Pharmacological properties of the drug Gizaar forte
Pharmacodynamics . Gizaar Forte is a combination drug consisting of losartan (Cozaar) and hydrochlorothiazide. In patients with hypertension (arterial hypertension) and left ventricular hypertrophy, the use of losartan, often in combination with hydrochlorothiazide, reduces the risk of cardiovascular disease and mortality, which was proven when assessing the combined incidence of cardiovascular mortality, stroke and myocardial infarction. The components of the drug Gizaar Forte have an additive hypotensive effect, reducing blood pressure levels to a greater extent than each of the components separately. As a result of the diuretic effect of hydrochlorothiazide, the activity of plasma renin increases, the secretion of aldosterone is stimulated, the level of angiotensin II increases and the level of potassium in the blood plasma decreases. Taking losartan inhibits all physiological effects of angiotensin II, reduces the severity of the action of aldosterone, which reduces the loss of potassium associated with taking the diuretic. Losartan has a moderate transient uricosuric effect. Hydrochlorothiazide slightly increases the level of uric acid in the blood plasma. The combined use of losartan and hydrochlorothiazide helps reduce the degree of hyperuricemia caused by taking a diuretic. Losartan Angiotensin II is a powerful vasoconstrictor, the main active hormone of the renin-angiotensin system, as well as a leading pathophysiological factor in the development of hypertension (arterial hypertension). Angiotensin II binds to the AT1 receptor, found in many tissues (eg vascular smooth muscle, adrenal glands, kidneys and heart), and mediates a cascade of important biological effects, including vasoconstriction and aldosterone release. Angiotensin II also stimulates the proliferation of smooth muscle cells. The role of another type of angiotensin II receptor, AT2 receptors, in the homeostasis of the cardiovascular system has not been studied. Losartan is a synthetic drug that is highly effective when taken orally. Angiotensin II selectively binds to AT1 receptors. Losartan and its pharmacologically active metabolite (E-3174) in vitro and in vivo block all physiologically significant effects of angiotensin II, regardless of the source or route of its synthesis. Unlike some peptides - angiotensin II antagonists - losartan does not have an agonistic effect. Losartan selectively binds to AT1 receptors and does not bind or block receptors of other hormones and ion channels that play an important role in regulating the functions of the cardiovascular system. In addition, losartan does not inhibit ACE, which promotes the breakdown of bradykinin. In this regard, effects not directly related to blockade of AT1 receptors (for example, increased effects of bradykinin or the development of edema in the group of patients taking losartan - 1.7%, taking placebo - 1.9%), are not related to the action losartan. In this regard, effects not directly related to AT1 receptor blockade are not associated with the use of losartan. Hydrochlorothiazide The mechanism of the hypotensive effect of thiazides has not been studied. Thiazides usually have no effect when blood pressure is normal. Hydrochlorothiazide is a diuretic and antihypertensive agent, affects the reabsorption of electrolytes in the distal tubules of the kidneys and increases the excretion of sodium chloride to approximately the same extent. Natriuresis may be accompanied by a slight loss of potassium and bicarbonate ions. When taken orally, the diuretic effect develops after 2 hours, the maximum effect occurs within 4 hours and lasts for 6–12 hours. Pharmacodynamics Losartan When taking losartan, negative feedback is inhibited, which consists of inhibition of renin secretion by angiotensin II, which leads to an increase blood plasma renin activity (PRA). An increase in ARP is accompanied by an increase in the level of angiotensin II in the blood plasma. During long-term treatment of patients with hypertension (arterial hypertension) (for 6 weeks) with losartan at a dose of 100 mg/day, a 3-fold increase in the level of angiotensin II in the blood plasma was observed at the time the maximum concentration of the drug in the blood plasma was reached. In some patients, the level of angiotensin II increased more significantly, especially with a short duration of treatment (2 weeks). However, a hypotensive effect and a decrease in plasma aldosterone concentrations were noted after 2 and 6 weeks of therapy, respectively, indicating effective blockade of angiotensin II receptors. ARP and angiotensin II levels return to baseline levels 3 days after discontinuation of losartan. The effect of losartan potassium hydrochlorothiazide 50/12.5 mg on ARP and angiotensin II levels was compared with that of losaratan 50 mg. A comparison of the effect of losartan potassium-hydrochlorothiazide at a dose of 100/12.5 mg and losartan at a dose of 50 mg on ARP and angiotensin II levels was not performed. Since losartan is a specific antagonist of angiotensin II AT1 receptors, it does not inhibit ACE kinase II, an enzyme that inactivates bradykinin. A study comparing the effects of losartan potassium (20 mg and 100 mg) with the effects of an ACE inhibitor on the activity of angiotensin I, angiotensin II and bradykinin showed that losartan blocked the effects of angiotensin I, angiotensin II, without affecting the effects bradykinin. These results are consistent with the specific mechanism of action of losartan. Conversely, the ACE inhibitor blocked the effect of angiotensin I and increased the effect of bradykinin, without affecting the severity of the effect of angiotensin II, which indicates a difference in the pharmacodynamics of losartan and ACE inhibitors. The concentration of losartan and its active metabolite in the blood plasma, as well as the hypotensive effect of losartan, increases with increasing doses of the drug. Since losartan and its active metabolite are angiotensin II receptor antagonists, they do not have a significant effect on the hypotensive effect. In a clinical study, a single dose of losartan potassium 100 mg in healthy male subjects on a high- or low-salt diet did not affect glomerular filtration rate (GFR), effective renal plasma flow, or filtration fraction. Losartan has a natriuretic effect, which is more pronounced when following a low-salt diet and is not associated with inhibition of early sodium reabsorption in the proximal tubules of the kidneys. Losartan also temporarily increases the secretion of uric acid by the