Sirdalud tablets - composition and principle of action
The main substance of the product, sold under the name Sirdalud, is tizanidine in a volume of 2 mg or 4 mg. Auxiliary components are:
- stearic acid;
- MCC;
- lactose monohydrate;
- anhydrous colloidal silicon dioxide.
The drug is sold in 30 pieces per package. Each package contains 3 blisters, each containing 10 doses. One tablet can contain 2 mg or 4 mg of the active substance, which allows the doctor to prescribe an effective and safe therapeutic dose with an accuracy of 1 mg.
Tizanidine is a skeletal muscle relaxant. It mainly acts on the spinal cord, reducing the high tone of the muscular skeleton and releasing the clamped areas from spasm. An additional effect of the drug is an analgesic effect.
Tizanidine is actively absorbed in the gastrointestinal tract. After an hour, its maximum concentration in the blood is reached. The kidneys are involved in removing the substance from the body.
Sirdalud belongs to the centrally acting drugs of the muscle relaxant group.
Sirdalud®
When using the drug Sirdalud® with inhibitors of the CYP1A2 isoenzyme, an increase in the concentration of tizanidine in the blood plasma is possible. In turn, an increase in the concentration of tizanidine in the blood plasma can lead to symptoms of drug overdose, including prolongation of the QT(c) interval.
The simultaneous use of Sirdalud® with inducers of the CYP1A2 isoenzyme may lead to a decrease in the concentration of tizanidine in the blood plasma, which may lead to a decrease in the therapeutic effect of the drug.
Contraindicated combinations with tizanidine
The simultaneous use of tizanidine with fluvoxamine or ciprofloxacin, inhibitors of the CYP1A2 isoenzyme, is contraindicated.
When tizanidine was used with fluvoxamine or ciprofloxacin, a 33-fold and 10-fold increase in tizanidine AUC was observed, respectively. The result of simultaneous use may be significant and prolonged hypotension accompanied by drowsiness, dizziness, and a decrease in the speed of psychomotor reactions (in some cases, up to circulatory collapse and loss of consciousness).
Not recommended combinations with tizanidine
It is not recommended to use tizanidine simultaneously with other inhibitors of the CYP1A2 isoenzyme - antiarrhythmic drugs (amiodarone, mexiletine, propafenone), cimetidine, some fluoroquinolones (enoxacin, pefloxacin, norfloxacin), rofecoxib, oral contraceptives, ticlopidine.
Combinations with tizanidine
requiring caution Caution
must be exercised when using Sirdalud® simultaneously with drugs that prolong the QT interval (for example, cisapride, amitriptyline, azithromycin) .
Antihypertensive drugs
The simultaneous use of Sirdalud® with antihypertensive drugs, including diuretics, can sometimes cause a pronounced decrease in blood pressure (in some cases, up to circulatory collapse and loss of consciousness) and bradycardia.
When the drug Sirdalud® was abruptly discontinued after simultaneous use with antihypertensive drugs, the development of tachycardia and an increase in blood pressure was observed, which in some cases can lead to acute cerebrovascular accident.
Rifampicin
Simultaneous administration of tizanidine and rifampicin leads to a 50% decrease in the concentration of tizanidine in the blood plasma. As a result, the therapeutic effect of the drug may be reduced, which may be clinically significant for some patients. Long-term simultaneous use of rifampicin and tizanidine should be avoided; if impossible, careful selection of the dose of tizanidine (increase) is recommended.
Smoking tobacco
The systemic bioavailability of tizanidine in smoking patients (more than 10 cigarettes per day) is reduced by approximately 30%. Long-term drug therapy in patients in this category may require higher doses of tizanidine than the average therapeutic dose.
Alcohol
During drug therapy, you should avoid drinking alcohol, as it may increase the likelihood of adverse events (for example, decreased blood pressure and lethargy). Tizanidine may enhance the depressant effect of alcohol on the central nervous system.
Other medicines
Sedatives, hypnotics (benzodiazepine, baclofen) and other drugs such as antihistamines may also increase the sedative effect of tizanidine. Avoid taking the drug with other alpha2-adrenergic agonists (eg, clonidine) due to the potential for increased hypotensive effects.
Sirdalud: what is the drug prescribed for?
