Eight small bones that make up the carpus (or carpus), which connects the hand to the forearm.
| Wrists | |
| Labeled image showing the eight bones of the wrist. | |
| details | |
| Identifiers | |
| Latin | Os Carpale sq. Ossa Carpi |
| MeSH | D002348 |
| TA98 | A02.4.08.001 |
| TA2 | 1249 |
| F.M.A. | 23889 |
| Anatomical terms of bone [edit in Wikidata] | |
In the carpal bones
eight small bones that make up the wrist (or wrists), which connects the hand to the forearm. The term "carpus" comes from the Latin carpus and Greek καρπός (karpós), meaning "wrist". In human anatomy, the primary role of the wrist is to facilitate effective positioning of the hand and effective use of the extensors and flexors of the forearm, and the mobility of the individual bones of the wrist increases freedom of movement of the wrist.[1]
In quadrupeds, then the wrist
the only cluster of carpal bones between the radius and ulna and metacarpus. The carpal bones do not belong to individual fingers (or toes in tetrapods), whereas the fingers on the metacarpal bone do. The corresponding part of the foot is the tarsus. The carpal bones allow the wrist to move and rotate vertically.[1]
Content
- 1 Structure 1.1 Bones
- 1.2 Joints
- 1.3 Accessory bones
- 3.1 Links
Development
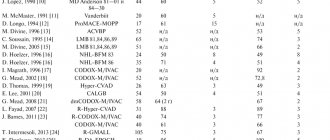
The appearance of foci of ossification of the wrist bones[6][7]
| Bone | Average | Variation[6] | Variation[7] |
| Capitate | 2.5 months | 1–6 months | 1–5 months |
| Hamate | 4-5.5 months | 1–7 months | 1–12 months |
| Triquetrum | 2 years | From 5 months to 3 years | From 9 months to 4 years and 2 months |
| Lunat | 5 years | 2-5.5 years | From 18 months to 4 years and 3 months |
| Trapezoid | 6 years | 4–8 years | |
| Trapezoid | 6 years | 4–8 years | |
| Scaphoid | 6 years | 4–7 years | |
| Pea | 12 years | 8–12 years |
The carpal bones are ossified endochondrally (from cartilage) and the ossifying centers appear only after birth.[5] The formation of these centers roughly follows a chronological spiral, starting with the capitate and chamate during the first year of life. The ulnae then ossify into the radii, while the sesamoid pisiform bone arises in the flexor carpi ulnaris tendon more than ten years later.[6] The onset of ossification of each bone occurs over time, just like other bones. This is useful in forensic age assessment.[7]
Fracture of the phalanges of the fingers
The cause is a blow with the fingers, an injury while fixing the fingers, or a direct blow to the phalanges. Fractures of the phalanges of the fingers can be:
- intra-articular;
- extra-articular;
- single;
- multiple - within one finger or several;
- combined with dislocations in the metacarpophalangeal or interphalangeal joints.
Symptoms: pain, swelling, hematoma, deformity. The pain intensifies when you try to move your fingers. The diagnosis is established on the basis of complaints, trauma history, objective examination and X-ray results. To treat a fracture of the phalanges of the fingers without displacement, fixation is performed with a plaster cast for 3-4 weeks. In case of fracture-dislocations, joint reduction is performed; in case of displacement of fragments, closed reduction is performed. If it is not possible to compare the fragments using a closed method, skeletal traction or pin osteosynthesis is indicated.
Function
Ligaments
Four groups of ligaments in the wrist area (shown in four different colors).
There are four groups of ligaments in the wrist area:[8]
- The carpal ligaments proper, which connect the ulna and radius to the wrist: ulnar and radial collateral ligaments; then the palmar and dorsal wrist ligaments; and palmar-ulnar ligament. (Shown in blue in the figure.)
- Intercarpal ligaments connecting the carpal bones to each other: radiate carpal ligament; then the dorsal, palmar, and interosseous intercarpal ligaments; and the pisohamate ligament. (Indicated in red in the figure.)
- Ligaments are the carpometacarpal joints that connect the carpal bones to the metacarpal bones: the pizometacarpal ligament and the palmar and dorsal carpometacarpal ligaments. (Shown in green in the figure.)
- Intermetacarpal ligaments connect the metacarpal bones: dorsal, interosseous, and palmo-metacarpal ligaments. (Shown in yellow in the picture.)
Movements
Main article: Anatomical conditions of movement § Special movements of the hands and feet
The hand is said to be in a straight position
when the third finger passes over the head bone and is in a straight line with the forearm.
