Home | About us | Delivery | Advertisers | Login | Registration
The pharmacy is closed on Sundays and holidays.
- Medicines
- dietary supplementsVitamins
- Categories from A to Z
- Brands from A to Z
- Products from A to Z
- Medical equipment
- beauty
- Child
- Care
- Honey products appointments
- Herbs and herbal teas
- Medical nutrition
- Journey
- Making medicinesStock
Pharmacy online is the best pharmacy in Almaty, delivering medicines to Almaty. An online pharmacy or online pharmacy provides the following types of services: delivery of medicines, medicines to your home. Online pharmacy Almaty or online pharmacy Almaty delivers medicines to your home, as well as home delivery of medicines in Almaty.
my basket
Apteka84.kz is an online pharmacy that offers its customers medicines, medicinal and decorative cosmetics, dietary supplements, vitamins, baby food, intimate products for adults, medical equipment and thousands of other medical and cosmetic products at low prices. All data presented on the Apteka84.kz website is for informational purposes only and is not a substitute for professional medical care. Apteka84.kz strongly recommends that you carefully read the instructions for use contained in each package of medicines and other products. If you currently have any symptoms of the disease, you should seek help from a doctor. You should always tell your doctor or pharmacist about all the medicines you take. If you feel you need further help, please consult your local pharmacist or contact our GP online or by telephone.
© 2021 Pharmacy 84.
SPIRIVA RESPIMAT
Pharmacokinetics
Tiotropium bromide is a quaternary ammonium derivative, sparingly soluble in water.
Tiotropium bromide is available as an inhalation solution, which is used with the RESPIMAT inhaler. Approximately 40% of the inhalation dose is deposited in the lungs, the rest enters the gastrointestinal tract. Some pharmacokinetic data described below were obtained using doses higher than those recommended for treatment.
Suction
After inhalation of the solution by young healthy volunteers, it was found that about 33% of the inhalation dose enters the systemic circulation. Taking pitti does not affect the absorption of tiotropium bromide, due to this. that it is poorly absorbed from the gastrointestinal tract.
Absolute bioavailability when taken orally is 2 - 3%. The maximum concentration in plasma is observed 5-7 minutes after inhalation. At the dynamic equilibrium stage, the peak plasma concentration of tiotropium in patients with COPD is 10.5 pg/ml and decreases rapidly. This indicates a multicompartmental type of drug distribution. At the stage of dynamic equilibrium, the basal concentration of tiotropium in the blood plasma is 1.6 pg/ml. At the stage of dynamic equilibrium, the peak concentration of tiotropium in blood plasma in patients with bronchial asthma was 5.15 pg/ml and was achieved after 5 minutes. Distribution
The binding of the drug to plasma proteins is 72%; volume of distribution 32 l/kg. Studies have shown that tiotropium bromide does not penetrate
blood-brain barrier. Biotransformation
The degree of biotransformation is insignificant. This is confirmed by the fact that after intravenous administration of the drug to young healthy volunteers, 74% of the substance tiotropium bromide in unchanged form is found in the urine. Tiotropium bromide is an ester that is cleaved into ethanol-M-methylscopine. and dithienylglycolic acid; these compounds do not bind to muscarinic receptors.
in vitro studies
it has been shown that some part of the drug (<20% of the dose after intravenous administration) is metabolized by oxidation by cytochrome P450, followed by conjugation with glutathione and the formation of various metabolites. This mechanism can be inhibited by inhibitors of the CYP450 isoenzymes 2D6 and 3A4, quinidine, ketoconazole and gestodene. Thus, CYP450 2D6 and 3A4 are involved in metabolism. Tiotropium bromide, even at supratherapeutic concentrations, does not inhibit cytochrome P450 1A1, 1A2, 2B6, 2C9, 2C19, 2D6, 2E1 or 3A in human liver microsomes.
Removal
The terminal half-life of tiotropium bromide after inhalation is 27 to 45 hours in patients with COPD. In patients with asthma, the effective half-life after inhalation is 34 hours.
The total clearance after intravenous administration of the drug to young healthy volunteers was 880 ml/min. Tiotropium bromide after intravenous administration is mainly excreted unchanged by the kidneys (74%). After inhalation of the solution in patients with COPD, renal excretion is 18.6% (0.93 mcg), the remaining unabsorbed portion is excreted through the intestine. At the pharmacokinetic equilibrium stage in patients with asthma, 11.9% (0.595 mcg) of the dose is excreted unchanged in the urine 24 hours after taking the drug. The renal clearance of tiotropium bromide exceeds the clearance of creatinine, indicating its tubular secretion. After long-term inhalation administration of the drug once a day by patients with COPD, pharmacokinetic equilibrium is achieved on day 7; however, no further accumulation is observed.
Tiotropium bromide has linear pharmacokinetics within therapeutic limits after intravenous administration, dry powder inhalation and solution inhalation. Pharmacokinetics in elderly patients
In old age, there is a decrease in renal clearance of tiotropium
(347 ml/min in patients with COPD under the age of 65 years and 275 ml/min in patients with COPD and asthma over 65 years of age), It has been established that in patients with bronchial asthma, the effect of tiotropium bromide does not depend on the age of the patients.
Patients with impaired renal function
After inhaled once-daily administration of tiotropium during steady-state pharmacokinetics in patients with COPD and mild renal impairment (creatinine clearance 50-80 ml/min), there was a slight increase in AUC0-6.ss by 1.8-30% and Cmax ,Ss compared with patients with normal renal function (creatinine clearance >80 ml/min). In patients with COPD and moderate to severe renal impairment (creatinine clearance <50 mL/min), intravenous tiotropium bromide resulted in a twofold increase in total exposure (AUC0-44 increased by 82% and Cmax increased by 52%) compared with patients with COPD and normal renal function. A similar increase in plasma concentration was noted after inhalation of the dry powder.
In patients with bronchial asthma and mild renal impairment (creatinine clearance 50-80 ml/min), inhaled tiotropium bromide did not lead to a significant increase in exposure compared to patients with normal renal function.
