ATTENTION – TICK-BORNE ENCEPHALITIS
Tick-borne encephalitis is an acute viral disease of the nervous system. Its main sources are two types of ixodid ticks - taiga and European forest ticks. The peak incidence of encephalitis occurs in spring (May-June) and late summer and early autumn (August-September).
Ticks are very fond of mixed forests with dense undergrowth, bushes, and tall grass. Prefer damp places. But they don’t like direct sunlight and dry air. In extreme heat or during heavy rain, these parasites are inactive and almost do not attack. The disease can lead to persistent neurological and psychiatric complications and even death of the patient.
Causes
Tick-borne encephalitis is sometimes called differently - spring-summer, taiga, Siberian, Russian. Synonyms arose due to the characteristics of the disease. Spring-summer, because the peak incidence occurs in the warm season, when ticks are most active. The first peak of the disease is recorded in May-June, the second - at the end of summer.
If you are bitten by an encephalitis tick, the virus enters the bloodstream within the first minutes of contact. According to statistics, six ticks out of a hundred are carriers of the virus (at the same time, from 2 to 6% of people bitten can get sick from an infected individual).
The causative agent of tick-borne encephalitis is an RNA virus belonging to the Vlaviviridae family. There are 3 types of virus:
- Far Eastern - the most virulent (can cause severe forms of the disease);
- Siberian - less contagious;
- Western - the causative agent of two-wave encephalitis - causes mild forms of the disease.
The bite of an ixodid tick is the main cause of encephalitis. Due to damage to the body by a natural focal viral infection, which is dangerous for the membranes of the brain and spinal cord, meningitis and meningoencephalitis occur.
There are known cases of human infection with tick-borne encephalitis after consuming milk from tick-infected domestic animals. Therefore, you can only drink pasteurized or boiled milk.
Features of the tick-borne encephalitis virus are its poor resistance to high temperatures, disinfectants and ultraviolet radiation. Thus, when boiled, it dies within 2 minutes and cannot be preserved in the environment in hot sunny weather. However, at low temperatures it is able to maintain viability for a long time.
What should I do if bitten by a tick
If you nevertheless find a parasite on your body or on your loved ones, you need to quickly and carefully remove it before it penetrates deep under the skin. Remember that you can cause blood poisoning even if you crush a tick. Therefore, you need to pull it out very carefully and preferably not with your bare hands.
Do not use gasoline, nail polish or other toxic chemicals. Take a strong and long thread, carefully tie a loop, capturing the body of the insect. Using gentle rotational movements, pull out the tick. The removed parasite must be placed in a glass container with a tight lid and taken to the laboratory for research.
Another way is to use tweezers with flat edges. They need to grab the bloodsucker at the very base, and also pull the parasite out of the skin with rotational movements. Then the wound needs to be disinfected.
The live encephalitis tick, which you placed in a glass container, must be taken to the laboratory for diagnosis. If the tick could not be kept alive, you need to donate blood to detect immunoglobulins for infections.
Incubation period
During a tick bite, some viruses begin to multiply in the subcutaneous tissue and tissue macrophages, while another part enters the blood and penetrates the vascular endothelium, lymph nodes, parenchymal organs, and into the tissue of the central nervous system, where they intensively multiply and accumulate. Treatment of tick-borne encephalitis is carried out using many groups of drugs that affect the virus itself and all parts of the pathological process.
Traditionally, the incubation period of infection lasts from 7 to 20 days after the bite of an infected parasite, if infection occurred through milk - 3-7 days.
Sometimes fulminant forms of tick-borne encephalitis are diagnosed (the first symptoms appear within a day) and protracted forms - the incubation period can include up to 30 days.
You should know that a patient with tick-borne encephalitis is not dangerous to others, as it is not contagious.
On average, the incubation period is 1-3 weeks, since the forms of development of the disease are different:
- Lightning fast. With it, the initial symptoms appear already on the first day.
- Lingering. In this case, the duration of the incubation period can be about a month, sometimes even a little longer.
Types of disease
Doctors distinguish three main forms of tick-borne encephalitis:
- febrile;
- meningeal;
- focal.
The first accounts for up to 50% of all clinically diagnosed cases. This type of encephalitis is characterized by systematic attacks of fever. The meningeal form develops when the virus infects the membranes of the patient’s spinal cord and brain. Its share in the total number of cases detected by doctors is 30%. Focal encephalitis is diagnosed in every fifth patient exposed to the flavivirus. The inflammatory process affects the gray matter of the brain and is accompanied by increasing neurological symptoms.
Symptoms of tick-borne encephalitis
Tick-borne encephalitis is a viral infection that initially occurs under the guise of a common cold. It may go unnoticed by the patient, or may cause severe damage to the nervous system.
