Hyperprolactinemia (persistent galactorrhea-amenorrhea syndrome, hyperprolactinemic hypogonadism) is not an independent disease, but a clinical and laboratory syndrome. The pathology was first described in 1855 by the German gynecologist D. Chiari. Prevalence varies from 10 to 30 people per 100,000 population. The condition is more common in women of reproductive age (ratio to men 2.5:1). Prolactinomas account for up to 60% of cases. About 30% of cases of female infertility are caused by hyperprolactinemia.
Causes of hyperprolactinemia
There are many reasons that cause an increase in prolactin levels. Even some physiological conditions, such as physical activity, emotional stress or sleep, can lead to a transient increase in the concentration of prolactin in the blood. Frequent physiological causes in women are pregnancy and lactation. The etiological factors of pathological hyperprolactinemia are:
- Prolactinoma and other pathologies of the pituitary gland.
A benign pituitary adenoma that excessively produces prolactin (prolactinoma) most often provokes hyperprolactinemia. Lymphocytic hypophysitis and surgical interventions in the pituitary region can also lead to an increase in hormone levels. - Diseases of the endocrine glands.
Another common cause of hyperprolactinemia is endocrine diseases such as acromegaly, primary hypothyroidism, and Cushing's disease. In women, this condition often occurs in conjunction with polycystic ovary syndrome (PCOS). - Taking medications.
Many drugs have an antidopamine effect, which leads to an increase in prolactin levels. This usually occurs when taking antipsychotics (haloperidol, risperidone), antidepressants (paroxetine, moclobemide), prokinetics (metoclopramide). In women, hyperprolactinemia often develops while taking oral contraceptives. - Systemic diseases.
Granulomatous or infiltrative processes localized in the pituitary gland can also cause an increase in prolactin levels. Such diseases include tuberculosis, sarcoidosis, and giant cell granuloma. - Other pathologies.
More rare causes are tumors in the area of the sella turcica, compressing the pituitary gland (craniopharyngioma, germinoma), empty sella syndrome, chronic renal failure (CRF).
Norm prolactin
The normal level of prolactin in the blood is no more than 15 ng/ml, it is secreted in impulses - on average there can be about fourteen emissions per day. It reaches its maximum levels in the morning (somewhere between 5 and 7 am), and after waking up it begins to decline - within a few hours it becomes minimal. These data may change due to various factors. For example, if a woman is breastfeeding, the level of prolactin in her body increases and becomes higher than the generally accepted norm. Among other things, the secretion of this hormone depends on the levels of others, such as estrogens, thyroid hormones, etc. Even the slightest changes in the production of these hormones leads to a sharp jump in prolactin levels. Psychoemotional and physical stress, uncontrolled or exceeding the required dosage of taking certain medications, surgery, previous injuries, and much more can also increase prolactin levels.
There are two types of designations for the content of prolactin in the blood: nanograms/liter - ng/l and international milli-units/liter - mIU/l. The first method is used most often - ng/l. Norms for prolactin levels:
- in adult women this figure should be - 64 - 395 mIU/l or 1* - 29 ng/l
- in men - 78 - 380 mIU/l or 1* - 18 ng/l
But in women, these readings can vary depending on the phase of the menstrual cycle: during the follicular phase they are 252 - 504 mIU/l, during the periovulatory phase - 361 - 619 mIU/l, and in the luteal phase - 299 - 612 mIU/l.
Pathogenesis
Excessive levels of prolactin in the blood through a negative feedback mechanism suppresses the secretion of GnRH in the hypothalamus, which leads to a decrease in the production of luteinizing and follicle-stimulating hormones. As a result, deficiency of sex hormones develops, hypoplasia of the external genitalia (hypogonadism), active proliferation of the secretory apparatus of the mammary gland, increased lactogenesis and lactation (galactorrhea), especially in women.
Long-lasting hyperprolactinemia stimulates bone resorption processes, which reduces its mineral density (osteoporosis). Leptin resistance, adiponectin deficiency and hypogonadism contribute to the deposition of fat in subcutaneous fat and an increase in the content of cholesterol fractions in the serum. There is moderate hyperproduction of androgens in the reticular zone of the adrenal cortex.
Diagnosis of hyperprolactinemia
The level of prolactin is determined by the results of a venous blood test.
In this case, it is extremely important to correctly collect biological material. Blood sampling is carried out in the morning, on an empty stomach, and the patient must remain awake for at least an hour. The day before, you must refrain from drinking alcohol, protein foods, visiting the sauna, baths, sexual contacts, intense physical activity, and refuse a gynecological examination or examination of the mammary glands. If the patient smokes, the cigarette should be smoked no later than 2 hours before blood sampling. In women, it is more advisable to carry out the analysis in the first phase of the menstrual cycle (3-7 days of the cycle).
To eliminate possible errors, it is important to strictly follow all of the recommendations listed before the study.
When hyperprolactinemia is confirmed (after 2-3 measurements on different days), the patient’s examination plan is expanded. Additionally it is necessary to carry out:
- Macroprolactin;
- TSH, free T4 (confirm or exclude hypothyroidism);
- LH, total testosterone in men;
- ACTH (to identify or exclude adrenal insufficiency in macroprolactinomas);
- IGF-1 to exclude somatotropinoma;
- C-peptide, insulin in the presence of obesity and metabolic syndrome to detect pre-diabetes mellitus;
- All women of childbearing age should undergo a pregnancy test because... this is the most common cause of hyperprolactinemia and secondary amenorrhea;
- MRI or CT scan of the pituitary gland;
- Consultation with an ophthalmologist, determination of visual fields for macroprolactinomas;
- Consultation with a neurosurgeon for macroprolactinomas and symptoms of tumor compression.