kidneys. In patients with hypertension (arterial hypertension), proteinuria (2 g/day) without concomitant diabetes mellitus, when taking losartan for 8 weeks at an initial dose of 50 mg with a gradual increase to 100 mg, a significant decrease in proteinuria by 42% was detected. Fractional excretion of albumin and IgG was also significantly reduced. In these patients, taking losartan stabilized GFR and reduced the filtration fraction. In postmenopausal women with hypertension (arterial hypertension), who took losartan potassium at a dose of 50 mg/day for 4 weeks, there was no effect of therapy on the renal and systemic levels of prostaglandins. Losartan does not affect autonomic reflexes and does not have a long-term effect on the level of norepinephrine in the blood plasma. In patients with hypertension (arterial hypertension), lozaratan in doses up to 150 mg/day did not cause clinically significant changes in TG levels when taken on an empty stomach, total cholesterol and HDL cholesterol. At the same doses, losartan had no effect on blood glucose levels when taken on an empty stomach. In general, losartan caused a decrease in serum uric acid levels (usually less than 0.4 mg/dL), which was maintained during long-term therapy. During controlled clinical studies in patients with hypertension (arterial hypertension), cases of drug withdrawal due to an increase in serum creatinine or potassium levels were not recorded. A 12-week parallel clinical trial, which included patients with left ventricular failure (NYHA class II–IV), most of whom were taking diuretics and/or cardiac glycosides, compared the effects of losartan at doses of 2.5; 10; 25 and 50 mg/day with placebo. At doses of 25 and 50 mg/day, the drug had positive hemodynamic and neurohumoral effects, which persisted throughout the study. The hemodynamic effect included an increase in cardiac index and a decrease in pulmonary capillary wedge pressure, as well as a decrease in systemic vascular resistance, mean systemic blood pressure and heart rate. The incidence of arterial hypotension in patients depended on the dose of the drug. The neurohumoral effect included a decrease in plasma aldosterone and norepinephrine levels. Pharmacokinetics. Suction . Losartan When taken orally, losartan is well absorbed and, as a result of metabolism during the initial passage through the liver, an active carboxylated metabolite and inactive metabolites are formed. The systemic bioavailability of losartan when taken orally is about 33%. The average maximum concentrations of losartan and its active metabolite in blood plasma are achieved within 1 hour and 3–4 hours, respectively. Taking losartan with food does not have a clinically significant effect on the drug concentration profile in the blood plasma. Distribution The binding of losartan and its active metabolite to plasma proteins (mainly albumin) is more than 99%. The volume of distribution of losartan is 34 l. Animal studies have shown that losartan practically does not penetrate the BBB. Hydrochlorothiazide Hydrochlorothiazide penetrates the placental barrier (but not the BBB) and is excreted into breast milk. Metabolism . Losartan When administered intravenously or orally, about 14% of the dose of losartan is metabolized to form an active metabolite. After oral and IV administration of C14-labeled losartan, the radioactivity of circulating plasma was determined mainly by the presence of losartan and its active metabolite. In addition to the active metabolite, biologically inactive ones are formed, two of which are the main metabolites formed due to hydroxylation of the butyl side chain, and one minor one is N-2-tetrazole glucuronide. Elimination Plasma clearance of losartan is about 600 ml/min, its active metabolite is 50 ml/min. The renal clearance of losartan is about 74 ml/min, the active metabolite is 26 ml/min. When losartan is taken orally, about 4% of the dose is excreted unchanged in the urine and about 6% as the active metabolite. Losartan and its active metabolite have linear pharmacokinetics when administered orally with losartan in doses up to 200 mg. After oral administration, the plasma concentration of losartan and its active metabolite decreases polyexponentially with a terminal half-life of approximately 2 and 6–9 hours, respectively. With a single dose of 100 mg/day, the accumulation of losartan and its active metabolite in the blood plasma is insignificant. Losartan and its metabolites are excreted in bile and urine. After oral administration of C14-labeled losartan, about 35% of radioactivity is detected in urine and 58% in feces. After intravenous administration of C14-labeled losartan, about 43% of radioactivity is determined in urine and 50% in feces. Hydrochlorothiazide Hydrochlorothiazide is not metabolized and is rapidly excreted by the kidneys. When plasma drug levels were monitored for at least 24 hours, the half-life ranged from 5.6 to 14.8 hours. When administered orally, at least 61% of the administered dose was excreted unchanged within 24 hours. Pharmacokinetics in special patient groups Patients elderly Losartan - hydrochlorothiazide The concentration of losartan and its active metabolite in the blood plasma and the rate of absorption of hydrochlorothiazide in elderly patients with hypertension (arterial hypertension) do not differ significantly from these indicators in young patients with hypertension (arterial hypertension). Losartan. Gender of patients The concentration of losartan in blood plasma was 2 times higher in women with hypertension (arterial hypertension) compared to men with hypertension (arterial hypertension). The concentration of the active metabolite in the blood plasma did not differ between women and men. This feature of the pharmacokinetics of the drug has no clinical significance. Patients with impaired liver and kidney function When taking losartan orally in patients with mild and moderate alcoholic cirrhosis, the concentration of the drug and its active metabolite in the blood plasma was respectively 5–1.7 times higher than in healthy male subjects. Plasma concentrations of losartan in patients with creatinine clearance above 10 ml/min did not differ from those in individuals with normal renal function. When compared, the AUC value in patients on hemodialysis was approximately 2 times greater than in patients with normal renal function. The concentration of the active metabolite in the blood plasma does not change in patients with impaired renal function or in patients on hemodialysis. Losartan and its active metabolite are not excreted by hemodialysis.
