Pharmacodynamics and pharmacokinetics
Pharmacodynamics
LP receptors of the liver regulate the content of lipoproteins in the blood. Lipoproteins are removed from the circulating blood by interacting with these receptors and cholesterol . The mechanism of action of Lovastatin is explained by the suppression of 3-hydroxy-3-methylglutaryl-coenzyme A reductase, an enzyme with the participation of which cholesterol synthesis occurs. A decrease in the formation of cholesterol in the liver entails a compensatory increase in the number of lipoprotein receptors on the surface of hepatocytes, as a result of which the removal of low-density lipoproteins from the plasma is accelerated and total cholesterol, intermediate-density lipoprotein cholesterol and very low-density lipoprotein cholesterol .
The drug reduces the content of triglycerides and apolipoprotein B , and slightly increases the level of high-density lipoproteins. The therapeutic effect appears after 14 days, and the maximum effect occurs after 6 weeks from the start of treatment, and persists for 1.5 months after discontinuation of the drug. Efficiency does not decrease with long-term use. Lovaststatin is obtained from biocultures of Monascus ruber and Aspergillus terreus.
Pharmacokinetics
Absorbed into the gastrointestinal tract slowly. Absorption is reduced by taking the drug on an empty stomach. Bioavailability is low - 30% of the dose. After 2-4 hours, the maximum concentration in the blood is reached, which decreases and after 24 hours is 10% of the maximum. 95% binds to blood proteins. Clearance of Lovastatin with a single dose is achieved within 2-3 days. Lovastatin is a prodrug and after the first passage through the liver it acquires the active dosage form. Metabolism occurs with the participation of isoenzymes. The half-life is 3 hours. The active substance and its metabolites are excreted through the intestines and kidneys.
Pharmacological properties of the drug Lovastatin
Lipid-lowering agent, HMG-CoA reductase inhibitor. Lovastatin is an inactive lactone form of the corresponding free hydroxy acid. After absorption in the digestive tract, lovastatin is rapidly hydrolyzed. The active form of lovastatin is a specific inhibitor of HMG-CoA reductase, an enzyme that catalyzes the conversion of HMG-CoA to mevalonate. Blocks the synthesis of cholesterol in the liver at the initial stage, which leads to a decrease in the concentration of cholesterol, triglycerides, LDL and VLDL in the blood; at the same time, it increases the content of HDL, which has an antiatherogenic effect. The drug is low toxic. When taken orally, the maximum concentration of lovastatin in the blood is observed after 1–2 hours. It is excreted mainly in the urine in the form of glucuronides.
Side effects
- heartburn , nausea, flatulence , constipation or diarrhea ; very rarely - taste perversion, hepatitis , biliary cholestasis , cholestatic jaundice ;
- headache, dizziness; sleep disorders, insomnia , general weakness, anxiety, paresthesia ;
- myalgia and muscle cramps, myositis ; in patients taking Cyclosporine , Nicotinic acid or Gemfibrozil , there is a risk of developing rhabdomyolysis ;
- hemolytic anemia , thrombocytopenia ;
- optic atrophy , cataracts ;
- increased activity of liver transaminases, creatine phosphokinase activity; very rarely alkaline phosphatase and bilirubin.
- rash, itching, angioedema , urticaria , arthralgia ;
- very rarely, decreased potency and alopecia .
Interaction with other drugs
When taking Lovastatin together with antibiotics (macrolides), immunosuppressants, nicotinic acid, the risk of rhabdomyolysis (a syndrome accompanied by the destruction of muscle tissue cells and the development of severe renal failure) significantly increases. This combination of drugs is especially dangerous in people suffering from diabetic nephropathy.
Combined use of the drug with anticoagulants, indanedione/coumarin derivatives increases the likelihood of an increase in prothrombin time, which leads to increased bleeding. The lipid-lowering effect of Lovastatin is reduced by treatment with thiazide and loop diuretics.
Isradipine, Diltiazem and Verapamil inhibit the CYP3A4 isoenzyme necessary for the elimination of Lovastatin. As a result, combined treatment with medications increases the concentration of lovastatin (the active substance) in the blood and increases the risk of muscle tissue breakdown.
Drugs for the treatment of vascular atherosclerosis
Special instructions:
- The drug should be prescribed with caution in people with liver pathologies and chronic alcoholics.
- The medication must be discontinued if there is a persistent increase in liver transaminases or CPK in the blood. The indication for cancellation is a person’s serious condition.
