About the drug
Palbocent 125 mg is a new generation antitumor agent . Used for the treatment of malignant neoplasms of the mammary gland in women. Effective in the treatment of severe forms of metastatic and locally advanced oncology . The drug is based on the active component Palbociclib. The medicine is approved by the World Health Organization and the FDA for the treatment of adult patients.
Palbocent should be purchased after completing hormonal therapy. An antitumor agent is used to inhibit the development of the tumor process and improve the general condition of the patient. Therapy with Palbociclib does not guarantee 100% recovery, but increases the chances of sustained remission and tumor reduction in size.
The drug is available in the form of tablets for oral use. Each unit of the medicine contains 125 mg of the active ingredient. 1 package of Palbocent contains 21 tablets. The medication is a prescription drug. Use without the advice of a specialist should be avoided.
Experience with palbociclib in metastatic breast cancer
A meta-analysis of randomized clinical trials has shown that hormonal therapy provides a life expectancy comparable to chemotherapy and is characterized by significantly less toxicity, but is slightly inferior in terms of objective response rate. The article presents the experience of using palbociclib in a real population of patients with metastatic breast cancer.
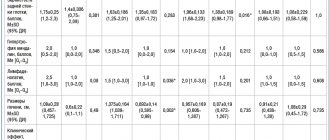
Main characteristics of observation groups
Introduction
Metastatic breast cancer (mBC) can be characterized by a long torpid course. The hormone-dependent HER2-negative tumor subtype is considered to have a favorable clinical prognosis. However, in the vast majority of cases with luminal HER2-negative mBC, resistance to endocrine therapy drugs develops. Moreover, the median progression-free survival (PFS) when using any first-line hormone therapy regimen does not exceed one year, and the median overall survival reaches almost three years [1–9].
The addition of the mTOR inhibitor everolimus to exemestane in patients with hormone receptor-positive (HR+) HER2-negative mBC progressing on non-steroidal aromatase inhibitors did not significantly change the situation: PFS increased (hazard ratio (HR) 0.43; 95% - confidence interval (CI) 0.35–0.54; p
The combination of palbociclib with letrozole or fulvestrant fundamentally improved the results of first- and second-line hormonal therapy in patients with HR+ mBC, breaking the plateau of therapeutic options and achieving PFS for more than two years [13, 14].
The high efficacy of the combination of palbociclib and letrozole in the first-line treatment of HR+ mBC was confirmed in a large phase III randomized clinical trial (RCT) PALOMA-2 involving 666 patients. The median PFS in the letrozole plus palbociclib group was significantly higher than that in the letrozole monotherapy group – 27.6 and 14.5 months, respectively (p
In the large PALOMA-3 RCT, adding palbociclib to fulvestrant in 521 patients with HR+ HER2-negative mBC who had received prior therapy achieved a median PFS of 11.2 months. In the fulvestrant monotherapy group, this indicator was 4.6 months (RR 0.50; 95% CI 0.40–0.62; p
Thus, in phase III RCTs evaluating the efficacy of palbociclib in combination with standard hormonal therapy, the combination strategy was superior to hormonal therapy.
Material and research methods
To assess the effectiveness of combination therapy with palbociclib, an analysis of data from patients with HR+ HER2-negative mBC who were examined and treated in medical institutions of the Moscow Department of Health was carried out. The observation period was 12 months - from September 2021 to September 2021. Patients received therapy with palbociclib at a standard dose of 125 mg once daily according to a 3/1 regimen in combination with any aromatase inhibitor or fulvestrant in doses approved for use [16 ].
results
We analyzed data from 110 patients with HR+ HER2-negative mBC who received palbociclib in combination with hormone therapy. Clinical and epidemiological characteristics are shown in the table.
Efficacy of palbociclib in combination with hormone therapy
In this analysis, with a median follow-up of 12 months, the ORR in the entire patient population in both combinations of aromatase inhibitors and fulvestrant was 43%, and in the subgroup of patients with measurable lesions - 52%. Overall, tumor growth control, including objective response and stabilization, was recorded in 78% of cases. At the time of data analysis, the median PFS in the palbociclib group in combination with any aromatase inhibitor had not been reached, more than 90% of patients continued to receive therapy. Palbociclib in combination with fulvestrant after progression on prior therapy provided a median PFS of 8.4 months, an ORR in patients with measurable lesions was 24.6%, and clinical benefit occurred in 64% of cases. The initial menopausal status of the patients did not affect the results of therapy.