Instructions for use GIZAAR® (HYZAAR)
Combination antihypertensive drug.
The active substances of the drug Gizaar® have an additive antihypertensive effect, reducing blood pressure to a greater extent than each of the components separately. Due to the diuretic effect, hydrochlorothiazide increases plasma renin activity (PRA), stimulates the secretion of aldosterone, increases the level of angiotensin II and reduces the level of potassium in the blood serum. Taking losartan blocks all physiological effects of angiotensin II and, by suppressing the effects of aldosterone, helps reduce potassium loss caused by taking the diuretic.
Losartan has a moderate and transient uricosuric effect. Hydrochlorothiazide causes a slight increase in uric acid levels in the blood; the combination of losartan and hydrochlorothiazide helps reduce the severity of diuretic-induced hyperuricemia.
Losartan
Losartan is an angiotensin II receptor antagonist. Angiotensin II is a powerful vasoconstrictor, the main active hormone of the renin-angiotensin system, as well as a decisive pathophysiological link in the development of arterial hypertension. Angiotensin II binds to receptors of the AT1 subtype, found in many tissues (for example, vascular smooth muscle, adrenal glands, kidneys and heart) and causes a number of important biological effects, including. vasoconstriction and aldosterone release. Angiotensin II also stimulates the proliferation of smooth muscle cells. The role of the second type of angiotensin II receptor, the AT2 subtype, in cardiovascular homeostasis is unknown.
Losartan is a highly effective synthetic drug when taken orally. Angiotensin II selectively binds to AT1 receptors. Losartan and its pharmacologically active metabolite (E-3174) both in vitro and in vivo block all physiological effects of angiotensin II, regardless of the source or route of synthesis. Unlike some peptide angiotensin II antagonists, losartan does not have agonist effects.
Losartan selectively binds to AT1 receptors and does not bind to or block receptors of other hormones and ion channels that play an important role in regulating the function of the cardiovascular system. In addition, losartan does not inhibit ACE, which promotes the degradation of bradykinin. Therefore, effects not directly related to AT1 receptor blockade, in particular, increased effects associated with bradykinin or the development of edema (losartan 1.7%, placebo 1.9%), are not related to the action of losartan.
Losartan eliminates the negative feedback consisting in the suppression of renin secretion by angiotensin II, which leads to an increase in blood ARP. An increase in ARP is accompanied by an increase in plasma angiotensin II levels. With long-term (6-week) treatment of patients with arterial hypertension with losartan at a dose of 100 mg/day, at the time the maximum concentration of the drug in the blood plasma was reached, a 2-3-fold increase in the level of angiotensin II was observed. Some patients experienced an even greater increase, especially with a short duration of treatment (2 weeks). Antihypertensive activity and a decrease in plasma aldosterone concentrations appear after 2-6 weeks of therapy, indicating effective blockade of angiotensin II receptors. ARP and angiotensin II levels decrease to baseline values 3 days after discontinuation of losartan. The effects of Gizaar on ARP and angiotensin II levels were comparable to those observed with 50 mg losartan.
Since losartan is a specific antagonist of angiotensin II AT1 receptors, it does not inhibit ACE (kininase II), an enzyme that inactivates bradykinin. The results of a study that compared the effects of 20 mg and 100 mg of losartan and an ACE inhibitor on angiotensin I, angiotensin II and bradykinin showed that losartan blocked the effects of angiotensin I and angiotensin II without affecting the effects of bradykinin. These data confirm the specific mechanism of action of losartan. In turn, the ACE inhibitor blocked the response to angiotensin I and increased the response to bradykinin without affecting the response to angiotensin II, demonstrating a pharmacodynamic difference between losartan and ACE inhibitors.
Plasma concentrations of losartan and its active metabolite, as well as the antihypertensive effect of losartan, increase with increasing dose of the drug. Since losartan and its active metabolite are angiotensin II receptor antagonists, they both contribute to the antihypertensive effect.
In a clinical study with a single dose of 100 mg of losartan, which included healthy male volunteers, taking the drug with a high- and low-salt diet did not affect the glomerular filtration rate (GFR), effective renal plasma flow and renal filtration fraction. Losartan has a natriuretic effect, which was more pronounced with a low-salt diet and did not appear to be associated with suppression of early sodium reabsorption in the proximal renal tubules. Losartan also caused a transient increase in renal excretion of uric acid.
In patients with arterial hypertension, proteinuria (> 2 g/day), who do not have diabetes mellitus and took losartan for 8 weeks at a dose of 50 mg with a gradual increase to 100 mg, there was a significant decrease in proteinuria by 42%. Fractional excretion of albumin and IgG also decreased significantly. In these patients, losartan stabilized GFR and reduced the filtration fraction.
In postmenopausal women with arterial hypertension who took losartan at a dose of 50 mg/day for 4 weeks, there was no effect of therapy on renal and systemic levels of prostaglandins.
Losartan does not affect autonomic reflexes and does not have a long-term effect on plasma norepinephrine levels. In patients with arterial hypertension, losartan in doses up to 150 mg/day did not cause clinically significant changes in the levels of fasting triglycerides, total cholesterol and HDL cholesterol. At the same doses, losartan had no effect on fasting blood glucose levels.
In general, losartan caused a decrease in serum uric acid levels (usually less than 0.4 mg/dL) that persisted during long-term therapy. In controlled clinical studies that included patients with arterial hypertension, there were no cases of drug withdrawal due to increases in serum creatinine or potassium levels.
