Eating dry food, snacking on the run - this has become commonplace in the modern world. Unfortunately, every year the number of patients with gastritis, as well as gastric and duodenal ulcers, is steadily increasing. Today, there are many drugs available to treat these diseases. One of the drugs - De-Nol - is effective and safe, which will help cope with gastritis and ulcers.
pharmachologic effect
The drug has an astringent effect, due to which a film forms on the surface of the mucous membrane of the stomach and duodenum at the site of the lesion. Thus, the affected areas are protected from the aggressive action of gastric juice, which means that the progression of the process is suspended. The presence of a protective film promotes scarring of ulcerative lesions.
De-Nol is harmful to Helicobacter pylori, which is the main culprit in the formation of ulcers on the gastrointestinal mucosa. Not a single strain of this pathogenic bacterium is resistant to this drug.
In addition, taking the drug has a beneficial effect on the digestion process in the stomach due to the fact that it improves microcirculation in the mucous membrane of its antrum.
How is Gastropanel performed?
Blood sampling to determine markers of atrophic gastritis is carried out in the morning on an empty stomach and 20 minutes after a protein breakfast. Blood is collected into serum tubes, which are centrifuged for analysis.
Blood serum analysis determines markers of chronic atrophic gastritis. Markers of atrophy of the mucous membrane of the fundic and antral parts of the stomach are:
- Pepsinogen I, Pepsinogen II and their ratio,
- Gastrin-17 and Gastrin-17 stimulated after a protein breakfast,
- determination of antibodies to Helicobacter pylori Ig G.
The tests are based on enzyme immunoassay technology.
Besides,
- Antibodies to parietal cells of the body of the stomach are determined in autoimmune atrophic gastritis with a high risk of disorders associated with vitamin B12 deficiency, for which the level of vitamin B12 is determined.
- Homocysteine is identified as a risk factor for vascular and thromboembolic diseases.
- To clarify Helicobacter pylori infection, an additional test of the acute phase of infection is performed, Ig A and IgM antibodies are determined.
What do De-Nol tablets help with?
Taking this medicine is indicated for:
- Acute and chronic gastritis and gastroduodenitis;
- Exacerbations of gastric and duodenal ulcers;
- Gastropathy that developed as a result of taking NSAIDs or alcohol;
- Functional dyspepsia.
In addition, a gastroenterologist may prescribe De-Nol for pancreatitis. In this case, the drug helps eliminate intestinal dyskinesia, which often accompanies a chronic inflammatory process in the pancreas.
Bismuth preparations in medical practice
Bismuth is a chemical element of the 15th group of the sixth period of the periodic table of chemical elements of D. I. Mendeleev; has atomic number 83, and under normal conditions is a shiny silvery metal with a pinkish tint. Actually, the element was introduced into chemical nomenclature as “bismuth” in 1819 by the Swedish chemist J. Berzelius. Without being malleable or malleable, bismuth is easily crushed into powder. Bismuth has been known since ancient times (the first mention of it in chemical literature dates back to the 15th century), but for a long time it was considered a type of tin, lead or antimony. The idea of bismuth as an independent chemical element emerged only in the 18th century, after its chemical identity was established in 1739 by the German chemist I. Pott [1, 2].
The biological role of bismuth has been poorly studied; scientists suggest that this element induces the synthesis of low molecular weight proteins, takes part in ossification processes, and forms intracellular inclusions in the epithelium of the renal tubules. The current level of knowledge does not allow us to speak definitely about any physiological role of bismuth in the human body. Its intake into the body with water or food is insignificant, since the absorption of bismuth entering the gastrointestinal tract is extremely small and amounts to about 5%. The daily intake of bismuth into the body from food is 0.02 mg, and from air - 0.00001 mg.
It seems much more likely that bismuth will enter the body with medications when taken orally or through the skin (for external use). In total, the human body enters the human body with food, as well as with air and water, in the amount of 5–20 mcg/day. After absorption, bismuth is found in the blood in the form of compounds with proteins, and also penetrates into red blood cells. Bismuth is distributed relatively evenly between organs and tissues. Some accumulation of bismuth may be observed in the liver, kidneys (up to 1 μg/g), spleen and bones. Bismuth is also found in the brain. Bismuth belongs to the category of heavy metals; it is a moderately toxic element. A number of sources even call bismuth “the most harmless” of all heavy metals. Being very close in its properties to lead, bismuth is much less toxic. In this regard, environmentalists are advocating for the gradual replacement of lead in industrial and production processes with bismuth. Occupational poisoning or skin diseases are almost never reported when working with bismuth; the carcinogenicity of this metal has also not been established. Usually, even huge doses of bismuth taken orally do not cause poisoning, which is explained by the difficulty of absorption of bismuth compounds [2].