After a tick bite, the virus multiplies in tissues and penetrates the lymph nodes and blood. When the virus multiplies and enters the bloodstream, flu-like symptoms form.
Often the disease begins with the following symptoms:
- an increase in body temperature to 39-40 C and with chills characteristic of this condition,
- severe pain in the lower back and limbs,
- pain in the eyeballs,
- general weakness
- nausea and vomiting,
- consciousness is preserved, but there is lethargy, drowsiness, and symptoms of stupor.
When the virus enters the membranes of the brain, and then into the substance of the brain, symptoms of disturbances in its activity appear (neurological):
- sensation of goose bumps, touches on the skin;
- skin sensitivity disorders;
- disturbances in muscle movements (first facial movements, then the ability to voluntarily make movements of the arms and legs is lost);
- convulsions are possible.
Violations may occur later:
- cardiovascular system (myocarditis, cardiovascular failure, arrhythmia),
- digestive system - stool retention, enlarged liver and spleen.
All of these symptoms are observed against the background of toxic damage to the body - an increase in body temperature to 39-40 degrees C.
The most common and noticeable signs of an encephalitis tick bite:
- transient weakness of the limbs;
- weakness of the muscle tissue of the cervical region;
- feeling of numbness of the facial and cervical skin.
Further, the severity of the disease will depend on the form of tick-borne encephalitis itself.
| Phases of the disease | Description |
| First | Latent – the virus accumulates in the human body (there are no symptoms, this is an incubation period that lasts on average 7-12 days, but can vary from 1 to 30 days); |
| Second | The virus enters the blood - viremia - and is introduced into the central nervous system (the patient has an infectious-toxic syndrome) |
| Third | neural (the patient has all the symptoms of damage to the nervous system) |
| Fourth | A person develops immunity and, as a rule, recovers. But, there are cases when the virus does not leave a person and then a chronic form sets in, the disease either subsides, or after a while it becomes active again. |
The outcome of tick-borne encephalitis comes in three main options:
- recovery with gradual long-term recovery;
- transition of the disease to a chronic form;
- death of a person infected with tick-borne encephalitis.
After a tick bite infected with the encephalitis virus, it is necessary to carry out emergency prevention for 3 days.
Lyme disease: features of tick-borne borreliosis
Lyme disease (tick-borne systemic borreliosis, Lyme borreliosis) is a transmissible, natural focal disease characterized by damage to the skin, joints, nervous system, heart, often taking a chronic, relapsing course. Among infectious diseases transmitted by ticks, Lyme disease (LD) is the most common.
The name of the disease comes from the name of the small town of Old Lyme in Connecticut (USA), where in the mid-1970s a number of cases of arthritis after tick bites were described. In Europe, Borrelia infection had already been known for a long time under various names (erythema migrans, Bannwart syndrome), but the pathogen was isolated only in 1982.
• Causative agents of Lyme disease
The causative agents are several species of Borrelia pathogenic to humans - Borrelia burgdorferi, Borrelia garinii and Borrelia afzelii. Borrelia are microaerophiles and, like other gram-negative spirochetes, are extremely demanding on cultivation conditions.
Infections caused by Borrelia burgdorferi most often present with arthritis (especially in North America, where it is the only causative agent of borreliosis), while B. garinii is more likely to cause neurological disorders and B. afzelii is more likely to cause chronic skin diseases. All three pathogens cause erythema migrans.
• Epidemiology of tick-borne borreliosis
The natural hosts of Borrelia in nature are wild animals (rodents, birds, deer), which feed ticks of the genus Ixodes - carriers of Borrelia. During blood sucking, borrelia enter the tick's intestines, where they multiply and are excreted in feces. Despite the high level of infection of ticks, the possibility of infection through a bite is not always realized, because borrelia are contained in the salivary glands in small quantities or are absent altogether.
In natural foci, the circulation of the pathogen occurs as follows: ticks → wild animals → ticks. It is possible that domestic animals – goats, sheep, cows – may be involved in the epidemiological chain. The likelihood of other carriers of Borrelia, such as horse flies, is being studied.
A person becomes infected with Lyme disease in natural foci. Natural foci of Lyme disease are found mainly in forest landscapes of the temperate climate zone. In recent years, it has been established that the area of distribution of tick-borne borreliosis coincides with tick-borne encephalitis, and the disease is registered throughout the Russian Federation.
However, the incidence of Lyme disease is 2–4 times higher than tick-borne encephalitis, and it occupies one of the first places among natural focal zoonoses.
Tick-borne borreliosis is widespread in Europe, Asia, and America. In Russia, borreliosis is widespread in the forest and forest-steppe zones from Kaliningrad to Sakhalin. In European Russia, borreliosis is the most common tick-borne infection.