The reason for prescribing Sirdalud is various muscle spasms caused by diseases of the spine, including localization in the cervical lumbar region. In addition, pain after surgical reduction of intervertebral hernias is also relieved by taking Sirdalud.
If the cause of pain in the muscles is multiple sclerosis, or a congenital pathology in the form of diagnosed cerebral palsy, which causes spasticity of the muscular skeleton, Sirdalud is prescribed.
Medicine Sirdalud: instructions
For the treatment of spasticity of skeletal muscles caused by neurological pathology, 6 mg of the drug per day is prescribed. The dose is divided into three doses in equal quantities. Thus, the minimum single dose starts from 2 mg. If it is necessary to increase the therapeutic effect, the daily dose is increased gradually, adding 2 mg per day every week. Severe diseases of muscle tone are relieved with a dose of 12 to 24 mg per day. The number of receptions can be increased up to 4 times.
At the same time, you should not exceed the maximum allowable amount of 36 mg per day.
For older patients over 65 years of age, it is recommended to begin treatment with a minimum amount of Tizanidine. If 2 mg does not give the expected effect, a gradual increase in daily intake is allowed while monitoring the patient's condition. It is recommended to follow the same regimen when treating patients with impaired renal function. Eating may increase the period during which the maximum amount of Tizanidine is concentrated in the patient's blood. Therefore, take the medicine an hour after eating.
Sirdalud
Sirdalud (active ingredient - tizanidine) is a central muscle relaxant that acts directly on the spinal cord. The main point of application of his efforts are presynaptic alpha-2 receptors. By stimulating them, sirdalud prevents the release of amino acids that excite receptors for N-methyl-D-aspartate. As a result, at the level of interneurons (interneurons) of the spinal cord, polysynaptic transmission of nerve impulses is inhibited. Since this mechanism is responsible for excessive muscle tone, when it is suppressed, a decrease in muscle tone will be observed. In addition to the muscle relaxant effect, sirdalud also has a moderately pronounced central analgesic effect. The drug is effective both for acute spastic muscle pain and for chronic muscle spasm of spinal and cerebral origin. Sirdalud reduces spasticity and stops clonic convulsions, as a result of which the physiological barrier to passive movements is removed and the range of active movements increases. Therapeutic effectiveness and severity of unwanted side reactions depend on the content of the active substance in the blood. The drug is quickly and completely absorbed in the gastrointestinal tract. The maximum concentration of the active component in the blood plasma is achieved on average 1 hour after taking the drug. The bioavailability of sirdalud is relatively low - about 35%, which is due to the effect of the first passage through the liver. The pharmacokinetic characteristics of the drug when taken with food change slightly. The half-life of sirdalud averages 2-4 hours. Excretion of the drug from the body is carried out mainly by the kidneys.
Sirdalud is available in tablets. The drug has a narrow therapeutic range, which requires careful selection of the dose in order to protect the patient as much as possible. It was experimentally found that a starting dose of 2 mg 3 times a day can minimize the risk of side effects. In any case, the dose should be selected individually.
For spastic muscle pain, 2 or 4 mg are usually prescribed three times a day, with the possibility of taking an additional dose in especially severe cases (optimally before bedtime). For spasticity of striated muscles associated with neurological diseases, the starting dose of the drug should be no more than 6 mg per day. The dose should be increased gradually, at intervals of 3-7 days. In most cases, a pronounced therapeutic effect can be achieved at a dose of 12-24 mg per day. The maximum daily dose is 36 mg. There is little experience with the use of sirdalud in people over 65 years of age. In such patients, pharmacotherapy begins with the minimum effective doses, followed by a gradual increase in order to achieve an acceptable ratio of effectiveness and tolerability of therapy. When stopping taking the drug, to reduce the likelihood of developing withdrawal syndrome, manifested in this case by increased blood pressure and tachycardia, it is necessary to slowly reduce the dose until the drug is completely stopped. This is especially true for individuals who have taken sirdalud for an extended period of time. Arterial hypotension that develops while taking sirdalud may be the result of its interaction with antihypertensive drugs or CYP1A2 inhibitors. A number of sources provided information about liver dysfunction caused by tizanidine, but this did not apply to those cases where the drug was used in daily doses of less than 12 mg. In any case, it is recommended to monitor liver function indicators once a month, at least at the initial stage of treatment (and subsequently - only if appropriate clinical signs are present). A 30% decrease in the systemic bioavailability of sirdalud was found in men who smoke more than 10 cigarettes per day. During treatment, it is recommended to abstain from another human vice - drinking alcohol, because... otherwise, the risk of side effects increases.