Tolerability of palbociclib in combination with hormone therapy
The main adverse events associated with palbociclib were neutropenia, leukopenia and thrombocytopenia. No cases of febrile neutropenia were recorded. However, due to grade 3–4 adverse events, treatment was interrupted in 5% of patients in the palbociclib and aromatase inhibitor group and 8% of patients in the palbociclib and fulvestrant group. The start of the next cycle was delayed in 27–32% of patients. In 24% of cases a dose reduction was required. This figure was lower than similar rates recorded in the PALOMA-2 and PALOMA-3 RCTs.
Conclusion
Literature data and the presented clinical experience demonstrate the high effectiveness and good tolerability of combined hormone therapy regimens with CDK type 4/6 inhibitors, in particular palbociclib. It is advisable to use such combinations already in the first lines of therapy, primarily in the presence of risk factors for the aggressive course of HR+ HER2-negative mBC (luminal type B tumors, visceral and combined metastases, including those with multiple metastasis loci, previous therapy with cytostatics).
Palbociclib has a manageable toxicity profile with a dose reduction schedule and requires minimal monitoring during treatment. In this observation, the frequency of drug dose reduction due to adverse events was lower than in registration clinical studies.
Active substance and treatment regimen
The active component of Palbocent 125 mg, Palbociclib, has a direct effect on abnormal cells - the main cause of the occurrence and development of malignant tumors in the mammary gland. The substance replaces the leading building proteins of cancer tissue. This leads to disruption of the process of division of cancer cells and their accelerated aging. As a result, the development of the tumor process is suspended, and the tumor itself decreases in size.
The medicine is used as a single drug or in tandem with other antitumor drugs. The choice of treatment regimen depends on the diagnosis and degree of damage to the mammary gland. For metastatic cancer, a combination with additional medications and radiation therapy is recommended. It is important to note that Palbocent is recommended after a course of taking medications that suppress estrogen production.
According to the results of an International Multicenter Randomized Blind Study, the effectiveness of the Palbociclib + Fulvestrant regimen was established. The combination is effective in terminal stages in the absence of positive results from previous therapy.
Itulsi, 125 mg, capsules, 21 pcs.
The pharmacokinetics of palbociclib have been described in patients with solid tumors, including advanced breast cancer, and in healthy volunteers.
Absorption The maximum concentration (Cmax) of palbociclib is generally achieved 6-12 hours (Cmax) after oral administration. The mean absolute bioavailability of palbociclib following a 125 mg oral dose is 46%. In the dose range from 25 mg to 225 mg, the area under the concentration-time curve (AUC) and Cmax generally increase proportionally to the dose. The equilibrium state was achieved within 8 days after repeated dosing of the drug once a day. Palbociclib accumulation occurs with repeated once-daily dosing, with a mean accumulation rate of 2.4 (range: 1.5-4.2).
Effect of food When administered on an empty stomach in approximately 13% of the population, absorption and exposure of palbociclib were very low. Food intake increased palbociclib exposure in a small subset of the population but did not change palbociclib exposure to a clinically significant amount in the rest of the population.
Compared with palbociclib administered in the morning in the fasted state, AUCinf and Cmax of palbociclib increased by 21% and 38% when administered with a high-fat meal, by 12% and 27% when administered with a low-fat meal, and by 13% and 24% , if a moderate-fat meal was taken 1 hour before and 2 hours after palbociclib. In addition, food intake significantly reduced variability in palbociclib exposure measurements both between different participants and within the same participant. Based on these results, palbociclib should be taken with food.
Distribution The binding of palbociclib to human plasma proteins in vitro was approximately 85%, with no concentration dependence observed in the concentration range of 500-5000 ng/ml. The mean free fraction (fu) of palbociclib in human plasma in vivo increased with impaired liver function. There were no significant changes in the mean fu value of palbociclib in human plasma in vivo with renal impairment. The geometric mean apparent volume of distribution (Vz/F) was 2583 L (25%).
Metabolism: In vitro and in vivo studies indicate that palbociclib is extensively metabolized in the liver in humans. Following oral administration of a single 125 mg dose of [14C]-palbociclib in humans, the major pathways of primary metabolism of palbociclib included oxidation and sulfonation, with acylation and glucuronidation serving as minor pathways. Palbociclib was the major circulating drug-associated compound in plasma. The major circulating metabolite was the glucuronic acid conjugate of palbociclib, although it represented only 1.5% of the administered dose in body secretions. Most of the material was excreted as metabolites. In stool, the main drug-associated component was palbociclib sulfamic acid conjugate, which represented 25.8% of the administered dose. In vitro studies using human hepatocytes, cytosolic and S9 fractions of liver cells, and recombinant sulfotransferase enzymes (SULTs) have shown that the metabolism of palbociclib primarily involves CYP3A and SULT2A1.