Patients with liver dysfunction
It is assumed that liver failure does not have a significant effect on the pharmacokinetics of tiotropium bromide, since tiotropium bromide is primarily excreted by the kidneys and by non-enzymatic cleavage of the ester bond to form derivatives that do not have pharmacological activity.
Pharmacological properties of the drug Tiotropium bromide
Anticholinergic, bronchodilator . As a result of inhibition of M3 receptors in the respiratory tract, bronchial smooth muscles relax. High affinity for receptors and slow dissociation from M3 receptors determine a pronounced and long-lasting bronchodilator effect when applied topically in patients with COPD. When administered by inhalation, the absolute bioavailability of tiotropium bromide is 19.5%. Due to its chemical structure (quaternary ammonium compound), tiotropium bromide is poorly absorbed from the gastrointestinal tract. For the same reason, food intake does not affect the absorption of tiotropium bromide. The maximum concentration in the blood serum after inhalation of the powder at a dose of 18 mcg is achieved after 5 minutes and is 17–19 pg/ml in patients with COPD, the equilibrium concentration in the blood plasma is 3–4 pg/ml. Plasma protein binding is 72%, volume of distribution is 32 l/kg. Does not penetrate the BBB. Biotransformation is insignificant, which is confirmed by the fact that after intravenous administration of the drug to young healthy volunteers, 74% of unchanged tiotropium is found in the urine. Tiotropium is broken down non-enzymatically to the alcohol N-methylscopine and dithienylglycolic acid, which do not bind to muscarinic receptors. Even at ultra-high doses, tiotropium does not inhibit cytochrome P450, 1A1, 1A2, 2B6, 2C9, 2C19, 2D6, 2E1 or 3A in human liver microsomes. After inhalation, the terminal half-life is 5–6 days, excreted by the kidneys (14% of the dose), the rest, not absorbed in the intestine, is excreted in feces. The bronchodilator effect is a consequence of local rather than systemic action, depends on the dose and lasts for at least 24 hours. The use of tiotropium significantly improves pulmonary function 30 minutes after a single inhalation for 24 hours. An equilibrium state was achieved during the first week, and a pronounced bronchodilator the effect was observed on the 3rd day. Evaluation of the bronchodilator effect over the course of a year did not reveal any manifestation of tolerance. Reduces the number of exacerbations of COPD, increases the period until the first exacerbation compared with placebo, improves quality of life throughout the treatment period, reduces the number of hospitalizations associated with exacerbation of COPD and increases the time until the first hospitalization.
Chronic obstructive pulmonary disease (COPD) is a progressive disease with incompletely reversible bronchial obstruction that occurs under the influence of various factors (the main one being smoking) [1]. According to a number of recent studies, the global prevalence of COPD among people over 40 years of age is 10.1% (11.8% of men and 8.5% of women) [3]. In the Russian Federation, about 16 million people suffer from COPD [3]. COPD is one of the most pressing medical and social problems. This is due not only to the widespread prevalence of the disease, but also to the high risk of serious complications that lead to disability and mortality, including among the working population [1].
Modern therapy for COPD
The current level of development of clinical medicine makes it possible to effectively influence the course of COPD. The range of medications recommended as long-term maintenance therapy for COPD includes short- and long-acting bronchodilators, inhaled glucocorticosteroids (ICS), combination drugs (ICS/long-acting β2-agonists), antioxidants (N-acetylcysteine) and vaccines [1 , 4]. A special place among drugs used in the treatment of stable COPD is occupied by long-acting bronchodilators (LABAs). According to the GOLD (Global Strategy of Chronic Obstructive Lung Disease) guidelines, LABAs are more effective and convenient than short-acting bronchodilators (SABAs) (level of evidence A) [1]. Currently, only three drugs are classified as LABAs: formoterol, salmeterol (long-acting β2-agonists - LABAs) and tiotropium bromide (long-acting anticholinergic drug - LDACP).
The advantage of tiotropium bromide (Spiriva) lies in its selectivity towards M1 and M3 receptors and the long duration of its action [5, 6]. The drug provides bronchodilation and protection against cholinergic bronchoconstrictor stimuli for 24 hours, which makes it possible to use it once a day. These properties of the drug significantly simplify the dosage regimen and improve patient adherence to therapy.
The increase in functional pulmonary parameters of patients with COPD during tiotropium therapy in all studies exceeded that of patients receiving comparator drugs, and this improvement was maintained throughout the entire study period without the development of tachyphylaxis [7]. Tiotropium was the first drug with a positive effect on pulmonary hyperinflation confirmed by randomized controlled trials (RCTs) [8]. Improvement in functional parameters during tiotropium therapy was accompanied by an improvement in the clinical picture, exercise tolerance, quality of life of patients, and a decrease in the frequency of dosing with CBD [6]. Among patients taking tiotropium, there was a lower number of exacerbations of COPD, a significant increase in the time to the first exacerbation, and a decrease in the number of hospitalizations [6].
According to modern international and national recommendations for the treatment of COPD, any of the LABDs - tiotropium or formoterol, or salmeterol - should be prescribed to all patients with COPD, starting with moderate severity of the disease (stage II according to the GOLD classification) [1]. Are there differences between these drugs?
Of course, today tiotropium is the only drug with 24-hour action, and it is considered, perhaps, the most studied drug for COPD [1]. However, over the coming years, new ultra-long-acting drugs (at least 24 hours) will appear in our arsenal of drugs for the treatment of COPD, both LABA (indacaterol, carmoterol, milveterol, etc.) and DDACP (aclidinium bromide, darotropium bromide, glycopyrrolium bromide, etc. ) [9]. Thus, the first studies on the new LABA, indacaterol, demonstrated that the new drug, like tiotropium, improves functional pulmonary parameters, symptoms, physical performance, quality of life in patients with COPD, and reduces the number of exacerbations of the disease [10–19].