Overdose of Sirdalud
If the patient was unjustifiably prescribed the maximum dose of the drug, or he independently increased the number of doses, the following adverse reactions caused by an overdose may be observed:
- vomit;
- drowsiness;
- loss of coordination;
- dizziness;
- decrease in systolic pressure;
- miosis;
- respiratory rhythm disturbances.
Significantly exceeding the maximum permissible daily dosage can put the patient into a coma.
Drug interactions
Simultaneous use with inhibitors is permissible only if treatment is carried out at low doses of Sirdalud. Once in the blood, CYP1A2 increases the amount of the main substance in human plasma, which can cause symptoms of overdose. In turn, CYP1A2 inducers, entering the blood with Sirdalud, on the contrary, reduce the amount of tizanidine in the body, which makes the expected therapeutic effect insignificant even at high doses of consumption.
Concomitant use with antibiotics leads to a sharp decrease in blood pressure, the development of dizziness and drowsiness, which can cause loss of consciousness.
Rifampin, entering the blood, displaces tizanidine, which means it reduces the therapeutic effect. Treatment with Sirdalud should not be combined with alcohol intake. The drug significantly enhances the effect of alcohols on the central nervous system, leading to a pronounced change in consciousness.
Sirdalud® MR (Sirdalud® MR)
With simultaneous use of the drug Sirdalud® MP with inhibitors of the CYP1A2 isoenzyme, an increase in the concentration of tizanidine in the blood plasma is possible. In turn, an increase in tizanidine plasma concentrations may lead to symptoms of drug overdose, including prolongation of the QT(c) interval.
The simultaneous use of Sirdalud®MR with inducers of the CYP1A2 isoenzyme may lead to a decrease in the concentration of tizanidine in the blood plasma, which may lead to a decrease in the therapeutic effect of the drug.
Contraindicated combinations with tizanidine
The simultaneous use of tizanidine with fluvoxamine or ciprofloxacin, inhibitors of the CYP1A2 isoenzyme, is contraindicated.
When tizanidine was used with fluvoxamine or ciprofloxacin, there was a 33-fold and 10-fold increase in tizanidine AUC, respectively. The result of simultaneous use may be clinically significant and prolonged arterial hypotension, accompanied by drowsiness, dizziness, and a decrease in the speed of psychomotor reactions (in some cases, up to collapse and loss of consciousness).
Combinations not recommended with tizanidine
It is not recommended to use tizanidine simultaneously with other inhibitors of the CYP1A2 isoenzyme - antiarrhythmic drugs (amiodarone, mexiletine, propafenone), cimetidine, some fluoroquinolones (enoxacin, pefloxacin, norfloxacin), rofecoxib, oral contraceptives, ticlopidine.
Combinations with tizanidine requiring caution
Caution must be exercised when using Sirdalud® MR simultaneously with drugs that prolong the QT interval (for example, cisapride, amitriptyline, azithromycin).
Antihypertensive drugs
The simultaneous use of Sirdalud® MR with antihypertensive drugs, including diuretics, can sometimes cause a decrease in blood pressure (in some cases, up to vascular collapse and loss of consciousness) and bradycardia.
When the drug Sirdalud® MR was abruptly discontinued after use together with antihypertensive drugs, the development of tachycardia and an increase in blood pressure was observed, which can in some cases lead to acute cerebrovascular accident.
Rifampicin
Simultaneous administration of tizanidine and rifampicin leads to a 50% decrease in the concentration of tizanidine in the blood plasma. As a result, the therapeutic effect of Sirdalud® MR may be reduced, which may be clinically significant for some patients. Long-term simultaneous use of rifampicin and tizanidine should be avoided; if this is not possible, careful selection of the dose of tizanidine (increasing) is recommended.
Smoking tobacco
The systemic bioavailability of tizanidine in smoking patients (more than 10 cigarettes per day) is reduced by approximately 30%. Long-term therapy with the drug in patients in this category may require higher doses of tizanidine than the average therapeutic ones.