Elimination In patients with advanced breast cancer, the geometric mean apparent oral clearance (CL/F) of palbociclib was 63.08 L/h and the mean plasma half-life was 28.8 hours. In 6 healthy male volunteers who received a single oral dose of [14C]-palbociclib, an average of 91.6% of the total radiolabeled dose administered was cleared after 15 days; the main route of elimination was intestinal excretion (74.1% of the dose), and 17.5% of the dose was excreted through the kidneys. Excreted unchanged, palbociclib accounted for 2.3% and 6.9% of the administered dose in feces and urine, respectively.
Age, Gender and Body Weight Based on the results of a population pharmacokinetic analysis, gender did not have an effect on palbociclib exposure, and age and body weight did not have a clinically significant effect on palbociclib exposure.
Use in Children The pharmacokinetics of palbociclib in patients 18 years of age and younger have not been studied.
Use in Elderly Patients There were no differences in safety or effectiveness observed in patients aged 65 years and older compared to younger patients.
Hepatic Impairment Pharmacokinetic data from a pharmacokinetic study in patients with varying degrees of hepatic impairment show that exposure to free palbociclib (free AUCinf) was reduced by 17% in patients with mild hepatic impairment (Child-Pugh A) and increased by 34%. and by 77% in patients with moderate (Child-Pugh class B) and severe (Child-Pugh class C) liver dysfunction, respectively, compared to patients with normal liver function. Peak exposure to free palbociclib (free Cmax) was increased by 7%, 38% and 72% in mild, moderate and severe hepatic impairment, respectively, relative to patients with normal hepatic function. In addition, based on the results of a population pharmacokinetic analysis of data from 183 patients with advanced cancer, of which 40 patients had mild liver dysfunction according to the National Cancer Institute classification (total bilirubin ≤ upper limit of normal (ULN) and aspartate aminotransferase (AST) > ULN or total bilirubin > 1.0-1.5 x ULN at any AST level), mild hepatic impairment did not affect the pharmacokinetics of palbociclib.
Renal Impairment Pharmacokinetics data from a pharmacokinetic study in patients with varying degrees of renal impairment indicate that total palbociclib exposure (AUCinf) was increased by 39%, 42%, and 31% in mild renal impairment (60 mL/min ≤CrCl < 90 mL/min ), moderate (30 ml/min <CK < 60 ml/min) and severe degree (CK < 30 ml/min), respectively, in relation to patients with normal renal function (CK ≥90 ml/min). Peak palbociclib exposure (Cmax) was increased by 17%, 12%, and 15% in mild, moderate, and severe renal impairment, respectively, relative to patients with normal renal function. Additionally, based on a population pharmacokinetic analysis of 183 patients with advanced cancer, of whom 73 patients had mild renal impairment and 29 patients had moderate renal impairment, mild to moderate renal impairment had no effect on the pharmacokinetics of palbociclib. . The pharmacokinetics of palbociclib in patients requiring hemodialysis have not been studied.
Cardiac Electrophysiology The effect of palbociclib on the adjusted QT interval was assessed using time-matched electrocardiograms assessing changes in baseline and related pharmacokinetic data in 77 patients with breast cancer. Palbociclib did not prolong the QT interval by any clinically significant amount at the recommended dose of 125 mg per day (regimen 3/1).
Palbociclib: instructions for use
According to the instructions, palbociclib should be taken once a day, 1 tablet. Individual adjustment of the dosage of the medicine by the attending physician is allowed. It is strictly not recommended to independently change the daily amount of the drug or stop therapy.
The tablet should be swallowed whole . For better dissolution, you can take the medicine with warm water or milk. The exception is forms of the disease when the patient is unable to swallow independently. In this case, the tablet is crushed and dissolved in a small amount of water.
The medicine should not be taken after the expiration date. The drug release information is indicated on the Palbocent packaging. The medicine should be stored in a dark place with good ventilation at a temperature not exceeding 25 degrees Celsius.
Contraindications and side effects
Before you buy Palbociclib, carefully read the instructions for use of this drug. Particular attention should be paid to contraindications and side effects of the antitumor drug. The medicine should not be taken if :
- Functional liver disorders: severe and moderate, with elevated levels of ALT and AST.
- Kidney pathologies with creatine clearance less than 30 ml per minute.
- The need for regular hemodialysis.
- Pregnancy and breastfeeding.
- Childhood or adolescence under 18 years of age.