However, tiotropium therapy alone has demonstrated the following benefits, not yet shown in studies of all other known LABDs:
- slowing the progression of COPD;
- reducing mortality in patients with COPD;
- reducing the risk of cardiovascular events;
- high efficiency in all studied COPD phenotypes.
Tiotropium therapy slows the progression of COPD
The progression of obstructive pulmonary diseases is usually assessed by the rate of decline in forced expiratory volume in 1 second (FEV1), in healthy people it is about 20–30 ml/year, in patients with COPD – 40–80 ml/year [20, 21]. To assess the rate of disease progression, it is necessary to study a large number of patients (usually more than 100 people) over a fairly long period of time (several years) [22].
For a long time, the only intervention capable of stopping the progression of COPD was early smoking cessation [23, 24]. The global study UPLIFT (Understanding the Potential Long-term Impacts on Function with Tiotropium) was devoted to studying the impact of long-term maintenance therapy with tiotropium on the clinical course of COPD (annual decline in functional indicators, quality of life, frequency of exacerbations and mortality of patients) [25]. The UPLIFT study had a randomized, controlled, double-blind design, lasted 4 years, involved 490 study sites from 37 countries, and included a total of 5993 COPD patients. In this study, all patients were randomized into two treatment groups: tiotropium 18 mcg once daily (2986 patients) or placebo (3006 patients). The study design was as close as possible to “real life” conditions, i.e., patients who took part in the study were allowed to take any drugs (including ICS, LABAs and theophyllines), with the exception of anticholinergics (ACP).
Although several 1-year studies have shown encouraging results in slowing the progression of COPD with tiotropium compared with ipratropium [26] or placebo, [27] the UPLIFT study assessed the entire COPD cohort and found no difference between groups in the rate of change in FEV1. . At the same time, it is noteworthy that the annual decrease in post-bronchodilator FEV1 (42 ml/year) even in the placebo group was less [25] than in other known studies (47–69 ml/year) (see table) [ 28–33].
How can the results be explained?
The nearly “normal physiological” annual changes in functional outcomes in the UPLIFT study can be explained in terms of the “real life” study design. As already mentioned, in this study the use of any medications (except ACP) was allowed; as a result, more than 70% of COPD patients took both ICS and LABA [25]. It is possible that such complex therapy, as well as active therapy for exacerbations of the disease themselves, could slow down the progression of COPD and the further addition of other drugs (tiotropium) did not lead to another slowdown in the decline in FEV1, since this indicator no longer differed from the “norm”, i.e. n. ceiling effect. The validity of this position is confirmed by a subgroup analysis, which showed significant differences between the tiotropium and placebo groups in the rate of annual decline in FEV1 in patients who did not receive either ICS or LABA (40 versus 47 ml/year, p = 0.046) [25].
In addition, in the UPLIFT study, the proportion of current smokers was only 30%, which is significantly lower compared to other studies (38–90%), and an additional 26% of patients changed their smoking status during the course of the study (the majority quit smoking). Another explanation for the lack of differences between groups in the rate of change in functional indicators was the higher risk of dropout from the study of patients taking placebo [25].
The UPLIFT study, due to its large sample size of patients, also made it possible to evaluate the effectiveness of tiotropium therapy in certain groups of COPD patients: patients with early stages of COPD, “naive” patients (i.e., who have never received any therapy for COPD), and patients under 50 years of age. It turned out that it is in these subtypes (phenotypes) that COPD therapy with tiotropium demonstrates a statistically significant slowdown in the rate of annual decline in FEV1 [34–36].
Among patients with COPD stage II, the rate of decline in post-bronchodilator FEV1 was significantly lower in the tiotropium group compared to the control group (43 versus 49 ml per year; p = 0.024; Fig. 1) [34]. For patients who had never received any therapy for COPD, the annual decline in post-bronchodilator FEV1 was slower than for patients receiving tiotropium (42 vs. 53 ml per year; p = 0.026), compared with control patients (Fig. 2 ) [35].
Even more impressive results were obtained from COPD patients under 50 years of age: the rate of decline in post-bronchodilator FEV1 in the tiotropium and control groups was 38 and 58 ml/year, respectively (p < 0.05) (Fig. 3) [36].
Thus, this subgroup analysis of the UPLIFT study showed that in patients with stage II COPD, “naive” patients and in patients under 50 years of age, taking tiotropium reduces the rate of decline in post-bronchodilator FEV1, i.e., it slows down the progression of COPD.
Tiotropium therapy reduces mortality in patients with COPD
COPD is one of the leading causes of morbidity and mortality in modern society; mortality from COPD ranks 4th among all causes of death in the general population [37]. Moreover, mortality from COPD is constantly increasing [38]. According to WHO experts, by 2021 COPD will rank third among all causes of mortality and first among all causes of disability in adults [38, 39].
Therapy that can reduce mortality in patients with COPD includes:
- long-term oxygen therapy (for severely ill patients with hypoxemia) [40, 41];
- smoking cessation (in the early stages of COPD) [42];
- surgical reduction of lung volume (patients with predominantly localized emphysema in the upper sections and low tolerance to physical activity) [43];
- non-invasive ventilation (for severe exacerbation of COPD) [44].
As for drugs, there is some reason to believe that modern drugs used in the treatment of COPD (and capable of improving functional parameters, reducing the number of exacerbations, slowing down the progression of the disease) can also reduce the mortality of patients.
An important achievement of the UPLIFT study was the evidence of a reduction in mortality in patients with COPD when taking tiotropium. When using tiotropium during the treatment of patients with COPD, there was a significant reduction in the relative risk of death by 16% (p < 0.05). This effect persisted until the end of the protocol-defined treatment period (day 1440) - in the intention-to-treat analysis, a significant reduction in the risk of death by 13% was noted (p < 0.05). But this effect was not statistically significant: the relative risk of death was reduced by 11% (p = 0.09) during the 30-day post-study follow-up period (day 1470), when patients stopped taking the study drug as per protocol.
It is noteworthy that the possibility of reducing mortality in patients with COPD while taking tiotropium has been shown in other recent studies.