Leukocytes are responsible for transporting bismuth to various organs in the body. Captured by leukocytes and carried by the blood and lymph throughout the body, bismuth accumulates in the spleen, central nervous system and excretory organs, which include the kidneys, liver, intestines, and salivary glands. Its bioavailability is very low - 0.16–1.5% of the dose taken. The average concentration of bismuth in the blood after a course of treatment does not exceed 3–58 mcg/l. Traces of this element have been found in sweat, tears and breast milk. Resorbed bismuth is excreted in the urine. Long-term use of bismuth preparations in large doses can cause symptoms of “bismuth” encephalopathy (especially in patients with impaired renal function). Based on an analysis of 945 clinical cases, it was proven that side effects occur only when very high doses of drugs (up to 20 g/day) are used for a long time (2–20 years or more) [3].
Bismuth is mentioned in the works of many authors of books of the 15th–17th centuries, in particular by Valentine and Paracelsus. 150 years ago, some bismuth compounds were used as a disinfectant, drying agent, astringent and antiseptic. Bismuth is an element that, like silver, has antimicrobial properties. The independent use of bismuth for therapeutic purposes is difficult due to a number of undesirable effects, therefore, optimization of the use of bismuth as an antibacterial agent is associated with the development of appropriate forms and complexes (salts) that allow efficient transport of this ion to the immediate site of action. The therapeutic activity of bismuth compounds has been known for a long time and has been described for various bismuth salts, and its oral and parenteral administration was intended for the treatment of a number of diseases, such as syphilis, Vincent's angina and amoebiasis dysentery [4]. When bismuth salts became widely in demand, small-scale production of their preparations in the form of mixtures was established. Bismuth ammonium citrate (BAC), sometimes bismuth tartrate, known as “bismuth ammonium citrate with pepsin,” became widely known in Great Britain in the first half of the 20th century. Bismuth preparations have been described in various articles of the British Pharmaceutical Codex since the 1929 edition.
Around the same time, bismuth preparations were developed in Germany, in which protein or peptide hydrolysates and their fractions were used as a complexing agent (German Pat. No. 117 269, German Pat. No. 101 683, German Pat. No. 202 955). But they had obvious disadvantages - the unregulated release of bismuth ions (determined by the pH values of the stomach) were adsorbed in the upper gastrointestinal tract, forming compounds that caused the penetration of bismuth ions into the internal environments of the body. These shortcomings contributed to the search for new effective and safe bismuth derivatives.
Bismuth compounds have an antispirochetal effect, and the mechanism of their action is that bismuth ions, penetrating into spirochetes, bind the sulfhydryl groups (SH) of their enzymes, leading to disruption of the vital functions and death of syphilis pathogens. Such drugs are administered intramuscularly, since when taken orally, bismuth-containing compounds are practically not absorbed from the digestive tract. However, with parenteral intake of bismuth into the body, there is a danger of damage to those organs in which bismuth ions accumulate. The toxic and lethal doses of the eighty-third element for humans have not been determined. Chronic intake of bismuth in quantities of 1–1.5 grams per day is considered dangerous. The importance of bismuth salts in medicine increases over time. Many drugs have been developed based on bismuth gallate, tartrate, carbonate, tribromophenolate, subcitrate and subsalicylate. In medical practice, drugs such as Vikalin, Vikair, Vikram, Neo-Anuzol, Bismuth ointment, Dermatol, Xeroform, Pentabismol, Bismutogvi, De-Nol, Novobismol and others are used.
Previous studies have determined that combining bismuth with thiol (-SH, sulfhydryl) compounds, such as bismuth ethanedithiol, improves the antimicrobial activity of bismuth compared to other bismuth salts. The search for new optimized bismuth transmitters continues, as evidenced by a recent patent for an invention [5], describing the preparation and use of a bismuth-thiol composition as an effective antibacterial agent.