Classification
By nature, pathological and physiological hyperprolactinemia are distinguished. Separately, macroprolactinemia is distinguished, in which an increased level of a biologically inactive high-molecular fraction of the hormone (big-big prolactin) is observed in the blood. In the latter version of the condition, there are no clinical symptoms. According to the mechanism of occurrence, hyperprolactinemia is divided into:
- Primary.
Caused by damage to the hypothalamic-pituitary system (tumors, surgical interventions). - Secondary.
Develops as a result of granulomatous processes, diseases of the endocrine system, kidneys, liver, taking medications,
Based on size, the following types of prolactinoma are distinguished:
- Microprolactinomas.
The size of the tumor does not exceed 10 mm. Occurs in the vast majority of cases (up to 90%). - Macroprolactinomas.
The diameter of the formation is more than 10 mm. It accounts for 10% of all prolactinomas and is more often detected in men.
Prevention of hyperprolactinemia
There are no special measures to prevent hyperprolactinemia. This disease does not require special recovery and rehabilitation methods. There is also no special diet or nutrition regimen. The lifestyle of a woman with hyperprolactinemia usually should not change; the most important thing is that she should avoid excessive physical and psycho-emotional stress.
After a course of treatment for hyperprolactinemia, the main difficulty is selecting suitable contraceptive methods for the patient, since the majority of oral contraceptives increase prolactin levels, and this is in no case acceptable. Intrauterine devices can also increase prolactin levels because they irritate the endometrial layer in the uterus. Based on all this, doctors advise women to undergo sterilization (if children are not planned in the future) or prescribe special contraceptives that do not affect prolactin levels.
Symptoms of hyperprolactinemia
Manifestations in women
In women, in the clinical picture, menstrual cycle disorders such as oligo-, opso- or amenorrhea, and anovulation come to the fore. Symptoms such as anorgasmia, decreased libido, and frigidity are observed. If hyperprolactinemia develops before the onset of puberty, hypoplasia of the uterus, labia minora, and clitoris is noted. Due to relative hyperandrogenism, hirsutism, seborrhea and acne may occur.
The most characteristic and specific symptom of hyperprolactinemia, occurring in 50-70% of women, is considered to be galactorrhea (discharge of milk from the mammary glands outside the feeding period), which often becomes the first sign of the disease. Its intensity may vary - from the appearance of a few drops of colostrum only during palpation of the mammary gland to spontaneous stream discharge.
There may be shocking photos of medical operations hidden here that show blood and guts.
Are you over 18 years old?
Yes
No
Galactorrhea
Manifestations in men
In men, the main symptoms are decreased libido, erectile dysfunction up to impotence, and gynecomastia (enlarged mammary glands associated with hypertrophy of glandular tissue). Galactorrhea occurs in approximately 30-35% of patients. The occurrence of hyperprolactinemia before puberty leads to underdevelopment of the genitals and secondary sexual characteristics (absence or weak growth of mustache and beard, high-pitched voice).
General manifestations
If hyperprolactinemia is caused by prolactinoma, reproductive disorders are accompanied by symptoms associated with the presence of a brain mass. They are usually caused by macroprolactinomas and are therefore more common in men. The most common neurological sign is headache. When the tumor compresses the optic chiasm, ophthalmological disorders occur - loss of visual fields, scotomas, bitemporal hemianopsia.
Sometimes a symptom such as ophthalmoplegia (paralysis of the eye muscles) is observed. The growth of prolactinoma into the structures of the diencephalon can provoke neuropsychic disorders in the form of emotional lability, sleep disturbances, and irritability. Often there are complaints of a nonspecific nature - general weakness, increased fatigue, memory impairment.
In recent years, the interest of doctors of various specialties has been attracted by diseases and syndromes associated with impaired prolactin secretion (PRL). Prolactin, which changed ideas about the regulation of reproductive function, was isolated as an independent hormone from the pituitary gland in 1970. It was shown that excessive secretion of PRL, which previously had a modest role in the regulation of lactation, quite often causes disorders of menstrual and generative functions. Hyperprolactinemia accounts for up to 25-40% of all cases of female infertility. Hyperprolactinemia also occurs in 10% of women with amenorrhea, 20-30% with galactorrhea, and 70% in patients with both of these symptoms [17, 22].
Accumulated clinical and experimental data have shown that impaired PRL secretion and the associated symptom complex occurs both with primary damage to prolactin-secreting structures, and with other endocrine and non-endocrine diseases, as well as when taking certain pharmacological drugs. These data formed the basis of the modern concept of primary hyperprolactinemia as an independent nosological unit and its secondary forms observed in other diseases.
Causes of hyperprolactinemia
PRL is a protein hormone involved in the initiation of lactation in the postpartum period. Its synthesis is carried out by lactotrophs of the anterior pituitary gland and is under the inhibitory influence of dopamine produced by the hypothalamus [20].
Physiological reasons for increased PRL levels are pregnancy and lactation, sexual intercourse (in women), sleep, psychological stress, exercise, food intake, hypoglycemia, general anesthesia, dehydration and medical procedures. An increase in the level of estrogen, TSH, and growth hormone also has a stimulating effect on lactotrophs [4, 21].
In addition to physiological hyperprolactinemia, pathological hyperprolactinemia is also distinguished. The pathogenetic mechanisms of hyperprolactinemia are based on a violation of the dopamininhibitory effect on the synthesis and release of PRL. As a result of constant stimulation of PRL secretion, hyperplasia of pituitary lactotrophs first occurs, and then the formation of micro- and macroadenomas of the pituitary gland is possible. Tumors and inflammatory processes in the hypothalamus can disrupt the synthesis and/or release of dopamine from neurons of the tuberoinfundibular region into the portal system [4].