Until recently, being male was also a contraindication for taking Palbocent. In 2019, clinical studies were conducted with the participation of groups of voluntary subjects. As a result of the experiment, it turned out that taking the drug is acceptable in the treatment of breast cancer in men, but Palbocent is recommended for the treatment of women.
Side effects of Palbociclib according to the instructions are::
- Decreased immunity: susceptibility to parasitic, viral and bacterial infections.
- Anemia and other disorders in the hematopoietic system.
- Dry eyes, blurred vision, tearing.
- Headaches, weakness, loss of appetite.
- Dry skin, rashes, alopecia.
- Nosebleeds.
Before you buy Palbociclib at the manufacturer's price, it is important to take care to prevent pregnancy during therapy. The active substance negatively affects the intrauterine development of the fetus.
Breast cancer (BC) is the most common tumor disease in women worldwide. Most often, the disease is detected at an early stage, but approximately 20% of patients experience the disease at the stage of local or systemic spread of the disease [11]. Despite advances in oncology over the past 10 years, metastatic disease remains incurable. A feature of malignant neoplasms is the ability to grow uncontrolled due to overexpression of growth factors and loss of the cell cycle checkpoint [9, 17]. Ways to overcome resistance to endocrine therapy is one of the most pressing problems in the treatment of breast cancer. Research on resistance has led to an understanding of the fundamental role of crosstalk in signaling pathways of different estrogen receptors and the influence of acquired mutations of estrogen receptors in the formation of resistance. Studies in preclinical models also suggest that adaptive activation of growth factor signaling pathways is associated with acquired or existing resistance to endocrine therapy [1, 3]. For example, the PI3K/AKT/mTOR signaling pathway directly and indirectly interacts with estrogen receptors and activation of this signaling pathway through mutation of PI3KCA (the most common mutation in hormone-positive breast cancer is a potential target) or AKT causes resistance to selective estrogen receptor modulators and receptor antagonists estrogens such as fulvestrant [19]. Mutations in PI3KCA, the α-catalytic subunit of PI3-kinase, are a common genetic phenomenon in hormone-positive breast cancer [25].
Activation of the CDK4/CDK6/E2F signaling pathway is a common feature of luminal (hormone-positive) breast cancer. Endocrine therapy achieves its effect by suppressing the activity of CDK4 and CDK6; reactivation of these kinases is involved in the formation of resistance to endocrine therapy [20]. Various studies show that endocrine-naïve and endocrine-resistant luminal breast cancer cell lines are sensitive to CDK4 and CDK6 inhibition and demonstrate synergy with endocrine therapy. In cell lines, the combination of CDK4 and CDK6 suppression and fulvestrant led to a decrease in retinoblastoma protein phosphorylation, which in turn led to sustained inhibition of the cell cycle and increased markers of cellular senescence [7, 12, 23].
Retinoblastoma protein functions as a cell cycle checkpoint regulator in a mammalian cell. In its hypophosphorylated state, the retinoblastoma protein suppresses the expression of proteins required for completion of the S phase of the cell cycle. G1-cyclin-dependent kinases types 4 and 6 (CDK 4 and 6), functioning together with D-type cyclins, initiate phosphorylation of the retinoblastoma protein and block the suppressive effect of the retinoblastoma protein on the cell cycle [14, 21, 24]. Thus, the cyclin D-CDK4/6 complex is a key regulator of the retinoblastoma protein.
Deviations in the cyclin-dependent kinase-retinoblastoma protein signaling pathway are often observed in breast cancer. In particular, cyclin D1 (encoded by the CCND1 gene) plays a critical role in the development of this disease. CCND1 amplification is observed in 15–20%, and overexpression of cyclin D1 in almost 50% of breast cancer cases [2].
Until recently, the principles of treatment of hormone-positive metastatic breast cancer (mBC) remained unchanged. Consistent use of various options for endocrine therapy allows us to achieve a significant increase in the survival rate of patients with mBC and at the same time maintain a high quality of life. However, despite these possibilities, patients inevitably face progression of the disease, which at a certain point becomes an indication for starting chemotherapy. Studying ways to overcome resistance to endocrine therapy is one of the basic tasks in the treatment of advanced breast cancer.
The possibility of using agents that affect the basic mechanisms of cell cycle regulation has become the subject of great interest. The first generation of CDK (Cyclin-dependent kinases) inhibitors turned out to be broadly targeted, affecting a wide range of cyclin-dependent kinases and accompanied by toxicity comparable to cytostatics and an unacceptable toxicity profile [10, 23]. Later, a new generation of more narrowly targeted CDK4/6 inhibitors was developed: palbociclib (PD0332991, Pfizer), abemaciclib (LY2835219, Lilly), ribociclib (LEE011, Novartis).
