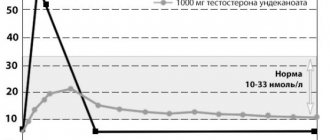
Updated: 04/23/2021 15:12:57
Expert: Abramova Tsilya
Yarina is a hormonal drug that is used as a contraceptive and in the treatment of certain hormone-dependent diseases. The product is available in two versions - Yarina and I Yarina Plus. They differ in one component in their composition. We analyzed the tools to find out in which situations it is preferable to use one or the other.
| Means | Advantages | Flaws |
| Yarina | + Popular COC based on drospirenone and ethinyl estradiol + Helps with acne and seborrhea + Convenient administration – once a day for 3 weeks with a break of 7 days + Normalizes the menstrual cycle + Reduces pain during menstruation | — Many contraindications — Greater risk of adverse symptoms |
| Yarina Plus | + Additionally contains folic acid + Used after abortion + Suitable for women who are planning pregnancy after discontinuation of the drug + Replenishes vitamin B9 deficiency + Taken without interruption, which helps prevent missed doses | — More restrictions on admission - Many possible side effects |
Compound
| Film-coated tablets | 1 table |
| active substances: | |
| ethinylestradiol | 30 mcg |
| drospirenone | 3 mg |
| excipients: lactose monohydrate - 48.17 mg; corn starch - 14.4 mg; pregelatinized corn starch - 9.6 mg; povidone K25 - 4 mg; magnesium stearate - 800 mcg; hypromellose (hydroxypropyl methylcellulose) - 1.0112 mg; macrogol 6000 - 202.4 mcg; talc (magnesium hydrosilicate) - 202.4 mcg; titanium dioxide (E171) - 556.5 μg; iron (II) oxide (E172) - 27.5 μg |
Pharmacodynamics
Yarina® is a low-dose monophasic oral combined estrogen-progestogen contraceptive drug.
The contraceptive effect of Yarina® is mainly achieved by suppressing ovulation and increasing the viscosity of cervical mucus.
The incidence of venous thromboembolism (VTE) in women with or without risk factors for VTE using ethinyl estradiol/drospirenone-containing oral contraceptives at a dose of 0.03 mg/3 mg is the same as in women using levonorgestrel-containing combined oral contraceptives or other combined oral contraceptives . This was confirmed in a prospective controlled database study that compared women using oral contraceptives at a dose of 0.03 mg ethinyl estradiol/3 mg drospirenone with women using other combined oral contraceptives. Data analysis revealed a similar risk of VTE among the sample.
In women taking combined oral contraceptives, the menstrual cycle becomes more regular, painful menstrual-like bleeding is less common, the intensity and duration of bleeding decreases, resulting in a reduced risk of iron deficiency anemia. There is also evidence of a reduced risk of endometrial and ovarian cancer.
Drospirenone contained in Yarin® has an antimineralocorticoid effect and is able to prevent weight gain and the appearance of other symptoms (for example, edema) associated with estrogen-dependent fluid retention. Drospirenone also has antiandrogenic activity and helps reduce acne (blackheads), oily skin and hair. This effect of drospirenone is similar to the effect of natural progesterone produced by the female body. This should be taken into account when choosing a contraceptive, especially for women with hormone-dependent fluid retention, as well as women with acne and seborrhea. When used correctly, the Pearl index (an indicator reflecting the number of pregnancies in 100 women using a contraceptive during the year) is less than 1. If pills are missed or used incorrectly, the Pearl index may increase.
Reviews about Yarina Plus
Reviews about Yarina Plus on forums are generally positive. Of the associated effects, the most often noted is the appearance or elimination of acne , deterioration or improvement in the condition of hair and nails. Based on the reports of patients, we can say that unplanned pregnancy does not occur if the rules of administration are followed.
Reviews from doctors focus on the presence of calcium levomefolate , which reduces the likelihood of fetal development defects if pregnancy occurs after discontinuation of Yarina Plus.
Pharmacokinetics
Drospirenone
When taken orally, drospirenone is rapidly and almost completely absorbed. After a single oral dose, the serum Cmax of drospirenone, equal to 37 ng/ml, is achieved within 1–2 hours. Bioavailability ranges from 76 to 85%. Food intake does not affect the bioavailability of drospirenone.