Prolactinomas (micro- and macroadenomas) are one of the most common causes of persistent hyperprolactinemia and occur in 40% of all cases of hormonally active pituitary tumors. More rare causes of pathological hyperprolactinemia in the absence of pregnancy are idiopathic hyperprolactinemia, hypothalamic-pituitary diseases (hormonally active and inactive pituitary tumors, “empty” sella syndrome, radiation and other traumatic effects), systemic diseases (including chronic renal failure, cirrhosis liver) and symptomatic hyperprolactinemia (drug-induced, alcoholic, psychogenic, due to damage to the peripheral endocrine glands), etc. (see table)
[21].
The presence of excess PRL production in patients leads to the development of hyperprolactinemic hypogonadism. Under the influence of hyperprolactinemia, the production of GnRH in the hypothalamus decreases, and therefore the synthesis and secretion of gonadotropins - LH and FSH - is suppressed, and the pulse activity of LH, characteristic of the normal functioning of the reproductive system, decreases. Hyperprolactinemia also blocks the effects of gonadotropins at the level of target organs (gonads), which leads to hypoestrogenemia, reduces the synthesis of progesterone, and stimulates the secretion of adrenal androgens. There is an increase in the level of dehydroepiandrosterone and dehydroepiandrosterone sulfate, which is also associated with the presence of receptors for PRL in the zona reticularis of the adrenal cortex and the commonality of the hypothalamic regulation of the synthesis and secretion of adrenocorticotropic hormone and PRL by the pituitary gland [22, 29].
On the other hand, secondary hyperprolactinemia can develop in diseases accompanied by excess levels of estrogens and androgens (polycystic ovary syndrome - PCOS, congenital dysfunction of the adrenal cortex, gonadal tumors). Thus, in PCOS, the presence of moderate hyperprolactinemia is due to a violation of dopaminergic control over the synthesis and release of both GnRH and PRL. In addition, chronic hyperestrogenemia in PCOS has a stimulating effect on PRL synthesis [8].
Symptoms of hyperprolactinemia
The clinical picture of hyperprolactinemia is characterized by menstrual irregularities, most often of the type of oligo- and opsomenorrhea, primary or secondary amenorrhea. With moderate hyperprolactinemia, the menstrual cycle can be regular, but may be accompanied by disturbances in the luteal phase of the cycle and infertility. In 1/5 of all cases of the disease, hyperprolactinemia and menstrual irregularities occur from the onset of menarche, which is manifested by oligomenorrhea or amenorrhea [15, 17].
Galactorrhea (lactorrhea) is a pathological process of secretion of colostrum from the mammary glands without connection with the feeding process - varies from single drops of colostrum to a stream of milk. This symptom is observed in women with hyperprolactinemia - in 30-80% of cases [29].
According to researchers [1], there is a statistically significant relationship between the level of PRL and the nature of the discharge. With severe hyperprolactinemia, milky discharge is more common.
According to the WHO classification (1993), there are three degrees of severity of galactorrhea:
— I degree — single drops with strong pressure;
- II degree - milk stream or copious drops with gentle pressure;
- III degree - spontaneous release of milk.
Infertility, both primary and secondary, is one of the main complaints of patients with hyperprolactinemia. Somewhat more often than in the general population, there are indications of miscarriages in early pregnancy [1].
Changes in the mammary glands with prolonged hyperprolactinemia and amenorrhea are characterized by the presence of their moderate hyperplasia, which is not typical for amenorrhea in estrogen deficiency conditions. This clinical sign may indicate hyperprolactinemia. Considering the presence of hypoestrogenemia in women with hyperprolactinemia, gynecological examination may reveal the characteristic condition of the vulva and vaginal mucosa, low cervical number and hypoplastic uterus, which clearly correlates with the duration of the disease and the level of PRL and estrogen [25].
Neurological symptoms in the presence of a prolactin-secreting tumor of the pituitary gland are more often observed with macroadenomas; they arise due to the effect of the tumor on the surrounding brain structures and are manifested by headache. Visual impairment in this case is possible if the optic chiasm is affected [18].
Hirsutism (in 25% of cases), as well as seborrhea and acne develop with hyperprolactinemia due to excess production of adrenal androgens. The degree of hair growth is determined using the Feriman scale. The level of hair growth is determined in 11 areas of the body and is assessed on a five-point scale (from 0 to 4 points). Hair growth is detected on the upper lip, chin, chest in the nipple area, upper and lower back, upper and lower abdomen, shoulders, forearms, thighs, legs, buttocks. Normally, the hirsute number is 1–7 points, borderline values are 8–12 points, pathology is more than 12 points [7, 13].
Excess weight is observed in patients with hyperprolactinemia in 60% of cases, obesity - in 20%. According to T.I. Romantsova et al. [1], overweight and obesity of the first degree occur in 1/3 of women with hyperprolactinemia, regardless of the form of the disease, while obesity of the second and third degrees is 2 times more likely to be observed with prolactinomas than with idiopathic hyperprolactinemia.
The reasons for weight gain with hyperprolactinemia are a decrease in dopaminergic influence, the occurrence of leptin resistance, a decrease in adiponectin levels and concomitant hypogonadism. Moreover, excess production of PRL is associated with the occurrence of metabolic disorders, the formation of insulin resistance and deterioration of lipid metabolism [6, 11].