Alcohol
During drug therapy, you should avoid drinking alcohol, as it may increase the likelihood of adverse events (for example, decreased blood pressure and lethargy). Tizanidine may enhance the depressant effect of alcohol on the central nervous system.
Other medicines
Sedatives, hypnotics (benzodiazepine, baclofen) and other drugs, such as H1-histamine receptor blockers, may also enhance the sedative effect of tizanidine.
Avoid taking Sirdalud® MR with other alpha2-agonists (for example, clonidine) due to the potential for increased hypotensive effects.
special instructions
Due to the fact that taking Sirdalud is often accompanied by drowsiness and decreased concentration, it is not prescribed to people whose daily activities involve driving vehicles or operating complex equipment.
Also, the drug is contraindicated for people with lactose intolerance, which is explained by the presence of lactose monohydrate.
The drug is sold strictly according to prescription. The validity period after which the drug must be disposed of is three years from the date of manufacture.
Sirdalud in the treatment of chronic headache
About the article
8894
0
Regular issues of "RMZh" No. 22 dated November 19, 2004 p. 1250
Category: Neurology
Author: Kalashnikova L.A.
For quotation:
Kalashnikova L.A. Sirdalud in the treatment of chronic headache. RMJ. 2004;22:1250.
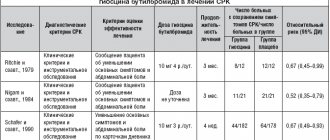
Sirdalud (Tizanidine hydrochloride) – an agonist? 2- (presynaptic) adrenergic receptors, blocking the release of excitatory neurotransmitters, primarily norepinephrine and aspartate in the spinal cord and brain (at the level of the blue spot - locus ceruleus). Thanks to this, Sirdalud has a muscle relaxant effect and, in addition, has an antinociceptive effect that is not associated with the effect on the central opioid system [2,4]. The drug is available in tablets of 2 and 4 mg and is used mainly to eliminate painful muscle spasms and reduce muscle spasticity observed in various neurological diseases. The central mechanism of action of the drug is associated with the effect on the structures of the brain stem (locus ceruleus), the presence of antinociceptive and muscle relaxant effects is a theoretical justification for the use of Sirdalud in the treatment of certain types of primary headaches, in the genesis of which central dysregulation of the tone of the cranial and cerebral arteries is important, tone of the pericranial muscles, as well as a decrease in the threshold of pain perception. According to the international classification of headaches (1988) and its revised version (2004), a distinction is made between primary headaches, which are independent nosologies, and secondary headaches, which are manifestations of various neurological and systemic diseases [7,8]. The two most common types of primary headaches are migraine and tension headache. The characteristic features of migraine are a moderate or severe headache, lasting from 4 to 72 hours, usually one-sided and pulsating, aggravated by movement, accompanied by nausea and/or vomiting, phono- and photophobia. Unlike migraines, tension headaches are of mild or moderate intensity, pressing or squeezing in nature, usually bilateral in localization, are not aggravated by physical activity, and are not accompanied by vomiting or severe nausea, although they may be combined with mild nausea or photo- or phonophobia. There are two subtypes of tension headache: those associated with tension in the pericranial muscles, which is recorded by palpation or electromyography; without tension of the pericranial muscles [7]. Both migraines and tension headaches can be episodic or chronic. At the same time, the chronic variant of migraine was first identified as its independent subtype only in the revised version of the international classification of headaches (2004) [8]. The most relevant is drug correction of the chronic version of migraine and tension headache. Pain is considered chronic if it bothers the patient more than 15 days a month for at least 3 months. Both types of primary chronic headache can be complicated by headache caused by excessive use of analgesics and other drugs [3]. The latter represent an independent type of cephalalgia. The relevance of the treatment of primary headaches is determined by their prevalence, the most frequent development in young and middle age, which is associated with considerable economic losses due to temporary disability. According to epidemiological studies conducted in the USA, the frequency of migraine in the population is 13% [9]. The prevalence of episodic tension-type headache reaches 38%, and chronic headache – 2% (and the latter significantly reduces the ability of patients to work) [14]. The relevance of the treatment of primary headaches is also due to the difficulties of drug correction that often arise, especially in chronic cases. In this regard, the search and use of non-traditional but pathogenetically based drugs is of great importance, one of which is Sirdalud, which affects the central brainstem regulatory mechanisms and the antinociceptive system, which are involved in the genesis of primary headaches. Special studies assessing the effectiveness of Sirdalud in the treatment of primary headaches are few. E.G. Filatova et al (1997) used Sirdalud in 32 patients with chronic tension-type headache at a daily dose of 4 and 6 mg [1]. The course of treatment was 14 days. In 75% of cases, a decrease in headache was noted, and in all cases its presence was combined with tension in the pericranial