Today in Russia, gastroenterologists most widely use colloidal bismuth subcitrate, or, as it is also called, bismuth tripotassium dicitrate (BTD). The discovery of Helicobacter pylori (H. pylori) in 1983 by Australians J. Warren and B. Marshall revolutionized the treatment of peptic ulcers [6], it renewed interest in bismuth compounds, since it was found that bismuth salts effectively suppress the growth of H. pylori in combination with antibiotics or in combination with antibiotics and acid-suppressive drugs [7, 8]. The first randomized controlled trial (RCT) using bismuth in anti-Helicobacter therapy found that bismuth was more effective than erythromycin monotherapy [9]. Another RCT compared the effectiveness of colloidal bismuth subcitrate versus cimetidine in H. pylori-positive duodenal ulcer over a 6-week period, with bismuth successfully eradicating H. pylori in 50% of patients [10]. The next RCT evaluated the combined use of colloidal bismuth subcitrate and cimetidine, alone or in combination with tinidazole, and found that colloidal bismuth subcitrate and tinidazole achieved H. pylori eradication in almost 75% of patients [11]. With the addition of a second antibiotic, tetracycline or amoxicillin, the eradication rate in later RCTs exceeded 80% [12–14]. However, some problems with bismuth-based triple therapy were identified, including the large number of pills patients were required to take, the duration of therapy, and side effects such as taste changes, nausea, and diarrhea. Systematic review and meta-analysis by A. Ford et al. There is strong evidence that bismuth compounds, used either alone or in combination with antibiotics and proton pump inhibitors (PPIs) to eradicate H. pylori, are safe and well tolerated [15].
VTD slows down the absorption of some antibiotics (tetracycline, amoxicillin), thereby increasing their concentration in the gastric contents - the site of application in the treatment of helicobacteriosis. In vitro and in vivo studies have shown that VTD is synergistic with other antibiotics against H. pylori. Thanks to this property, it has become an indispensable component of anti-Helicobacter therapy, and its combination with two antibiotics is still called “classical triple therapy.” In addition, one of the ways to overcome H. pylori resistance is to use bismuth dicitrate as a base preparation of colloidal tripotassium. This position is confirmed by studying the in vitro antibacterial activity of combinations of various drugs with clarithromycin and amoxicillin against H. pylori strains sensitive or resistant to macrolides. It was shown that the properties of VTD played a decisive role in overcoming strain resistance and obtaining a persistent bactericidal effect of these drug combinations [16].
Numerous scientific studies conducted on the background of the use of bismuth tripotassium dicitrate for erosive and ulcerative lesions of various etiologies have shown that the drug has a wide range of cytoprotection mechanisms. VTD reduces pepsin activity (by 20–30%); selectively binds to the proteins of the bottom of the ulcer and creates a protective layer - a barrier to the diffusion of H+, which prevents damage to the area of the mucous membrane (MU) of the stomach, devoid of a protective epithelial cover; stimulates local synthesis of prostaglandins (on average by 50%); increases the secretion of mucus and bicarbonates; increases local blood flow; suppresses the production of cytokines by cells of the inflammatory infiltrate; ensures reconstruction of the extracellular matrix and full angiogenesis; enhances the reparative effect mediated by epidermal growth factor. Morphologically, the mucous membrane of the gastroduodenal zone after healing of the ulcer is closer to the normal microstructure than when treated with other means. The use of high doses of VTD stimulates the production of prostaglandin E2 in gastric mucus, which is considered to be part of the mechanism that accelerates the healing of ulcerative lesions. Therapeutic doses of VDT cause sustained stimulation of prostaglandin production [17].
The mechanism of the antibacterial action of bismuth tripotassium dicitrate is associated not only with disruption of the adhesion of microorganisms to the epithelium of the mucous membrane, but also with disruption of ATP synthesis in the bacterial cell. Thus, in an in vitro study, incubation of H. pylori with tripotassium bismuth dicitrate led to a pronounced inhibition of the growth of the microorganism and its subsequent death [18]. Due to their anti-Helicobacter activity, colloidal bismuth preparations make it possible to increase or maintain the effectiveness of eradication therapy, especially in conditions of increasing antibiotic resistance of H. pylori. The anti-Helicobacter monoeffect of VTD averages 14–40%. The advantage of the drug is that there is no natural or acquired resistance of H. pylori to bismuth ions. Combination with antibiotics increases the degree of eradication to 50%, and the combination of two basic drugs - a proton pump inhibitor and bismuth tripotassium dicitrate - with two antibiotics makes it possible to overcome the resistance of H. pylori strains to nitrimidazole derivatives or clarithromycin.
Interesting results were presented by C. Srinarong et al. - 7-day standard triple therapy plus VTD and probiotic provided excellent eradication of H. pylori (100%) in areas with low clarithromycin resistance, such as Thailand, regardless of the CYP2C19 genotype of the pathogen [19].
In recent years, the importance of oxidative stress, potentiated by H. pylori bacteria (especially those with the CagA+/vacAs1 genotype), in the development of chronic gastritis has been shown [20]. Bismuth preparations turned out to be able to trap free oxygen radicals that are formed during oxidative stress and damage gastric mucosa, which serves as one of the components of their cytoprotective effect [21].