With hyperprolactinemia caused by hypothyroidism, symptoms characteristic of hypothyroidism are observed: dry skin, hair loss, brittle nails, increased fatigue, changes in behavioral reactions (apathy, indifference, memory impairment). Sometimes the first manifestation of hypothyroidism is spontaneous galactorrhea, accompanied by various menstrual irregularities, for which patients consult a gynecologist [15].
An increase in PRL levels may be accompanied by a decrease in libido, neuropsychic reactions in the form of depression, irritability, emotional lability, resulting from a decrease in testosterone levels and hypoestrogenemia. The latter also leads to a decrease in bone density, which is not always restored when PRL levels are normalized. Hyperprolactinemia can also be asymptomatic [21].
Diagnosis and differential diagnosis of hyperprolactinemia
The diagnosis of hyperprolactinemia, according to the latest international recommendations [21], is based on the determination of elevated levels of PRL in the blood serum.
The PRL content in the blood serum of healthy women does not exceed 600 mIU/l (20 ng/ml). An increase in the PRL level to 2000 mU/l is caused mainly by “functional” reasons and is more often characteristic of hyperprolactinemia in the “empty” sella syndrome, hormonally inactive pituitary tumor, idiopathic hyperprolactinemia and symptomatic forms. A hormone level of more than 2000 mU/l is characteristic of hyperprolactinemia of tumor origin. Higher levels of PRL are characteristic of patients with pituitary macroadenomas. When PRL increases to 1000 mU/l, it is recommended to carry out repeated two or three studies to avoid errors in its determination [4].
In this case, even slight hyperprolactinemia does not contradict the presence of prolactinoma, especially microadenoma, but in this case it is necessary first of all to exclude pituitary tumors that are not involved in the secretion of PRL. In patients with asymptomatic hyperprolactinemia, it is necessary to study the level of macroprolactin [21].
Despite the fact that 85% of circulating PRL is represented by monomeric PRL with a molecular weight of 23 kDa, covalently bound dimers - “big” PRL and even larger molecules - “big-big” PRL, the predominance of which in serum is designated by the term macroprolactinemia [ 21].
According to some researchers [9], the incidence of galactorrhea and menstrual irregularities in patients with true hyperprolactinemia and macroprolactinemia does not differ significantly. Moreover, the presence of macroprolactinemia does not require specific treatment aimed at reducing PRL levels.
The generally accepted practice of studying serum PRL levels using polyethylene glycol will avoid overdiagnosis of the disease, including unnecessary imaging studies, as well as the initiation of unnecessary treatment of patients with hyperprolactinemia [16].
In the presence of macroprolactinomas, when determining the level of PRL in undiluted blood serum, in some cases there is a significant underestimation of the result at true excessively high concentrations of the hormone, which is associated with a change in the optical density of the solution, on the basis of which the concentration is determined by the photometric method (“hook-effect”). In this regard, when pituitary macroadenomas are detected, accompanied by a moderate increase in PRL levels and severe clinical symptoms that do not correspond to it, a repeat study of PRL levels with blood serum dilution is recommended [26].
X-ray craniography has been used for a long time as a visualization research method for diagnosing space-occupying formations of the pituitary gland, which is most informative only for identifying pituitary macroadenomas. Large adenomas cause an increase in size, expansion of the entrance to the sella turcica, and destruction of its back. Early radiological signs of a pituitary tumor are local or total osteoporosis of the walls of the sella turcica, unevenness of the internal contour of its bone wall with an unchanged structure of the bones of the cranial vault. Currently, the method of choice in the diagnosis of pituitary adenomas, especially microprolactinomas, is brain magnetic resonance imaging (MRI) [4].
When hyperprolactinemia is detected in women with amenorrhea, it is recommended to study the level of gonadotropins LH and FSH to exclude primary ovarian insufficiency. A study of the level of thyroid-stimulating hormone is also carried out to exclude primary hypothyroidism. Determining the level of other blood hormones does not play a decisive role in the diagnosis of hyperprolactinemia. However, if an “empty” sella turcica is detected by MRI, additional examination is necessary to identify a violation of the secretion of tropic hormones of the pituitary gland to exclude hypopituitarism. Examination of the fundus and visual fields is mandatory in the presence of macroprolactinoma, as well as in cases of symptoms indicating tumor spread to the chiasmal region. In women with hyperprolactinemia and hypogonadism, additional densitometry is necessary to assess bone density [4, 15].
Various functional tests have been described (including tests with thyrotropin-releasing hormone, metoclopramide, bromocriptine) for the differential diagnosis of functional hyperprolactinemia and pituitary prolactinoma, which have now lost their significance due to the advent of more advanced computer diagnostic methods [4].
Transvaginal echography of the pelvic organs helps in the differential diagnosis of PCOS. Hyperprolactinemia is characterized by multifollicular ovaries, which are characterized by normal size and volume with many follicles with a diameter of 4-8 mm, diffusely located in the stroma. Laparoscopy is performed for women with hyperprolactinemia and infertility with a regular ovulatory menstrual cycle, since in this group of women an increase in PRL levels is not the cause of infertility and occurs secondary to various gynecological pathologies. During laparoscopy, the most common pathology is external endometriosis, chronic salpingitis, and adhesions in the pelvis [12].
Treatment of hyperprolactinemia
Therapy is carried out taking into account the form of hyperprolactinemia. First of all, it is necessary to exclude primary hypothyroidism, the treatment of which is carried out with thyroid hormone preparations under the supervision of an endocrinologist, and, if possible, to exclude the use of certain groups of pharmacological drugs that contribute to an increase in the level of PRL. Therapy aimed at normalizing PRL levels is not prescribed in this case. In case of asymptomatic hyperprolactinemia in the presence of microadenoma, treatment is also not required. With functional hyperprolactinemia against the background of various gynecological diseases in women with infertility, treatment of the underlying disease should also be a priority [21].