The risk of getting borreliosis after a tick bite is much higher than tick-borne encephalitis. Natural foci of tick-borne borreliosis coincide with the range of ixodid ticks. The incidence of borreliosis is always seasonal and coincides with the activity of ticks. The first patients with tick bites are usually registered in March-April. The latter, in the presence of warm weather, are recorded even in October. Peak activity occurs in May-June. The percentage of ticks infected with borreliosis differs in different regions.
A tick can simultaneously be infected with Borrelia, tick-borne encephalitis virus and other pathogens. Therefore, the development of a mixed infection is possible.
Transmission of the infection occurs transmissibly through a tick bite (inoculation), although the possibility of infection cannot be ruled out when tick feces come into contact with the skin, followed by rubbing them in when scratching (contamination). If the tick ruptures, if removed incorrectly, the pathogen may enter the wound. The nutritional route of infection through consumption of raw goat or cow milk is also discussed. The main risk groups are workers of forestry farms, timber industry enterprises, hunters, foresters and residents of forested areas.
Carriers of Borrelia are ticks of the genus Ixodes , in our country and Europe - I. ricinus and I. persulcatus, in America - I. pacificus and I. scapularis. The life cycle of these ticks (larva → nymph → adult) lasts an average of three years. Ticks become infected from numerous rodents, as well as hares, hedgehogs, birds, etc. Ticks live in grasses, ferns and low shrubs.
• Pathogenesis of Lyme disease
Clinical symptoms that appear at different stages of the disease are caused by a combination of immunopathological reactions and the presence of the pathogen and its antigens in the tissues. Penetrating into the human body, borrelia at the site of introduction cause the formation of a primary affect - papules, tick-borne erythema, then hematogenously enter various organs and tissues, where they are adsorbed on cells, interacting most actively with galactocerebrosides of neuroglial membranes.
Perivascular infiltrates appear, consisting of lymphocytes, macrophages, plasma cells, and diffuse infiltration of damaged tissues by these elements. Borrelia and the resulting immune complexes lead to the development of vasculitis and vascular occlusion.
Borrelia are capable of persisting in tissues for a long time, up to several years, especially in the absence of treatment, which is associated with a chronic relapsing course of the disease.
In the later stages of the disease, borrelia, playing the role of a trigger, provoke the development of immunopathological processes that are of great importance for the pathogenesis of neuroborreliosis and chronic arthritis. Among this kind of patients, the most common are those with the HLA-DR2 and HLA-DR4 genotypes. Already in the early stages of the disease, specific antibodies are produced, the titer of which increases over the course of the disease.
The immune response is most pronounced in the later stages, especially when joints are affected. With effective therapy and recovery, antibody levels normalize. Their long-term persistence or appearance in high titers in later stages indicates the persistence of the pathogen even in the absence of clinical manifestations.
• Borreliosis infection
The incubation period ranges from 2 to 30 days, with an average of 14 days. The infection may be asymptomatic, but may also have a different clinical picture of the disease. The infection is divided into three stages, but in principle these are different clinical pictures of the disease.
The division of the disease into stages is arbitrary, and clinical manifestations of all stages of the disease in one patient are not necessary. In some cases, the first stage may be absent, in others - the second or third.
Sometimes the disease manifests itself only in the chronic stage, so the general practitioner should remember that patients with arthritis, polyneuropathy, encephalomyelitis and other syndromes characteristic of Lyme disease must be examined to exclude borreliosis.
• Diagnosis of Lyme disease
Early diagnosis is based on clinical and epidemiological data. With the classic picture of erythema migrans, the diagnosis is made based on clinical signs; the diagnosis is registered even in the absence of laboratory confirmation and data on a tick bite. In other cases, the diagnosis is confirmed by laboratory methods.
Culture, detection of pathogen antigen and histological examination of the skin are not sensitive and specific enough; histological examination is, in addition, invasive. Therefore, the diagnosis is confirmed mainly by serological methods - the detection of specific antibodies to the pathogen in the blood.
Borreliosis can occur without symptoms, and an acute infectious process can be confirmed or refuted using a blood test for antibodies (IgM).
PCR testing for the presence of genetic material of the pathogen is ineffective in this case. IgG antibodies can be detected 1-3 weeks after infection; the maximum amount of IgG antibodies is synthesized 1.5-3 months after infection. IgG antibodies are often not detected in the early, localized stage of the disease or with early antimicrobial therapy. IgG antibodies circulate in the blood for a long period of time (from several months to several years), even after successful antimicrobial therapy and cure of the infection.
Immunity against Borrelia is not sterile. People who have been ill may become infected again after a few years.