BTD has also proven itself well as a drug that can be successfully prescribed in the treatment of erosive and ulcerative lesions of the stomach and duodenum caused by taking non-steroidal anti-inflammatory drugs (NSAID-associated gastropathy). Thus, in a comparative study of the effectiveness of the use of VTD and ranitidine, healing of ulcers and multiple erosions of the stomach and duodenum after 4 weeks of treatment was achieved in 84.6% of patients receiving VTD, and only in 50% of patients receiving ranitidine [22]. In a comparative study on the effectiveness of using VTD (at a dose of 240 mg 2 times a day) in combination with a standard dose of omeprazole (20 mg per day) and omeprazole monotherapy in patients with NSAID-associated gastropathy, healing of erosive and ulcerative lesions of the stomach and duodenum after 2 weeks of treatment was achieved in 56.7% and 30.3% of patients, respectively, and after 4 weeks - in 100% and 93.9% of patients. An increase in the level of prostaglandins in the gastric mucosa, observed while taking VTD, indicated the cytoprotective effect of the drug [23, 24].
Due to their known antidiarrheal properties, bismuth compounds have been widely used to treat episodic diarrhea in children and adults for a century [25–28]. A number of studies have confirmed the effectiveness of bismuth subsalicylate in the prevention and treatment of traveler's diarrhea (E. coli enterotoxigenic). Enterotoxigenic E. coli was detected less frequently in travelers who received bismuth subsalicylate than in those who received placebo, demonstrating that bismuth subsalicylate prevents diarrhea by reducing the number and inhibiting the proliferation of enterotoxigenic E. coli [29].
Two studies reported the effectiveness of bismuth enema treatment for distal ulcerative colitis. Clinical and laboratory improvement was observed in 60% of patients resistant to conventional therapy, and 40% of patients achieved complete remission after 8 weeks of therapy [30]. A multicenter, double-blind, randomized, comparative study showed that when comparing the effectiveness of treatment with bismuth enemas with 5-aminosalicylic acid enemas, an equivalent therapeutic effect was established in the treatment of left-sided ulcerative colitis [31]. Oral bismuth is also effective for microscopic colitis [32] and as a colostomy deodorant [33].
In addition to its antibacterial properties [34, 25], bismuth also has anti-inflammatory effects [36] when passing through the intestines. There is experimental evidence supporting the role of bismuth in inhibiting the activity of inducible nitric oxide synthase in intestinal epithelial cells, as well as in the induction of heme oxygenase-1, thereby providing a therapeutic effect on inflammatory and oxidative reactions associated with inflammatory bowel diseases [37]. Another experimental study demonstrated the ability of bismuth to scavenge free radical oxygen in the context of chemical damage to the gastric mucosa [38]. Given these antibacterial and anti-inflammatory mechanisms, it can be theoretically assumed that bismuth should play a certain role in the pathogenetic treatment of acute and chronic diarrhea, as an antibacterial and antitoxic agent [39].
Hydrogen sulfide and other foul-smelling and toxic compounds are produced by colon bacteria when protein rots. In moderately severe ulcerative colitis [40], hydrogen sulfide is involved in inhibiting the oxidation of butyrate in the colon mucosa, which makes the mucosa more vulnerable to inflammatory agents [41, 42]. Bismuth, combining with hydrogen sulfide, forms insoluble, harmless bismuth sulfide and turns stool black [43].
The purpose of our original study was to evaluate the comparative characteristics of the infrared spectra (IR spectra) of two finished dosage forms of bismuth. The study analyzed the spectral characteristics of the most popular bismuth-containing drugs, namely the drugs De-Nol® (Netherlands) and Novobismol® (Russia). The active ingredient of these drugs is bismuth tripotassium dicitrate.
Spectral characteristics were obtained using an FSM-1202 infrared Fourier spectrometer (Russia). The pharmacologically active part of the tablet form was mixed with potassium bromide (Fluka, Germany) in a ratio of 1:100, and a disc was formed using a hydraulic press. The measurements were carried out in the range of 4000–400 cm-1, with a resolution of 4 cm-1 and a number of scans of 25. The device was controlled and data processed using the Fspec 4.0 program. The samples we studied had identical infrared spectra (Fig.).