Currently, dopamine agonist drugs are successfully used in the treatment of menstrual disorders and infertility associated with hyperprolactinemia. Restoration of the ovulatory menstrual cycle is observed in 70-80% of patients treated with bromocriptine and quinagolide, and in more than 90% of patients treated with cabergoline. When first starting dopaminergic therapy, women should be warned that restoration of ovulation and fertility may occur immediately (even before their first normal menstruation). In this regard, it is necessary to recommend that a woman use barrier contraception, since the use of oral contraceptives is not indicated in this category of patients [2].
However, it should be mentioned that, despite the existing hypothesis, the risk of progression of prolactinomas when using oral contraceptives has not been proven [15].
Currently, in clinical practice, in the treatment of hyperprolactinemia, preference is given to the dopamine agonist cabergoline. When taking cabergoline, there are fewer side effects and, as a result, better tolerability of the drug compared to bromocriptine. This is due to the greater selectivity of cabergoline in relation to D-2 dopamine receptors, a longer half-life of the drug and slight fluctuations in the concentration of the drug in the blood plasma of patients. Numerous studies [30] have also confirmed the greater effectiveness of cabergoline in comparison with bromocriptine drugs in terms of normalizing PRL levels, reducing tumor size, the degree of restoration of ovulatory cycles and pregnancy.
Thus, during a long-term (over 24 months) observation of 207 patients with hyperprolactinemia due to micro- and macrodenomas of the pituitary gland, as well as hyperprolactinemia of non-tumor origin, during treatment with cabergoline, better indicators were noted in normalizing the level of PRL and reducing tumor volumes as in macroprolactinomas (82.1 % versus 46.4%), and for microprolactinomas (90% versus 56.8%) in comparison with bromocriptine [24].
Another study of 459 women with hyperprolactinemic amenorrhea due to microprolactinomas and idiopathic hyperprolactinemia for 24 weeks of cabergoline also showed a greater trend toward normalization of PRL levels (83% vs. 59%) and restoration of ovulatory cycles and pregnancy (72% vs. 52%) than when taking bromocriptine. When the duration of cabergoline intake was increased to 40 weeks, restoration of ovulation and/or pregnancy was observed in 90% of patients [30].
Contraceptive measures during treatment with dopamine agonists must be observed even in women wishing to become pregnant. In this case, the use of mechanical contraception is recommended in the first 2-3 menstrual cycles after the start of therapy, which makes it possible to determine the intermenstrual interval, suspect pregnancy in time, and carry out its biochemical confirmation for further accurate calculation of the age of the fetus [2].
Therapy with cabergoline drugs (Dostinex, Agalates) should be started with 1/2 tablet (0.25 mg) 2 times a week under the control of PRL levels, adjusting the dose depending on its indicators until stable normoprolactinemia is achieved. The maximum dose of the drug is 1-2 mg per week, dose adjustment is carried out no more than once a month by 0.5 mg. Therapy with bromocriptine (parlodel, abergin, bromergon) begins with 1/3 tablet during the first 3 days with an evening meal, from the 4th day - 2/3 tablets, from the 7th day - 1 tablet (2. 5 mg) per day. A dose of the drug exceeding 2.5 mg is taken 2-3 times a day with meals. The dose of the drug is also adjusted according to the level of PRL in the blood; the dose is increased gradually - by 2.5 mg once a month. Average therapeutic doses are 2.5-15 mg, in rare cases - up to 30 mg per day. Further monitoring of PRL levels is carried out once every 6 months [1].
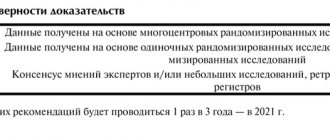
The optimal duration of therapy has not been precisely determined. However, drug treatment is carried out for at least 2-3 years, i.e. not only until the PRL level is normalized and reproductive function is restored, but also further in the process of dispensary observation. Subsequently, drugs can be discontinued under monitoring of PRL levels. With long-term normoprolactinemia and no signs of pituitary adenoma according to MRI data after 2 years of taking the drug, patients have a high chance of developing remission of the disease when treatment is stopped [15].
In case of pituitary macroadenomas and there is no effect from treatment with dopamine agonists, preference is given to neurosurgical intervention. For large tumor sizes, the use of dopamine agonists in the preoperative period is recommended, which makes the adenoma operable. Given the frequent relapses of the tumor, long-term administration of drugs from this group is recommended in the postoperative period. It is also possible to develop complications such as hypopituitarism and diabetes insipidus. Radiation therapy for prolactinomas is currently used extremely rarely [1].
International clinical practice guidelines for the diagnosis and treatment of hyperprolactinemia, once pregnancy is established, recommend discontinuation of dopamine agonists in women with prolactinomas. Some patients with macroadenomas who become pregnant while taking dopamine agonists and have not previously undergone surgery or radiotherapy for a pituitary adenoma may continue to take dopamine agonists during pregnancy, especially if the tumor tends to grow invasively or affects the optic chiasm. Since dopamine agonists cross the placenta, the drug in most cases must be discontinued in the first 4 weeks after conception. Dopamine agonist drugs do not have embryotoxicity, and their withdrawal is due to the fact that during pregnancy the increased level of PRL is physiological [3, 21].
The safety of the use of bromocriptine and cabergoline in women with idiopathic or hyperprolactinemia caused by pituitary adenomas during the first trimester of pregnancy has been proven and widely confirmed by many foreign studies [23, 27, 30].
