Contraindications to the use of Arcoxia
- complete or incomplete combination of bronchial asthma, recurrent nasal polyposis or paranasal sinuses and intolerance to acetylsalicylic acid and other NSAIDs (including a history);
- erosive and ulcerative changes in the mucous membrane of the stomach or duodenum, active gastrointestinal bleeding, cerebrovascular or other bleeding;
- inflammatory bowel diseases (Crohn's disease, ulcerative colitis) in the acute phase;
- hemophilia and other bleeding disorders;
— severe heart failure (II-IV functional classes according to the NYHA classification);
- severe liver failure (more than 9 points on the Child-Pugh scale) or active liver disease;
- severe renal failure (creatinine clearance less than 30 ml/min), progressive kidney disease, confirmed hyperkalemia;
— the period after coronary artery bypass grafting; peripheral arterial diseases, cerebrovascular diseases, clinically significant ischemic heart disease;
- persistent blood pressure values exceeding 140/90 mm Hg. Art. with uncontrolled arterial hypertension;
- pregnancy;
- lactation period (breastfeeding);
- children under 16 years of age;
- hypersensitivity to any component of the drug.
The drug should be used with caution in the presence of anamnestic data on the development of ulcerative lesions of the gastrointestinal tract, Helicobacter pylori infection, in the elderly, in patients who have used NSAIDs for a long time, frequently drinking alcohol, with severe somatic diseases, dyslipidemia/hyperlipidemia, with diabetes mellitus, arterial hypertension, edema and fluid retention, smoking, in patients with CC less than 60 ml/min, with concomitant therapy with the following drugs: anticoagulants (for example, warfarin), antiplatelet agents (for example, acetylsalicylic acid, clopidogrel), corticosteroids (for example, prednisolone), selective inhibitors serotonin reuptake (for example, citalopram, fluoxetine, paroxetine, sertraline).
Arcoxia, 14 pcs., 60 mg, film-coated tablets
Etoricoxib, when administered orally at therapeutic concentrations, is a selective cyclooxygenase-2 (COX-2) inhibitor. In clinical pharmacological studies, the drug ARCOXIA® dose-dependently inhibited COX-2, without affecting COX-1 when using a daily dose of up to 150 mg. Etoricoxib does not inhibit prostaglandin synthesis in the gastric mucosa and does not affect platelet function.
Cyclooxygenase is responsible for the formation of prostaglandins. Two isoforms of cyclooxygenase have been isolated: COX-1 and COX-2. COX-2 is an isoenzyme that is induced by various proinflammatory mediators and is considered as the main enzyme responsible for the synthesis of prostanoid mediators of pain, inflammation and fever. COX-2 is involved in the processes of ovulation, implantation and closure of the ductus arteriosus, regulation of kidney and central nervous system function (induction of fever, pain sensation, cognitive function), and may also play a role in the healing process of ulcers. COX-2 has been found in tissue surrounding human gastric ulcers, but its importance in ulcer healing has not been established.
Efficiency
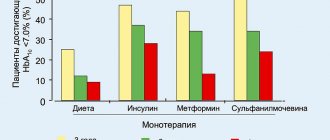
In patients with osteoarthritis (OA), etoricoxib, administered at a dose of 60 mg once daily, provided significant pain relief and improved patient assessment of their condition. These beneficial effects were observed as early as the second day of treatment and persisted for 52 weeks. Studies of etoricoxib at a dose of 30 mg once daily demonstrated superior efficacy compared to placebo over a treatment period of 12 weeks (using similar assessment methods). In an optimal dose determination study, etoricoxib 60 mg demonstrated significantly greater improvement than 30 mg for all 3 primary endpoints after 6 weeks of treatment. The 30 mg dose has not been studied in osteoarthritis of the hand joints.
In patients with rheumatoid arthritis (RA), etoricoxib 60 mg and 90 mg once daily provided both significant reductions in pain and inflammation and improvements in mobility. In studies evaluating etoricoxib doses of 60 mg and 90 mg, these beneficial effects were maintained over a 12-week treatment period.
In patients with acute gouty arthritis attacks, etoricoxib 120 mg once daily for an eight-day treatment period reduced moderate to severe joint pain and inflammation. Efficacy was comparable to that of indomethacin when administered at a dose of 50 mg three times daily. A decrease in pain was noted within four hours after the start of treatment.