Palbociclib is an oral selective inhibitor of CDK4 and CDK6 that blocks proliferation by preventing the transition of the cell cycle from G1 to S phase [15]. The emergence of data on the effectiveness of palbociclib for patients with hormone-positive advanced breast cancer may make significant changes to established ideas about the treatment of this form of the disease.
Preliminary data from only a few phase II studies are known about the preoperative use of palbociclib. In 2015, L. Chow et al. presented the first results of using the combination of palbociclib and letrozole for 4 months in 11 (out of 45 planned for inclusion in the phase II OOTR-N007 study) patients with EC (estrogen receptor)-positive, HER2 (human epidermal growth factor receptor-2)-negative breast cancer and a tumor larger than 2 cm. The objective response rate was 89%, the rate of achieving a complete morphological response was 11% [4].
At ESMO (European Society for Medical Oncology) 2021, the first results of the randomized phase II NeoPal trial were reported, the purpose of which was to compare the rate of achieving complete morphological regression after using the combination of palbociclib with letrozole and standard neoadjuvant chemotherapy, which included 3 courses of FEC (fluorouracil + epirubicin +cyclophosphamide) and 3 courses of docetaxel, in patients with EC+HER2-BC (confirmed by the results of Prosigna®IC genetic analysis) stages II–III.
The analysis included 106 patients, 53 in each group, of which 52 were operated on in the palbociclib + letrozole group and 51 in the chemotherapy group. About a third of patients in both groups had lymph node metastases, a high risk, according to genetic testing; had 86.8 and 84.9%, respectively. The duration of therapy was 18 weeks. The rate of achieving a complete clinical response in the groups was the same: 16 (31.4%) in the endocrine therapy group and 15 (30%) in the chemotherapy group. Organ-preserving operations were performed in 36 (69.2%) and 35 (68.6%) patients, respectively. Complete therapeutic pathomorphosis was achieved by 2 (3.8%) patients in the palbociclib therapy group and 3 (5.9%) in the chemotherapy group. Therapy with palbociclib with letrozole was safer: not a single episode of febrile neutropenia was noted, while in the chemotherapy group - in 6% of patients; Serious adverse events were recorded in 2 and 17 patients, respectively. A dose reduction of palbociclib was required in 10 patients, docetaxel in 16 patients, premature cessation of therapy was required in 2 patients in the endocrine therapy group and 7 in the chemotherapy group. In the postoperative period, 70% of patients in the palbociclib group received adjuvant chemotherapy. Results of 3-year event-free survival will be reported soon [5].
Results are expected from two more phase II studies of the combination of palbociclib with endocrine therapy in the neoadjuvant setting (NCT 02764541, NCT 02296801), the NeoPalAna study (NCT 01723774), as well as one study of the combination of palbociclib with letrozole and trastuzumab in patients with HR+HER2 breast cancer stages II–III ( NCT 02907918).
A number of studies and adjuvant use of palbociclib in breast cancer patients with hormone-positive, HER2-negative tumors are being conducted.
The phase III PENELOPE-B trial (NCT 18644746) is examining the efficacy of 13 cycles of palbociclib/placebo in combination with standard endocrine therapy in patients with residual disease after neoadjuvant chemotherapy. The study plans to include 1,100 patients, with treatment results expected by 2023.
The phase III PALLAS trial (NCT 02513394) is studying the use of palbociclib for two years in addition to standard endocrine therapy in stages II and III breast cancer. The planned enrollment in the study is 4600 patients, results are expected by 2025.
The efficacy of palbociclib monotherapy was studied in a phase II study in 37 patients with retinoblastoma protein-expressing breast cancer who had previously received several lines of treatment; 84% of patients included in the study had hormone-positive, HER2-negative breast cancer. The median progression-free survival (PFS) for all patients included in the study was 3.7 months, while the median survival among patients with HR+HER2 tumors was 5.1. An objective response in the group with hormone-positive tumors was achieved in 6%, disease control in 21% of cases, respectively [8]. Another study presented at ASCO (American Society of Clinical Oncology) 2021 demonstrated that palbociclib monotherapy in pretreated patients (67% received 1 line of endocrine therapy and 33% received 2 lines; 1 line of chemotherapy received 33% of patients) allowed to achieve disease control in 60% of cases, the median duration of which was 6 months. The median PFS was 11.5 months [18].
