Alcoholism is an important medical and social problem, the relevance of which is due to both the high prevalence of this disease and its negative social consequences [1]. Therefore, the development of new effective methods of its treatment is an important and urgent task of modern narcology.
In the last 20 years, a lot of experimental and clinical data have appeared indicating the role of the GABAergic system in the formation of alcohol dependence. Alcohol abuse, by reducing the activity of GABAergic neuromediation in the ventral region of the brain, enhances dopamine neurotransmission, which mediates the implementation of the reinforcing effects of alcohol (“reward system”) and plays an important role in the formation of alcohol dependence [2–4]. It is believed that with the development of alcohol dependence, there is a functional insufficiency of the inhibitory GABAergic system of the brain with simultaneous hyperactivity of monoaminergic systems (primarily dopaminergic). Considering the close functional relationship of all neurochemical processes in the brain, normalization of the state of the dopamine system can be achieved both through direct influence on various links and regulators of dopamine neurotransmission, and through other neurotransmitters and neuromodulators, including the GABA system [5-7].
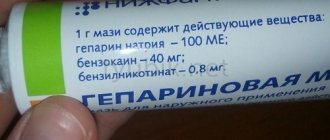
According to its chemical structure, baclofen is a derivative of chlorophenylbutyric acid (parachlorophenyl-GABA) and can be considered as a derivative of gamma-aminobutyric acid, as well as its stereospecific agonist. The main mechanism of action of baclofen is associated with the activation of presynaptic GABA-B receptors [8, 9].
An experiment on animals established the effect of reducing dopamine secretion, as well as reducing addictive behavior in response to the use of GABA-B receptor agonists (baclofen), while there was no effect of these drugs on feeding and water behavior, as well as on locomotor activity [10-14 ].
The first clinical study of the therapeutic effect of baclofen in persons suffering from alcohol dependence in combination with affective disorders was conducted in 1993 (cited from [15]). The study included 90 patients with secondary affective disorders (anxiety, depression), who were divided into four groups. Group 1 received baclofen, group 2 received diazepam, group 3 received amitriptyline, and group 4 received placebo. The effectiveness of therapy for affective disorders was assessed using clinical methods, psychological tests and electrophysiological (ultra-slow omega potential) techniques. The results of the study demonstrated the effectiveness of baclofen in correcting depression and anxiety in patients with alcohol dependence, comparable to the effectiveness of diazepam and amitriptyline. The advantage of baclofen was that it caused relatively few side effects.
A study of the safety of taking baclofen in combination with alcohol consumption was conducted by S. Evans and A. Bisaga [16] on 18 previously untreated volunteers who drank alcohol in high doses (an average of 28 standard drinks per week), but however, they did not meet the criteria for alcohol dependence. A test series of 6 two-day experiments in a hospital setting was performed in a double-blind, placebo-controlled, double-masked design. Baclofen (0, 40, and 80 mg) or an identical-looking placebo was administered 2.5 hours before alcohol consumption. The individual dose of alcohol for each subject was calculated based on weight (0.75 g/kg) and was divided into 4 doses with an interval of 20 minutes. In this study, there were no serious side effects of combining baclofen with alcohol and, in addition, there was no increase in either stimulant or sedative effects when baclofen was given in combination with alcohol, which allowed the researchers to conclude that the use of baclofen in combination with alcohol was safe.
The results of studies of the effectiveness of baclofen for the treatment of alcohol dependence, carried out in a double-blind, placebo-controlled study design, were contradictory. The first randomized, double-blind, placebo-controlled study of the efficacy and safety of baclofen for stabilizing remission in patients with alcoholic cirrhosis was conducted by G. Addolorato et al. [17]. The choice of baclofen for the treatment of patients suffering from alcohol dependence, combined with impaired liver function, was due to the pharmacokinetic characteristics of the drug, which is not metabolized in the liver (up to 80% of the oral dose is excreted by the kidneys), which makes baclofen the drug of choice for this group of patients. The study screened 148 patients with alcohol dependence and alcoholic cirrhosis, of which 84 patients who met the inclusion criteria were randomized. The patients were distributed in a 1:1 ratio into two groups: the 1st group received baclofen (5 mg 3 times a day for the first 3 days, the remaining days up to 12 weeks - 10 mg 3 times a day), and the 2nd group received took an identical-looking placebo for 12 weeks. Kaplan-Meier survival analysis showed a significantly higher retention of patients in remission in the baclofen group. Cox regression analysis also revealed a significantly lower risk of relapse and relapse among patients taking baclofen. In group 1, a lower severity of craving for alcohol was also revealed on the obsessive-compulsive scale.