In patients with ankylosing spondylitis, etoricoxib 90 mg once daily provided significant improvements in back pain, inflammation, stiffness, and function. Clinical efficacy of etoricoxib was observed as early as the second day of treatment and was maintained throughout the 52-week treatment period. In a second study comparing etoricoxib 60 mg dose with etoricoxib 90 mg dose, etoricoxib 60 mg once daily and 90 mg once daily demonstrated similar efficacy compared with naproxen 1000 mg once daily.
In a clinical trial examining pain after dental surgery, etoricoxib 90 mg was given once daily for three days. In the subgroup of patients with moderate pain at baseline, etoricoxib 90 mg had the same analgesic effect as ibuprofen 600 mg (16.11 vs. 16.39; P = 0.722) and was superior to the combination. paracetamol/codeine 600 mg/60 mg (11.00, P < 0.001) and placebo (6.84, P < 0.001) according to the Total Pain Relief in the First 6 Hours (TOPAR6) score. The proportion of patients who required rapid-acting pain medications within the first 24 hours of study drug use was 40.8% with etoricoxib 90 mg, 25.5% with ibuprofen 600 mg every 6 hours, and 46.7 % when using a combination of paracetamol/codeine at a dose of 600 mg/60 mg every 6 hours compared with 76.2% in the placebo group. In this study, the median onset of action (perceived pain relief) with etoricoxib 90 mg was 28 minutes after dosing.
Safety
Multinational Program for the Evaluation of Long-Term Use of Etoricoxib and Diclofenac in Arthritis (MEDAL)
The MEDAL program was a prospective safety assessment program based on cardiovascular (CV) events from pooled data from three randomized, double-blind, active-controlled studies: MEDAL, EDGE II, and EDGE.
The MEDAL study was a duration-of-endpoint (SS) study of 17,804 patients with OA and 5,700 patients with RA who received etoricoxib 60 (OA) or 90 mg (OA and RA) or diclofenac 150 mg. per day for an average of 20.3 months (maximum 42.3 months, median 21.3 months). In this study, only serious adverse events and dropouts due to any adverse events were recorded.
The EDGE and EDGE II studies compared the gastrointestinal tolerability of etoricoxib and diclofenac. The EDGE study included 7111 patients with OA who received etoricoxib 90 mg per day (1.5 times the dose recommended for OA) or diclofenac 150 mg per day for an average of 9.1 months (maximum 16.6 months, median 11.4 months). The EDGE II study included 4086 patients with RA who received etoricoxib 90 mg daily or diclofenac 150 mg daily for an average of 19.2 months (maximum 33.1 months, median 24 months).
In the combined MEDAL Program, 34,701 patients with OA or RA were treated for an average of 17.9 months (maximum 42.3 months, median 16.3 months), and approximately 12,800 patients were treated for more than 24 months. Patients enrolled in the MEDAL Program had a wide range of cardiovascular and gastrointestinal risk factors at baseline assessment. Patients with a recent myocardial infarction, as well as coronary artery bypass grafting or percutaneous coronary intervention within 6 months before inclusion in the study were excluded. The studies allowed the use of gastroprotectors and low-dose aspirin.
General security
There were no significant differences between etoricoxib and diclofenac in the incidence of thrombotic cardiovascular events. Cardiorenal adverse events were observed more frequently with etoricoxib than with diclofenac; this effect was dose-dependent (selected results are presented below). Adverse events from the gastrointestinal tract and liver were significantly more often observed when prescribing diclofenac than when prescribing etoricoxib. The incidence of adverse events in the EDGE and EDGE II studies, as well as adverse events considered serious or requiring treatment discontinuation in the MEDAL study, was higher with etoricoxib than with diclofenac.
Cardiovascular safety results
The incidence of confirmed serious thrombotic cardiovascular adverse events (including cardiac, cerebrovascular and peripheral vascular events) was comparable between the groups receiving etoricoxib or diclofenac (data are shown in the table below). There were no statistically significant differences in the incidence of thrombotic events between etoricoxib and diclofenac in all analyzed subgroups, including categories of patients in the range of baseline cardiovascular risk. When considered individually, the relative risks for confirmed serious thrombotic cardiovascular adverse events were similar for etoricoxib (60 mg or 90 mg doses) and diclofenac (150 mg doses).