False-positive results of determining IgG antibodies to Borrelia may be due to the presence in the blood of specific antibodies for diseases caused by spirochetes (syphilis, relapsing fever); a low level of IgG antibodies is possible in infectious mononucleosis, hepatitis B, rheumatic diseases (SLE), periodontal diseases, in 5-15% of healthy individuals from the epidemic zone.
• Clinical picture of Lyme disease
The spring-summer period is considered a favorable time for the development of the disease. The disease occurs in 3 stages
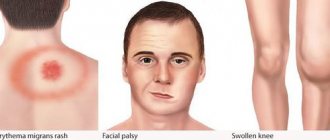
- Stage I begins a week after the tick bite and lasts from 3 days to a month. The main symptoms are fever, fatigue, chills, headaches and erythema migrans (a ring-shaped redness of the skin that gradually widens). Initiating therapy at this stage helps prevent further development of the disease;
- Stage II occurs 4 weeks after the bite. It is characterized by cardiac damage and a neurological “triad”: aseptic meningitis, facial paralysis and peripheral neuropathies;
- Stage III begins after 6 weeks, and in some cases, after several years. If the disease is not treated, severe joint damage develops at this stage.
When classic symptoms of erythema migrans appear, the diagnosis is made based on clinical signs, in other cases it is confirmed by laboratory methods. Antibodies to Borrelia burgdorferi
IgG immunoglobulins to Borrelia burgdorferi are synthesized in the blood within 1–3 weeks, reaching their maximum 1.5–3 months after infection. Very often, antibodies to Borrelia burgdorferi are not detected at an early stage of the disease or with early antimicrobial therapy.
• Treatment of Lyme disease
Patients with moderate Lyme disease are subject to mandatory hospitalization in an infectious diseases hospital at all stages of the disease. Patients with a mild course of the disease (tick-borne erythema, in the absence of fever and intoxication) can be treated at home.
Antibiotics are used as etiotropic drugs, the choice of which, dose and duration of use depend on the stage of the disease, the prevailing clinical syndrome and severity. All those bitten by ticks and who have recovered from Lyme disease are subject to clinical observation for 2 years.
Clinical examination is carried out by an infectious disease specialist or a general practitioner. Patients and persons after a tick bite should be examined clinically and serologically after 3, 6, 12 months and 2 years. According to indications, consultations with a cardiologist, rheumatologist, neurologist are prescribed, an ECG test is performed, a blood test for CRP, rheumatoid factor.
Pregnant women bitten by ticks deserve special attention.
Due to the lack of specific prophylaxis and the known teratogenic effect of Borrelia in the early stages of pregnancy, it is advisable to decide on an individual basis for maintaining pregnancy.
If late manifestations of borreliosis occur, patients are treated in specialized hospitals (rheumatology, neurology, cardiology) according to clinical indications. Convalescents of borreliosis with residual effects are observed by specialists, depending on the damage to one or another system (neurologist, cardiologist, rheumatologist).
• Prevention of Lyme disease
— There is no prophylactic vaccine to prevent borreliosis! — The best prevention is protection against tick bites!
Prevention consists of observing individual protection measures against tick attacks and raising awareness among the general public. Proper tick removal is of great importance for preventing infection.
If the tick has attached itself, it needs to be removed quickly. Borrelia live in the intestines of the tick and do not immediately enter the bloodstream. The longer the tick was on the body, the higher the risk of borreliosis.
Symptoms of Lyme disease can be mistaken for COVID-19, with serious consequences.
Lyme disease shares a number of symptoms with COVID-19, including fever, pain and chills. Anyone who mistakes Lyme disease for COVID-19 may unknowingly delay needed treatment, which can have serious consequences!
Close-up of a tick's head under an electron microscope. Fernando Otalora-Luna / University of Richmond, CC BY
Awareness is a key component of tick-borne disease prevention and treatment!
Read more.
©Source: CITYLAB
We recommend reading a scientific article →
“Epidemiology, etiology, clinical picture, diagnosis, treatment and prevention of ixodid tick-borne borreliosis”
Authors: Yu.V. Lobzin, A.G. Rakhmanova, V.S. Antonov, A.N. Uskov, L.P. Antykova, N.V. Skripchenko, G.P. Ivanova, O.V. Platoshina Edition: Recommendations for doctors Year: 2000
Abstract: In terms of the level of incidence and severity of the clinical course, ixodic tick-borne borreliosis is one of the pressing problems of modern infectious pathology. The purpose of these guidelines is to contribute to the improvement and improvement of the prevention, diagnosis and treatment of ixodid tick-borne borreliosis.