This should not be confused with the average arm position
, which corresponds to 12 degrees of ulnar deviation. From the straight position, two pairs of arm movements are possible: abduction (movement towards the radius, the so-called radial deviation or abduction) 15 degrees and adduction (movement towards the ulna, the so-called ulnar deviation or adduction) 40 degrees, when the arm is in strict supination and slightly more in strict pronation.[9]Flexion (bending toward the palm, called palmar flexion) and extension (bending toward the back of the hand, called dorsiflexion) are possible over a total range of 170 degrees.[10]
Radial abduction/ulnar adduction
Remaining
: Ulnar adduction
Correct
: Radial abduction
Remaining
: Dorsiflexion
Correct
: Palmar flexion.
During radial abduction
the scaphoid is inclined toward the palmar side, allowing the trapezium and trapezium to approach the radius. Because the trapezius is rigidly attached to the second metacarpal bone, to which the flexor carpi radialis and extensor carpi radialis are also attached, radial abduction effectively pulls this combined structure toward the radius. In radial abduction, the pisiform crosses the longest path of all the carpal bones.[9]Radial abduction is produced by (in order of importance) extensor carpi radialis, abductor pollicis longus, extensor pollicis longus, flexor carpi radialis, and flexor pollicis longus.[11 ]
Ulnar adduction
causes tilting or dorsal displacement of the proximal row of carpal bones.[9]Produces extensor carpi ulnaris, flexor carpi ulnaris, extensor digitorum, and extensor digitorum minimus.[11]
Both radial abduction and ulnar adduction occur around a dorsopalmar axis passing through the head of the cephalic bone.[9]
Palmar flexion/dorsiflexion
During palmar flexion
The proximal carpal bones are displaced towards
the dorsal
side and towards
the palmar
side during
dorsiflexion
. While flexion and extension consist of movements around a pair of transverse axes—passing through the lunate for the proximal row and through the capitate for the distal row—volar flexion occurs primarily at the wrist joint and dorsiflexion at the middle carpal joint.[10]
Dorsiflexion is produced by (in order of importance) the extensor digitorum, extensor carpi radialis, extensor carpi radialis, extensor digitorum longus, extensor pollicis longus, and extensor digitorum minimalis muscles. Palmar flexion is produced by (in order of importance) flexor digitorum superficialis, flexor digitorum profundus, flexor carpi ulnaris, flexor pollicis longus, flexor carpi radialis, and abductor pollicis longus.[11]
Combined movements
In combination with movements in the elbow and shoulder joints, medium
or
wrist movements
Auxiliary movements
Anteroposterior gliding motion between adjacent carpal bones or along the midcarpal joint can be achieved by stabilizing one bone while moving another (i.e., pinching a bone between the thumb and index finger).[12]
Metacarpal fractures
The long, thin metacarpal bones are often broken by a punch or direct trauma. Muscle traction and movements in the hand until the fracture is immobilized often lead to displacement of bone fragments. There are epiphyseal fractures, when the fracture line is localized in the area of the bone heads, and diaphyseal fractures, when the fracture line is located in the bone body.
First metacarpal fracture
The cause is a blow with a bent first finger, less often a direct blow to the first metacarpal bone.
Fracture of the base of the first metacarpal bone . A typical injury for boxers and MMA fighters. A Bennett fracture is a separation of the base of the first metacarpal bone, which is held by ligaments, with simultaneous dislocation of most of it in the carpometacarpal joint. Rolando's fracture is a comminuted fracture-dislocation of the first metacarpal bone. Both injuries present with pain, deformation and swelling in the “anatomical snuffbox” area - the area under the base of the first finger - with increased pain when moving or trying to make a fist. Diagnosis is carried out taking into account complaints, trauma history, examination of the area of injury and x-ray of the hand. Bennett and Rolando fractures are treated surgically using osteosynthesis - restoring bone integrity by fixing fragments with metal knitting needles, pins or plates.
Fracture of the middle part of the first metacarpal bone . More often it occurs due to a direct blow to the bone. It manifests itself as pain, swelling and deformation in the area of the first metacarpal bone. The diagnosis is established taking into account the patient's complaints, information about the mechanism of injury, examination of the area of the first metacarpal bone and x-ray examination of the bones of the hand. Treatment is plaster immobilization for a period of 4-5 weeks; if the fragments are displaced, preliminary closed reposition is required. If conservative reduction is ineffective, an operation - pin osteosynthesis - is performed to compare the fragments.
An example of Dr. Valeev’s operation to restore after a fracture of the first metacarpal bone:
Before surgery:
After operation:
Fracture of II, III, IV, V metacarpal bones
The cause is a blow with a fist or a fall on fingers clenched into a fist. They can be single, but more often several metacarpal bones are broken, usually the fourth and fifth. It manifests itself as pain, swelling and deformation of the hand, and a hematoma often occurs. Diagnosed on the basis of complaints, history of injury, objective examination and X-ray results of the bones of the hand. To treat a non-displaced fracture, immobilization is performed for a period of 4-5 weeks. If fragments are displaced, closed reduction is indicated, and if it is ineffective, skeletal traction or pin osteosynthesis is indicated.