A 12-week, parallel, placebo-controlled study in patients with left ventricular failure (NYHA functional class II-IV), most of whom were receiving diuretics and/or digitalis, compared the effects of losartan potassium at doses of 2.5, 10, 25 and 50 mg/day. days At doses of 25 mg and 50 mg/day, the drug had positive hemodynamic and neurohormonal effects, which were observed throughout the study. Hemodynamic effects included an increase in cardiac index and a decrease in pulmonary capillary wedge pressure, as well as a decrease in peripheral vascular resistance, mean systemic blood pressure, and heart rate. The incidence of arterial hypotension in these patients depended on the dose of the drug. Neurohormonal effects manifested themselves in the form of a decrease in the level of aldosterone and norepinephrine in the blood.
In patients with arterial hypertension and left ventricular hypertrophy, losartan, often in combination with hydrochlorothiazide, reduces the risk of cardiovascular morbidity and mortality, which was demonstrated by assessing the combined incidence of stroke and myocardial infarction, as well as the rate of cardiovascular mortality in this category patients.
Hydrochlorothiazide
The mechanism of the antihypertensive effect of thiazides is unknown. Thiazides usually have no effect on normal blood pressure levels.
Hydrochlorothiazide is a diuretic and antihypertensive agent. It affects the reabsorption of electrolytes in the distal tubules of the kidneys. Hydrochlorothiazide approximately equally increases the excretion of sodium and chloride. Natriuresis may be accompanied by a slight loss of potassium and bicarbonate ions.
When taken orally, the diuretic effect begins after 2 hours, reaches a maximum after an average of 4 hours and lasts from 6 to 12 hours.
Use of the drug Gizaar forte
Gizaar Forte is taken regardless of meals. The drug can be prescribed in combination with other antihypertensive drugs. AH (arterial hypertension) The usual initial and maintenance dose of Gizaar is 50/12.5 mg (1 tablet 1 time per day). In patients without a therapeutic effect when taking 1 tablet of Gizaar (50/12.5 mg) for 2–4 weeks, the dose of the drug can be increased to 2 tablets of Gizaar (50/12.5 mg) or 1 tablet of Gizaar Forte (100/12 .5 mg) 1 time per day. The maximum dose is 2 tablets of Gizaar 50/12.5 mg or 1 tablet of Gizaar Forte 100/12.5 mg 1 time per day. As a rule, the hypotensive effect is achieved within 3 weeks after the start of treatment. Selection of the initial dose of the drug - 1 tablet of Gizaar containing 50/12.5 mg - is not required in elderly patients. In elderly patients, Gizaar should not be used as initial therapy at a dose of 2 tablets of 50/12.5 mg or 1 tablet of 100/12.5 mg. Reducing the risk of cardiovascular complications and mortality in patients with hypertension (arterial hypertension) and hypertrophy left ventricle The standard initial dose of losartan is 50 mg 1 time per day. In patients who fail to achieve the target blood pressure level when taking losartan at a dose of 50 mg / day, a combination of losartan and low doses of hydrochlorothiazide (12.5 mg) should be used and, if necessary, the dose of losartan should be increased to 100 mg / day in combination with hydrochlorothiazide at a dose of 12.5 mg/day (1 tablet of Gizaar Forte), then increase the dose to 2 tablets of Gizaar (50 mg/12.5 mg) once a day (total 100 mg of losartan and 25 mg of hydrochlorothiazide). The duration of treatment is determined individually.
Hyzaar® forte
Combination antihypertensive drug.
The active substances of the drug Gizaar® have an additive antihypertensive effect, reducing blood pressure to a greater extent than each of the components separately. Due to the diuretic effect, hydrochlorothiazide increases plasma renin activity (PRA), stimulates the secretion of aldosterone, increases the level of angiotensin II and reduces the level of potassium in the blood serum. Taking losartan blocks all physiological effects of angiotensin II and, by suppressing the effects of aldosterone, helps reduce potassium loss caused by taking the diuretic.
Losartan has a moderate and transient uricosuric effect. Hydrochlorothiazide causes a slight increase in uric acid levels in the blood; the combination of losartan and hydrochlorothiazide helps reduce the severity of diuretic-induced hyperuricemia.
Losartan
Losartan is an angiotensin II receptor antagonist.
Angiotensin II is a powerful vasoconstrictor, the main active hormone of the renin-angiotensin system, as well as a decisive pathophysiological link in the development of arterial hypertension. Angiotensin II binds to receptors of the AT1 subtype, found in many tissues (for example, vascular smooth muscle, adrenal glands, kidneys and heart) and causes a number of important biological effects, including. vasoconstriction and aldosterone release. Angiotensin II also stimulates the proliferation of smooth muscle cells. The role of the second type of angiotensin II receptor, the AT2 subtype, in cardiovascular homeostasis is unknown.
Angiotensin II selectively binds to AT1 receptors. Losartan and its pharmacologically active metabolite (E-3174) both in vitro and in vivo block all physiological effects of angiotensin II, regardless of the source or route of synthesis. Unlike some peptide angiotensin II antagonists, losartan does not have agonist effects.
Losartan selectively binds to AT1 receptors and does not bind to or block receptors of other hormones and ion channels that play an important role in regulating the function of the cardiovascular system. In addition, losartan does not inhibit ACE, which promotes the degradation of bradykinin. Therefore, effects not directly related to AT1 receptor blockade, in particular, increased effects associated with bradykinin or the development of edema (losartan 1.7%, placebo 1.9%), are not related to the action of losartan.