Key words: Lyme borreliosis treatment, tick-borne encephalitis treatment, immunomodulator, lycopid, damage to the nervous system, prevention of ixodid tick-borne borreliosis, tick-borne encephalitis symptoms in adults
“When the nervous system is damaged, pathogenetic therapy is of great importance: to improve microcirculation in tissues and accelerate remyelination processes - vascular agents (trental, instenon, cavinton), antioxidants (vitamin E, C, solcoseryl, actovegin), as well as drugs that stimulate metabolic processes in nervous tissue (nootropics, B vitamins), non-steroidal anti-inflammatory drugs (indomethacin, piroxicam), analgesics (paracetamol, tramal), drugs that improve neuromuscular conduction (prozerin, oxazil, ubretide), immunomodulator Lykopid®, in case of severe damage to the central nervous system — short course corticosteroids, plasmapheresis, HBOT, symptomatic medications, exercise therapy, massage, physiotherapy at various stages of the disease.”
Forms of tick-borne encephalitis
Currently, the following forms of the disease are distinguished:
Febrile form of tick-borne encephalitis
Tick-borne encephalitis in this form occurs with a predominance of a febrile state, which can last from 2 to 10 days. The most typical manifestations include headache, weakness and nausea. In this case, neurological symptoms are mild.
Meningeal
Meningeal, which proceeds relatively favorably. It begins, like any other manifestation, with the phenomena of intoxication of the body:
- weakness,
- increase in body temperature,
- sweating
Then symptoms of brain damage appear (occipital headaches, vomiting, fear of light and impaired reflexes). Within two to three weeks, typical symptoms of meningitis appear.
Meningoencephalitic
Meningoencephalitis is characterized by a two-wave temperature reaction. Each wave lasts from 2 to 7 days. At intervals of 1-2 weeks. The first wave occurs with general toxic symptoms, and the second with meningeal and cerebral signs. The course of this form is favorable, rapid recovery and absence of complications are observed.
Poliomyelitis form
It is observed in 30% of patients. It begins with general lethargy of the whole body, observed within 1-2 days. Accompanied by the following symptoms:
- weakness in the limbs, which can subsequently lead to numbness;
- characterized by pain in the neck;
- all violations described in the previous forms are possible;
- the ability to hold the head in an upright position disappears;
- loss of movement in the hands.
Motor pathologies progress over 1-1.5 weeks. From the beginning of the second to the end of the third week, the muscles begin to atrophy.
Polyradiculoneuritic form
It is observed rarely, in no more than 4% of cases. In addition to the symptoms of meningitis, with the development of this variant of tick-borne encephalitis, severe paresthesia (tingling) in the extremities and severe sensitivity in the area of the fingers appear. Sensitivity in the central parts of the body is impaired.
As you can see, the signs of this disease can be completely different. Some forms of encephalitis are quite difficult to diagnose. That is why it is extremely important to consult a doctor in time, preferably before the appearance of disorders of the nervous system.
What to do if you are bitten by a tick and how to prevent viral encephalitis. Expanded instructions
We recently published a major piece on the current tick season and the diseases they carry. In connection with updated information about the foci of tick-borne viral encephalitis (TBE) in Moscow, Mednovosti provides detailed instructions on what to do if you are bitten by a tick.
According to the April report of the Research Institute of Epidemiology of Rospotrebnadzor, which is cited by Izvestia, a cluster of TVE was discovered in the city of Moscow. Epidemiologists refer to data from last year’s studies that discovered ticks and mammals infected with TVE in the Krylatsky Forest Park. In 2021, one victim, bitten by an encephalitis tick, contacted the research institute; another person ended up in the hospital a year earlier. Experts point out that these were the first cases of detection of the virus in the city. They warn residents of the capital that the situation could repeat itself this year.
It was previously reported that last year 13,332 people (2,699 of them children) visited medical institutions in the capital alone due to tick bites. This year, in 70 constituent entities of the federation, about four thousand victims, including 1,591 children, contacted medical organizations, which is below average.
Here are recommendations on what to do if you find a tick on yourself, taken from the leaflet “Beware of Ticks,” compiled by the chief freelance specialist in infectious diseases of the Ministry of Health of the Russian Federation, Professor I.V. Shestakova.
Removing the tick
Contact the specialists
If tick suction does occur, an initial consultation can always be obtained by calling a landline number: 103, or from a mobile (cell) phone: 103* or 112.
A person who has suffered from a tick bite must seek medical help from the territorial clinic at his place of residence, the regional SES or the regional emergency room to remove the tick and deliver it for examination, as well as to organize medical observation, in order to make a timely diagnosis of tick-borne infection and resolve the question of prescribing preventive treatment.
If for some reason you do not have the opportunity to seek help from a medical institution, then you will have to remove the tick yourself, and the sooner you remove the embedded parasite, the better.