Table “Rate of Confirmed Thrombotic Cardiovascular Events (MEDAL Program)”
| Etoricoxib (N=16819) 25836 patient-years | Diclofenac (N=16483) 24766 patient-years | Comparison between treatments | |
| Frequency1 (95% CI) | Frequency1 (95% CI) | Relative risk (95% CI) | |
| Confirmed thrombotic cardiovascular serious adverse events | |||
| When meeting protocol requirements | 1,24 (1,11, 1,38) | 1,30 (1,17, 1,45) | 0,95 (0,81, 1,11) |
| Depending on the prescribed treatment | 1,25 (1,14, 1,36) | 1,19 (1,08, 1,30) | 1,05 (0,93, 1,19) |
| Confirmed cardiac events | |||
| When meeting protocol requirements | 0,71 (0,61, 0,82) | 0,78 (0,68, 0,90) | 0,90 (0,74,1,10) |
| Depending on the prescribed treatment | 0,69 (0,61, 0,78) | 0,70 (0,62, 0,79) | 0,99 (0,84, 1,17) |
| Confirmed cerebrovascular events | |||
| When meeting protocol requirements | 0,34 (0,28, 0,42) | 0,32 (0,25, 0,40) | 1,08 (0,80, 1,46) |
| Depending on the prescribed treatment | 0,33 (0,28, 0,39) | 0,29 (0,24, 0,35) | 1,12 (0,87, 1,44) |
| Confirmed peripheral vascular events | |||
| When meeting protocol requirements | 0,20 (0,15,0,27) | 0,22 (0,17, 0,29) | 0,92 (0,63, 1,35) |
| Depending on the prescribed treatment | 0,24 (0,20, 0,30) | 0,23 (0,18, 0,28) | 1,08 (0,81, 1,44) |
| 1 Number of events per 100 patient-years; CI=confidence interval; N=total number of patients included in the protocol-compliant patient population. If the requirements of the protocol are met, all events that developed during study therapy or within 14 days of its cessation (patients who received <75% of the study drug and patients who took NSAIDs not included in the study >10% of the time are excluded). Depending on the assigned treatment, all confirmed events that occurred before the end of the study (included patients who may have undergone non-study interventions after discontinuation of the study drug). Total number of patients randomized: n=17412 for etoricoxib and n=17289 for diclofenac. | |||
Both CV mortality and all-cause mortality were comparable between the etoricoxib and diclofenac treatment groups.
Cardiorenal phenomena
Approximately 50% of patients enrolled in the MEDAL study had a history of hypertension at baseline assessment. In this study, the dropout rate due to hypertension-related adverse events was statistically significantly higher for etoricoxib than for diclofenac. The incidence of adverse events associated with chronic heart failure (study withdrawals and serious events) was similar for etoricoxib 60 mg and diclofenac 150 mg, but was higher for etoricoxib 90 mg compared with diclofenac 150 mg. mg (statistically significantly higher for etoricoxib 90 mg compared to diclofenac 150 mg in the OA group of the MEDAL study). The incidence of confirmed adverse events associated with chronic heart failure (events that were serious and resulted in hospitalization or an emergency department visit) was not significantly higher for etoricoxib compared with diclofenac 150 mg, and this effect was dose-related. The rate of withdrawal from the study due to adverse events related to edema was higher for etoricoxib compared with diclofenac 150 mg, and this effect was dose-related (statistically significant for etoricoxib 90 mg, but not for etoricoxib 60 mg) .
Cardiorenal safety results from the EDGE and EDGE II studies are consistent with those from the MEDAL study
In the individual MEDAL Program studies, the absolute dropout rate in any treatment arm for etoricoxib (60 mg or 90 mg) was up to 2.6% due to hypertension, up to 1.9% due to edema, and up to 1.1% due to association with chronic heart failure. Patients treated with etoricoxib 90 mg had a higher dropout rate than patients treated with etoricoxib 60 mg.
Results of gastrointestinal tolerance assessment in the MEDAL Program
In each of the three studies included in the MEDAL Program, the dropout rate for any clinical GI adverse event (eg, dyspepsia, abdominal pain, ulcers) was significantly lower for etoricoxib compared with diclofenac. The rate of withdrawal from the study due to adverse clinical events from the gastrointestinal tract per 100 patient-years for the entire study period was as follows: 3.23 for etoricoxib and 4.96 for diclofenac in the MEDAL study; 9.12 for etoricoxib and 12.28 for diclofenac in the EDGE study; and 3.71 for etoricoxib and 4.81 for diclofenac in the EDGE II study.
