No studies have been conducted to study the effect of the drug Tiotropium - native on the ability to drive vehicles and operate machinery. In the event of the development of such undesirable reactions as dizziness, headache and blurred vision, it is necessary to refrain from driving vehicles and operating machinery, as well as from engaging in other potentially hazardous activities that require increased concentration and speed of psychomotor reactions.
Tiotropiui-Nativ caps spor d/ing 18mkg No. 30
Additional information: Drug type medicinal product
Pharmacological group m-long-acting anticholinergic
Prescription drug yes
Active ingredient: tiotropium bromide monohydrate
Capsule release form
Area of application for pulmonary diseases
Pharmacological action : bronchodilator
Indications for use : maintenance therapy in patients with COPD, including chronic bronchitis and emphysema (maintenance therapy for persistent shortness of breath and to prevent exacerbations
Composition per 1 capsule: active substance: tiotropium bromide monohydrate 22.5 mcg (in terms of tiotropium) (18 mcg); excipients: sodium benzoate 20 mcg, lactose monohydrate 10 mg, hard capsules No. 3: hypromellose
Interaction is possible when using the drug Tiotropium-native in combination with other drugs commonly used to treat COPD: sympathomimetics, methylxanthines, oral and inhaled glucocorticosteroids; combined use with long-acting 2-agonists, inhaled glucocorticosteroids and their combinations does not affect the effect of tiotropium bromide; chronic concomitant use of other anticholinergic drugs and Tiotropium-native has not been studied and is therefore not recommended
Contraindications: hypersensitivity to atropine or its derivatives (including ipratropium and oxitropium) and/or to other components of the drug (in particular, to lactose monohydrate, which contains milk protein, with lactase deficiency, lactose intolerance, glucose-galactose malabsorption) ; I trimester of pregnancy; age up to 18 years
Dosage Tiotropium-native is prescribed in the form of inhalations, one capsule per day at the same time, using the Inhaler CDM inhaler; the drug should not be swallowed; Tiotropium-native should be used no more than once a day
Use in Pregnancy should not be used in pregnant or breastfeeding women unless the expected benefit outweighs the possible risk to the fetus or child.
effects of immune system disorders: rarely - urticaria, hypersensitivity reactions, including immediate reactions, angioedema (Quincke's edema); frequency unknown - anaphylactic reactions; metabolic and nutritional disorders: frequency unknown – dehydration; Nervous system disorders: uncommon - dizziness, headache, taste disorder; rarely – insomnia; visual disturbances: infrequently - blurred vision; rarely - increased intraocular pressure, glaucoma; cardiac disorders: infrequently - atrial fibrillation; rarely - tachycardia (including supraventricular tachycardia), palpitations; disorders of the respiratory system, chest and mediastinal organs: infrequently - dysphonia, cough, pharyngitis; rarely - paradoxical bronchospasm, laryngitis, sinusitis, nosebleeds; disorders of the gastrointestinal tract: often - dry mouth, usually mild; uncommon - constipation, gastroesophageal reflux, oropharyngeal candidiasis; rarely - nausea, stomatitis, gingitis, glossitis, intestinal obstruction, including paralytic ileus, dysphagia; frequency unknown – caries; disorders of the skin and subcutaneous tissues: infrequently - rash; rarely - itching; frequency unknown - infectious skin diseases, skin ulcers, dry skin; Musculoskeletal and connective tissue disorders: frequency unknown - joint swelling; disorders of the kidneys and urinary tract: infrequently - difficulty urinating and urinary retention (in men with predisposing factors), dysuria; rarely - urinary tract infection
Overdose when using high doses of tiotropium bromide may cause minor manifestations of systemic anticholinergic effects; however, systemic anticholinergic adverse reactions were not observed after a single inhaled dose of tiotropium bromide up to 340 mcg in healthy volunteers; when tiotropium bromide was used in doses up to 170 mcg by healthy volunteers for 7 days, no relevant adverse reactions were observed, with the exception of dry mouth; There is evidence that when tiotropium bromide was used by patients with COPD at a maximum daily dose of 43 mcg for more than 4 weeks, no significant adverse reactions were observed; acute intoxication associated with accidental ingestion of capsules is unlikely due to the low bioavailability of tiotropium bromide
Storage conditions : protected from light, at a temperature not exceeding 25°C, out of the reach of children
Special instructions: Do not allow the powder to get into your eyes; eye pain or discomfort, blurred vision, visual halos in combination with eye redness, conjunctival congestion and corneal edema may indicate an acute attack of angle-closure glaucoma; If any combination of these symptoms develops, you should immediately consult a doctor; the use of drugs that cause miosis is not an effective treatment in this case