Removing ticks yourself There are several ways to remove ticks. They differ only in the tool used to remove the tick. It is most convenient to remove a tick with curved tweezers or a surgical clamp; in principle, any other tweezers will do. In this case, the tick must be grabbed as close to the proboscis as possible, then it is carefully pulled up, while rotating around its axis in a convenient direction. Usually, after 1-3 turns, the entire tick is removed along with the proboscis. If you try to pull the tick out, there is a high probability of it breaking.
If you have neither tweezers nor special devices for removing ticks at hand, then the tick can be removed using a thread. A strong thread is tied into a knot as close as possible to the tick's proboscis, then the tick is removed, slowly shaking it to the sides and pulling it up. Sudden movements are not allowed.
If you don’t have tweezers or thread at hand, you should grab the tick with your fingers (it’s better to wrap your fingers in a clean bandage) as close to the skin as possible. Pull the tick slightly and rotate it around its axis. There is no need to crush the tick with your hands. After removing a tick, be sure to wash your hands. The wound must be treated at home with an antiseptic.
Removing a tick must be done with care, without squeezing its body, since this may squeeze the contents of the tick along with pathogens into the wound. It is important not to tear the tick when removing it - the remaining part in the skin can cause inflammation and suppuration. It is worth considering that when the head of the tick is torn off, the infection process can continue, since a significant concentration of the tick-borne encephalitis virus is present in the salivary glands and ducts.
If, when removing the tick, its head, which looks like a black dot, comes off, wipe the suction site with cotton wool or a bandage moistened with alcohol, and then remove the head with a sterile needle (previously calcined in a fire) in the same way as you remove an ordinary splinter.
After removing the tick After removing the tick, the skin at the site of its attachment is treated with tincture of iodine or alcohol, or another available skin antiseptic. A bandage is usually not required. Subsequently, the wound is treated with iodine until healing. There is no need to pour in a lot of iodine, as it can burn the skin. If everything is normal, the wound will heal within a week. Hands and tools should be thoroughly washed after removing the tick.
When removing a tick you do not need to:
- apply caustic liquids (ammonia, gasoline, etc.) to the bite site;
- burn a tick with a cigarette; - jerk the tick sharply - it will break off;
- picking at the wound with a dirty needle;
- apply various compresses to the bite site;
- crush the tick with your fingers.
There is no basis for some far-fetched advice that for better removal one should apply ointment dressings to the attached tick or use oil solutions. The oil can clog the tick's breathing holes, and the tick will die while remaining in the skin. Dripping oil, kerosene onto a tick, or burning the tick is pointless and dangerous. The tick's respiratory organs will become clogged, and the tick will regurgitate the contents, increasing the risk of infection.
We send the removed tick for examination
If research is not possible, the tick should be burned or doused with boiling water. The removed tick should be placed in a small hermetically sealed container with a small piece of slightly damp cotton wool or a napkin and sent to the laboratory. The jar with the tick is placed in the refrigerator if it is impossible to transport it to the laboratory immediately after removing the tick. Within two days, the tick must be taken to the laboratory to be tested for tick-borne infections. Usually the analysis can be done in a regional infectious diseases hospital or a special laboratory.
Laboratory addresses
For Moscow residents:
- in the department of especially dangerous infections of the microbiological laboratory of the Federal State Institution "Center for Hygiene and Epidemiology in Moscow" at the address: Moscow, Grafsky lane, 4/9 (entrance from the courtyard, 2nd floor), tel.. Reception is held from 9-00 until 15-30 daily, except Saturday, Sunday and holidays (lunch break from 13-00 to 13-30), the results of research can be found out from 15-00 to 18-00;
- branch of the Federal State Institution "Center for Hygiene and Epidemiology in Moscow" at the address Moscow, Krasnogvardeisky Boulevard, 17 building 1 microbiological laboratory, reception from 9.30 to 15.00 daily, except Saturday and Sunday, tel.;
- Federal Budgetary Institution of Health "Federal Center for Hygiene and Epidemiology of Rospotrebnadzor" in Moscow at the address Varshavskoye Highway 19a (Nagatinskaya metro station) Mon-Fri from 9.00-18.00 tel. +7(495)954-45-36.
Residents of the Moscow region can receive specialized assistance at their place of residence in the Central District Hospital or at the above addresses.
What should a person bitten by an infected tick understand?
It is impossible to judge by the appearance of a tick whether it is a carrier of infection or not. The tick becomes infected when feeding on an infected animal. The virus can be contained in females, males, nymphs, and larvae. Even if the tick bite was short-lived, the risk of contracting tick-borne infections cannot be ruled out.
However, it should be understood that the presence of an infection in a tick does not mean that a person will get sick. A tick analysis is needed for peace of mind in case of a negative result and vigilance in case of a positive result.