Losartan eliminates the negative feedback consisting in the suppression of renin secretion by angiotensin II, which leads to an increase in blood ARP. An increase in ARP is accompanied by an increase in plasma angiotensin II levels. With long-term (6-week) treatment of patients with arterial hypertension with losartan at a dose of 100 mg/day, at the time the maximum concentration of the drug in the blood plasma was reached, a 2-3-fold increase in the level of angiotensin II was observed. Some patients experienced an even greater increase, especially with a short duration of treatment (2 weeks). Antihypertensive activity and a decrease in plasma aldosterone concentrations appear after 2-6 weeks of therapy, indicating effective blockade of angiotensin II receptors. ARP and angiotensin II levels decrease to baseline values 3 days after discontinuation of losartan. The effects of Gizaar on ARP and angiotensin II levels were comparable to those observed with 50 mg losartan.
Since losartan is a specific antagonist of angiotensin II AT1 receptors, it does not inhibit ACE (kininase II), an enzyme that inactivates bradykinin. The results of a study that compared the effects of 20 mg and 100 mg of losartan and an ACE inhibitor on angiotensin I, angiotensin II and bradykinin showed that losartan blocked the effects of angiotensin I and angiotensin II without affecting the effects of bradykinin. These data confirm the specific mechanism of action of losartan. In turn, the ACE inhibitor blocked the response to angiotensin I and increased the response to bradykinin without affecting the response to angiotensin II, demonstrating a pharmacodynamic difference between losartan and ACE inhibitors.
Plasma concentrations of losartan and its active metabolite, as well as the antihypertensive effect of losartan, increase with increasing dose of the drug. Since losartan and its active metabolite are angiotensin II receptor antagonists, they both contribute to the antihypertensive effect.
In a clinical study with a single dose of 100 mg of losartan, which included healthy male volunteers, taking the drug with a high- and low-salt diet did not affect the glomerular filtration rate (GFR), effective renal plasma flow and renal filtration fraction. Losartan demonstrated a natriuretic effect that was more pronounced with a low-salt diet and did not appear to be associated with suppression of early sodium reabsorption in the proximal renal tubules. Losartan also caused a transient increase in renal excretion of uric acid.
In patients with arterial hypertension, proteinuria (> 2 g/day), who do not have diabetes mellitus and took losartan for 8 weeks at a dose of 50 mg with a gradual increase to 100 mg, there was a significant decrease in proteinuria by 42%. Fractional excretion of albumin also decreased significantly. In these patients, losartan stabilized GFR and reduced the filtration fraction.
In postmenopausal women with arterial hypertension who took losartan at a dose of 50 mg/day for 4 weeks, there was no effect of therapy on renal and systemic levels of prostaglandins.
Losartan does not affect autonomic reflexes and does not have a long-term effect on plasma norepinephrine levels. In patients with arterial hypertension, losartan in doses up to 150 mg/day did not cause clinically significant changes in the levels of fasting triglycerides, total cholesterol and HDL cholesterol. At the same doses, losartan had no effect on fasting blood glucose levels.
In general, losartan caused a decrease in serum uric acid levels (usually less than 0.4 mg/dL) that persisted during long-term therapy. In controlled clinical studies that included patients with arterial hypertension, there were no cases of drug withdrawal due to increases in serum creatinine or potassium levels.
A 12-week, parallel, placebo-controlled study in patients with left ventricular failure (NYHA functional class II-IV), most of whom were receiving diuretics and/or digitalis, compared the effects of losartan potassium at doses of 2.5, 10, 25 and 50 mg/day. days At doses of 25 mg and 50 mg/day, the drug had positive hemodynamic and neurohormonal effects, which were observed throughout the study. Hemodynamic effects included an increase in cardiac index and a decrease in pulmonary capillary wedge pressure, as well as a decrease in peripheral vascular resistance, mean systemic blood pressure, and heart rate. Neurohormonal effects manifested themselves in the form of a decrease in the level of aldosterone and norepinephrine in the blood.
In patients with arterial hypertension and left ventricular hypertrophy, losartan, often in combination with hydrochlorothiazide, reduces the risk of cardiovascular morbidity and mortality, which was demonstrated by assessing the combined incidence of stroke and myocardial infarction, as well as the rate of cardiovascular mortality in this category patients.
Hydrochlorothiazide
The mechanism of the antihypertensive effect of thiazides is unknown. Thiazides usually have no effect on normal blood pressure levels.
Hydrochlorothiazide is a diuretic and antihypertensive agent. It affects the reabsorption of electrolytes in the distal tubules of the kidneys. Hydrochlorothiazide approximately equally increases the excretion of sodium and chloride. Natriuresis may be accompanied by a slight loss of potassium and bicarbonate ions.
When taken orally, the diuretic effect begins after 2 hours, reaches a maximum after an average of 4 hours and lasts from 6 to 12 hours.
Side effects of the drug Gizaar forte
In general, treatment with the drug is well tolerated. In most cases, side effects are moderate and short-term and do not require discontinuation of treatment. Hypersensitivity: anaphylactic reactions, angioedema, including swelling of the larynx and glottis with the development of airway obstruction and/or swelling of the face, lips, larynx and/or tongue. Some of these patients had a history of angioedema while using other drugs, including ACE inhibitors. Isolated cases of vasculitis, including Henoch-Schönlein disease, have been reported when taking losartan. From the gastrointestinal tract: there are isolated reports of the development of hepatitis and diarrhea. From the respiratory system: cases of cough have been reported while taking losartan. Skin disorders: urticaria. Other side effects that have been observed with each of the components of the drug may be potential side effects when taking Gizaara Forte. Associated with losartan: rash, dose-dependent orthostatic effects, abdominal pain, asthenia/fatigue, chest pain, edema/edema, palpitations, tachycardia, dyspepsia, nausea, back pain, muscle cramps, myalgia, headache, insomnia, cough, nasal congestion, pharyngitis, sinusitis, upper respiratory tract infections, migraine, liver dysfunction, anemia, prurigus. Associated with hydrochlorothiazide: anorexia, irritation of the gastric mucosa, nausea, vomiting, cramps, diarrhea, constipation, jaundice (intrahepatic cholestatic jaundice), pancreatitis, sialadenitis, vertigo, paresthesia, headache, xanthopsia, leukopenia, agranulocytosis, thrombocytopenia, aplastic anemia , hemolytic anemia, purpura, photosensitivity, fever, necrotizing angiitis (vasculitis), respiratory distress syndrome (including pneumonitis, pulmonary edema), toxic epidermal necrolysis, hyperglycemia, glycosuria, hyperuricemia, electrolyte imbalance, including hyponatremia and hypokalemia, renal dysfunction, muscle cramps, weakness, transient decrease in visual acuity. Changes in laboratory parameters Based on data from controlled clinical studies, clinically significant changes in standard laboratory parameters were rarely associated with the use of Gizaar Forte. Hyperkalemia (serum potassium level 5.5 mEq/L) was noted in 0.7% of patients, which was not a reason to discontinue therapy with Gizaar Forte. Increases in ALT levels were rare and usually returned to normal after discontinuation of therapy.