A meta-analysis by Salpeter et al., combining the results of 22 RCTs involving patients with COPD, showed that ACPs (ipratropium and tiotropium) reduced the incidence of severe exacerbations of COPD by 33%, and respiratory mortality by 73% compared with placebo [45]. The absolute reduction in the risk of respiratory death when using ACP was 0.36% per year.
In a population-based cohort study based on a Danish health database and including 2870 COPD patients treated with tiotropium and 7773 COPD controls, all causes of death were analyzed over 6 years [46]. It turned out that taking tiotropium is associated with a significant reduction in the risk of death in patients with COPD from all causes (relative risk [RR] = 0.77; 95% confidence interval [CI] - 0.65–0.91) and there was no increase in risk of death in patients from heart failure (RR = 0.84, 95% CI – 0.41–1.75) or acute myocardial infarction (AMI) (RR = 1.25, 95% CI – 0.49–3.17) .
Tiotropium therapy reduces the risk of cardiovascular events
Large epidemiological studies have demonstrated that the leading cause of mortality in patients with mild/moderate COPD remains not only respiratory failure, as traditionally believed, but also cardiovascular diseases - coronary heart disease and heart failure [47, 48]. According to population studies, in patients with COPD the risk of cardiovascular death is increased by 2–3 times and accounts for approximately 50% of the total number of deaths [49, 50].
ACP (ipratropium and tiotropium) have minimal cardiovascular effect; they are not absorbed from the mucous membranes of the respiratory tract and therefore do not cause systemic side effects inherent in atropine (tachycardia, arrhythmias). Unlike β2-agonists, ACPs do not induce tachycardia or increased cardiac output in patients with COPD, do not worsen the ventilation-perfusion balance, and do not aggravate hypoxemia [51].
Relatively recently, a study was published that called into question generally accepted ideas about the cardiovascular safety of ACP.
In a meta-analysis by Singh et al., which included a total of 17 RCTs (14,783 patients with COPD), the authors concluded that the use of anticholinergic drugs (ipratropium or tiotropium) leads to an increased risk of cardiovascular events (RR = 1.58, 95% CI – 1.21–2.06), AMI (RR = 1.53, 95% CI – 1.05–2.23) and cardiovascular mortality in patients with COPD (RR = 1.80, 95% CI – 1.17–2.77) [52]. Because this meta-analysis had serious design flaws and the validity of its conclusions was questioned, data from more well-designed studies were needed to confirm or refute the cardiovascular risk of DDACP. Therefore, the appearance of the results of the UPLIFT study could not have come at a better time, since the data from this study demonstrated that tiotropium not only does not increase the risk of cardiovascular events and mortality, but, on the contrary, reduces the risk of mortality from cardiovascular causes (by 27%) and the number of serious cardiovascular adverse reactions (by 16%). AMI occurred in 67 patients receiving tiotropium and in 85 patients receiving placebo (HR = 0.73, 95% CI - 0.53-1.00), stroke was observed in 82 patients in the tiotropium group and in 80 patients in the placebo group (RR = 0.95, 95% CI – 0.70–1.29). It should be noted that taking tiotropium significantly reduced the number of episodes of respiratory failure (RR = 0.69, 95% CI – 0.52–0.92).
The most comprehensive to date is a recent meta-analysis by Celli et al., based on all RCTs (n = 30) on the use of tiotropium in patients with COPD (n = 19,545) [53]. The incidence of all deaths during treatment with tiotropium was 3.44, placebo – 4.10 per 100 patient-years (RR = 0.88, 95% CI – 0.77–0.999). Patients taking tiotropium were significantly less likely to develop cardiovascular events: 2.15 versus 2.67 (placebo) per 100 patient-years (RR = 0.83, 95% CI – 0.71–0.98) and fatal cardiovascular events: 0.91 vs 1.24 (placebo) per 100 patient-years (RR = 0.77, 95% CI - 0.60-0.98). For all cases of AMI, heart failure, and stroke, the ORs (95% CI) were 0.78 (0.59–1.02), 0.82 (0.69–0.98), and 1.03 (0.79 –1.35) respectively.
Thus, tiotropium therapy reduces the risk of cardiovascular events, all-cause mortality, and cardiovascular mortality in patients with COPD.
Tiotropium therapy is highly effective in all COPD phenotypes studied
Today, many experts and practitioners share the view that COPD is a syndrome comprising a group of obstructive diseases that share similar features, such as the inhalational source of injury, and certain differences, such as the mechanisms of disease development and response to therapy [54].
The discussion about the need to identify different sub- or phenotypes of COPD has been going on for quite a long time [55], but only over the past two years have there been significant changes in defining the problem of heterogeneity of the disease [56].
It should be recognized that for COPD the concept of “phenotype” is relatively new and there is no generally accepted definition of the “COPD phenotype” yet. More recently, a group of experts has proposed a definition of COPD phenotype: “a characteristic feature or combination of such features that describes differences between patients with COPD that are associated with clinically relevant outcomes (symptoms, exacerbations, response to therapy, rate of disease progression, or death)” [57]. Ideally, individuals included in the same phenotype and demonstrating similar clinical outcomes should also demonstrate a similar therapeutic response profile due to similar biological or pathophysiological mechanisms. Identification and subsequent grouping of key elements of the COPD syndrome into clinically significant and useful subgroups (phenotypes) will allow more effective therapy for patients with COPD [57].
A recent study by Lee et al. It was found that in COPD, ICS/LABA therapy is most effective for patients with a predominantly obstructive (bronchitis) variant of COPD - they had the greatest increase in FEV1 and a more pronounced decrease in dyspnea, but was ineffective in the predominantly emphysematous variant of COPD [58]. At the same time, in the study by Gelb et al. It has been shown that the effectiveness of tiotropium therapy in patients with COPD does not depend on the severity of their emphysema [59].