It is advisable that a person who has suffered from a tick bite be observed by an infectious disease specialist for a month, who, if necessary, will prescribe the necessary preventive or treatment measures. If more than 2 months have passed since the tick bite, there is no need to worry.
There is no need to self-medicate; if in doubt, consult a doctor! If a tick bite has occurred, if your health worsens, consult a doctor immediately!
We carry out specific prevention (only tick-borne viral encephalitis)
Emergency prevention of tick-borne borreliosis, human monocytic ehrlichiosis and human granulocytic anaplasmosis is usually not carried out.
Tick-borne viral encephalitis is a very dangerous tick-borne infection. Emergency prevention of tick-borne encephalitis should be carried out as early as possible, preferably on the first day. It is carried out using antiviral drugs or immunoglobulin (when virus ticks are sucked on by people who have not been sick or previously vaccinated, as well as those who have an incomplete or defective vaccine course in the first 96 hours after sucking, intramuscularly, once). A doctor carries out preventive measures.
When an encephalitis tick bites, the virus enters the bloodstream with saliva. In the future, events may develop differently. If the bitten person has been vaccinated and the level of antibodies is sufficient, the virus immediately binds and the disease does not develop. The development of tick-borne viral encephalitis can be stopped by other factors of antiviral protection. Therefore, even if the tick was encephalitic, the person bitten may not get sick. The presence of a virus in a tick does not mean that the disease will develop. The number of people bitten by encephalitis ticks significantly exceeds the number of people sick with tick-borne encephalitis. But even one bite can lead to serious illness.
Where to go for emergency prevention against tick-borne encephalitis in Moscow
For adults:
- Infectious Clinical Hospital No. 2 of the Moscow Department of Health, Moscow, 8th st. Sokolinaya Gora, 15. Help service.
- City advisory office on vaccine-serum prevention of tick-borne viral encephalitis: tel., (www.mosgorzdrav.ru/ikb2)
For children:
- Children's City Clinical Hospital No. 13 named after. N.F.Filatova, Moscow, st. Sadovaya Kudrinskaya, 15. Help Desk.
Vaccinations against tick-borne encephalitis
If you frequently visit tick habitats, it is advisable to get vaccinated against tick-borne viral encephalitis. The vaccine protects for at least 3 years. Persons working in endemic areas (foresters, geologists, etc.) and children living in endemic areas are subject to mandatory vaccination.
In Russia, vaccination is carried out with domestic vaccines (Tick-borne encephalitis vaccine, cultural purified concentrated inactivated dry, EnceVir) and foreign vaccines (FSME-Immun Inject/Junior, Encepur adult, Encepur children) or by primary and emergency schemes. All vaccines have the same immunogenicity. Vaccination can be carried out according to two schemes: the main and emergency. The main scheme (0, 1-3, 9-12 months) is carried out with subsequent revaccination every 3-5 years. To form immunity to the onset of an epidemic season, the first dose is administered in the fall, the second in winter. An emergency regimen (two injections with an interval of 14 days) is used for previously unvaccinated persons arriving in endemic foci in the spring and summer. Emergency vaccinated persons are immunized for only one season (immunity develops after 2- 3 weeks), after 9-12 months they are given the 3rd injection.
source
Signs of tick-borne encephalitis in children
The main symptoms and signs of tick-borne encephalitis in children include:
- the first sign of tick-borne encephalitis is headache, expressed by a rise in body temperature;
- sleep disorders;
- eyeball disorders;
- disorders of the vestibular apparatus.
The best measure to prevent tick-borne encephalitis in children and adults has been and remains vaccination. Vaccination against tick-borne encephalitis is recommended for everyone who lives in or stays in epidemic foci. The Kamchatka region is not endemic for tick-borne encephalitis, but nevertheless, persons planning to travel outside the region to endemic areas should take care of vaccination in advance.
Infection statistics in Moscow
Rospotrebnadzor publishes annual reports on the number of Muscovites infected with encephalitis. The period of tick activity in the region begins in mid-April and continues until the end of October. By May 1 of this year, the number of patients who applied to Moscow clinics due to insect suction exceeded 750 people (including 260 children). Laboratory studies revealed that 10% of ticks were carriers of borreliosis, 2% of granulocytic anaplasmosis, and 1% of Lyme disease. Cases of tick-borne encephalitis were identified in Moscow in the spring of 2020.
Diagnostics
It should be taken into account that a disease preceded by a tick bite will not necessarily be diagnosed as encephalitis, since no more than 5% of parasites can be carriers of the virus.
The only answer to the question: what to do if suddenly bitten by an encephalitis tick is to urgently go to the nearest emergency room!!! Doctors will provide first aid, help you correctly remove the tick and deliver it to the laboratory for examination.