J. Garbutt et al. [18] a randomized, double-blind, placebo-controlled study of the effectiveness and safety of baclofen in alcoholism was also conducted in the United States. The study included 80 patients randomized into two groups: group 1, taking baclofen, and group 2, placebo. The duration of therapy was 12 weeks, the daily dose of baclofen was 30 mg. Pharmacotherapy was supplemented with low-intensity drug counseling. Effectiveness measures included the number of days of heavy drinking, anxiety levels, and cravings for alcohol. 76% of all subjects completed the study. In general, the researchers noted that the drug was well tolerated, and no serious side effects were noted. Baclofen, unlike placebo, significantly reduced anxiety. At the same time, there was no statistically significant difference in the main and control groups in the number of days of heavy drinking and the frequency of relapses into alcoholism.
Two recent prospective cohort studies [19, 20] have established the effectiveness of high doses of baclofen (up to 330 mg/day) in reducing alcohol consumption. In the first study [19], 80 out of 100 alcohol-dependent patients reduced their alcohol consumption from an initial high level to moderate or low after 3 months of taking high doses of baclofen. After 2 years of observation, 60% of patients remained in the moderate and low alcohol consumption group. Similar results were found in a second study [20], which showed that after taking high-dose baclofen for a year, 80% of 132 heavy drinkers reduced their drinking to low levels. Both studies were open-label and were not accompanied by placebo control, which requires caution in the results obtained.
Thus, given the ambiguity of the data obtained, as well as the good tolerability of baclofen and the absence of serious side effects when used in patients with alcoholism, a real double-blind, randomized, placebo-controlled study (with double masking) was undertaken, the purpose of which was to study the effectiveness of baclofen (baclosan ) with alcoholism.
History of the drug
Baclofen was originally created as a treatment for epileptic disease. The substance was first synthesized by the large Swiss company Ciba-Geigy in 1962 by the famous pharmaceutical chemist Heinrich Keberle. Despite the fact that the drug did not succeed in treating epilepsy, it had a positive effect on the condition of patients who previously had:
- Stroke.
- Muscle spasms.
- Traumatic brain injuries.
The synthesized drug was initially intended to be used only orally, but the intrathecal method made it possible to achieve more effective treatment, without the side effects that could occur with the usual swallowing of tablets. Currently, Baclofen is used to treat a number of diseases.
Conclusion
Baclofen is a drug that has recently become increasingly popular among young people. We have to deal with facts of its non-medical use more and more often. Its consumers, who seek specifically narcotic effects, are citizens who do not have the means to purchase more expensive prohibited substances.
The constant desire to regularly feel euphoria and cause hallucinations leads to the need to systematically increase the dose of the drug, which is dangerous due to severe poisoning and death of a person.
Using this product is deadly. Relatives should remember this and seek help at the first signs of addiction in a person close to them. In rehabilitation, they can count on a free consultation, drawing up an individual treatment program, and psychological support for the patient at all stages. For help to be effective, it is important to contact specialists as early as possible, before the drug has completely enslaved the mind.
Medical use
Depending on the purpose, the drug is used in several ways, namely:
Oral route:
- A state of increased muscle tone.
- For tumors.
- Cerebral palsy.
- Stroke.
- Meningitis.
- With alcohol withdrawal syndrome.
Intrathecal method (injection into the spinal cord):
- Pronounced static.
- Multiple sclerosis.
- Damage to the brain or spinal cord.
The intrathecal method can also be used if the patient is intolerant to certain components when taken orally.
Treatment
It is recommended to begin therapy with detox and comprehensive diagnostics, which will allow you to develop a treatment regimen and select the necessary medications and techniques.
Detoxification
The detoxification method is aimed at removing metabolites and harmful substances from the body. Due to complete cleansing, it is possible to free the patient from physical addiction, completely relieve withdrawal symptoms, or minimize the symptoms of withdrawal.