Drospirenone binds to serum albumin (0.5–0.7%) and does not bind to sex hormone binding globulin (SHBG) or corticosteroid binding globulin (CBG). Only 3–5% of the total concentration in the blood serum is found in free form. The increase in SHBG induced by ethinyl estradiol does not affect the binding of drospirenone to plasma proteins.
After oral administration, drospirenone is completely metabolized.
Most metabolites in plasma are represented by acidic forms of drospirenone, which are formed without the involvement of cytochrome P450.
The concentration of drospirenone in blood plasma decreases in 2 phases. Drospirenone is not excreted unchanged. Drospirenone metabolites are excreted by the kidneys and intestines in a ratio of approximately 1.2–1.4. T1/2 for excretion of metabolites in urine and feces is approximately 40 hours.
During cyclic treatment, the maximum steady-state serum concentration of drospirenone is achieved in the second half of the cycle.
A further increase in the serum concentration of drosperinone is observed after 1–6 cycles of administration, after which no increase in concentration is observed.
Additional information for special categories of patients
Patients with liver disorders. In women with moderate liver dysfunction (class B on the Child-Pugh scale), AUC is comparable to the corresponding indicator in healthy women with similar Cmax values in the absorption and distribution phases. T1/2 of drospirenone in patients with moderate liver dysfunction was 1.8 times higher than in healthy volunteers with intact liver function.
In patients with moderate liver dysfunction, a 50% decrease in the clearance of drospirenone was observed compared with women with preserved liver function, while there were no differences in the concentration of potassium in the blood plasma in the studied groups. When diabetes mellitus is detected and concomitant use of spironolactone (both conditions are regarded as factors predisposing to the development of hyperkalemia), an increase in the concentration of potassium in the blood plasma has not been established.
It should be concluded that drospirenone is well tolerated in women with mild to moderate liver dysfunction (Child-Pugh class B).
Patients with kidney disorders. The concentration of drospirenone in the blood plasma when reaching a steady state was comparable in women with mild renal impairment (Cl creatinine - 50-80 ml/min) and in women with preserved renal function (Cl creatinine - > 80 ml/min). However, in women with moderate renal impairment (Cl creatinine 30–50 ml/min), the average plasma concentration of drospirenone was 37% higher than in patients with preserved renal function. Drospirenone was well tolerated by all groups of patients. There were no changes in the concentration of potassium in the blood plasma when using drospirenone.
Ethinyl estradiol
After oral administration, ethinyl estradiol is rapidly and completely absorbed. Cmax in blood plasma, equal to approximately 54–100 pg/ml, is achieved in 1–2 hours. During absorption and first passage through the liver, ethinyl estradiol is metabolized, resulting in its oral bioavailability, on average, about 45%.
Ethinyl estradiol is almost completely (approximately 98%), although nonspecifically, bound by albumin. Ethinyl estradiol induces the synthesis of SHBG.
Ethinyl estradiol undergoes presystemic conjugation, both in the mucous membrane of the small intestine and in the liver. The main route of metabolism is aromatic hydroxylation.
The decrease in the concentration of ethinyl estradiol in the blood plasma is biphasic. It is not excreted from the body unchanged. Metabolites of ethinyl estradiol are excreted in urine and bile in a ratio of 4:6 with T1/2 for about 24 hours.
Css is achieved during the second half of the cycle.
Drug effectiveness criteria
Yarina and Yarina Plus are contraceptives with a unique composition. To date, these are the only drugs that have undergone large-scale randomized trials and proven to be effective. It is known that the combination of ethinyl estradiol + drospirenone reliably protects against unwanted pregnancy, controls the menstrual cycle and relieves premenstrual syndrome.
Yarina FDA not only as a contraceptive, but also for the treatment of acne. that drospirenone in combination with ethinyl estradiol effectively copes with the symptoms of mild to moderate acne. The antiandrogenic effect of drugs is used in dermatology.
Yarina is a drug recommended for the treatment of certain gynecological diseases. The contraceptive is successful in the treatment of conditions associated with hyperandrogenism and excess hair growth, and some forms of infertility.