When making a diagnosis of tick-borne encephalitis, it is necessary to take into account a combination of three factors:
- clinical manifestations (symptoms),
- epidemiological data (time of year, whether the vaccine was given, whether there was a tick bite)
- laboratory tests (analysis of the tick itself - optional, blood test, cerebrospinal fluid analysis, etc.).
To accurately confirm the diagnosis, it is necessary to determine specific antibodies:
- immunoglobulin class M for encephalitis (IgM) – the presence indicates an acute infection,
- IgG - the presence indicates contact with an infection in the past, or the formation of immunity.
If both types of antibodies are present, this is a current infection.
All patients with tick-borne encephalitis must be examined for tick-borne borreliosis, because It is possible to become infected with both infections at the same time.
What does a tick look like?
The carrier of the disease is the ixodid tick. This hardy insect survives even during sudden temperature changes and can go hungry for a long time. The danger of the carrier is that it indiscriminately attaches itself to a person, animal or bird and stays on the body from several days to 2-3 weeks, feeding on the blood of its victim. Ticks hide in tall grass and smell food from another 10 meters away.
The most dangerous ticks for humans are forest (taiga) ticks. They become infected with encephalitis viruses from rodents and wild animals. The parasite transmits the virus to humans through saliva and secretions.
A tick bite is not felt by humans, so most often the pest is noticed when it has already attached itself to the skin. Parasites love to hide in the thin and delicate coverings of the human body - on the neck, under the arms, in the groin. They look like small black dots, similar to moles, slightly protruding from the surface.
An allergic reaction may also occur in the form of redness, rashes on the body and itching. If the tick falls off on its own, it is almost impossible to determine the presence of a bite, since no visible traces of the bite remain.
Treatment
Anti-encephalitis immunoglobulin therapy is considered an effective treatment method for tick-borne encephalitis at an early stage of detection . An inactivated vaccine and ribonucleic acid (RNA) are also most useful for successful recovery. Timely vaccination and protection against ticks are effective methods of preventing the complex course of the disease.
When prescribing treatment, they are guided by the principle of symptom relief. Therefore, medications are mainly prescribed to maintain the body. It includes:
- antipyretics,
- detoxifying drugs,
- vitamins,
- medications that normalize the body's water balance.
The patient is prescribed strict bed rest. The specific treatment regimen depends on the time that has passed since the first symptoms appeared.
Patients are discharged on days 14-21 of normal temperature. Dispensary observation is provided by an infectious disease specialist and a neurologist for 1 year after a febrile form with examination once every 6 months. After other forms of the disease - 3 years with quarterly examination.
Detection of pathology
Diagnosis of tick-borne encephalitis is carried out on the basis of clinical manifestations, laboratory tests and data on the epidemiological situation in the region.
A patient with symptoms of pathology is examined by a neurologist. The doctor records the clinical manifestations of the disease. During the examination, signs of damage to internal organs are revealed.
Laboratory tests can detect the presence of the causative agent of encephalitis in the patient’s blood and cerebrospinal fluid. In some cases, biological materials are analyzed for the presence of antibodies to the flavivirus. Clinical recommendations for tick-borne encephalitis include computer or magnetic resonance imaging against the background of signs of severe damage to the patient’s brain.
Prevention of tick-borne encephalitis
Prevention of tick-borne encephalitis is carried out in two directions:
- vaccination - the most reliable protection against tick-borne encephalitis is one’s own antibodies, which are produced in response to vaccination. Traditionally, they are held in advance in the autumn-winter period.
- preventive measures (nonspecific prevention).
Preventive measures also include:
- refusal to consume dairy products that have not undergone heat treatment during the warm season;
- timely vaccination (can be carried out both in the autumn-winter period and within 4 days after a tick is detected on oneself - different types of vaccines are used for this);
- wearing clothing that covers the body (it is better to go out into nature in clothes with long sleeves and pants, the head should be covered with a cap);
- promptly consult a doctor if any insects are detected (removing ticks on your own is not recommended at all);
- use of tick repellents;
- after returning home, you need to take off all your clothes and immediately take a shower, then you need to carefully examine your clothes “from the forest” and your body for ticks.
If you find a tick embedded in your skin on your body, immediately seek help from medical professionals - they will remove the insect and carry out anti-encephalitic vaccination.
Questions and answers
Is it possible to visit city parks after seasonal treatment of green areas against ticks?
Yes. Visits to forested areas after acaricidal treatment are absolutely safe. A complex of insectoacaricidal preparations helps kill insects.
Are repellent preparations effective when walking in the forest or spending a long time outside the city?
These medications contain substances that repel ticks. Treating clothing with repellents is a mandatory step in preparing a person for a visit to the forest. The duration of the sprays depends on the concentration of the active substance. Detailed information can be obtained on the websites of manufacturing companies.