Physical consequences for the body can be stopped with the help of:
- diets;
- multivitamin complexes;
- gymnastics;
- special drinking regime.
As prescribed by a doctor, it is possible to use symptomatic therapy to ensure the restoration of internal organs and body systems.
Help from psychologists
[us_image image=”17981″ size=”full” align=”center”][us_separator size=”small”]
Baklosan causes psychological dependence. Therefore, you cannot do without consulting a psychologist. The duration of this course is from 8 to 10 weeks.
Working with a psychotherapist allows the patient to return healthy communication skills, reconsider personal priorities in life, take a sober look at their problems, realizing ways to solve them. Psychotherapeutic sessions are designed to give a person back the ability to independently solve his problems without resorting to drugs and alcohol.
Socialization
[us_image image=”3396″ size=”full” align=”center”][us_separator size=”small”]
An important and final stage of rehabilitation. After going through it, you will be able to answer positively whether it is possible to recover from Baklosan addiction. Long-term use of this drug gives a person self-confidence, he enjoys communication, and easily makes new acquaintances. At the socialization stage, psychologists actually teach a person to communicate again, without turning to drugs for help.
The result of this work is the normalization of the patient’s psychological state. He can be taught to control his desires and actions, and to adequately respond to environmental challenges.
Trying to cope with addiction to this drug on your own will lead nowhere. Abrupt withdrawal will only provoke severe withdrawal symptoms.
Signs of Baclofen Use
Due to its potent component, the drug is actively used by drug addicts, mostly of a young age. The fact is that in case of an overdose, Baclofen has a strong, intoxicating effect.
To get high, drug addicts take from 6 to 14 tablets at a time and wash it down with low-alcohol drinks. After 30–40, drug intoxication sets in, which is accompanied by the following symptoms:
- Nausea and vomiting.
- Severe dry mouth.
- The appearance of visual and auditory hallucinations.
- Severe hand trembling.
- Drowsiness.
- A state of complete apathy.
- Dilated pupils.
- Slurred speech.
- Dizziness.
- Impaired coordination of movements.
Amphetamine addicts also often use Baclofen. The drug can easily be diluted with a synthetic analogue of cocaine, thus turning one dose into two. Addicts who take this “mix” experience a strong feeling of euphoria, a surge of energy and auditory hallucinations.
Help your loved one get back on the right path! Leave your phone number and our specialists will contact you!
[edit] Links
- Instructions for medical use
- About treating alcoholism with baclofen
- Journey to Sklif by the co-author of “The Book of the Psychonaut”
- How to have a snack after it
- Legal drug baclofen
- Baclofen from a psychiatric point of view
- We had five tablets of 25 baclosan, 2 phenotropil, 5 picamilon, 4 phenibut, 1 capsule of 300 lyrica, 4 sodium caffeine benzoate, a bottle of taufon
- Baclofen and pregabalin on Encyclopedia Pathologica
- Narcogenic potential of Lyrica
| [ + ] Baclofen - a healing panacea for all diseases | |||||||||||||||
| |||||||||||||||
| [ + ] Baclofen has everything to do with substances | |||||||||||||||||||
| |||||||||||||||||||
Baclofen - development of addiction
This drug is often used by patients to enhance other drugs, so it is often combined with alcohol. The development of addiction is due to the fact that the drug opens up potentially hidden capabilities in a person. Fears, complexes, depression, nervousness - all this disappears.
The addict is filled with energy and wants to do something just as long as the effect of the next dose lasts. Chemical dependence is not typical for this drug; the main threat is the development of psychological attraction.
The mechanism of development of addiction can be represented as follows:
- Drug use.
- The effect of the substance on the body.
- Experience of euphoria.
- The end of the pleasure effect.
- Repeat dose to restore effect.
After developing persistent mental dependence, a person feels bad without taking the next dose.