Subgroup analyzes of the UPLIFT study made it possible to study the effectiveness of tiotropium therapy in individual subtypes (phenotypes) of COPD patients [35, 36, 60, 61]. As already mentioned, administration slowed the progression of COPD in patients, “naive” patients and in patients under 50 years of age [35, 36]. In addition, regardless of the COPD phenotype (“naïve” patients, patients under 50 years of age, smokers, former smokers, men and women), tiotropium therapy led to a noticeable, persistent improvement in FEV1 and forced vital capacity, a decrease in the number of exacerbations and an improvement in quality of life [ 35, 36, 60, 61].
Conclusion
Tiotropium is a basic drug for long-term maintenance therapy for COPD. Tiotropium improves functional pulmonary parameters, symptoms, physical performance, quality of life of patients with COPD, and reduces the number of exacerbations of the disease. Currently, only tiotropium therapy has demonstrated benefits not yet shown by studying all other known LABD: slowing the progression of COPD, reducing mortality in COPD patients, reducing the risk of cardiovascular events and high efficacy of the drug in all COPD phenotypes studied.
Side effects of the drug Tiotropium bromide
From the gastrointestinal tract - dry mouth (usually mild, often disappears with continued treatment), constipation. From the respiratory system: cough, local irritation, possible development of bronchospasm, as well as when taking other inhalation agents. Other: tachycardia, difficulty or retention of urination (in men with prostatic hyperplasia), angioedema, blurred vision, acute glaucoma (associated with anticholinergic effects).
Special instructions for the use of Tiotropium bromide
Careful monitoring of patients with moderate or severe renal impairment receiving tiotropium bromide in combination with other drugs excreted primarily by the kidneys is necessary. Prescribe with caution to patients with narrow-angle glaucoma, prostatic hyperplasia or bladder neck obstruction. It should not be used as a means of emergency treatment to relieve bronchospasm attacks. Do not allow the powder to get into your eyes. Use is contraindicated in the first trimester of pregnancy. During other periods of pregnancy and during breastfeeding - only if the expected benefit outweighs any possible risk to the fetus or infant.
Tiotropium bromide is a new long-acting anticholinergic drug
T
Iotropium bromide (TB) is a quaternary ammonium compound similar in chemical structure to ipratropium bromide. Both drugs are practically not absorbed through the mucous membrane of the oropharynx and respiratory tract and are characterized by insignificant oral bioavailability, which explains the absence or minimal frequency and severity of systemic anticholinergic effects when used by inhalation [1,2].
Non-selective anticholinergic drugs - atropine, ipratropium bromide and oxytropium bromide - are known to interact with all three types of muscarinic receptors. Moreover, if blockade of M1 and M3 receptors leads to bronchodilation, then blockade of M2 receptors, accompanied by increased release of acetylcholine into the synaptic cleft, can to some extent reduce the beneficial effects of blockade of postsynaptic M3 receptors. From a theoretical point of view, the use of a selective M3 receptor blocker seems optimal, but to date it has not been possible to create such a drug [3].
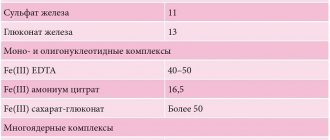
TB has unique kinetic selectivity with a predominant effect on M1 and M3 receptors [1,4,5]. The drug demonstrates a comparatively high degree of affinity for all types of muscarinic receptors, however, the dissociation of the drug with M1 and especially M3 receptors is significantly slowed down, which causes a prolonged blockade of cholinergic bronchoconstriction. On the contrary, the dissociation of TB with M2 receptors is significantly faster (Table 1), which suggests the so-called kinetic selectivity of the drug [6,7].
Like other bronchodilators,
TB is characterized by the following sanogenetic effects:
- Bronchodilation
- relaxation of the tone of the smooth muscle cells of the airways - is characterized by an increase in forced expiratory volume in 1 second (FEV1), but in patients with COPD the dynamics of this indicator are often minimal (<10% of the expected values). - A decrease in dynamic hyperinflation
, accompanied by a decrease in residual volume and functional residual capacity of the lungs, which explains the patient’s symptomatic improvement: the severity of shortness of breath decreases, breathing becomes more “comfortable” [8,9]. - Symptomatic improvement is often more pronounced
in comparison with the minimum dynamics of FEV1, especially in patients with moderate to severe COPD [10,11]. - An increase in exercise tolerance
is one of the most noticeable therapeutic effects when using bronchodilators in patients with COPD [12]. - Increased mucociliary clearance
[13].
Unfortunately, to date there is no direct evidence that bronchodilators are able to modify the natural course of COPD, i.e. slow down the rate of decline in bronchial patency indicators (FEV1) [14].
The duration of the bronchodilator effect of TB exceeds 24 hours. After inhalation of 10 mcg of TB, rapid absorption is observed within the next 5 minutes, reaching a peak plasma concentration of 6 pg/ml; over the next hour, a steady state is established with a plasma concentration of 2 pg/ml, and the terminal half-life is 5–6 days (regardless of the dose taken) [4]. It is estimated that the amount of drug taken “occupies” less than 5% of muscarinic receptors, which partly explains the almost complete absence of systemic adverse events. There is no evidence that TB accumulates with repeated use. In the therapeutic dose range (intravenous administration, powder inhalation), TB is characterized by linear pharmacokinetics [13].
The pharmacokinetics of TB have been well studied in both experimental and clinical settings [15]:
Absorption
. After inhalation of TB in the form of a dry powder, the absolute bioavailability of the drug is 19.5%, indicating that the pulmonary fraction of the drug is characterized by high bioavailability. On the contrary, since TB is a quaternary ammonium compound, it is characterized by extremely low gastrointestinal absorption (10–15%).
Distribution
. 72% of TB are bound to plasma proteins and the volume of distribution is 32 L/kg. 5 minutes after inhalation of 18 μg of TB by patients with COPD, the peak plasma concentration of TB reaches 17–19 pc/ml, and the equilibrium plasma concentration is 3–4 pg/ml.
Metabolism
. The degree of biotransformation of TB is insignificant - in studies on young healthy volunteers after intravenous administration, 74% of the drug is excreted unchanged in the urine.