Special instructions for the use of the drug Gizaar forte
The drug should be prescribed with caution to the following categories of patients: with impaired water-electrolyte blood balance (dehydration, hyponatremia, hypochloremic alkalosis, hypomagnesemia, hypokalemia), which can develop with intercurrent diarrhea or vomiting. Patients with bilateral renal artery stenosis or stenosis of the artery of a single kidney; with diabetes mellitus, hypercalcemia, hyperuricemia and/or gout; with a burdened allergic history and asthma; systemic connective tissue diseases (including systemic lupus erythematosus); with hypovolemia (in patients receiving high doses of diuretics); and also when taken simultaneously with NSAIDs (including COX-2 inhibitors). The following provides data regarding the features of the use of some active components of the drug Gizaar Forte. These data should be taken into account when using it. Losartan Impaired renal function There is evidence of impaired renal function, including renal failure, that developed while taking the drug (due to inhibition of the function of the renin-angiotensin system). These changes may be reversible after cessation of therapy. Other drugs that act on the renin-angiotensin system may increase plasma urea and creatinine levels in patients with bilateral renal artery stenosis or arterial stenosis of a solitary kidney. Side effects were noted when taking losartan. These changes may be reversible and disappear after cessation of therapy. Hydrochlorothiazide Hypotension and electrolyte imbalance As with any antihypertensive drug, symptomatic hypotension may occur in some patients. It is necessary to monitor patients in order to promptly identify symptoms of fluid and electrolyte imbalance (for example, dehydration, hyponatremia, hypochloremic alkalosis, hypomagnesemia or hypokalemia), which may develop with intercurrent diarrhea or vomiting. In these patients, it is necessary to monitor the level of serum electrolytes. Metabolic and endocrine effects Thiazide therapy can lead to impaired glucose tolerance. In some cases, it may be necessary to adjust the dose of hypoglycemic drugs, including insulin. Thiazides may reduce urinary calcium excretion and cause occasional and mild increases in serum calcium levels. Severe hypercalcemia may indicate the presence of latent hyperparathyroidism. The thiazide diuretic should be discontinued before testing parathyroid function. An increase in the level of total cholesterol and TG in the blood plasma may also be associated with therapy with thiazide diuretics. In some patients, taking thiazide diuretics can lead to hyperuricemia and/or the development of gout. Since losartan reduces plasma uric acid levels, its combination with hydrochlorothiazide reduces the severity of diuretic-induced hyperuricemia. Other effects In patients taking thiazide diuretics, hypersensitivity reactions may occur even in the absence of allergic symptoms or a history of asthma. There is evidence of exacerbation or progression of systemic lupus erythematosus during treatment with thiazide diuretics. During pregnancy and breastfeeding. Drugs that directly act on the renin-angiotensin system, when used in the second or third trimester of pregnancy, can cause developmental pathology and even fetal death. Once pregnancy is established, the use of Gizaar Forte should be stopped immediately. Thiazide diuretics penetrate the placental barrier and are detected in the umbilical cord blood. The use of diuretics during pregnancy without other pathology is not recommended because this poses an unnecessary risk in the mother and fetus of developing disorders such as fetal and neonatal jaundice, thrombocytopenia, and possibly other adverse reactions observed in adults. Diuretics do not prevent the development of toxemia in pregnancy and there is no reliable evidence that they are effective in treating toxemia. It is not known whether losartan is excreted into breast milk. Thiazide diuretics pass into breast milk. The decision regarding discontinuation of therapy should be made taking into account the need for the drug for the mother. If it is necessary to take the drug, breastfeeding should be stopped, taking into account the potential for side effects in the child. Children. The safety and effectiveness of Gizaar Forte in children have not been established, therefore the drug is not used in pediatric practice. Impact on the ability to drive vehicles and operate other machinery. Considering the possibility of developing such adverse reactions as dizziness, loss of consciousness, arterial hypotension, muscle cramps, weakness, transient decrease in visual acuity, the drug should be used with caution when driving vehicles and operating other mechanisms.
Hyzaar®
Hydrochlorothiazide
Arterial hypotension and water-electrolyte imbalance
When using antihypertensive drugs, some patients may develop symptomatic arterial hypotension. Patients should be monitored for clinical signs of fluid and electrolyte imbalance, such as dehydration, hyponatremia, hypochloremic alkalosis, hypomagnesemia, or hypokalemia, which may occur with concomitant diarrhea or vomiting. In such patients, regular monitoring of serum electrolytes is necessary. Patients with edema may experience dilutional hyponatremia in hot weather.