The spectral characteristics of bismuth tripotassium dicitrate samples are interesting from the point of view of the spectral characteristics of the complex compound. Thus, in the spectrum of the samples, two characteristic broad absorption bands can be noted at 1579 and 1393 cm-1, caused by symmetric and asymmetric stretching vibrations in the COO fragment. This type of bond occurs in a chelate compound between the carboxyl groups of the citrate moieties and the complexing agent bismuth. It is this chelate form that causes a shift in the absorption bands corresponding to RCOO- and under normal conditions can be traced around 1560 and 1410 cm-1. It should be noted that similar shifts in the IR region of absorption bands for complex compounds of another type were previously described in the literature [44]. The absorption band at 1290 cm-1 found in the complex, in our opinion, is due to vibrations of C-O and O-Me (where Me are potassium or bismuth ions). It is the metal ions that cause the shift of the deformation (out-of-plane) vibrations of OH (950–900 cm-1) to a value of 845 cm-1, which corresponds to the bismuth complex under consideration. The vibrations of C-C bonds correspond to the absorption band at 910 cm-1. Accordingly, the bands at 1142, 1076, 1020 cm-1 are due to stretching vibrations of C-O and CH-O– fragments [45].
Thus, this study indicates almost complete pharmaceutical equivalence of the drugs we studied, De-Nol® and Novobismol®.
Literature
- Glinka N. L. General chemistry. L.: Chemistry, 2004. 702 p.
- https://ru.wikipedia.org/w/index.php?title=Bismuth.
- Bismuth-containing drugs in gastroenterology. Review // Health of Ukraine. 2009. No. 13–14. pp. 64–65.
- Kuever RA, Wheeler LM Bismuth compounds / United States Patent US2414650. Publication Date: January 21, 1947. Application Number: US48796443A.
- Bismuth-thiols as antiseptics for epithelial tissues, acute and chronic wounds, bacterial biofilms and other indications / United States Patent US8389021. Publication Date: 05/03/2013.
- Warren JR, Marshall BJ Unidentified curved bacilli on gastric epithelium in active chronic gastritis // Lancet. 1983. No. 321. R. 1273–1275.
- Wolle K., Malfertheiner P. Treatment of Helicobacter pylori // Best Pract Res Clin Gastroenterol. 2007. No. 21. R. 315–324.
- Marshall BJ, Warren JR Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration // Lancet. 1984. No. 1. R. 1311–1315.
- McNulty CA, Gearty JC, Crump B., Davis M., Donovan IA, Melikian V., Lister DM, Wise R. Campylobacter pyloridis and associated gastritis: investigator blind, placebo controlled trial of bismuth salicylate and erythromycin ethylsuccinate // Br Med J (Clin Res Ed). 1986. No. 293. R. 645–649.
- Coghlan JG, Gilligan D., Humphries H., McKenna D., Dooley C., Sweeney E., Keane C., O'Morain C. Campylobacter pylori and recurrence of duodenal ulcers—a 12-month follow-up study. Lancet. 1987. No. 2. R. 1109–1111.
- Marshall BJ, Goodwin CS, Warren JR, Murray R., Blincow ED, Blackbourn SJ, Phillips M., Waters TE, Sanderson CR Prospective double-blind trial of duodenal ulcer relapse after eradication of Campylobacter pylori // Lancet. 1988. No. 2. R. 1437–1442.
- Graham DY, Lew GM, Evans DG, Evans DJ, Klein PD Effect of triple therapy (antibiotics plus bismuth) on duodenal ulcer healing. A randomized controlled trial // Ann Intern Med. 1991. No. 115. R. 266–269.
- Graham DY, Lew GM, Klein PD, Evans DG, Evans DJ Jr., Saeed Z. A, Malaty HM Effect of treatment of Helicobacter pylori infection on the long-term recurrence of gastric or duodenal ulcer. A randomized, controlled study // Ann Intern Med. 1992. No. 116. R. 705–708.
- Rauws EA, Tytgat GN Cure of duodenal ulcer associated with eradication of Helicobacter pylori // Lancet. 1990. No. 335. R. 1233–1235.
- Ford AC, Malfertheiner P, Giguère M et al. Adverse events with bismuth salts for Helicobacter pylori eradication: Systematic review and meta-analysis // World J Gastroenterol. 2008. No. 14 (48). R. 7361–7370.
- Shcherbakov P. L., Vartapetova E. E., Nizhevich A. A. et al. Efficacy and safety of the use of bismuth tripotassium dicitrate (de-nol) in children // Klin. Pharmacol. ter. 2005. No. 1. P. 41–44.
- Okovityy S.V., Ivkin D.Yu. Bismuth preparations - pharmacological basis of the clinical effect // Treating Physician. 2015. No. 10. pp. 1–7.
- Stratton CW, Warner RR, Coudron PE, Lilly NA Bismuth-mediated disruption of the glycocalyx-cell wall of Helicobacter pylori: ultrastructural evidence for a mechanism of action for bismuth salts // J Antimicrob Chemother. 1999, May. No. 43 (5). R. 659–666.