[edit] Memeticity
Baklodram
| ◄ ► |
Baclofen for dummies
The same Nofap-kun
Until recently, baclofen remained a little-known substance in narrow circles of therapists and pharmacologists, but with the popularization of the psychonaut vale by forums like Bihai, a wide circle of students and schoolchildren learned about baclofen. The relatively low price of around 200-300 rubles made it affordable, and the set of positive effects made it also desirable. Despite the side effects and without reading the instructions, the indoor Siddy Barretts ate white wheels in bottles, after which they continued annealing in the appropriate institutions with orderlies. One of these pretzels described it in the “Book of a Psychonaut”, and another copied this chapter into the “ABC of Domestic Terrorism”, and the last comrade clearly did not stick to it, otherwise he would not have written it down among the substances safe for the carcass, but, in general, then, it is forbidden for phishists to take drugs on kagbe.
An important role in the popularization of baclofen among the new beatniks was played by the imageboards Ychan, Dobrochan and Dvach, where the official baclofen thread was posted in //, which later migrated to Sosach, and after it to Chukhach. At one time there was a neumphag on Ychan, who advocated nofap and regularly took baclofen. During one of the Anonymous gatherings, the character rolled 15 wheels in a couple of sittings and, with the words “I won’t even fall,” sprawled on the ground, babbling incoherent speeches, after which he safely drove off to the hospital.
Still, videos with baclofen gopniks are found on the pipe less often than with bottled carriers, but the hero of the article still has a long way to go in this regard, since psychotropic de facto and de iure bottle is becoming more and more difficult to stir up every year, and it is becoming more difficult to add buckle to the lists of Onishchenko and They haven't made up their minds yet.
Fatal consequences of use and assistance with an overdose of Baclofen
The use of Baclofen as a drug is characterized by greatly exceeding the dosage in order to achieve maximum pleasure and hallucinations. Often, in pursuit of such sensations, patients experience depression of the respiratory center and simply die.
People lose touch with the real world, their heart muscle activity and the vast majority of internal organs are disrupted. Also developing:
- Manic-depressive syndrome.
- Complete lack of connection with reality.
- Sociopathy.
According to experts, regular use of the drug in excessive doses over several weeks can lead to death.
If you overdose on Baclofen, you must act immediately. The optimal algorithm of actions will be as follows:
- Call an ambulance.
- Provide fresh air flow.
- Rinse the patient's stomach.
- Give plenty of fluids.
- If there is no pulse or breathing, perform resuscitation measures.
There are no specific antidotes for this substance, so relieving intoxication involves eliminating its most dangerous manifestations.
Baclofen is a cheap, youth drug that leads to fatal consequences literally from the first use. Such a drug is easy to obtain and this makes it one of the most dangerous, which is why if your loved ones are addicted to the drug without the necessary indications, seek drug treatment help.
results
Demographic and clinical data characterizing the patients are given in Table. 1. It shows that the selected groups of patients did not differ in basic indicators, such as age, gender, duration of alcohol dependence, etc. There were also no significant differences between the groups in other indicators.
Rates of medication regularity, measured respectively by missed capsules and urinary riboflavin, ranged from 65% to 100% in both groups and exceeded 80% at most visits. There were no differences between groups in these indicators.
As for the dropout of patients from the study program, in the main group 6 (37.5%) people completed the treatment program in remission, 8 (50%) patients relapsed into alcoholism, and another 2 (12.5%) patients dropped out of the study for other reasons not related to the underlying disease. In the 2nd, control group, the distribution of patients into the above three groups was similar. There were no differences between groups in treatment completion rates or relapse into alcoholism.
However, the results of the Kaplan-Meier survival analysis demonstrated a trend towards better retention in the treatment program in the group of patients receiving baclofen (Fig. 1), although the differences between the main group and the comparison group were not statistically significant (the significance of the differences was based on the Mantel log-rank test —Cox for the event “relapse” p
=0.651, and for the event “dropout for any reason”
p
=0.656).
Rice.
1. Results of the analysis of “dropout from the study” according to Kaplan-Meier. Significance of differences according to the Mantel-Cox log-rank test (p=0.656). The average duration of remission in the main group (8.6±0.9 weeks) did not differ significantly from that in the control group (7.4±1.0; p
=0.66).
The time to the first use of alcohol (“break of remission”) between the groups also did not differ much: 8.4 ± 1.0 weeks in the main group versus 6.2 ± 1.1 weeks in the control group ( p
= 0.23). It should, however, be noted that there was a tendency for a longer time to failure and relapse in the group of patients receiving baclofen.