Metabolic and endocrine effects
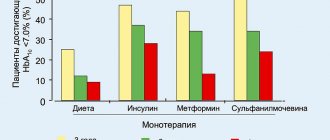
Thiazide therapy may impair glucose tolerance. In some cases, it may be necessary to adjust the dose of hypoglycemic drugs, including insulin (see Interaction with other drugs).
Thiazides may reduce renal excretion of calcium and cause a transient and slight increase in serum calcium. Severe hypercalcemia may indicate latent hyperparathyroidism. Due to the effect of thiazides on calcium metabolism, their use may distort the results of testing the function of the parathyroid glands, therefore, before testing the function of the parathyroid glands, the thiazide diuretic should be discontinued.
Increased concentrations of cholesterol and triglycerides in the blood may also be associated with therapy with thiazide diuretics.
In some patients, taking thiazide diuretics can lead to hyperuricemia and/or the development of gout. Since losartan reduces the concentration of uric acid, its simultaneous use with hydrochlorothiazide reduces the severity of hyperuricemia caused by the diuretic.
Liver dysfunction
Thiazides should be used with caution in patients with impaired liver function or progressive liver disease, as this can lead to the development of intrahepatic cholestasis, and minor changes in water and electrolyte balance can trigger the development of hepatic coma. Gizaar® is contraindicated in patients with severe liver dysfunction.
Choroidal effusion, acute myopia and secondary angle-closure glaucoma
Drugs based on sulfonamide or sulfonamide derivatives can cause an idiosyncratic reaction in the form of choroidal effusion with visual field defect, transient myopia and acute angle-closure glaucoma. Symptoms of these disorders include a sudden decrease in visual acuity or eye pain, which typically occurs within a few hours to several weeks after starting to use the drug. If left untreated, acute angle-closure glaucoma can lead to vision loss. The main treatment is to discontinue hydrochlorothiazide as quickly as possible. It is important to keep in mind that if intraocular pressure remains uncontrolled, emergency medical or surgical treatment may be required. Risk factors for the development of acute angle-closure glaucoma include a history of allergies to sulfonamides or penicillin.
Non-melanoma skin cancer (NMSC)
In epidemiological studies, an increased risk of non-melanoma skin cancer (basal cell carcinoma and squamous cell carcinoma) was observed due to an increase in the total (cumulative) dose of hydrochlorothiazide. A possible mechanism for the development of NMSC is the photosensitizing effect of hydrochlorothiazide.
Patients taking hydrochlorothiazide should be aware of the risk of developing NMSC. Such patients should be advised to follow preventative measures such as limiting exposure to sunlight and artificial UVA rays. Patients should regularly examine their skin to identify any new suspicious lesions and report them promptly to their physician. In patients with a history of NMSC, it is recommended to reconsider the advisability of using hydrochlorothiazide (see Side effects).
Other effects
In patients taking thiazide diuretics, hypersensitivity reactions may occur even in the absence of a history of allergic reactions or bronchial asthma. Relapses or worsening of the severity of systemic lupus erythematosus have been reported in patients taking thiazide diuretics.
Special patient groups
Race
An analysis of data from the entire population of patients included in the LIFE study to study the effect of losartan on reducing the incidence of the primary endpoint in patients with hypertension and left ventricular hypertrophy (n = 9193) showed that the ability of losartan to reduce compared to atenolol by 13.0% the risk of developing cardiovascular complications (p = 0.021) does not apply to patients of the black race, although both treatment regimens effectively reduced blood pressure in these patients. However, in this study, black patients receiving atenolol had a lower risk of the primary endpoint (cardiovascular mortality, stroke, and myocardial infarction) compared with race-matched patients receiving losartan (p = 0.03).
Children and teenagers
The effectiveness and safety of the use of Gizaar® in children and adolescents under 18 years of age have not been established.
If newborns whose mothers took the drug Gizaar during pregnancy develop oliguria or arterial hypotension, symptomatic therapy aimed at maintaining blood pressure and renal perfusion is necessary. Blood transfusions or dialysis may be required to prevent hypotension and/or maintain renal function.
Elderly patients
Clinical studies have not revealed any particularities regarding the safety and effectiveness of Gizaar® in elderly patients (over 65 years of age).
Losartan
Arterial hypotension and decreased circulating blood volume (CBV)
In patients with reduced blood volume or sodium content in the blood, which developed due to intensive diuretic therapy, a salt-restricted diet, diarrhea or vomiting, symptomatic arterial hypotension may develop, especially after taking the first dose of Gizaar®. Correction of such conditions must be carried out before prescribing the drug Gizaar®.
Water-electrolyte imbalance
Fluid and electrolyte imbalance is common in patients with renal failure with or without diabetes mellitus, so careful monitoring of these patients is necessary. Careful monitoring of potassium levels in the blood or CK is necessary, especially in patients with heart failure and CK 30-50 ml/min.
During treatment with Gizaar®, it is not recommended to take potassium-sparing diuretics, potassium supplements or potassium-containing salt substitutes. Aortic or mitral stenosis, hypertrophic obstructive cardiomyopathy
Like all drugs that have a vasodilating effect, ARA II should be prescribed with caution to patients with aortic or mitral stenosis or hypertrophic obstructive cardiomyopathy.
Coronary heart disease and cerebrovascular diseases
Like all drugs that have a vasodilating effect, ARA II should be prescribed with caution to patients with coronary heart disease or cerebrovascular diseases, since an excessive decrease in blood pressure in this group of patients can lead to the development of myocardial infarction or stroke.
Chronic heart failure (CHF)
As with the use of other drugs that act on the RAAS, patients with CHF and with or without impaired renal function are at risk of developing severe hypotension or acute renal failure.