- Srinarong C., Siramolpiwat S., Wongcha-Um A., Mahachai V., Vilaichone RK Improved Eradication Rate of Standard Triple Therapy by Adding Bismuth and Probiotic Supplement for Helicobacter pylori Treatment in Thailand // Asian Pac J Cancer Prev. 2014. No. 15 (22). R. 9909–9913.
- Augusto AC, Miguel F., Mendonca S. et al. Oxidative stress expression status associated to Helicobacter pylori virulence in gastric disease // Clin. Biochem. 2007. Vol. 40. P. 615–622.
- Bagchi D., McGinn Th., Ye X. et al. Mechanism of gastroprotection by bismuth subsalicylate against chemically induced oxidative stress in cultured human gastric mucosal cells // Dig. Dis. Sci. 1999. Vol. 44. P. 2419–2428.
- Karateev A. E., Nasonov E. L., Radenska-Lopovok S. G. Efficacy of bismuth tripotassium dicitrate (De-Nol) in gastropathy induced by nonsteroidal anti-inflammatory drugs: an open, controlled 4-week study // Ter. arch. 2005. No. 2. P. 45–49.
- Maev I.V., Vyuchnova E.S., Staseva I.V. Comparative assessment of various treatment regimens for gastropathy caused by non-steroidal anti-inflammatory drugs // Ter. arch. 2004. No. 2. pp. 27–30.
- Sheptulin A. A., Vize-Khripunova M. A. Modern possibilities of using bismuth preparations in gastroenterology // Russian Journal of Gastroenterology, Hepatology, Coloproctology. 2010. No. 3. pp. 63–67.
- DuPont HL, Sullivan P., Pickering LK, Haynes G., Ackerman PB Symptomatic treatment of diarrhea with bismuth subsalicylate among students attending a Mexican university // Gastroenterology. 1977. No. 73. R. 715–718.
- Bierer DW Bismuth subsalicylate: history, chemistry, and safety // Rev Infect Dis. 1990. No. 12. R. S3–S8.
- Gryboski JD, Kokoshis S. Effect of bismuth subsalicylate on chronic diarrhea in childhood: a preliminary report // Rev Infect Dis. 1990. No. 12. R. S36–S40.
- Figueroa-Quintanilla D., Salazar-Lindo E., Sack RB et al. A controlled trial of bismuth subsalicylate in infants with acute watery diarrheal disease // N Engl J Med. 1993. No. 328. R. 1653–1658.
- De la Cabada BJ, Dupont HL New Developments in Traveler's Diarrhea // Gastroenterol Hepatol. 2011, Feb. No. 7 (2). R. 88–95.
- Ryder SD, Walker RJ, Jones H., Rhodes JM Rectal bismuth subsalicylate as therapy for ulcerative colitis // Aliment Pharmacol Ther. 1990. No. 4. R. 333–338.
- Pullan R.D., Ganesh S., Mani V. et al. Comparison of bismuth citrate and 5-aminosalicylic acid enemas in distal ulcerative colitis: a controlled trial // Gut. 1993. No. 34. R. 676–679..
- Fine KD, Lee EL Efficacy of open-label bismuth subsalicylate for the treatment of microscopic colitis // Gastroenterology. 1998. No. 114. R. 29–36.
- Degos R. Bismuth in the treatment of syphilis // Int J Dermatol. 1977. No. 16. R. 391–392.
- Sun H., Zhang L., Szeto KY Bismuth in medicine // Met Ions Biol Syst. 2004. No. 41. R. 333–378.
- Degos R. Bismuth in the treatment of syphilis // Int J Dermatol. 1977. No. 16. R. 391–392.
- Ericsson CD, Tannenbaum C., Charles TT Antisecretory and antiinflammatory properties of bismuth subsalicylate // Rev Infect Dis. 1990. No. 12. R. S16–S20.
- Cavicchi M., Gibbs L., Whittle BJ Inhibition of inducible nitric oxide synthase in the human intestinal epithelial cell line, DLD-1, by the inducers of heme oxygenase 1, bismuth salts, heme, and nitric oxide donors // Gut. 2000. No. 47. R. 771–778.
- Bagchi D., McGinn TR, Ye X. et al. Mechanism of gastroprotection by bismuth subsalicylate against chemically-induced oxidative injury in human gastric mucosal cells // Gastroenterology. 1998. No. 114. R. A62.
- Thazhath S., Haque M., Florin T. Oral bismuth for chronic intractable diarrheal conditions? // Clin Exp Gastroenterol. 2013. No. 6. R. 19–25.