- Lovastatin should not be prescribed to pregnant or breastfeeding women.
- The medication is contraindicated in case of liver pathologies (in the acute period), increased activity of liver transaminases.
A history of liver disease is prohibited from use. The development of weakness and muscle pain against the background of feverish conditions is a signal to discontinue the drug.
No ads 2
Lovastatin, instructions for use (Method and dosage)
Tablets are taken orally 1 time per day during dinner. For hyperlipidemia - from 10 to 80 mg once, depending on the severity of hyperlipidemia. Treatment begins with a small dose, then gradually increases it. The maximum daily dose of 80 mg can be taken in one or two doses (morning and evening). Dose selection is carried out at intervals of 4 weeks.
For coronary atherosclerosis, the dose is 20–40 mg. If ineffective, increase to 60–80 mg. When taking fibrates or nicotinic acid , the dose of Lovastatin should not exceed 20 mg per day.
Lovastatin
Description Tablets are white with a yellowish tint, flat-cylindrical in shape, with a bevel. Composition Each tablet contains: lovastatin - 20 mg or 40 mg; excipients: corn starch, microcrystalline cellulose, aerosil, magnesium stearate, butylated hydroxyanisole, lactose monohydrate.
Release form Tablets 20 mg and 40 mg. Pharmacotherapeutic group: Lipid-lowering drugs. HMG-CoA reductase inhibitors. ATX code S10AA02
Pharmacodynamics Hypolipidemic agent. Lovastatin disrupts the first stage of cholesterol synthesis in the liver - the formation of mevalonic acid. In the body, lovastatin is hydrolyzed to its active form - β-hydroxy acid, which inhibits 3-hydroxy-3-methylglutaryl-CoA reductase and disrupts the conversion of HMG-CoA to mevalonic acid, resulting in decreased cholesterol synthesis and increased catabolism. Reduces the blood levels of very low-density lipoproteins, low-density lipoproteins and triglycerides, moderately increases the content of high-density lipoproteins. Since the conversion of HMG-CoA to mevalonic acid is an early step in cholesterol synthesis, lovastatin therapy does not lead to the accumulation of toxic sterols. When taking the drug once a day, the duration of action is 24 hours. After discontinuation during a course of treatment, the effect of the drug persists for 4-6 weeks.
Pharmacokinetics , the maximum concentration in the blood plasma is reached after 2-4 hours. When taking the drug on an empty stomach, the degree of absorption is reduced by 30% compared to taking it with food. Plasma protein binding is 95%. Lovastatin penetrates the blood-brain barrier and the placental barrier. Metabolized in the liver to form several metabolites, including the pharmacologically active metabolite - β-hydroxy acid. Excreted in bile - 83% and in urine - 10%. In a study of patients with severe renal impairment (creatinine clearance 10-30 ml/min), plasma concentrations of total inhibitors after a single dose of lovastatin were approximately twice as high as in healthy volunteers. Plasma concentrations of lovastatin are higher in older adults (aged 70–78 years) (Cmax approximately 45%) than in younger adults (aged 18–30 years).
Indications for use The use of Lovastatin should be an integral part in the treatment of patients with dyslipidemia, where there is a risk of developing atherosclerotic vascular diseases. Lovastatin should be used in addition to a diet limited in saturated fat and cholesterol in combination therapy to reduce total cholesterol and LDL-cholesterol to normal levels when diet therapy and other non-drug treatments are ineffective. Primary prevention of coronary heart disease Lovastatin is indicated for patients without clinical signs of cardiovascular diseases, with moderately elevated levels of total cholesterol, LDL cholesterol and reduced levels of HDL to reduce the risk of: myocardial infarction; unstable angina; coronary revascularization procedures. Coronary heart disease Lovastatin is prescribed to slow the progression of coronary atherosclerosis in patients with coronary heart disease, in complex treatment to reduce total cholesterol and LDL cholesterol to normal. Hypercholesterolemia Lovastatin is prescribed as an adjunct to diet to reduce elevated levels of total cholesterol and LDL cholesterol in patients with primary hypercholesterolemia (types IIa and IIb) when non-drug treatments, including diet therapy, are ineffective.