Contraindications
Yarina® should not be used if you have any of the conditions/diseases listed below:
thrombosis (venous and arterial) and thromboembolism currently or in history (including deep vein thrombosis, pulmonary embolism, myocardial infarction, stroke), cerebrovascular disorders;
conditions preceding thrombosis (including transient ischemic attacks, angina) currently or in history;
migraine with focal neurological symptoms currently or in history;
diabetes mellitus with vascular complications;
multiple or severe risk factors for venous or arterial thrombosis, incl. complicated lesions of the valvular apparatus of the heart, atrial fibrillation, diseases of the cerebral vessels or coronary arteries; uncontrolled arterial hypertension, major surgery with prolonged immobilization, smoking over the age of 35 years;
pancreatitis with severe hypertriglyceridemia currently or in history;
liver failure and severe liver diseases (until normalization of liver tests);
liver tumors (benign or malignant) currently or in history;
severe and/or acute renal failure;
identified hormone-dependent malignant diseases (including genital organs or mammary glands) or suspicion of them;
bleeding from the vagina of unknown origin;
pregnancy or suspicion of it;
breastfeeding period;
hypersensitivity to any of the components of the drug Yarina®.
If any of these conditions develop for the first time while taking Yarina®, the drug should be discontinued immediately.
CAREFULLY
The potential risks and expected benefits of using combined oral contraceptives should be carefully weighed in each individual case in the presence of the following diseases/conditions and risk factors:
risk factors for the development of thrombosis and thromboembolism: smoking, obesity, dyslipoproteinemia, arterial hypertension, migraine, heart valve defects, prolonged immobilization, major surgical interventions, extensive trauma, hereditary predisposition to thrombosis (thrombosis, myocardial infarction or cerebrovascular accident at a young age in anyone - or one of the closest relatives);
other diseases in which peripheral circulatory disorders may occur (diabetes mellitus, systemic lupus erythematosus, hemolytic uremic syndrome, Crohn's disease and ulcerative colitis, sickle cell anemia), phlebitis of the superficial veins;
hereditary angioedema;
hypertriglyceridemia;
liver diseases;
diseases that first appeared or worsened during pregnancy or against the background of previous use of sex hormones (for example, jaundice and/or itching associated with cholestasis, cholelithiasis, otosclerosis with hearing impairment, porphyria, pregnancy herpes, Sydenham's chorea);
postpartum period.
Use during pregnancy and breastfeeding
The drug is not prescribed during pregnancy and breastfeeding. If pregnancy is detected while taking Yarina®, it should be discontinued immediately. However, extensive epidemiological studies have not revealed an increased risk of developmental defects in children born to women who received sex hormones before pregnancy or teratogenic effects in cases of inadvertent use of sex hormones in early pregnancy. At the same time, data on the results of taking Yarina® during pregnancy are limited, which does not allow us to draw any conclusions about the negative impact of the drug on pregnancy, the health of the newborn and the fetus. Currently, no significant epidemiological data are available.
Taking combined oral contraceptives may reduce the amount of breast milk and change its composition, so their use is not recommended until you stop breastfeeding. Small amounts of sex steroids and/or their metabolites may be excreted in milk.
Analogs
Level 4 ATC code matches:
Ovidon
Rigevidon
Non-Ovlon
Mercilon
Yarina
Miniziston 20 fem
Novinet
Microgynon
Janine
Lindineth
Cyclo-Proginova
Regulon
Logest
Midiana
Belara
Femoden
Jess Plus
Jess
Zoely
The closest analogue of the described product is a drug called Jazz Plus .
Side effects
The most commonly reported adverse reactions to Yarina® include nausea and breast pain. They occurred in more than 6% of women using this drug.
Serious adverse reactions include arterial and venous thromboembolism.
The table below shows the frequency of adverse reactions. reported during clinical trials of Yarina® (N=4897). Within each group, allocated depending on the frequency of occurrence of an adverse reaction, adverse reactions are presented in order of decreasing severity. Based on frequency, they are divided into frequent (≥1/100 and <1/10), infrequent (≥1/1000 and <1/100) and rare (≥1/10000 and <1/1000). For additional adverse reactions identified only during post-marketing studies, and for which it was not possible to estimate the frequency of occurrence, “frequency unknown” is indicated (see Table 1).