Other animals
See also: Carpus and tarsus of terrestrial vertebrates
The structure of the carpus varies greatly among different groups of tetrapods, even among those that retain a full set of five digits. In primitive fossil amphibians such as Eryops
the wrist consists of three rows of bones;
a proximal row of three carpals, a second row of four bones, and a distal row of five bones. The proximal carpal bones are called the radius
,
ponticus
, and
ulna
, after their proximal articulations, and are homologous with the scaphoid, lunate, and triquetrum bones, respectively.
The rest of the dice are simply numbered, from one to four. centralia
(singular:
central
), and the first to fifth
distal carpals
. Initially, each of the distal bones appears to articulate with one metacarpal bone.
However, the vast majority of later vertebrates, including modern amphibians, underwent varying degrees of loss and fusion of these primitive bones, resulting in a decrease in the number of carpal bones. Almost all mammals and reptiles, for example, have lost the fifth distal carpus and have only one central part - and even this is missing in humans. The pisiform bone is somewhat unusual, as it first appears in primitive reptiles and is never found in amphibians.
Since many tetrapods have fewer than five digits on their forelimbs, even large degrees of fusion are common, and a huge number of different possible combinations are found. The wing of a modern bird, for example, has only two wrists left; the radiate (scaphoid in mammals) and the bone formed by the fusion of the four distal parts of the carpus.[13]
Both the carpals and tarsals are described as podial elements or (clusters of) podial bones.[14]
In some, the macropods, scaphoid and lunate are fused to the scaphoid.[15]
In crustaceans, "carpal" is the scientific term for the claws or "claws" on some legs. (See Anatomy of decapods)
Structure of the wrist bones
The hand performs a large number of tasks.
This is achieved due to the peculiarities of its structure. Bones and joints form a unique motor system. This article will examine in detail the issue of the structure of the carpal bones. The hand is a complex set of joints, which is a distant structural link of the upper limb girdle.
Articular wrist complex
The grasping abilities of the hand directly depend on the wrist joint complex. The ideal position of the hand is ensured thanks to the well-coordinated cooperation of the two joints that make up the wrist complex:
- wrist;
- midcarpal.
The spatial orientation of the hand is provided by the auxiliary abilities of the distal epiphyses of the forearm. The inferior radioulnar joint unites the ends of the ulna and radius bones. Although it does not belong to the hand, it plays an important role in its functioning, namely, it ensures its rotation. This strikingly distinguishes the human hand from the skeletal formations of animals.
Brief description of the wrist joint
The wrist joint looks like an ellipse. Its anatomical features are as follows:
- The lower epiphysis of the wrist joint (from the side of the forearm) is formed from the radius.
- The wrist joint is formed from the three bones of the nearest row on the side of the wrist. These are the lunate, scaphoid and triquetral bones.
- The three bones are covered with a hyaline plate, resulting in a solid articular surface.
Characteristics of the midcarpal joint
This is an atypical joint, which is located between two rows of carpal bones, forming a solid plane. Movement of the joint is possible due to the characteristics of the lunate bone. Its significance is compared to the axis around which movement is carried out, which has a limited scope. The stability of these processes is achieved thanks to the work of the ligamentous apparatus.
Interestingly, the strength of the ligaments is very high. If damaged, it is more likely that one of the small carpal bones will dislocate or, in extreme cases, break, than the ligaments will tear.
Imagine the structure of the wrist with its small bones, like a bag filled with small stones. Thus, it is easier to understand the nature of movements and interosseous interaction, possible thanks to the work of ligaments that guarantee the stable functioning of this connection.
All joints that make up the wrist take part in every movement. Flexion of the hand by 50º is possible due to the work of the wrist joint. 35º flexion is provided by the midcarpal joint. In turn, extension of the hand by 50º is achieved thanks to the mid-carpal joint, and by 35º – by the wrist.
Physiological and anatomical characteristics of the hand
Modification of the shape of the hand is the main condition for performing the grasping function. Therefore, in order to grasp an object and hold it, the hand must form a concavity or flatten when resting on a flat surface. Thanks to this, 3 arches are formed, which are located in different planes:
- Due to the concavity of the wrist, a transverse arch is formed.
- An inclined arch is formed due to the opposition of the thumb to the other fingers. This movement creates a palmar depression.
- The longitudinal arch is formed by the carpal bones, which arise from the metacarpophalangeal joints.