To date, extensive experience has been accumulated in assessing the effectiveness and safety of TB in the treatment of patients with COPD.
Single-dose TB studies
In a study assessing the spirometric effects and safety of a single dose of TB in patients with COPD, nebulization of the solution was carried out in a dose range from 10 to 160 μg of the drug. The long-lasting bronchodilator effect of TB (>24 hours) and the absence of significant adverse events were confirmed [3]. In another study, TB was administered in a dose range from 10 to 80 mcg (in the form of a metered dose powder inhaler - DPI) and a clear dose-dependent effect of the drug was confirmed [16].
7-day TB studies
The study demonstrated that about 70% of the bronchodilator effect achieved after using TB is observed after taking the first two doses of the drug, and the equilibrium state of FEV1 is achieved within the next 48 hours [17].
4-week TB studies
During a 4-week administration of TB (once daily, in the dose range from 4.5 to 36.0 mcg), when assessing the dynamics of FEV1, a flat dose-effect curve was established. Based on these data, for long-term use of TB, the choice was made in favor of 18 mcg of the drug (1 time/day), since a dose of 36 mcg was characterized by a clear increase in the frequency of such an adverse event as dry mouth, in the absence of a significant increase in FEV1 [18].
13-week TB studies
When TB was prescribed at a dose of 18 mcg 1 time/day in the form of DPI “Handihaler” for 13 weeks, it was shown that the use of TB was more effective than monotherapy with IB, prescribed 4 times/day [19].
In a study conducted by members of The US Tiotropium Study Group
, 13-week administration of TB in patients with COPD was compared with administration of placebo: the anticholinergic drug demonstrated significant superiority in its effect on bronchial obstruction parameters (FEV1, peak expiratory flow rate), disease symptoms, use of short-acting b2-agonists “on demand”, etc. [20 ].
12-month TB studies
Long-term continuous use of TB in patients with moderate/severe COPD was accompanied by a significant improvement in bronchial obstruction, regression of clinical symptoms, optimization of quality of life indicators and a decrease in the frequency of exacerbations of the disease [10,11]. These studies demonstrated that the effect initially observed in the 4- and 13-week studies extended over a significantly longer period of time, indicating no development of tolerance (tachyphylaxis) for at least 12 months.
In particular, the effect of long-term use of TB on the frequency of exacerbations of COPD is indicative: taking the drug was accompanied by the development of an exacerbation within a year in less than half of the observed patients, and only every 10th patient was hospitalized.
TB compared with salmeterol (6-month use)
During six-month administration of TB or salmeterol in patients with COPD, the superiority of TB in the severity of bronchodilation, regression of shortness of breath, and optimization of quality of life indicators was demonstrated [21].
In addition to these now classic studies, works have recently been published that expand our understanding of TB in the treatment of patients with COPD.
The purpose of one study was to prove the possibility of long-term symptomatic improvement in patients with COPD during long-term maintenance therapy for TB, despite the absence or insignificant increase in FEV1 against the background of previous short-term use of bronchodilators [22]. The authors analyzed the results of two 12-month studies that compared the effectiveness of tiotropium (18 mcg/day) and placebo in influencing long-term improvements in functional parameters and health status of patients depending on the results of the bronchodilator test performed on the first day of the study (it was considered positive with dynamics of FEV1 >= 12% or >= 200 ml). All patients receiving TB were divided into two groups: a) positive test – TB – “ responders”
"(i.e. those who responded);
b) negative test – TB – “ non responders
” (i.e. those who responded poorly).
A year later, in both groups, FEV1 values (in the morning, before the next TB inhalation) increased by 212±17 ml and 94±17 ml, respectively (compared to placebo). The same applied to the severity of shortness of breath and quality of life assessment according to the SGRQ (St. George's Respiratory Questionnaire): –3.96±0.99 and –3.05±1.00 points, respectively, compared to placebo. At the same time, a weak correlation between the results of the bronchodilator test on the first day of the study and the subsequent dynamics of the dyspnea index and the integral score of quality of life according to the SGRQ questionnaire was confirmed. Thus, TB demonstrates high effectiveness regardless of the results of the bronchodilator test
, so the latter cannot be used as a predictor of the effectiveness of long-term therapy.
During two 6-month placebo-controlled comparative studies of the effectiveness of TB (18 mcg once a day, Handihaler DPI) and salmeterol (50 mcg twice a day, MDI), the dynamics of the frequency of exacerbations, the severity of shortness of breath, and the integral indicator of quality of life were assessed (SGRQ) and spirometry indicators [23]. A total of 1207 patients were included in the studies (TB - 402, salmeterol - 405, placebo - 400). The lowest number of exacerbations of COPD (patient/year) was in the group of patients taking TB - 1.07 compared with placebo - 1.49 (<0.05) and salmeterol - 1.23. The mechanism for reducing the frequency of exacerbations of COPD during long-term bronchodilator therapy remains incompletely understood. As is known, the leading clinical manifestation of COPD is dyspnea that progresses in intensity, which, as a rule, is a consequence of the increase in hyperinflation during an exacerbation of COPD. Bronchodilators (b2-agonists, anticholinergic drugs) increase the FEV1 value, but FVC is also optimized, which ultimately can lead to a decrease in hyperinflation. Such an improvement in ventilation parameters is accompanied by a decrease in the severity of shortness of breath, especially when performing physical activity. The result of the study - TB, in comparison with placebo, demonstrates a clear decrease in the severity of shortness of breath, improvement in bronchial obstruction, a decrease in the frequency of exacerbations and an improvement in the quality of life of patients
. When taking salmeterol compared to placebo, such effects are less pronounced, unreliable and insignificant from a clinical point of view.