Method of administration and dosage For oral administration. The patient must be prescribed a standard cholesterol-lowering diet before starting to take lovastatin, which must be followed during treatment with the drug. Doses should be adjusted according to the primary goals of therapy and the patient's response to treatment. The usual initial dose is 20 mg 1 time per day. The drug is taken during dinner. If necessary, the dose is adjusted after at least 4 weeks. The maximum daily dose is 80 mg in 1 or 2 doses (during breakfast and dinner). Patients requiring a 20% or greater reduction in LDL cholesterol should start with 20 mg/day. It is necessary to periodically monitor the level of cholesterol in the blood; if the concentration of total cholesterol decreases to 140 mg/100 ml (3.6 mmol/l) or low-density lipoproteins to 75 mg/100 ml (1.94 mmol/l), the dose of lovastatin should be reduced . For patients receiving immunosuppressive therapy and patients with severe renal failure (creatinine clearance less than 30 ml/min), the maximum daily dose is 20 mg. Patients with a history of liver disease and/or who consume significant amounts of alcohol should be carefully monitored during lovastatin therapy. If significant pathological changes are detected (an increase in the activity of hepatic transaminases by more than 3 times compared to the upper limit of normal), the dose of the drug should be reduced or treatment should be discontinued. In patients taking danazol, diltiazem or verapamil concomitantly with lovastatin, the dose of the drug should not exceed 20 mg / day. In patients taking amiodarone concomitantly with lovastatin, the dose should not exceed 40 mg/day. When using the drug in elderly patients, no dose adjustment is required. If you miss the current dose, the drug must be taken as soon as possible. If it is time for the next dose, do not double the dose. Side effects Sleep disturbance, including insomnia, nightmares, memory loss, sexual dysfunction, depression, very rare cases of interstitial lung disease, especially with long-term therapy, headache, dizziness, peripheral neuropathy, general weakness, convulsions, myopathy, arthralgia, heartburn, dyspepsia, nausea, constipation, cholestatic jaundice, hepatitis, pancreatitis, lens opacities, cataracts, optic nerve atrophy, blurred vision, hemolytic anemia, leukopenia, thrombocytopenia, increased levels of hepatic transaminases and creatine phosphokinase in the blood serum, asthenia, abdominal pain, diarrhea, flatulence, myalgia, allergic reactions, diabetes mellitus: the incidence will depend on the presence or absence of risk factors (fasting glucose ≥ 5.6, body mass index >30 kg/m2, increased triglyceride levels, history of hypertension). It is necessary to consult your doctor if the listed adverse reactions occur, as well as a reaction not indicated in the instructions.
Contraindications Hypersensitivity to any of the components of the drug, acute liver diseases, constant increase in the activity of liver transaminases of unknown origin, cholestasis, pregnancy, lactation, age under 18 years. Co-administration of lovastatin with: itraconazole, ketoconazole, posaconazole, erythromycin, clarithromycin, telithromycin, HIV protease inhibitors, boceprevir, telaprevir, nefazodone is contraindicated. Overdose Symptoms: overdose is accompanied by increased side effects. Treatment: monitoring liver function, symptomatic therapy. Warnings and Special Instructions Lovastatin, like other HMG-CoA reductase inhibitors, can cause myopathy (muscle pain, tenderness and weakness with creatine kinase elevated ten times the upper limit of normal). Myopathy sometimes takes the form of rhabdomyolysis with or without acute renal failure resulting in myoglobinuria, and is rarely fatal. The risk of myopathy increases due to increased inhibitory activity against HMG-CoA reductase in the blood plasma. The risk of developing myopathy/rhabdomyolysis depends on the dose of the drug. All patients starting treatment with lovastatin, or whose dosage of lovastatin is increased, should be warned of the risk of myopathy and the need to promptly report any unexplained muscle pain, tenderness, or weakness. If confirmed or suspected myopathy is present, treatment with lovastatin should be discontinued immediately. In most cases, when treatment is stopped quickly, muscle symptoms disappear and creatine kinase levels return to normal. Periodic creatine kinase determinations may be indicated in patients initiating lovastatin therapy or whose dosage is being increased, which does not guarantee the prevention of myopathy. Many patients who developed rhabdomyolysis during treatment with lovastatin had complex medical histories, including renal failure, which is usually a consequence of long-term diabetes mellitus. Such patients deserve more careful monitoring. If CPK levels increase, treatment with lovastatin should be discontinued. Treatment with lovastatin should be temporarily discontinued if the patient experiences acute or serious illness predisposing to the development of renal failure secondary to rhabdomyolysis, such as sepsis, hypotension, major surgery, trauma, severe metabolic, endocrine or electrolyte disturbances, or uncontrolled epilepsy. The risk of developing myopathy/rhabdomyolysis is