Also, according to J. Raymond et al. [28], with long-term (from birth to 9 years) observation of children whose mothers took bromocriptine during pregnancy, no negative effect of the drug on their mental and physical development was established.
The use of other dopamine agonist drugs, in particular quinagolide, during pregnancy is not indicated due to the increase in cases of pregnancy complications and the occurrence of intrauterine malformations observed in a number of studies while taking the drug [5].
The absence of pregnancy upon restoration of ovulatory menstrual cycles during the use of dopamine agonists requires the exclusion of peritoneal factors of infertility during hysterosalpingography or laparoscopy [15].
An important issue is the management of women with hyperprolactinemia during menopause. The majority of cases of newly diagnosed pituitary adenomas in menopausal women are macroadenomas, which is associated with a longer duration of previously undetected disease [19].
Estrogens have a stimulating effect on lactotrophs, and therefore their use leads to an increase in the size of the pituitary adenoma. The decrease in estrogen concentration in the body due to menopause is accompanied by a decrease in PRL levels. At the same time, the presence of microprolactinoma in menopausal women is not an absolute contraindication for the prescription of hormone replacement therapy based on natural estrogens. According to studies [1, 10], it has been confirmed that hormone replacement therapy, carried out in conjunction with the use of dopamine agonists, does not have a negative effect on the level of PRL and the size of pituitary adenoma in menopausal women.
Women receiving treatment for hyperprolactinemia with the development of menopause have a significantly higher chance of normalization of PRL levels than before its onset. In this regard, menopause in women with pituitary microadenomas receiving dopamine agonists for hyperprolactinemia is an indication to reconsider the need to continue treatment with these drugs [14].
Thus, hyperprolactinemia has a great impact on the woman’s reproductive system, leading to significant disturbances. Specific diagnosis, treatment of hyperprolactinemia and further management of the patient should be carried out by a gynecologist, taking into account the characteristics specific to each period of a woman’s life.
Complications
The main and most common adverse consequence of hyperprolactinemia is primary infertility (up to 70%) associated with ovulatory dysfunction in women and oligo-or azoospermia in men. The stimulating effect of the hormone on the mammary glands provokes the development of mastopathy. Elevated lipid levels accelerate the process of atherosclerosis, which increases the risk of myocardial infarction.
More serious complications are caused by the growth of tumor formation. Long-term mechanical impact on the chiasm can cause atrophy of the optic nerves and lead to blindness. Due to compression of adjacent zones of the pituitary gland, other hormonal disorders occur - diabetes insipidus, panhypopituitarism. Rarely, when very large in size, prolactinoma compresses the brain stem or aqueduct and grows into the nasal cavity.
Prolactin has other functions:
- The hormone helps women overcome excessive stress during breastfeeding;
- Increases insulin synthesis in the pancreas, thereby participating in the absorption of nutrients;
- Regulates the immune system, allowing the fetus to develop in the uterine cavity without rejection reactions and inflammation;
- Provides achievement of orgasm.
During lactation, prolactin levels increase, and this is a normal condition. If the hormone exceeds normal levels in other periods not associated with childbirth, we are talking about the development of pathology. In this case, you need to consult a doctor, undergo an examination and begin timely therapy. The consequence of hyperprolactinemia in women is frigidity and infertility, in men - impotence and infertility. This is due to the active participation of prolactin in the functioning of the reproductive system. These are just some of the possible complications of this pathological condition.
At CELT you can consult an endocrinologist.
- Initial consultation – 3,500
- Repeated consultation – 2,300
Make an appointment
Diagnostics
Patients with hyperprolactinemia are managed by an endocrinologist or gynecologist. When collecting anamnestic data, they find out what medications the patient is taking in order to exclude the medicinal nature of the pathology. For women, information about menstruation is clarified (frequency of occurrence, abundance, duration). Then an additional examination is prescribed, including:
- Determination of prolactin level.
To avoid a false positive test result on the eve of blood donation, the patient must adhere to rules that will avoid a transient increase in prolactin levels. For women with an intact menstrual cycle, blood is taken no later than the 7th day of the cycle. To exclude the phenomenon of macroprolactinemia, the big-big fraction of the hormone is determined. - Other hormonal studies.
There is a decrease in sex hormones (LH, FSH, estrogens). To diagnose endocrine pathologies, the levels of TSH, ACTH, anti-Mullerian hormone, etc. are determined. - MRI of the brain.
For better visualization of prolactinoma, it is recommended to perform MRI in T1 and T2 weighted images using a contrast agent (gadolinium). If MRI is not possible (for example, in the presence of metal prostheses, a pacemaker), it is prescribed with high resolution. - Consultation with an ophthalmologist.
If a pituitary tumor is detected, an examination by an ophthalmologist is required. Assessing visual acuity, visual fields using computer perimetry, and determining the state of the optic nerve during ophthalmoscopy help identify indications for surgical removal of prolactinoma.
Based on clinical symptoms, the differential diagnosis is primarily made with hypogonadotropic hypogonadism - a violation of the synthesis of gonadosteroids due to pathology of the organs of the reproductive system (ovaries in women, testes in men). Particularly difficult is the differential diagnosis between non-tumor causes of high serum prolactin levels.
Our doctors
Mikhailova Elena Vladimirovna
Endocrinologist, diabetologist, candidate of medical sciences
Experience 46 years
Make an appointment
Slovesnova Tatyana Alekseevna
Endocrinologist, Candidate of Medical Sciences, doctor of the highest category
Experience 48 years
Make an appointment
Kolodko Inna Mikhailovna
Doctor - endocrinologist, doctor of the highest category
Experience 26 years
Make an appointment
Treatment of hyperprolactinemia
Conservative therapy
In most cases, the patient is treated on an outpatient basis. Hospitalization is necessary in exceptional situations - for further examination if the cause of the pathology is unclear or for preparation for surgery. If hyperprolactinemia is asymptomatic, therapy is not required. Conservative treatment includes the following areas:
- Treatment of prolactinoma.