The randomized phase II PALOMA-1/TRIO-18 trial (NCT00721409) examined the efficacy of palbociclib plus letrozole versus letrozole in patients with hormone-positive, HER2-negative breast cancer. The study consisted of two parts. The first included patients who had not previously received treatment for advanced breast cancer. In the second part, patients were additionally screened for CCND1 amplification and/or p16 loss. 66 and 90 patients were randomized into each arm of the study, respectively. Response and disease control rates in the palbociclib+letrozole group (n=84) were 42% and 80%, respectively; in the letrozole monotherapy group (n=84) – 32 and 57% (p=0.0046). PFS for all patients (n=165) receiving palbociclib plus letrozole was 20.2 months compared with 10.2 months in the letrozole group (hazard ratio [HR]=0.48, 95% confidence interval [CI] - 0.319 to 0.748; p=0.0004). However, there was no significant difference in overall survival between the groups. The most common grade 3–4 adverse events were neutropenia (54 vs. 1%), leukopenia (19 vs. 0%), anemia (6 vs. 1%), and fatigue (4 vs. 1%) [22].
Relatively recently, the results of the phase III double-blind PALOMA-2 study were published, studying letrozole +/- palbociclib in 666 patients with hormone-positive, HER2-negative breast cancer. Randomization was carried out in a 2:1 ratio.
The study included patients with confirmed menopause. More than a third of patients had primary mBC, about 20% progressed within less than 12 months from completion of adjuvant endocrine therapy. Adjuvant or neoadjuvant use of aromatase inhibitors was possible unless disease progression occurred during their use or within 12 months after completion of therapy. The somatic status of the patients according to the ECOG (Eastern Cooperative Oncology Group) scale was 0–2, measured manifestations of the disease were assessed in accordance with RECIST (Response evaluation criteria in solid tumors) 1.1 criteria. Inclusion of patients was allowed, incl. only bone metastases.
The primary objective of the study was to evaluate the PFS of the disease. Secondary study objectives included overall survival, objective response, duration of objective response, clinical benefit (confirmed complete or partial disease regression or stabilization >24 weeks), pharmacokinetic studies, safety, and evaluation of biomarkers in tumor tissue.
A total of 444 patients were randomized to the letrozole+palbociclib group and 222 to the letrozole+placebo group. Their mean age was 62 years in the letrozole+palbociclib group and 61 years in the letrozole+placebo group. Among all patients, 48.6% had visceral metastases, only bone metastases – in 22.4%. 48.6% of patients received previous neo- or adjuvant chemotherapy, and 56.5% of patients received endocrine therapy.
The study confirmed the results of the PALOMA-1 study. Median PFS in the palbociclib group was 24.8 months (95% CI 22.1 to not assessed) versus 14.5 months in the letrozole monotherapy group (HR=0.58; CI 0.46 to 0.72; p<0.001 ). Based on stratification factors and baseline characteristics, subgroup analysis confirmed a significant benefit of letrozole + palbociclib in all subgroups.
The objective response rate in the letrozole + palbociclib group was 42.1% (95% CI 37.5 to 46.9). Among patients with measurable disease, the objective response rate was 55.3% (95% CI 49.9 to 60.7). In the letrozole + placebo group, the objective response rate was 34.7% (95% CI 28.4 to 41.3), in patients with measurable disease manifestations - 44.4% (95% CI 36.9 and 52.2 ).
The most common side effect is stage 3. There was neutropenia (56.1%) in the palbociclib group, with febrile neutropenia occurring in 1.8% of patients. With the exception of neutropenia and leukopenia, 57% of patients had grade 1–2 side effects, and 39.2% of patients had grade 3–4 side effects. Hematological toxicity was observed in 79.5% in the letrozole + palbociclib group and 6.3% in the letrozole + placebo group. Grade 3–4 hematologic toxicities included neutropenia (66.4% in the letrozole + palbociclib group and 1.4% in the letrozole + placebo group), leukopenia (24.8 and 0%), anemia (5.4 and 1. 8%) and thrombocytopenia (1.6 and 0%). The most common non-hematological side effects were weakness (37.5 and 27.5%), nausea (35.1 and 26.1%) and arthralgias (33.3 and 33.8%). Other side effects that were more common in the letrozole + palbociclib group were diarrhea (26.1 vs. 19.4%), cough (25.0 vs. 18.9%), and stomatitis (15.3 vs. 5.9%) [ 13].
Thus, the PALOMA-2 study demonstrated that the combination of palbociclib + letrozole in the 1st line of therapy allows an increase in PFS of more than 10 months, which is rightfully considered the best result in the duration of PFS of the disease in the entire history of the development of drug treatment for hormone-positive, HER2- negative mBC.