increased when lovastatin is used concomitantly with the following drugs: strong CYP3A4 inhibitors: increase plasma levels of lovastatin, which increases the risk of developing myopathy. These drugs include itraconazole, ketoconazole, posaconazole, the macrolide antibiotics erythromycin and clarithromycin, the ketolide antibiotic telithromycin, HIV protease inhibitors, boceprevir, telaprevir, and the antidepressant nefazodone. The combination of these drugs with lovastatin is contraindicated. If therapy with these drugs is necessary, lovastatin should be discontinued during the course of treatment. In vitro, voriconazole has been shown to inhibit the metabolism of lovastatin and increase plasma concentrations of lovastatin, which is why it is recommended to adjust the dose of lovastatin when used concomitantly with voriconazole. Gemfibrozil: Concomitant use of lovastatin with gemfibrozil should be avoided. other lipid-lowering drugs (fibrates or niacin at a dose of > 1 g/day): Caution should be exercised when prescribing fibrates or niacin at lipid-lowering doses (> 1 g/day) with lovastatin, as these drugs can lead to myopathy when used alone. The expected benefits and risks of treatment should be carefully weighed when using lovastatin in combination with fibrates or nicotinic acid. cyclosporine: Use of lovastatin with cyclosporine should be avoided. danazol, diltiazem or verapamil with high-dose lovastatin: The dose of lovastatin should not exceed 20 mg when taken together. Amiodarone: The dose of lovastatin should not exceed 40 mg per day in patients receiving concomitant treatment with amiodarone. It is possible to use lovastatin at a dose higher than 40 mg per day with amiodarone if the clinical effect outweighs the increased risk of developing myopathy. The risk of developing myopathy/rhabdomyolysis is increased when amiodarone is used concomitantly with high doses of HMG-CoA reductase inhibitors. Colchicine: Cases of myopathy/rhabdomyolysis have been reported with concomitant use and caution should be exercised when administering lovastatin with colchicine. Ranolazine: The risk of myopathy/rhabdomyolysis may be increased with concomitant use; dosage adjustment is necessary. It is necessary to monitor the level of activity of transaminases and other liver enzymes in the blood serum before starting statin therapy and as clinically indicated during use. In the presence of serious liver damage with clinical symptoms and/or hyperbilirubinemia, jaundice appearing during administration, the use of statins should be discontinued. Unless another cause of serious liver damage has been identified, statin use should not be restarted. Prescribed with caution for a history of liver disease, chronic alcoholism, organ transplantation, concomitant immunosuppressive therapy, chronic renal failure, urgent surgical procedures (including dental). There have been reports of very rare cases of the development of interstitial lung disease when taking statins, especially with long-term therapy. If symptoms of interstitial lung disease appear, such as respiratory distress, shortness of breath, nonproductive cough, deterioration in general condition (fatigue, weight loss, fever), statin therapy should be discontinued. Statins as a class increase blood glucose levels and, in patients at high risk of developing diabetes, may cause elevated blood sugar levels that require appropriate treatment. However, the benefits of statins in reducing the risk of cardiovascular disease outweigh the small increase in the risk of diabetes, so statin use should not be stopped. Periodic monitoring of glycemia is necessary in patients at risk (fasting glucose 5.6 - 6.9 mmol/l, body mass index >30 kg/m2, increased triglyceride levels, hypertension), according to current recommendations. Concomitant use of grapefruit juice with the drug may lead to increased plasma concentrations of lovastatin, so patients taking the drug should avoid consuming grapefruit juice. Use with caution in patients with rare hereditary diseases: congenital galactosemia, lactase deficiency, glucose/galactose malabsorption syndrome. Patients should be warned about substances that should not be taken concomitantly with lovastatin and advised to promptly report unexplained muscle pain, tenderness, or weakness. Patients should be advised to inform other prescribers of a new drug that they are taking Lovastatin.
Use during pregnancy and lactation Safety in pregnant women has not been established. The drug is contraindicated during pregnancy and lactation. The drug should not be used by women who are pregnant or planning pregnancy. If pregnancy occurs, lovastatin should be discontinued immediately. Lovastatin can be prescribed to women of childbearing age if the possibility of pregnancy has been reliably excluded and the patient has been informed of the potential danger. There is no data on the excretion of lovastatin in breast milk. Given the possibility of adverse reactions in infants, women receiving this drug should stop breastfeeding.
Impact on the ability to drive vehicles and operate machinery During the treatment period, care must be taken when driving vehicles and engaging in other potentially hazardous activities that require increased concentration and speed of psychomotor reactions.