Table 1
| System-organ classes (MedDRA version) | Often | Infrequently | Frequency unknown |
| Mental disorders | Mood swings, depression, depressed mood, decreased or loss of libido | ||
| Nervous system | Migraine | ||
| Vascular disorders | Venous or arterial thromboembolism* | ||
| Gastrointestinal tract | Nausea | ||
| Skin and subcutaneous tissues | Erythema multiforme | ||
| Reproductive system and mammary glands | Pain in the mammary glands, irregular uterine bleeding, bleeding from the genital tract of unspecified origin |
Adverse events during clinical trials were codified using the MedDRA dictionary (Medical Dictionary for Regulatory Activities, version 12.1). Different MedDRA terms reflecting the same symptom were grouped together and presented as a single adverse reaction to avoid diluting or diluting the true effect.
* — Approximate frequency based on the results of epidemiological studies covering the group of combined oral contraceptives. The frequency bordered on very rare.
— Venous or arterial thromboembolism includes the following entities: peripheral deep vein occlusion, thrombosis and embolism/pulmonary vascular occlusion, thrombosis, embolism and infarction/myocardial infarction/cerebral infarction and stroke not defined as hemorrhagic.
For venous and arterial thromboembolism, migraine, see also “Contraindications” and “Special instructions”.
Additional Information
Listed below are adverse reactions with a very rare incidence or with delayed symptoms, which are believed to be associated with taking drugs from the group of combined oral contraceptives (see also “Contraindications” and “Special instructions”).
Tumors:
- The incidence of breast cancer diagnosis in women taking combined oral contraceptives is slightly increased. Because breast cancer is rare in women under 40 years of age, the increase in breast cancer diagnoses in women taking combined oral contraceptives is small relative to the overall risk of breast cancer.
- liver tumors (benign and malignant).
Other states:
- erythema nodosum;
- women with hypertriglyceridemia (increased risk of pancreatitis while taking combined oral contraceptives);
- increased blood pressure;
- conditions that develop or worsen while taking combined oral contraceptives, but their connection with taking the drug has not been proven (jaundice and/or itching associated with cholestasis; formation of gallstones; porphyria; systemic lupus erythematosus; hemolytic-uremic syndrome; chorea Sydenham; herpes of pregnant women; hearing loss associated with otosclerosis);
- in women with hereditary angioedema, taking estrogens can cause or aggravate its symptoms;
- liver dysfunction;
- impaired glucose tolerance or effect on insulin resistance;
- Crohn's disease, ulcerative colitis;
- chloasma;
- hypersensitivity (including symptoms such as rash, urticaria).
Interaction. The interaction of combined oral contraceptives with other drugs (inducers of microsomal liver enzymes, some antibiotics) can lead to breakthrough bleeding and/or a decrease in contraceptive effectiveness (see “Interaction”).
Yarina Plus price, where to buy
The price of Yarina Plus in Russian pharmacies averages 890-940 rubles for package No. 28.
In Ukraine, a similar form of release will cost 250-320 hryvnia, depending on the region.
- Online pharmacies in RussiaRussia
- Online pharmacies in UkraineUkraine
ZdravCity
- Yarina plus tab.
p.p.o. 3mg+0.03mg+0.451mg n28 Bayer Weimar/Bayer Pharma RUB 1,186 order - Yarina plus tab. p.p.o. 3mg+0.03mg+0.451mg n84 Bayer Weimar/Bayer Pharma
RUR 3,080 order
Pharmacy Dialogue
- Yarina plus (tab. No. 28) Bayer
RUB 1,157 order
- Yarina plus (tab. No. 28) Bayer
RUB 1,185 order
- Yarina plus (table p/o No. 28x3) Bayer
RUB 2,977 order
show more
Pharmacy24
- Yarina plus N28 tablets - 3 packs Promotion of Bayer Pharma AG, Nimecchina/Bayer Weimar GmbH i Co.
KG, Nimechchyna 631 UAH.order - Yarina plus No. 28 tablets Bayer Pharma AG, Nimechchina/Bayer Weimar GmbH i Co. KG, Nimechchyna
261 UAH. order
Interaction
Interaction of oral contraceptives with other drugs may lead to breakthrough bleeding and/or decreased contraceptive reliability. Women taking these drugs should temporarily use barrier methods of contraception in addition to Yarina®, or choose another method of contraception.