Results of the gastrointestinal safety assessment in the MEDAL Program
Overall, upper gastrointestinal adverse events were defined as perforation, ulceration, and bleeding. Complicated upper GI adverse events included perforation, obstruction, and complicated bleeding; uncomplicated upper GI adverse events included uncomplicated bleeding and uncomplicated ulcers. The overall incidence of upper gastrointestinal adverse events was significantly lower for etoricoxib compared with diclofenac. No significant differences were found between etoricoxib and diclofenac in the incidence of complicated events. For the subgroup of upper gastrointestinal hemorrhagic adverse events (complicated and uncomplicated combined), no significant differences were found between etoricoxib and diclofenac. The upper GI benefit of etoricoxib compared with diclofenac in patients taking concomitant low-dose aspirin (about 33% of patients) was not statistically significant.
The incidence of confirmed complicated and uncomplicated upper gastrointestinal clinical adverse events per 100 patient-years (perforation, ulceration and bleeding (PUB)) was 0.67 (95% CI 0.57, 0.77) for etoricoxib and 0.97 (95% CI 0.85, 1.10) for diclofenac, resulting in a relative risk of 0.69 (95% CI 0.57, 0.83).
The incidence of confirmed upper gastrointestinal adverse events in elderly patients was studied; the greatest reduction in incidence was observed in patients aged ≥75 years (1.35 [95% CI 0.94, 1.87] vs. 2.78 [95% CI 2.14, 3.56]) events per 100 patients -years for etoricoxib and diclofenac, respectively. The incidence of confirmed lower gastrointestinal adverse events (small or large bowel perforation, obstruction or bleeding (OB)) was not significantly different between etoricoxib and diclofenac.
Liver Safety Results from the MEDAL Program
Etoricoxib had a statistically significantly lower rate of withdrawal from the study due to adverse liver events compared with diclofenac. In the pooled MEDAL Program, 0.3% of patients receiving etoricoxib and 2.7% of patients receiving diclofenac withdrew from the study due to liver adverse events. The incidence of adverse events per 100 patient-years was 0.22 for etoricoxib and 1.84 for diclofenac (p < 0.001 for etoricoxib versus diclofenac). However, the majority of liver adverse events in the MEDAL Program were non-serious.
Additional safety data related to thrombotic cardiovascular events
In clinical studies excluding the MEDAL Program studies, approximately 3100 patients received etoricoxib at a dose of ≥60 mg per day for 12 weeks or longer. There were no significant differences in the incidence of confirmed serious thrombotic cardiovascular events in patients receiving etoricoxib ≥60 mg, placebo, or non-naproxen NSAIDs.
However, compared with patients receiving naproxen 500 mg twice daily, the incidence of these events was higher in patients receiving etoricoxib. The difference in antiplatelet activity between some COX-1 inhibitory NSAIDs and selective COX-2 inhibitors may be of clinical significance in patients at risk for thromboembolic events. Selective COX-2 inhibitors suppress the formation of systemic (and, as a consequence, possibly endothelial) prostacyclin without affecting platelet thromboxane. The clinical significance of these observations has not been established.
Additional gastrointestinal safety data
In two double-blind endoscopic studies lasting 12 weeks, the cumulative incidence of gastroduodenal ulcers was significantly lower in patients receiving etoricoxib 120 mg once daily than in patients receiving naproxen 500 mg twice daily or ibuprofen 800 mg. mg three times a day. The incidence of ulcers was higher for etoricoxib compared with placebo.
Renal function testing in the elderly
A randomized, double-blind, placebo-controlled, parallel group study assessed the effects of 15 days of treatment with etoricoxib (90 mg), celecoxib (200 mg twice daily), naproxen (500 mg twice daily), and placebo on renal sodium excretion, arterial blood pressure and other measures of renal function in patients aged 60 to 85 years receiving a diet containing 200 mEq/day sodium. Etoricoxib, celecoxib, and naproxen had similar effects on renal sodium excretion after 2 weeks of treatment. All active comparators increased systolic blood pressure relative to placebo, but etoricoxib resulted in a statistically significant increase at day 14 compared with celecoxib and naproxen (mean change from baseline in systolic blood pressure: etoricoxib 7.7 mm Hg, celecoxib - 2.4 mm Hg, naproxen - 3.6 mm Hg).