Interaction with other drugs Interaction with inhibitors of the CYP3A4 isoenzyme Lovastatin is metabolized by the CYP3A4 isoenzyme, but does not have inhibitory activity against this isoenzyme, therefore lovastatin cannot lead to an increase in plasma concentrations of other drugs metabolized by CYP3A4. Co-administration of strong CYP3A4 inhibitors (itraconazole, ketoconazole, posaconazole, clarithromycin, telithromycin, HIV protease inhibitors, boceprevir, telaprevir, nefazodone and erythromycin) with lovastatin is contraindicated due to an increased risk of myopathy due to a decrease in the rate of elimination of lovastatin. In vitro, voriconazole inhibits the metabolism of lovastatin. When used concomitantly, it is recommended to adjust the dose of lovastatin to reduce the risk of developing myopathy/rhabdomyolysis. Interaction with lipid-lowering drugs that may cause myopathy when used alone The risk of developing myopathy is also increased with lipid-lowering drugs that are not strong inhibitors of CYP3A4, but which may lead to myopathy when used alone. Cyclosporine, gemfibrozil: The risk of myopathy/rhabdomyolysis increases when cyclosporine or gemfibrozil is used concomitantly with lovastatin. The combined use of these drugs should be avoided. Danazol, diltiazem, or verapamil: The risk of myopathy/rhabdomyolysis is increased when danazol, diltiazem, or verapamil are coadministered, especially with higher doses of lovastatin. The dose of lovastatin should not exceed 20 mg per day when taken together with danazol, diltiazem or verapamil. Amiodarone: The risk of developing myopathy/rhabdomyolysis increases when amiodarone is used concomitantly with other statin drugs (HMG-CoA reductase inhibitors). The dose of lovastatin should not exceed 40 mg per day when taken together with amiodarone. Coumarin anticoagulants: It is recommended that the prothrombin time be determined in patients taking anticoagulants before starting treatment with lovastatin, and it is often sufficient to determine the prothrombin time at the start of therapy to ensure that no significant changes occur. Once a stable level of prothrombin time is achieved, its further monitoring should be carried out at intervals recommended for patients receiving anticoagulant therapy. When changing the dosage of lovastatin, prothrombin time should also be monitored according to the above scheme. Lovastatin therapy does not cause changes in prothrombin time and the risk of bleeding in patients not taking anticoagulants. Colchicine: Cases of myopathy, including rhabdomyolysis, have been reported when colchicine was used concomitantly with lovastatin. Ranolazine: The risk of myopathy, including rhabdomyolysis, may be increased by concomitant use of ranolazine with lovastatin. Propranolol: There were no clinically significant pharmacokinetic or pharmacodynamic interactions when single doses of lovastatin and propranolol were co-administered in healthy volunteers. Digoxin: in patients with hypercholesterolemia, concomitant administration of lovastatin and digoxin did not change the plasma digoxin concentration. Oral hypoglycemic agents: In pharmacokinetic studies in patients with hypercholesterolemic non-insulin-dependent diabetes, lovastatin did not interact with the drugs glipizide or chlorpropamide. Endocrine function: Patients with endocrine dysfunction or taking drugs that affect the activity of endogenous steroid hormones require medical monitoring when co-administered with lovastatin.
Storage conditions In a place protected from moisture and light at a temperature not exceeding 25 ° C. Keep out of the reach of children.
Shelf life: 3 years. Do not use after the expiration date stated on the package.
Packaging 10 tablets in a blister pack. Two or three blister packs per pack.
Interaction
Taking with Nicotinic acid , Erythromycin , Clarithromycin , Cyclosporine , antifungal drugs ( Ketoconazole , Itraconazole ), Ritonavir , Nefazodone leads to an increase in the concentration of the drug, the risk of developing myopathy and destruction of muscle tissue.
Simultaneous intake of large amounts of grapefruit juice, Gemfibrozil , Fenofibrate also carries a risk of developing myopathies.
Co-administration of Warfarin increases the risk of bleeding.
Cholestyramine reduces the bioavailability of the drug, so the time between taking these drugs should be 2-4 hours.
Overdose
If the recommended doses of the drug are exceeded, an overdose cannot be ruled out. Treatment is symptomatic, aimed at alleviating the current condition. Absorbents, enterosorbents, and diuretics may be prescribed. The patient should drink plenty of fluids.
If the recommended dosage is exceeded and side symptoms develop, drugs from the group of enterosorbents are prescribed
Important! The hemodialysis procedure is effective only in severe cases of poisoning.