The promising results of the use of palbociclib in patients who had previously received endocrine therapy, demonstrated in phase II studies, became the basis for further study of the drug in the 2nd line of endocrine therapy in phase III.
The double-blind, multicenter, phase III PALOMA-3 study examined the efficacy of the combination of fulvestrant + palbociclib and fulvestrant + placebo in 521 patients with hormone-positive, HER2-negative advanced breast cancer after relapse or progression of the disease during endocrine therapy [6]. Pre- and perimenopausal patients were allowed to be included if they were prescribed goserelin. 79% of patients were considered hormone sensitive, approximately a third of patients had received chemotherapy for breast cancer previously, 40% of patients were treated with aromatase inhibitors, 15% with tamoxifen, 45% with both drugs. Patients were randomized into the fulvestrant + palbociclib and fulvestrant + placebo groups in a 2:1 ratio. Patients received fulvestrant in a standard regimen (500 mg IM on days 1, 15 and then every 28 days continuously). Patients also received palbociclib 125 mg/day or placebo for 3 weeks at 1-week intervals; cycle – 28 days. Study treatment was continued until disease progression into intolerable toxicity, withdrawal of informed consent, or death.
The primary objective of the study was to assess PFS survival. The assessment was based on RECIST 1.1 criteria. The secondary objectives of the study were to evaluate objective response (complete and partial response), disease control, tumor tissue biomarkers, and treatment safety.
521 patients were included and randomized into the fulvestrant+palbociclib (n=347) and fulvestrant+placebo (n=174) groups. The initial characteristics of the patients in both groups did not differ significantly. 347 (67%) patients had metastases in two or more zones, and 406 (78%) patients had measurable manifestations of the disease. More patients in the palbociclib group than in the placebo group had a history of two lines of endocrine therapy: 140 (40%) of 347 versus 61 (65%) of 174 patients; 177 (34%) patients had a history of chemotherapy for metastatic disease.
Median PFS was 9.5 months in the palbociclib + fulvestrant group and 4.6 months in the fulvestrant + placebo group (HR = 0.46; 95% CI 0.036 to 0.5; p < 0.0001). An objective effect in the placebo group was observed in only 15 patients (10.9%; 95% CI - 6.2–17.3). It should be noted that the effect of palbociclib was also observed in pre- and postmenopausal patients [6].
Neither the effectiveness of the fulvestrant + palbociclib combination nor the likelihood of disease progression more than 6 months after inclusion in the study depended on the level of expression of estrogen and progesterone receptors.
PIK3CA gene status did not significantly influence the degree of clinical benefit associated with fulvestrant + palbociclib or receptor status. There was also no connection between the expression of estrogen receptors and the presence of PIK3CA mutations.
Grade 3–4 toxicities included neutropenia (65 vs. 1.0%), leukopenia (28 vs. 1%), anemia (3 vs. 2%), thrombocytopenia (3 vs. 0%), and fatigue (2 vs. 1%) in palbociclib and placebo groups, respectively. Febrile neutropenia was a rare side effect in both groups. Infections, alopecia, rash, and stomatitis were also more common in the palbociclib group.
Serious adverse events occurred in 44 (13%) of 345 patients in the fulvestrant + palbociclib group and 30 (17%) of 172 patients in the fulvestrant + placebo group. In 187 (54%) patients in the fulvestrant + palbociclib group, there was a temporary cessation of treatment due to toxicity, in 123 (36%) there was a delay in the next cycle, in 117 (34%) there was at least a single dose reduction of palbociclib, in the fulvestrant + placebo group - 10 (6%), 3 (2%) and 3 (2%) respectively. In 14 (4%) patients in the fulvestrant + placebo group and 3 (2%) in the fulvestrant + placebo group, treatment was discontinued due to side effects.
Despite the high frequency of side effects, incl. 3–4 degrees, the quality of life of patients receiving fulvestrant with palbociclib remained unchanged for a long time (65.9–66.1%), while during treatment with placebo + fulvestrant a significant difference was noted (p = 0. 0313) decrease in global quality of life (from 65.3 to 63%) [16].
Thus, in the PALOMA-3 study, a significant increase in PFS of the disease occurred in the fulvestrant + palbociclib group in patients with receptor-positive, HER2-negative breast cancer who had previously received endocrine therapy. Also, the use of the fulvestrant + palbociclib combination was accompanied by a significant increase in the objective response rate, clinical benefit and relapse-free survival. The effectiveness of palbociclib did not depend on the number of lines of endocrine therapy in history, sensitivity to previous endocrine therapy, or biomarkers that influenced the effectiveness of treatment (such as the level of expression of estrogen and progesterone receptors). In addition, the combination was effective in patients with a history of two ineffective lines of endocrine therapy.