The joints of the wrist and metacarpus contribute to the development of the arch of the palm. They are connected by a ligamentous apparatus, and are also highly mobile and consist of the distal carpal joints and the proximal metacarpal bones. On the side of the wrist, the trapezoid bone is associated with the first and second metacarpal bones. The first trapezio-metacarpal joint provides the thumb with a counterpoint to its fellows. This joint differs from the others in its saddle-shaped shape. The main difference between the joint is that it has greater freedom and range of movement, which is possible due to the fact that the capsule is not stretched. There is also a drawback: such freedom leads to the fact that dislocation of the thumb occurs more often than in others.
The conjugation of the metacarpophalangeal joints ensures the flexion and extension of the fingers with a considerable range. The joints are saddle-shaped. The head of the metacarpal bone is biconvex, and the base of the first phalanx is biconvex, but the area of the base of the phalanx is less than that of the metacarpal bone.
It is noteworthy that if the planes of the joints were more equal, then the likelihood of their displacement relative to each other would decrease. Moreover, such a situation would significantly worsen the dexterity of the hand, which, of course, is unacceptable.
The metacarpophalangeal joint allows for a wide range of movement. Interestingly, the muscles and tendons of the fingers turn them into circular ones. The index finger has the greatest ability to move to the right and left.
Brief description of interphalangeal joints
Interphalangeal joints allow human hands to hold tools. The activity of the joints is supported by the thumb. His task is to press the object into the palm of his hand and hold it. The interphalangeal joints resemble balls in appearance, which allows the fingers to bend/extend.
There is a block-like concavity in the middle of the base of the phalanx. The head of the next phalanx has two small projections that are covered with hyaline cartilage. In the middle of the phalanx head is the central ridge. A distinctive characteristic of the joint is that the range of flexion exceeds 90º. However, the ligaments of the phalanges and interphalangeal joints prevent the joint from bending as much.
The structure of the bones of the wrist improves the grasping capabilities of the palm. No living creature can perform such complex manipulations with a brush that are accessible to humans.
Notes
- ^ a b
Kingston 2000, pp. 126-127 - ^ a b
Platzer 2004, p.124. - ^ a b
Schmidt-Lanz 2003, p.29. - ^ a b Thieme Atlas of Anatomy
2006, p.224. - ^ a b
Platzer 2004, p. 126 - ^ a b c
Schmidt, Hans-Martin;
Lanz, Ulrich (2003). Surgical anatomy of the hand
. Time. clause 7. ISBN 1-58890-007-X. - ^ a b c
Balachandran, Ajay;
Map, Moumita; Krishna, Anuj; Thomas, Jerry; K, Pratilash; TN, Prem; G.K., Libu; B, Krishnan; John, Lisa (2014). "Study of ossification of the cephalon, hamata, triquetral and lunate in forensic assessment." Indian Journal of Forensic Medicine and Toxicology
.
8
(2): 218–224. Doi:10.5958/0973-9130.2014.00720.8. ISSN 0973-9130. Retrieved August 18, 2014. - Platzer 2004, p.130.
- ^ a b c d
Platzer 2004, page 132 - ^ a b c
Platzer 2004, page 134 - ^ a b c
Platzer 2004, page 172 - Palastanga 2006, p.184
- Romer, Alfred Sherwood; Parsons, Thomas S. (1977). Vertebrate body
. Philadelphia, PA: Holt-Saunders International. pp. 200–202. ISBN 0-03-910284-X. - Galateanu, Gabriela; Hildebrandt, Thomas B.; Mayo, Alexis; Etienne, Pascal; Pothier, Romain; Mulot, Baptiste; Saragasti, Joseph; Hermes, Robert (2013-07-09). “One small step for rhinos, one giant leap for wildlife management—imaging diagnosis of bone pathology in distal limbs.” PLOS ONE
.
8
(7):e68493. Doi:10.1371/journal.pone.0068493. ISSN 1932-6203. PMC 3706412. PMID 23874643. - Swamp wallaby ( Wallabia bicolor
) wrists Archived 2007-09-30 on the Wayback Machine - Diab 1999, page 48
References
- Diab, Mohammad (1999). Lexicon of Orthopedic Etymology
. Taylor and Francis. ISBN 90-5702-597-3. - Kingston, Bernard (2000). What Are Joints: A Practical Guide to Their Structure and Function
. Nelson Thorns. ISBN 0-7487-5399-0. - Palastanga, Nigel; Field, Derek; Soames, Roger (2006). Human Anatomy and Movement: Structure and Function
. Elsevier Health Sciences. ISBN 0-7506-8814-9. - Platzer, Werner (2004). Color Atlas of Human Anatomy, Vol.
1: musculoskeletal system (5th ed.). Time. ISBN 3-13-533305-1. - Schmidt, Hans-Martin; Lanz, Ulrich (2003). Surgical anatomy of the hand
. Time. ISBN 1-58890-007-X. - Thieme's Atlas of Anatomy: General Anatomy and the Musculoskeletal System
. Time. 2006 ISBN 1-58890-419-9.