Primary hyperaldosteronism
Since patients with primary hyperaldosteronism, as a rule, do not respond positively to therapy with antihypertensive drugs that act by inhibiting the RAAS, the use of Gizaar® is not recommended in this group of patients.
Liver dysfunction
Data from pharmacokinetic studies indicate that the concentration of losartan in the blood plasma in patients with cirrhosis of the liver is significantly increased, therefore patients with a history of mild or moderate impaired liver function should be prescribed Gizaar® with caution. There is no experience with the use of losartan in patients with severely impaired liver function (more than 9 points on the Child-Pugh scale), therefore the drug Gizaar® should not be used in this group of patients (see Contraindications).
Renal dysfunction
Due to inhibition of the RAAS, changes in renal function, including the development of renal failure, have been observed in some susceptible patients. These changes in renal function may return to normal after treatment is stopped.
Some drugs that affect the RAAS may increase blood urea and serum creatinine concentrations in patients with bilateral renal artery stenosis or renal artery stenosis of a solitary kidney. Similar effects have been reported with losartan. Such renal dysfunction may be reversible after discontinuation of therapy. Losartan should be used with caution in patients with bilateral renal artery stenosis or renal artery stenosis of a solitary kidney.
Increased serum potassium concentration
The simultaneous use of other drugs that can increase the potassium content in the blood serum can lead to the development of hyperkalemia (see Interaction with other drugs).
Losartan-hydrochlorothiazide
Hypersensitivity reactions
In patients with a history of angioedema (swelling of the face, lips, pharynx/larynx and/or tongue), monitoring of the use of the drug is necessary (see Side effects).
Renal and liver dysfunction
The drug Gizaar® is contraindicated for use in patients with severely impaired liver function and severely impaired renal function (creatinine clearance not more than 30 ml/min) (see Contraindications).
Embryotoxicity
The use of drugs that affect the RAAS during the second and third trimester of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and mortality. The development of oligohydramnios may be associated with fetal lung hypoplasia and skeletal deformities. Possible adverse events in neonates include calvarial hypoplasia, anuria, hypotension, renal failure and death. If pregnancy is diagnosed, Gizaar® should be discontinued immediately (see Use during pregnancy and breastfeeding).
Interactions of the drug Gizaar forte
Losartan Pharmacokinetic studies did not reveal clinically significant interactions of the drug with hydrochlorothiazide, digoxin, warfarin, cimetidine, phenobarbital, ketoconazole and erythromycin. There is evidence of a decrease in the level of the active metabolite in the blood plasma when using rifampicin and fluconazole. The clinical effects of these interactions have not been studied. The combined use of losartan, as well as other drugs that block angiotensin II or its effects, with potassium-sparing diuretics (for example, spirinolactone, triamterene, amiloride), potassium supplements or potassium salts may lead to an increase in serum potassium levels. NSAIDs, including selective COX-2 inhibitors, may reduce the effect of diuretics and other antihypertensive drugs. Therefore, the hypotensive effect of angiotensin II receptor antagonists may be attenuated by NSAIDs, including COX-2 inhibitors. In some patients with impaired renal function during treatment with NSAIDs (including COX-2 inhibitors), treatment with angiotensin II receptor antagonists may lead to a further decrease in renal function. These effects are usually reversible. Hydrochlorothiazide When used in combination with thiazide diuretics: Ethanol, barbiturates and narcotics may potentiate the risk of orthostatic hypotension. Hypoglycemic agents (oral and injectable (insulin)) - dosage adjustment of hypoglycemic agents may be required. With other antihypertensive drugs there is an additive effect. Cholestyramine and colestipol - in the presence of anion exchange resins, the absorption of hydrochlorothiazide is impaired. Single doses of cholestyramine and colestipol bind hydrochlorothiazide and reduce its absorption in the gastrointestinal tract by 85 and 43%, respectively. Corticosteroids, ACTH - a significant decrease in the level of electrolytes in the blood plasma, in particular hypokalemia. Pressor amines (for example, adrenaline ) - it is possible to reduce the severity of the response when using pressor amines, which does not require their withdrawal. Muscle relaxants of a non-depolarizing type of action (for example tubocurarine ) - the effect of the muscle relaxant may be enhanced. Lithium - Diuretics reduce the renal clearance of lithium and increase the risk of its toxic effects. It is not recommended to use this combination with drugs that contain lithium. Prescription of lithium drugs must be carried out according to the instructions. NSAIDs (including COX-2 inhibitors) - in some patients, the concomitant use of NSAIDs, including selective COX-2 inhibitors, may reduce the diuretic, natriuretic and hypotensive effects of diuretics. Effect of the drug on laboratory test results Given the effect of thiazides on calcium metabolism, their use may distort the results of studies of parathyroid function.
Overdose of the drug Gizaar forte, symptoms and treatment
Losartan The most likely symptoms of overdose are hypotension and tachycardia; bradycardia may result from parasympathetic (vagal) stimulation. In case of symptomatic arterial hypotension, maintenance therapy is indicated. Losartan and its active metabolite are not eliminated by hemodialysis. Hydrochlorothiazide The most common symptoms of overdose are electrolyte deficiency (hypokalemia, hypochloremia, hyponatremia) and dehydration due to increased diuresis. When taking cardiac glycosides simultaneously, hypokalemia may cause increased arrhythmia. Hydrochlorothiazide is eliminated by hemodialysis, although the extent of elimination has not been established. There is no data on specific treatment for overdose of Gizaar Forte. Treatment is symptomatic and supportive. Therapy with Gizaar Forte should be discontinued and the patient should be monitored. Possible therapeutic measures include inducing vomiting in the case of recent use of the drug, as well as correction of dehydration, electrolyte disturbances, hepatic coma and hypotension using symptomatic therapy.