Lovastatin analogues
Level 4 ATX code matches:
Akorta
Atomax
Lipitor
Pravastatin
Simvastol
Owencore
Simgal
Tulip
Liptonorm
Rozulip
Zokor
Rosart
Tevastor
Atorvastatin
Liprimar
Simvastatin
Atoris
Basilip
Rosecard
Roxera
Apexstatin , Cardiostatin , Vero-Lovastatin , Choletar , Mevacor , Lovacor , Lovasterol , Mevinacor , Pravastatin , Iinvastin , Fluvastatin .
Analogs
Lovastatin analogues are numerous. Among the budget substitutes it is worth highlighting:
- Holetar. The active ingredient in it is lovastatin, so all side effects/indications/contraindications are identical to Lovastatin.
- Cardiostatin. A drug with hypolipidemic properties. The active ingredient is lovastatin. It is used to prevent the development of myocardial infarction and reduce the likelihood of atherosclerosis.
- Zokor. The main indication is hypercholesterolemia. The drug is recommended for use for preventive purposes - it prevents the occurrence of cardiac pathologies.
- Provastatin. Prescribed for high cholesterol levels and as a prevention of the formation of atherosclerosis.
Choletar and Cardiostatin are structural analogues of Lovastatin. If necessary, you can use: Lovacor, Liprox, Lovasterol, Medostatin, Mevacor, Vasoclin, Simvastatin and other drugs from the statin group.
Cardiostatin is one of the structural analogues of Lovastatin
Reviews of Lovastatin
Lipid-lowering drugs are used in complex treatment and for the prevention of atherosclerosis and its complications. Their main effect is to reduce the content of atherogenic lipoproteins in the blood. Representatives of the statin group (in order of increasing effect) are: Lovastatin , Simvastatin , Fluvastatin , Pravastatin , Atorvastatin and Rosuvastatin . Often, as the main effect increases, the risk of side effects also increases.
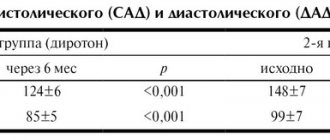
Extensive experience has been accumulated in the clinical use of Lovastatin, which is the safest drug and is well tolerated during long-term treatment. According to patient reviews, side effects appeared quite rarely: flatulence , diarrhea or constipation , abdominal pain, insomnia, muscle pain. As a rule, these reactions disappeared after 2 weeks of taking the drug or after reducing the dose. If the levels of AST and ALT increased after a month, the tests were monitored and the dose of the drug was reduced. After 1.5-2 months from the start of treatment, a control determination of lipid levels was carried out and positive dynamics were noted in the tests.
Indications for use
Lovastatin is used to diagnose the following conditions:
- hypercholesterolemia (primary type IIa/IIb, combined)
- hypertriglyceridemia;
- hyperlipoproteinemia;
- atherosclerosis.
Cholesterol synthesis and the effect of statins on the level of the substance in the body
The medication is used in patients with diabetes to prevent the development of serious complications. Treatment with Lovestatin can be combined with antihyperglycemic drugs. Taking a lipid-lowering drug is possible to prevent the development of pathologies of the heart and blood vessels. This is especially true for possible relapses of heart attack, stroke and others. In this case, it is prescribed in combination with cardiac medications.
No ads 1
Reviews
It is important to remember that the medication is intended to be taken when elevated blood cholesterol is detected for various reasons. Reviews for the drug are positive.
Elena, 35 years old: My father was prescribed coronary bypass surgery. During the operation, some vessels were replaced because they were clogged with cholesterol. To prevent the development of this condition, he was prescribed continuous use of Lovastatin. Dad is feeling good.
Olga, 54 years old: The doctor prescribed me tests for hormones, and at the same time, blood biochemistry for cholesterol and triglyceride levels. It turned out that cholesterol was high. The doctor prescribed a course of Lovastatin. After finishing the course, I took repeated tests. Cholesterol levels returned to normal.
Oleg, 45 years old: I was diagnosed with atherosclerosis. The doctor prescribed this particular drug. Of course, there are a lot of possible side effects. But I started the course anyway. I feel good so far. I didn't notice any side effects.
Lovastatin is a drug intended to normalize (lower) blood cholesterol levels. The drug is available with a prescription. Independent use is unacceptable. It is important to remember that during the entire period of taking the medication it is necessary to follow a low-cholesterol diet and constant monitoring of the latter.