It is generally accepted that COPD is a disease characterized by progressive bronchial obstruction, which is only partially reversible [24]. At the same time, not a single therapeutic effect is capable of “interfering” with the natural course of the disease, i.e. to slow down the rate of annual decline in FEV1 to any significant extent. At the same time, somewhat encouraging data have recently emerged - we are talking about the beneficial consequences of long-term use of TB in patients with COPD. Thus, in one of the placebo-controlled studies assessing the effectiveness of 12-month TB treatment, it was shown that in the group of patients taking placebo (n = 328), the decrease in FEV1 over the specified time period averaged 58.0 ml, and in to the group of patients taking a bronchodilator (n=518) – only 12.4 ml (p<0.005) [25].
So, in the course of numerous controlled studies, it was possible to prove the superiority of TB compared to placebo, ipratropium bromide and salmeterol in influencing individual clinical manifestations, spirometric parameters, indicators of the quality of life of patients with COPD, etc. (Table 2).
Adverse events (AEs) of TB, like any other anticholinergic drug, are pharmacologically predictable and dose-dependent. The inhalation route of delivery of anticholinergic drugs determines the minimum frequency and severity of systemic AEs. However, the majority of COPD patients are older people, often suffering from concomitant diseases. Hence, obviously, the risk of developing AEs from drug therapy increases. The extreme rarity of AEs when taking TB is explained by the inhalation route of administration and the virtual absence of systemic absorption of the drug. Numerous studies have proven that inhaled anticholinergic drugs are extremely safe medications. The most common AEs when using anticholinergic drugs [13]:
1) Dry mouth and cough are the most common AEs observed with the use of TB in 15% of patients (a similar frequency of these AEs was noted with the use of ipratropium bromide) [19].
2) Pharyngitis, upper respiratory tract infections.
3) Bitter metallic taste in the mouth (noted by some patients).
4) Paradoxical bronchoconstriction (possible with nebulization of ipratropium solution).
5) Immediate hypersensitivity reactions (rare).
6) An increase in intraocular pressure can be observed in elderly patients when using a face mask solution during nebulization (associated with the direct effect of the drug on the eye).
7) Systemic AEs are extremely rare: urinary retention, constipation, tachycardia, palpitations.
 Headache, increased excitability, irritability, dizziness.
Headache, increased excitability, irritability, dizziness.
It is important to note that when anticholinergic drugs are used, mucociliary clearance remains intact, although bronchial mucus secretion may be reduced. Anticholinergic drugs do not have a significant effect on the tone of the pulmonary vessels and therefore, unlike b2-agonists and theophylline, do not lead to a drop in the partial oxygen tension in the arterial blood.
In the following clinical situations, anticholinergic drugs (including TB) should be used with caution:
A) Dryness of the oral mucosa, which is often observed in patients suffering from caries.
B) Conjunctivitis.
C) Benign prostatic hyperplasia, urinary retention, urinary disorders associated with bladder dysfunction.
D) Heart rhythm disturbances.
E) Patients with renal and liver failure can use TB in recommended doses, although there is no experience with long-term use of the drug in these categories of patients.
The developer and manufacturer of TB – – entered into a marketing agreement with the promotion of TB under the trade name “ Spiriva”
» in all countries at the same time (including the Russian Federation). TB comes in the form of a single-dose powder inhaler called Handihaler. Each capsule contains 22.5 mcg tiotropium bromide monohydrate, equivalent to 18 mcg tiotropium. The dose of TB released by inhalation of Handihaler is 10 µg [26]. As with any other device, for inhalation therapy, effective use of the discussed DPI requires the patient to have perfect inhalation maneuver technique. Since the majority of patients with COPD are older people, the use of a MDI causes certain difficulties for them, which requires clear coordination of inhalation and actuation of the aerosol generator. On the contrary, DPIs have certain advantages in this category of patients due to their ease of use. When using Handihaler, to evacuate the contents of the capsule, a low inspiratory volumetric flow rate (IVR) is required, which even patients with severe COPD can develop (to carry out a full inhalation maneuver and evacuate the contents of the capsule, an ISV of 20 l/min is sufficient). For comparison, when using the Turbuhaler multi-dose powder inhaler, it is necessary to develop an TWS of 60 l/min [13].
The TB dosing regimen is simple and convenient - the drug is prescribed at a dose of 18 mcg in the form of DPI once a day, usually in the morning or at noon. This property of the drug explains the high adherence of patients to medical recommendations: during a 12-month observation, compliance of more than 90% is demonstrated by 85% of COPD patients (regardless of gender, age and severity of bronchial obstruction) [27], which significantly exceeds the frequency of satisfactory or good compliance in cases long-term use of IB and β-agonists (~60%) [28].
Conclusion
TB is a long-acting (>24 hours) anticholinergic drug given once daily. It has been shown that such a long-lasting effect of the drug is due to its slow dissociation with postsynaptic (effector) muscarinic (M3) receptors. TB is characterized by unique kinetic selectivity, consisting of slow dissociation with M1 and M3 receptors and, conversely, faster dissociation with M2 receptors, and demonstrates the selectivity of action that is so desirable in the treatment of patients with obstructive pulmonary diseases. Clinical studies assessing the effectiveness of TB in patients with COPD demonstrated a stable improvement in bronchial obstruction and the achievement of symptomatic control, exceeding the “consequences” of currently traditionally used IB.
TB is well tolerated; Dry mouth is the most commonly reported symptom (about 10%), but this AE is of little clinical significance.
Pharmacologists are naturally interested in the unique kinetic selectivity of the action of TB
.
From a theoretical point of view, this property may explain a certain attractiveness in the treatment of chronic obstructive pulmonary diseases, since it eliminates the increase in acetylcholine production, and therefore counteracts the final effect of the drug. However, it is unlikely that this property of TB is of particular clinical significance. Obviously, the most important property of TB is long-term bronchodilation and bronchoprotection (>24 hours). This property makes it possible to use the drug once a day, which is extremely important from a clinical point of view, since it ensures higher compliance. Another beneficial consequence of the long-term effect of the drug is the fact that periodic omissions of the next dose will not have a negative impact on the achieved control over the course of the disease, since the anticholinergic activity of the drug persists for more than 24 hours. Clinical studies have shown that TB prescribed once provides better control over the course of the disease. course of COPD
, rather than the modern standard of anticholinergic therapy - ipratropium bromide, used 4 times a day. It has also been shown that maximum bronchodilation can be achieved with relatively small doses of TB.