muscles. Along with this, the patients also experienced a decrease in anxiety and depression, which indicated the psychotropic effect of the drug. In addition, there was a normalization of night sleep and a decrease in autonomic disorders. When studying the nociceptive flexor reflex, the authors found an increase in its threshold, as well as in the pain threshold, which indicated an increase in the activity of the antinociceptive system. In the absence of tension in the pericranial muscles or with a high level of anxiety, there was no effect from the use of Sirlalud. Side effects included drowsiness and mild dizziness. The authors concluded that, along with antidepressants, Sirdalud plays an important role in the treatment of chronic tension-type headaches associated with pericranial muscle tension. Clinical trials conducted abroad have also shown the effectiveness of Sirdalud in the treatment of chronic headaches [5,6,11,12,13,15,16]. A double-blind placebo-controlled study conducted by R. Fogelhom et al., K. Murros (1992) [5] showed that treatment with Sirdalud at a dose of 6-18 mg per day for 6 weeks significantly reduced the intensity of chronic tension-type headache. Smaller doses of Sirdalud (3 mg per day, divided into 3 doses), according to Japanese researchers, also provide a good effect: a significant reduction in the intensity, frequency and duration of chronic tension headaches during a 4-week course of treatment was noted in 2/3 of patients [ 15,16]. It should be noted that the use of small doses of the drug is especially important in patients prone to hypotension, because Sirdalud may slightly reduce blood pressure. The reduction in chronic tension headaches noted by M. Sakuta and K. Takeda (1991) [11] in 90% of patients was accompanied by positive changes in electromyographic parameters recorded in the pericranial muscles. A preliminary study of 39 patients with chronic headaches (mainly migraine type) demonstrated the feasibility of using Sirdalud [12]. Thus, a decrease in the intensity, frequency and daily duration of headaches in the first 4 weeks of treatment was noted in 49% of patients, in 5–8 and 9–12 weeks – in 64% and 65% of patients, respectively. Moreover, at 9–12 weeks of treatment, the condition of 67% of patients improved by half compared to the baseline. The dose of the drug was increased gradually over 4 weeks and varied from 4 to 20 mg per day, averaging 13.5 mg/day. (divided into 3 doses). Side effects noted in more than 10% of patients were mild or moderate and included drowsiness, weakness, dry mouth, and rarely constipation and hyperkinesis. An increase in liver enzymes while taking Sirdalud was observed in only 1 out of 39 patients, and after cessation of treatment the indicators completely returned to normal. Preliminary data on the effectiveness, good tolerability and safety of Sirdalud were confirmed in a blinded, placebo-controlled trial that included 292 patients with primary headaches (migraine - 77%, chronic migraine headache or chronic tension-type headache - 23%) [13]. It was shown that a decrease in the frequency, duration and intensity of headaches in the first 4 weeks of treatment with Sirdalud (three times a day with a gradual increase in dose to an average daily dose of 18 mg) was observed in more than half of the cases, which was statistically significantly different from the placebo effect. Moreover, the drug was equally effective in treating all three types of primary headaches. Adverse effects were reported in more than 10% of patients and included drowsiness (47%), dizziness (24%), dry mouth (23%), asthenia (19%). The high effectiveness of the drug for various types of headaches, according to the authors, indicates the participation of? 2 adrenergic receptors in their pathophysiology, that is, consistent with the role of central mechanisms in their genesis. The possibility of using Sirdalud in combination with non-steroidal anti-inflammatory drugs in the treatment of headaches arising from excessive use of analgesics and other drugs to relieve migraine attacks (drug-dependent headache) deserves attention. As a rule, when analgesics are discontinued in these cases, the headache intensifies (rebound phenomenon). According to TR Smith (2002) [17], in these cases, the administration of Sirdalud in combination with non-steroidal anti-inflammatory drugs is effective. After 6 weeks of treatment, the effect was noted in 65% of patients, after 12 – in 69%. In contrast to the positive assessment of Sirdalud in the treatment of headaches, K. Murros et al. (2000) obtained different data [10]. Considering the effectiveness of Sirdalud in the treatment of chronic tension headaches, in a randomized, double-blind, placebo-controlled study, the authors unexpectedly obtained a pronounced placebo effect. Thus, the effectiveness of 6 mg or 12 mg of Sirdalud, taken once in the evening by 165 patients for 6 weeks, did not differ from that in patients taking placebo. The data obtained, according to the authors, confirm the significant role of psychophysiological mechanisms in the development of chronic tension-type headache. Thus, the summation of the few studies shows the effectiveness of Sirdalud in most cases of chronic headaches, primarily tension headaches involving the pericranial muscles, as well as chronic migraine. The inconsistency of the data obtained by K. Murros et al. with the rest available in the literature is apparently associated with the peculiarities of the dosage of the drug, and therefore further research is advisable.