The following types of interactions have been reported in the literature.
Effect on hepatic metabolism. The use of drugs that induce liver microsomal enzymes can lead to an increase in the clearance of sex hormones, which in turn can lead to breakthrough bleeding or reduced contraceptive reliability. These drugs include: phenytoin, barbiturates, primidone, carbamazepine, rifampicin, rifabutin, possibly also oxcarbazepine, topiramate, felbamate, griseofulvin and preparations containing St. John's wort.
HIV protease inhibitors (eg ritonavir) and non-nucleoside reverse transcriptase inhibitors (eg nevirapine) and combinations thereof also have the potential to affect hepatic metabolism.
Effect on enterohepatic circulation. According to individual studies, some antibiotics (for example, penicillins and tetracyclines) may reduce the enterohepatic circulation of estrogens, thereby lowering the concentration of ethinyl estradiol.
While taking medications that affect microsomal enzymes, and for 28 days after their discontinuation, you should additionally use a barrier method of contraception.
While taking antibiotics (such as penicillins and tetracyclines) and for 7 days after their discontinuation, you should additionally use a barrier method of contraception. If during these 7 days of the barrier method of contraception the tablets in the current package run out, then you should start taking tablets from the next package of Yarina® without the usual break in taking the tablets.
The main metabolites of drospirenone are formed in plasma without the participation of the cytochrome P450 system. Therefore, the effect of inhibitors of the cytochrome P450 system on the metabolism of drospirenone is unlikely.
Oral combination contraceptives may affect the metabolism of other drugs, leading to an increase (for example, cyclosporine) or a decrease (for example, lamotrigine) in their plasma and tissue concentrations.
Based on in vitro interaction studies, as well as an in vivo study in female volunteers taking omeprazole, simvastatin and midazolam as markers, it can be concluded that the effect of drospirenone 3 mg on the metabolism of other medicinal substances is unlikely.
There is a theoretical possibility of an increase in serum potassium levels in women receiving Yarina® concomitantly with other drugs that can increase serum potassium levels. These drugs include angiotensin II receptor antagonists, some anti-inflammatory drugs, potassium-sparing diuretics, and aldosterone antagonists. However, in studies evaluating the interaction of drospirenone with ACE inhibitors or indomethacin, there was no significant difference in serum potassium concentrations compared with placebo.
Directions for use and doses
Orally, in the order indicated on the package, every day at approximately the same time, with a small amount of water.
Take one tablet per day continuously for 21 days. Taking tablets from the next package begins after a 7-day break, during which menstrual-like bleeding usually develops (withdrawal bleeding). As a rule, it begins on the 2-3rd day after taking the last tablet and may not end until you start taking tablets from a new package.
How to start taking Yarina®
If you have not taken any hormonal contraceptives in the previous month
Taking Yarina® begins on the first day of the menstrual cycle (i.e., on the first day of menstrual bleeding). It is possible to start taking it on the 2nd–5th day of the menstrual cycle, but in this case it is recommended to additionally use a barrier method of contraception during the first 7 days of taking the tablets from the first package.
When switching from other combined oral contraceptives, vaginal ring or contraceptive patch
It is preferable to start taking Yarina® the next day after taking the last active tablet from the previous package, but in no case later than the next day after the usual 7-day break (for drugs containing 21 tablets) or after taking the last inactive tablet (for drugs containing containing 28 tablets per package). Taking Yarina® should begin on the day the vaginal ring or patch is removed, but no later than the day when a new ring is to be inserted or a new patch is applied.
When switching from contraceptives containing only gestagens (mini-pills, injectable forms, implant), or from a gestagen-releasing intrauterine contraceptive (Mirena)
You can switch from the “mini-pill” to Yarina® on any day (without a break), from an implant or intrauterine contraceptive with gestagen - on the day of its removal, from the injection form - from the day when the next injection is due. In all cases, it is necessary to use an additional barrier method of contraception during the first 7 days of taking the pills.
After an abortion in the first trimester of pregnancy
You can start taking the drug immediately, on the day of the abortion. If this condition is met, the woman does not need additional contraception.