The number of days of alcohol consumption, days of sobriety and alcohol consumption in grams of pure ethanol, verified by retrospective analysis, as well as indicators of GGT activity, which is a marker of massive alcoholization, are shown respectively in Table. 2 and 3.
Table 2. Dynamics of alcohol consumption indicators Note. Here and in other tables: for intergroup comparisons, statistical significance was determined based on the results of analysis of variance; for comparisons with respect to initial values, post hoc tests using the Bonferroni method were used; + — statistically significant differences in relation to the initial values of indicators within the group (p<0.05); *—differences between groups are close to statistically significant (p<0.1).
Table 3. Dynamics of GGT activity during treatment Note. + — statistically significant differences in relation to the initial values of indicators within the group (p<0.05); There are no statistically significant differences between the groups.
As can be seen from table. 2, all indicators of alcohol consumption decreased significantly during therapy relative to the initial data in both groups. Although there were no significant differences between the baclofen and placebo groups in terms of alcohol consumption (see Table 2), it should be noted that there was a trend towards lower alcohol consumption in the baclofen group, approaching the level of statistical significance in the 2nd week of the study (reliability of differences in the number of days of severe drunkenness in a week
=0.073, and in the number of grams of pure ethanol consumed per week -
p
=0.085). In addition, the grams of pure ethanol consumed per week in the baclofen group were significantly lower than baseline values throughout the study, while in the placebo group such differences were observed only in the last weeks of the study and, moreover, were observed throughout a significant portion of the study. increased alcohol consumption (Fig. 2).
Rice.
2. Average amount of ethanol consumed per week, g. + - significance of differences from the initial value in the baclofen group - p<0.05; * — significance of differences from the initial value in the placebo group — p<0.05. The dynamics of GGT parameters (a biochemical marker of massive alcoholization) in the baclofen and placebo groups did not differ significantly (Table 3). At the same time, the values of GGT activity indicators in both groups significantly decreased during treatment relative to the initial values (Table 3).
In the present study, we used three quantified scales for assessing craving for alcohol: Pennsylvania scale (PSVA), obsessive-compulsive scale (OCSHVA) and visual analogue scale (VASHVA). The dynamics of craving for alcohol (craving) in the baclofen and placebo groups are shown in Table. 4.
Table 4. Dynamics of craving for alcohol during treatment Note. There were no statistically significant differences between the groups on all scales; *—statistically significant differences relative to the initial values within the group (p<0.05).
During the treatment, the intensity of craving for alcohol according to OKSHVA significantly decreased in both groups relative to the initial level (Table 5), and the decrease was statistically significant more often in the baclofen group. According to PSHVA and VASVA, a decrease in the intensity of desire during treatment was noted in both groups of patients, but it was statistically significant only in the baclofen group. There were no statistically significant differences in the dynamics of craving for alcohol between the groups of patients receiving baclofen and placebo on any of the three scales used in this study (see Table 5).
Table 5. Dynamics of anxiety and depression indicators during treatment Note. There were no statistically significant differences between the groups on all scales; *—statistically significant differences relative to the initial values within the group (p<0.05).
The results of the study of the dynamics of anxiety and depression in patients of both groups are shown in table. 5.
During treatment, the intensity of anxiety and depression on all scales decreased significantly in both groups relative to the initial values (see Table 5), and, as in the case of craving for alcohol, the decrease was significant much more often in the baclofen group. There were no statistically significant differences in the dynamics of anxiety and depression between the groups of patients receiving baclofen and placebo on any of the scales used in this study.
Overall treatment efficacy rates were obtained from SCS. There were no statistically significant differences between the groups at the end of the treatment course (Table 6).
Table 6. Changes in SHOCV in the studied groups of patients Note. The differences between the groups are not statistically significant.
In the main group of patients receiving baclofen, side effects were observed in 1 (6.25%) patient, and in the control group (placebo) - in 3 (18.75%) patients (the differences are not statistically significant). The most common adverse event was drowsiness (2 patients).
Indicators of liver enzyme activity decreased relative to the initial values in both groups, while there were no significant differences between the groups (Table 7).
Table 7. Dynamics of ALT and AST levels during treatment Note. For between-group and baseline comparisons, statistical significance was determined by analysis of variance; there are no statistically significant differences between groups; *—statistically significant differences relative to the initial values (p<0.05).