Literature 1. Filatova E.G., Solovyova A.D., Danilov A.B Treatment of tension headaches with sirdalud. Journal of Neurology and Psychiatry named after. S.S. Korsakova 1997; No. 7; 36–38. 2. Chen D–F, Bianchetti V., Weissendanger M. Involvement of noradrenergic systems in the modulation of cutaneous reflexes. Motor disturbances I. Ed. R Benecke ea London 1987:187–195. 3. Colas R., Munoz P., Temprano R., ea Chronic daily headache with analgesic overuse: epidemiology and impact on quality of life. Neurology 2004; 62:1338–42. 4. Davis J., Johanston S.E. InhibitionbyDS103–282 of D– (3–H)–aspartate release from spinal cord slices. Br J Pharmacol 1983;78:28–30. 5. Fogelholm R., Murros K. Tizanidine in chronic tension-type headache: a placebo controlled double-blind crosses-over study. Headache 1992; 32:509–513. 6. Freitag FG Preventative treatment for migraine and tension–type headaches: do drugs having effects on muscle spasm and tone have a role? CNS Drugs. 2003; 17(6): 373–81. 7. Headache Classification Committee of the International Headache Society. Classification and Diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia 1988; 8 (suppl 7): 1–96. 8. Headache Classification Committee of the International Headache Society. The international classification of headache disorders. Cephalalgia 2004; 24:1–160. 9. Lipton RB, Stewart WF, Diamond S. et al. Prevalence and burden of migraine in the United States: results from the American Migraine Study II. Headache 2001; 41: 646–657. 10. Murros K, Kataja M, Hedman C, Havanka H, et al. Modified–release formulation of tizanidine in chronic tension–type headache. Headache. 2000; 40(8): 633–7. 11. Sakuta M., Takeda K. Beneficial effect of tizanidine on the ischemic muscle contraction in chronic muscle contraction headache. Cephalalgia 1991; 11(suppl.11):339–340. 12. Saper JR, Lake AE 3rd, Cantrell DT, Winner PK, White JR. Chronic daily headache prophylaxis with tizanidine: a double-blind, placebo-controlled, multicenter outcome study. Headache. 2002; 42(6): 470–82. 13. Saper JR, Winner PK, Lake AE 3rd. An open–label dose–titration study of the efficacy and tolerability of tizanidine hydrochloride tablets in the prophylaxis of chronic daily headache. Headache. 2001; 41(4): 357–68. 14. Schwartz BS, Stewart WF, Simon D., Lipton RB Epidemiology of tension-type headache. JAMA 1998; 279:381–383. 15. Shimomura T., Awaki E., Takahashi K. Treatment of tension-type headache with tizanidine hydrochloride: relationship between plasma MHPG concentration and clinical effects. Cephalalgia 1991; 11 (suppl 11): 333–334. 16. Shimomura T., Awaki E., Kowa H., Takahashi K. Treatment of tension–type headache with tizanidine hydrochloride: its efficacy and relationship to the plasma MHPG concentration. Headache 1991; 31:601–604. 17. Smith TR Low–dose tizanidine with nonsteroidal anti–inflammatory drugs for detoxification from analgesic rebound headache. Headache. 2002 Mar;42(3):175–7.
Content is licensed under a Creative Commons Attribution 4.0 International License.
Share the article on social networks
Recommend the article to your colleagues