After childbirth or abortion in the second trimester of pregnancy
You should start taking the drug no earlier than 21–28 days after childbirth (in the absence of breastfeeding) or abortion in the second trimester of pregnancy. If use is started later, it is necessary to use an additional barrier method of contraception during the first 7 days of taking the pills. However, if a woman has already been sexually active, pregnancy should be excluded before starting to take Yarina® or she must wait until her first menstruation.
Taking missed pills
If the delay in taking the drug is less than 12 hours, contraceptive protection is not reduced. The woman should take the pill as soon as possible, and the next one should be taken at the usual time.
If the delay in taking the pills is more than 12 hours, contraceptive protection is reduced. The more pills are missed and the closer the missed pill is to the 7-day break in taking pills, the greater the likelihood of pregnancy.
In this case, you can be guided by the following two basic rules:
- taking the drug should never be interrupted for more than 7 days;
— to achieve adequate suppression of hypothalamic-pituitary-ovarian regulation, 7 days of continuous pill taking are required.
Accordingly, the following advice can be given if the delay in taking tablets exceeds 12 hours (the interval since the last tablet was taken is more than 36 hours).
First week of taking the drug
The last missed pill should be taken as soon as possible, as soon as the woman remembers (even if this means taking two pills at the same time). The next tablet is taken at the usual time. Additionally, a barrier method of contraception (such as a condom) should be used for the next 7 days. If sexual intercourse took place within a week before missing the pill, the possibility of pregnancy must be taken into account.
Second week of taking the drug
The last missed pill should be taken as soon as possible, as soon as the woman remembers (even if this means taking two pills at the same time). The next tablet is taken at the usual time. Provided that the woman has taken the pills correctly for the 7 days preceding the first missed pill, there is no need to use additional contraceptive measures. Otherwise, or if you miss two or more tablets, you must additionally use barrier methods of contraception (for example, a condom) for 7 days.
Third week of taking the drug
The risk of pregnancy increases due to the upcoming break in taking the pills. A woman must strictly adhere to one of the two options below. However, if during the 7 days preceding the first missed pill, all pills were taken correctly, there is no need to use additional contraceptive methods.
1. It is necessary to take the last missed pill as soon as possible, as soon as the woman remembers it (even if this means taking two pills at the same time). The next tablets are taken at the usual time until the tablets in the current pack are gone. You should start taking the tablets from the next package immediately without interruption. Withdrawal bleeding is unlikely until the second pack is finished, but spotting and breakthrough bleeding may occur while taking the tablets.
2. You can stop taking tablets from the current package, thus starting a 7-day break (including the day you skipped tablets), and then start taking tablets from a new package.
If a woman misses taking pills and then does not have withdrawal bleeding during the break, pregnancy must be ruled out.
Recommendations in case of vomiting and diarrhea
If vomiting or diarrhea occurs within 4 hours of taking the tablets, absorption may not be complete and additional measures should be taken to protect against unwanted pregnancy. In such cases, you should follow the above recommendations when skipping pills.
Changing the day of the onset of menstrual bleeding
In order to delay the onset of menstrual bleeding, it is necessary to continue taking tablets from the new package of Yarina® without a 7-day break. Tablets from the new package can be taken for as long as necessary, incl. until the tablets in the package run out. While taking the drug from the second package, spotting from the vagina or breakthrough uterine bleeding are possible. You should resume taking Yarina® from the next package after the usual 7-day break.
In order to move the day of the onset of menstrual bleeding to another day of the week, a woman should shorten the next break in taking pills by as many days as she wants. The shorter the interval, the higher the risk that she will not have withdrawal bleeding, and will subsequently experience spotting and breakthrough bleeding while taking the second pack (just as if she would like to delay the onset of menstrual-like bleeding).
Additional information for special categories of patients
Children and teenagers. The drug Yarina is indicated only after the onset of menarche. Available data do not suggest dose adjustment in this group of patients.
Elderly patients. Not applicable. Yarina® is not indicated after menopause.
Patients with liver disorders. Yarina® is contraindicated in women with severe liver disease until liver function tests return to normal (see also “Contraindications” and “Pharmacokinetics”).
Patients with kidney disorders. Yarina® is contraindicated in women with severe renal failure or acute renal failure (see also “Contraindications” and “Pharmacokinetics”).