The drugs of choice are dopamine receptor agonists (cabergoline, bromocriptine) - these drugs normalize prolactin concentrations, provide regression of clinical symptoms and can reduce tumor size. Cabergoline is more often used, which has a prolonged effect and higher selectivity for pituitary dopamine receptors (lower frequency of systemic side effects). - Treatment of the underlying disease.
With the development of secondary hyperprolactinemia, treatment of the underlying pathology is carried out to correct prolactin levels. L-thyroxine is prescribed for hypothyroidism, combinations of antibiotics for tuberculosis, glucocorticosteroids for sarcoidosis, etc. - Treatment of drug-induced hyperprolactinemia.
If an increase in prolactin concentration occurs when using a drug, it is replaced with another drug that does not have such a side effect. If it is impossible to discontinue the medication, sex hormone replacement therapy is performed to combat the symptoms of hypogonadism.
Surgery
Surgical removal of prolactinoma is indicated only in some cases. These include resistance to dopamine agonists or their individual intolerance, compression of the optic chiasm by a tumor, causing vision problems. Surgical treatment is also recommended for women with macroprolactinoma who are planning pregnancy. Transsphenoidal adenomectomy is considered the method of choice. The risk of relapse for macroprolactinomas is very high – up to 80%.
Hyperprolactinemia and pregnancy
Elevated prolactin leads to infertility. The question arises: can a woman become pregnant, safely give birth to a baby and feed him with breast milk? After all, prolactin regulates the functioning of the reproductive system. A woman can become pregnant only if the hormone is slightly higher than normal - no more than 27 ng/ml or 540 mU/l. In other cases, conception is impossible.
Hyperprolactinemia leads to the following pathological conditions:
- To disruption of the menstrual cycle or to the complete cessation of menstruation (amenorrhea);
- Anovulation is a cycle disorder in which the egg does not mature in the follicle and does not leave the ovary. Actually, this is the main obstacle to successful conception.
- Progesterone deficiency, as a result of which a woman cannot bear a child.
Do not forget that directly during gestation, prolactin increases, which is a natural physiological process. The increase in the amount of the hormone begins already from 5-7 weeks of pregnancy, then there is a significant increase in its level, which is also typical for the postpartum period. This is especially true in cases where the baby is fed with breast milk, because it is prolactin that significantly influences this process. Subsequently, in the absence of pathology, the numbers gradually normalize, and the hormone reaches a normal value for the body.
Prolactin is divided into several fractions:
- Small is the active fraction of prolactin that binds to receptors.
- The big one is several times less active than the small one.
- Big-big – even less active prolactin.
- Glycolyzed – this fraction is characterized by the absence of any activity; it does not bind to receptors.
Laboratories often determine the total amount of prolactin. It can be increased, but the woman still manages to get pregnant. How does this work? The fact is that hyperprolactinemia causes infertility only if the concentration of the active fraction of prolactin increases. Statistics show that in 30% of women, the pathology is caused by an increased level of inactive or low-active fractions, which means there is a chance of getting pregnant.
Therefore, it is necessary to conduct a detailed examination by qualified specialists, and then undergo treatment, the main purpose of which is to normalize the menstrual cycle and prolactin levels.
Prognosis and prevention
Hyperprolactinemia has a favorable prognosis. Cases of death are extremely rare and only when the pituitary tumor is malignant. The main problem is infertility and visual impairment (up to complete loss). When treating prolactinoma with dopamine agonists, it is necessary to determine serum prolactin levels once a month and conduct an MRI of the pituitary gland annually (for macroprolactinomas - every 6 months).
There is no primary prevention for prolactinomas. If a patient has diseases that can cause an increase in prolactin concentration (hypothyroidism, systemic granulomatous diseases), it is recommended to conduct a blood test for this hormone. The study is also performed when prescribing medications that have hyperprolactinemia in the list of adverse side effects.
Complications of hyperprolactinemia
Do not underestimate the severity and seriousness of the consequences for the human body that hyperprolactinemia can lead to if left untreated. This pathology can lead to the development of pituitary insufficiency, and this, in turn, causes disruption of the endocrine system - a person’s adrenal glands, thyroid gland, etc. begin to fail. Tumor growth quite often leads to deterioration of vision, and after a while - his complete loss. Patients with hyperprolactinemia often develop osteoporosis. And a pituitary tumor without timely treatment can develop from benign to malignant.
So, if you have any symptoms or signs of hyperprolactinemia, you should not postpone a visit to the doctor, otherwise the consequences of this disease can be very disastrous for you.
Radical methods of treating pituitary tumors
Due to the effectiveness of drug treatment for prolactinomas, surgery and radiation therapy are rarely used. Only a small proportion of patients with macroprolactinomas whose tumor size does not decrease with drug treatment may require surgery, especially if there is no improvement in vision. It should be noted that this operation is currently performed through a small incision near the sinuses, the so-called transsphenoidal approach. If a large prolactinoma steadily decreases in size as a result of taking pills, then this use continues in the future.
Sometimes experts recommend radiation therapy, which allows you to stop taking the medication. The effect of radiation develops gradually and is fully manifested only after a few years, so radiation therapy is not prescribed to young women who want to become pregnant (it is these women who predominate among patients with prolactinomas). For microprolactinomas, selective transsphenoidal adenomectomy is most often performed, but in 20-50% of patients, within 5 years after surgery, the tumor recurs and hyperprolactinemia resumes. With macroprolactinomas, even a short-term initial improvement after surgery occurs in only 10-30% of patients.