Overall, TB is seen as a very promising drug with a promising future. Since bronchodilators are the main class of drugs that have proven their effectiveness in long-term use by patients with COPD, TB can become the drug of choice for a large number of patients with moderate/severe (extremely severe) disease (Tables 3, 4).
Active research is currently underway to create new drugs that can interrupt the progression of COPD, but to date there is not a single drug that has this property.
For practical medicine, this means that TB will gain a stable position as a “leader” in bronchodilator therapy for COPD for many years. References:
1. Barnes PJ Tiotropium bromide. Expert Opin Investig Drugs 2001; 10: 733–740.
2. Hvizdos KM, Goa KL Tiotropium bromide. Drugs 2002; 62:1195–1203.
3. Maesen FPV, Smeets JJ, Costongs Ma AL et al. Ba 679 Br, a new long-acting antimuscarinic bronchodilator: A pilot dose-escalation study in COPD. Eur Respir J 1993; 6:1031–1036.
4. Disse B., Speck GA, Rominger KL et al. Tiotropium (Spiriva) mechanistic considerations and clinical profile in obstructive lung disease. Life Sci 1999; 64:457–464.
5. Barnes PJ The pharmacological properties of tiotropium. Chest 2000; 117 (2 Suppl.): 63–68.
6. Disse B., Reichi R., Speck G. et al. A novel long-acting anticholinergic bronchodilator. Life Sci 1993; 52:537–544.
7. Haddad EB, Mak JC, Barnes PJ et al. Characterization of [3H]Ba 679 BR, a slowly dissociating muscarinic antagonist, in human lung: Radioligand binding and autoradiographic mapping. Mol Pharmacol 1994; 45:899–907.
8. Nisar M, Earis JE, Pearson MG et al. Acute bronchodilator trials in chronic obstructive pulmonary disease. Am Rev Respir Dis 1992; 146:555–559.
9. O'Donnel DE, Lam M., Webb KA Measurement of symptoms, lung hyperinflation, m and endurance during exercise in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1998; 158:1557–1565.
10. Casaburi R., Mahler DA, Jones PW et al. A long–term evaluation of once–daily inhaled tiotropium in chronic obstructive pulmonary disease. Eur Respir J 2002; 19: 217–224.
11. Vincken W., van Noord JA, Greethorst AP et al. Improved health outcomes in patients with COPD during 1 yr's treatment with tiptropium. Eur Respir J 2002; 19: 209–216.
12. Belman MJ, Botnick WC, Shin JW Inhaled bronchodilators reduce dynamic hyperinflation during exercise in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1996; 153:967–975.
13. Hansel TT, Barnes PJ Tiotropium bromide: a novel once–daily anticholinergic bronchodilator for the treatment of COPD. Drugs of Today 2002; 38:585–600.
14. Anthonisen NR, Connett JE, Kiley JP et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study. JAMA 1994; 272:1497–1505.
15. Leusch A., Eichhorn B., Muller G. et al. Pharmacokinetics and tissue distribution of the anticholinergics tiotropium and ipratropium in the rat and dog. Biopharm Drug Dispos 2001; 22: 199–212.
16. Maesen FPV, Smeets JJ, Sledsens TJH et al. Tiotropium bromide, a new long-acting antimuscarinic bronchodilator. A pharmacodynamic study in patients with chronic obstructive pulmonary disease. Eur Respir J 1995; 8:1506–1513.
17. van Noord JA, Smeets JJ, Custers FL et al. Pharmacodynamic steady state of tiotropium in patients with chronic obstructive pulmonary disease. Eur Respir J 2002; 19: 639–644.
18. Littner MR, Ilowite JS, Tashkin DP et al. Long–acting bronchodilation with once–daily dosing of tiotropium (Spiriva) in stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2000; 161:1136–1142.
19. van Noord JA, Bantje TA, Eland ME et al. A randomized controlled comparison of tiotropium and ipratropium in the treatment of chronic obstructive pulmonary disease. The Dutch Tiotropium Study Group. Thorax 2000; 55:289–294.
20. Casaburi R., Serby W., Menjoge SS et al. The spirometric efficacy of once daily dosing with tiotropium in stable COPD. Am J Respir Crit Care Med 1999; 159:A524 (Abst.).
21. Donohue JF, van Noord JA, Babeman ED et al. A 6–month, placebo–controlled comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest 2002; 122:47–55.
22. Tashkin D., Kesten S. Long–term treatment benefits with tiotropium in COPD patients with and without short–term bronchodilator responses. Chest 2003;123:1441–1449.
23. Busasco V., Hodder R., Miravitlles M. et al. Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients
with COPD. Thorax, 2003; 58:399–404.
24. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Executive summary. Updated 2003 (www.goldcopd.com)
25. Anzueto A., Menjoge SS, Kesten S. Changes in FEV1 over time in 1-year clinical trials of tiotropium in COPD. Proceedings of the Annual Meeting of the American Thoracic Society (ATS), San Francisco, USA, 21–25 May 2001.
26. Chodosh S, Flanders JS, Kesten S, et al. Effective delivery of particles with the HandiHaler Dry Powder Inhalation System over a range of chronic obstructive pulmonary disease severity. J Aerosol Med 2001; 14: 309–315.
27 Rand CS, Nides M, Cowles MK et al. Long-term metered-dose inhaler adherence in a clinical trial: The Lung Health Study Research Group. Am J Respir Crit Care Med 1995; 152:580–588.
28. Rand CS, Nides M, Cowles MK et al. Long-term metered-dose inhaler adherence in a clinical trial: The Lung Health Study Research Group. Am J Respir Crit Care Med 1995; 152:580–588.
29. Canadian Thoracic Society COPD Guidelines: summary of highlights for family doctors. Can Respir J 2003; 10: 183–186.