- Florin THJ, Gibson GR, Neale G., Cummings JH A role for sulfate reducing bacteria in ulcerative colitis? // Gastroenterology. 1990. No. 98. R. A170.
- Roediger WE The colonic epithelium in ulcerative colitis: an energy-deficiency disease? // Lancet. 1980. No. 2. R. 712–715.
- Chapman MA, Grahn MF, Boyle MA, Hutton M., Rogers J., Williams NS Butyrate oxidation is impaired in the colonic mucosa of sufferers of quiescent ulcerative colitis // Gut. 1994. No. 35. R. 73–76.
- Suarez FL, Furne JK, Springfield J., Levitt MD Bismuth subsalicylate markedly decreases hydrogen sulfide release in the human colon // Gastroenterology. 1998. No. 114. R. 923–929.
- McQuillin FJ, Parker DG, Stephenson GR Transition metal organometallics for organic synthesis // Cambridge university press, Cambridge. 1991. P. 19–20.
- Prech E., Bühlmann F., Affolter K. M. Determination of the structure of organic compounds / World; BINOMIAL. 2006. 438 p.
E. Yu. Plotnikova1, Doctor of Medical Sciences, Professor A. S. Sukhikh, Candidate of Medical Sciences
State Budgetary Educational Institution of Higher Professional Education Kemerovo State Medical Academy of the Ministry of Health of the Russian Federation, Kemerovo
1 Contact information
* The drug is not registered in the Russian Federation.
How to drink De-Nol
Adults and children over 12 years of age can take 4 tablets per day. They can be divided into 4 or 2 doses.
It is recommended to take the tablets half an hour before meals with water.
The drug is also used for diseases of the stomach and duodenum that are associated with the bacterium Helicobacter pylori. De-Nol is included in schemes for destroying this microbe along with antibacterial drugs.
According to experts, this drug increases the effectiveness of the Helicobacter pylori eradication (destruction) regimen. In addition, taking De-Nol is not accompanied by the risk of developing unnecessary adverse reactions, which is also important when using such a serious treatment regimen.
Advantages of Gastropanel for diagnosing “atrophic gastritis”
Thus, Gastropanel allows you to answer the following questions:
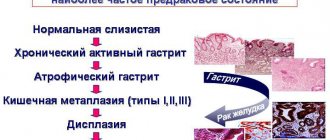
- does the patient have atrophic gastritis, in which part of the stomach are the changes localized,
- assess the risk of developing stomach cancer and peptic ulcers,
- does the patient suffer from gastritis caused by Helicobacter pylori,
- identify autoimmune gastritis or atrophic gastritis with damage to the body of the stomach, which may determine the risk of developing vitamin B12 deficiency, which can be associated with many diseases (atherosclerosis, vascular damage to the brain and heart, depression, polyneuropathy, dementia, etc.)
What advantages of Gastropanel can be noted: it is a simple non-invasive serological test, high sensitivity, specificity, safety and convenience for the patient, quick results, and meets the principles of evidence-based medicine.
Is De-Nol an antibiotic?
Despite the fact that the drug is capable of destroying Helicobacter pylori, it does not belong to the group of antibacterial agents. Consequently, its use is not associated with the appearance of such unpleasant side symptoms as diarrhea and mucosal candidiasis.
Bacteria cannot develop resistance to De-Nol due to the peculiarities of its pharmacological action. That is why the inclusion of this drug to destroy the pathogenic bacteria helps to completely get rid of the infection.
Atrophic gastritis - treatment
Replacement therapy
Replacement therapy includes the use of hydrochloric acid preparations and gastric juice enzymes:
- Natural gastric juice is a preparation of animal origin, the composition corresponding to human gastric juice, contains hydrochloric acid and enzymes. Use 1-2 tablespoons (15 - 30 ml) during meals or after meals 2-3 times a day.
- Acidin-pepsin , containing betaine hydrochloride, which is hydrolyzed in the stomach to release free hydrochloric acid and the enzyme pepsin. Before use, tablets (500 mg) are dissolved in 50-100 ml of water and taken with meals. These medications are administered through a straw.
- Abomin - the drug contains the sum of proteolytic enzymes of the stomach and is obtained from the gastric mucosa of calves and lambs. Use 1 tablet (0.2 g each containing 50,000 units in 1 tablet) 2 - 3 times a day with meals for 1 - 3 months.
Stimulant therapy
Some drugs that stimulate the secretion of gastric juice:
- Mineral water (Essentuki N17, Narzan) is used warm 15-20 minutes before meals, the course is 2-3 weeks, twice a year.