When carrying out radiation therapy or surgical treatment, pituitary insufficiency may develop, as a result of which secondary adrenal insufficiency and hypothyroidism develop and replacement therapy is required - glucocorticoids in the presence of adrenal insufficiency, L-thyroxine in the presence of thyroid insufficiency (hypothyroidism) and, possibly, sex hormones (estrogens for women and testosterone for men) as replacement therapy.
Doctor's opinion
Prognosis for prolactinoma depends on its size, clinical symptoms, as well as the timeliness of therapy initiated.
According to statistical data, when observing patients for five years after surgical treatment, relapse of the disease occurs in approximately 20-50% of cases. — Osina Ekaterina Aleksandrovna Reproductologist, obstetrician-gynecologist, Ph.D.
As for drug therapy, with its proper and long-term administration, regression and even complete disappearance of the adenoma is observed.
Treatment of prolactinoma
The main goals when drawing up a treatment plan for prolactinoma are to reduce the concentration of prolactin in the blood, influence the tumor by reducing it and preventing further growth, as well as corrective measures to combat infertility, hypogonadism, disorders of the visual organs and the skeletal system.
If a pituitary tumor is detected for the first time, there are signs of rapid growth, surgery is contemplated, or the disease is detected during pregnancy, patients should be hospitalized.
Conservative treatment of prolactinoma involves the use of dopamine agonists - cabergoline, bromocriptine, abergin, which affect the level of prolactin in the blood, allowing to restore menstrual function and influence the size of the tumor.
In cases where the use of medications does not bring the expected effect and the clinical signs of the disease progress, surgical treatment is resorted to, which involves removing the tumor transsphenoidally (through the nasal sinuses). If patients have contraindications to surgery due to the presence of severe concomitant pathology, or patients refuse surgery, radiation is used to treat prolactinoma.
After surgical or radiation exposure, patients take medication for a long time, sometimes even throughout their lives. Control images of magnetic resonance imaging are recommended to be carried out once a year, and prolactin levels in the blood are examined twice a year.
What is prolactinoma
Prolactinoma is a benign neoplasm that is localized in the anterior pituitary gland in the brain, which produces prolactin. This problem can arise much more often among the female population than among representatives of the stronger half of humanity. Quite rarely, such neoplasms undergo malignancy.
Prolactin normally stimulates lactation in women to establish and prolong breastfeeding, regulates the production of estrogen, and has an effect on the ovarian-menstrual cycle and ovulation. Normally, prolactin is also produced in small quantities in men. Together with luteinizing hormone (LH) and follicle-stimulating hormone (FSH), prolactin regulates the functioning of the reproductive system in the form of testosterone synthesis and influence on sperm activity.
- What causes pituitary adenoma (prolactinoma) in women?
An excessive amount of prolactin, which is observed when it is excessively synthesized by a neoplasm, causes inhibition of estrogenogenesis, that is, a decrease in estrogen synthesis. This provokes disturbances of the ovarian-menstrual cycle, which are characterized by anovulation (lack of ovulation). Also, estrogen deficiency leads to a lack of proliferative changes in the endometrium (endometrial hypoplasia), which also negatively affects the ability of a fertilized egg to implant into the uterine wall. This is fraught with infertility. - What causes pituitary prolactinoma in men?
Prolactinoma in men can cause erectile dysfunction, enlargement of the mammary glands (gynecomastia), and lack of sexual desire.
Diagnosis of prolactinoma
The most informative research method for identifying prolactinomas is magnetic resonance imaging of the pituitary gland
with a contrast agent, which allows you to determine the outlines of microadenomas, their location inside or outside the sella turcica.
When diagnosing macroadenomas, it is recommended to use computed tomography
of the sella region, in which the bone structures are clearly visible.
Laboratory research methods consist primarily of determining the level of prolactin in the blood, and the study is recommended to be carried out three times to exclude random fluctuations in the level of the hormone due to stress or other predisposing factors. Prolactinoma is characterized by a prolactin level in the blood exceeding 200 ng/ml.
Previously, to diagnose prolactinoma, stimulation tests with thyrotropin-releasing hormone were used, after the introduction of which into the body, in the first 20-30 minutes, the production of prolactin normally increased, doubling the initial level, and in patients with prolactinoma, the level of prolactin after stimulation did not change. Currently, this diagnostic method is not used due to its low reliability.
Causes of prolactinomas
Doctors have not yet fully studied the reasons for the appearance of prolactinomas. It is true that the development of prolactinomas can be facilitated by certain genetic disorders (for example, multiple endocrine neoplasia of the first type), as well as a hereditary tendency, some pathologies of the liver, kidneys and ovaries (for example, renal failure or cirrhosis of the liver). Sometimes the diagnosis of prolactinoma and the causes of its occurrence are associated with the use of certain medications (hormonal drugs, antidepressants, antihypertensive drugs). Some natural factors can also provoke an increase in prolactin levels - for example, childbirth, sexual intercourse, physical activity, and breastfeeding.
Prevention
The main direction of preventing the occurrence of pituitary adenomas is to minimize the impact on the body of provoking factors (brain injuries, neuroinfections). And prevention of relapses in the presence of a history of prolactinomas is constant monitoring and follow-up of such patients with MRI or CT scanning over time.
Our center’s specialists are always ready to find an approach to each patient and choose the most appropriate treatment tactics in each individual case, taking into account the nuances of the person’s health condition.