- Rosehip decoction , cabbage, tomato, carrot, lemon juice, 50 ml each, diluted with boiled water 1:1 before meals, alternate.
- Medicinal mixtures: plantain, St. John's wort, wormwood, thyme in equal proportions.
- Plantaglucide is widely used - granules of plantain leaves to prepare a suspension, for which take 1/1 -1 teaspoon (½-1 g) per ¼ glass of warm water and apply 30 minutes before meals 2-3 times a day, course of treatment 3- 4 weeks, for preventive treatment 1-2 months. Plantaglucide activates gastric secretion, has an enveloping, regenerative, anti-inflammatory and antispasmodic effect.
- Collection of herbalist Mikhalchenko S.I.:
Ingredients: angelica, yarrow, dandelion, birch, trifoliate, plantain, caraway, burnet, licorice, fumifera, calendula, chamomile. Application: pour 1 dessert spoon of the mixture into 500 ml of boiling water, leave in a thermos by volume overnight, strain. Take 150 ml 3 times a day an hour before meals. Before use, warm up by diluting with hot water. Keep refrigerated. Reception: 10 days admission - 2 days break, 3-4 months.
During the period of relative remission of atrophic gastritis, the main drugs are replacement and stimulating therapy, which affect the secretory insufficiency of the stomach.
Side effects of the drug De-Nol
Taking the drug may be accompanied by the following side effects:
- Nausea and vomiting, frequent bowel movements or constipation.
- On the part of the central nervous system – the development of encephalopathy. This phenomenon is observed only with long-term use of the drug in high doses.
- Skin itching and rashes in case of hypersensitivity to the components of the drug.
The development of adverse symptoms when taking De-Nol is rare. Usually, if all the rules for taking this medicine are followed, patients do not encounter such problems.
If you do get sick with COVID-19
It is important to inform the doctor treating COVID-19 about the chronic disease you have and the medications you are taking.
.
This will allow the doctor to choose the safest treatment for you and avoid prescribing medications that may adversely interact with the medications you regularly take.
If you have chronic liver disease, when infected with COVID-19, you should avoid an overdose of paracetamol (no more than 2 grams per day), and also minimize the use of non-steroidal anti-inflammatory drugs. Do not cancel your ongoing treatment for liver disease; discuss with your doctor the addition of ursodeoxycholic acid for the prevention and treatment of drug-induced liver damage.
If you have an autoimmune liver or intestinal disease, doctors recommend continuing your ongoing therapy, but taking medications such as azathioprine and methotrexate may be temporarily suspended.
If you have GERD or a peptic ulcer, then among antisecretory drugs you should give preference to rabeprazole or pantoprozole - safer in terms of the risk of drug interactions. It is important to avoid or minimize the use of non-steroidal anti-inflammatory drugs. During the period of COVID-19 disease, to prevent complications, doctors recommend additionally taking drugs that have a protective effect on the mucous membrane of the esophagus and stomach (rebamipide, etc.).
Overdose symptoms
An overdose of De-Nol is accompanied by impaired functional activity of the kidneys. These changes are reversible: after discontinuation of the drug, kidney function is completely normalized.
In case of overdose, saline laxatives and enterosorbents are used. Gastric lavage is also recommended.
In rare cases, if the dose is repeatedly exceeded, renal failure may develop. In this case, renal dysfunction can only be compensated for by hemodialysis.
Consequences of COVID-19 in patients with digestive diseases
A severe infection can lead to exacerbation and decompensation of chronic liver disease
, especially at the stage of liver cirrhosis.
It is rare to experience a severe reaction to drugs used to treat COVID-19 in the form of drug-induced hepatitis. This disease can also develop in patients with a previously healthy liver. Even more rarely, a virus and drugs can trigger the development of autoimmune liver disease
.
Therefore, all patients who have had COVID-19 should monitor a biochemical blood test after the infection resolves and, if abnormalities in biochemical parameters persist, contact a hepatologist
.
Previous COVID-19 and drug exposure can lead to exacerbation and complications (for example, bleeding, diarrhea) of other digestive diseases. Taking antibacterial drugs can lead to disruption of intestinal microflora
with the development of loose stools (so-called antibiotic-induced diarrhea).
This diarrhea goes away on its own and with the use of medications - probiotics, adsorbents. However, in some cases, if a special bacterium (clostridium) is present in the intestines, a severe and dangerous form of diarrhea can develop, which is called pseudomembranous colitis
.
Therefore, in all cases of abdominal pain, heartburn, nausea, diarrhea and bloating after COVID-19, you should consult a gastroenterologist and conduct a full examination to clarify the cause and carry out appropriate treatment
.