Patients in this category are most often considered to be refractory to endocrine therapy, and subsequently they are prescribed chemotherapy in monotherapy (taxanes, capecitabine, eribulin, etc.), the choice of which is quite limited. Objective response was observed in 66 (25%) of 268 patients with measurable disease treated with fulvestrant + palbociclib, which was generally comparable to the effect of chemotherapy. At the same time, the toxicity profile of the fulvestrant + palbociclib combination appears to be more favorable compared to chemotherapy.
Conclusion
Over the past 15 years, the principles of treatment of advanced hormone-positive, HER2-negative breast cancer have not changed significantly. There were no fundamental changes in the results of treatment of this category of patients. With the advent of palbociclib, an oral selective inhibitor of CDK4 and CDK6, and its subsequent introduction into widespread clinical practice, we can witness dramatic changes in the fate of patients and the very nature of the course of this form of advanced breast cancer.
From our point of view, the main candidates for therapy with a combination based on palbociclib may be patients with hormone-positive, HER2-negative breast cancer, including patients with visceral lesions (without signs of visceral crisis), for whom chemotherapy would definitely be recommended before the possibility of treatment with palbociclib due to with the spread of the disease. Strong arguments in favor of prescribing this treatment regimen are the advantages in the safety profile and a significant increase in PFS compared to standard therapy.
Palbociclib price
The price of Palbociclib in Russia depends on the manufacturer of the drug. Indian and Bangladeshi medicines are somewhat cheaper than antitumor drugs from the USA or the European Union. Moreover, in terms of quality characteristics and composition, the drugs are completely identical.
It is important to note that when purchasing Bangladeshi Palbociclib Palbocent, price is of paramount importance. In other countries, an antitumor drug may not cost much more or less.
When selling Palbocent, a price several times higher than the manufacturer's price indicates the dealer's dishonesty. An undervalued price indicates a possible counterfeit of the medicine. Manufacturers will not work to their detriment and sell drugs too cheap.
If you purchase a medicine on the InApteka portal, the buyer receives the medicine at the official price. The price of Bangladeshi Palbociclib in Russia is 19,900 rubles per package .
Description of the drug PALBOCICLIB
After oral administration, the average Cmax of palbociclib is usually achieved within 6-12 hours (Tmax). At a dose of 125 mg, the average absolute bioavailability is 46%. In general, AUC and Cmax in the dose range from 25 mg to 225 mg increase proportionally with dose. The equilibrium state was achieved within 8 days after repeated dosing of the drug once a day. With multiple doses of palbociclib once a day, accumulation of palbociclib occurs, with a median accumulation coefficient of 2.4 (range 1.5-4.2).
Compared with morning fasting, the population mean AUCinf and Cmax of palbociclib increased by 21% and 38%, respectively, when administered with a high-calorie, high-fat meal (approximately 800 to 1000 calories, of which 150, 250, and 500 to 600 calories). calories came from proteins, carbohydrates and fats, respectively); by 12% and 27%, respectively, when taken with a low-calorie, low-fat meal (approximately 400 to 500 calories, of which 120, 250, and 28 to 35 calories came from protein, carbohydrates, and fat, respectively); and by 13% and 24%, respectively, when eating a meal of normal calorie content and moderate fat content (approximately 500 to 700 calories, of which 75-105, 250-350 and 175-245 calories came from protein, carbohydrates and fat, respectively) was carried out 1 hour before administration and 2 hours after administration of palbociclib.
The binding of palbociclib to human plasma proteins in vitro was approximately 85%, with no dependence on the concentration of the active substance observed in the concentration range of 500-5000 ng/ml. The mean unbound fraction (fu) of palbociclib in human plasma in vivo increased gradually with deterioration of liver function. There was no apparent trend in the mean human plasma fu value of palbociclib in vivo with worsening renal function. The geometric mean apparent volume of distribution (Vz/F) was 2583 L with a coefficient of variation (CV) of 26%.
In vitro and in vivo studies indicate that palbociclib undergoes hepatic biotransformation in humans. Following a single 125 mg oral dose of [14C]-labeled palbociclib, the major metabolic pathways of palbociclib included oxidation and sulfonation, with minor pathways including acylation and glucuronidation. Palbociclib was the main compound released from the drug and circulating in the blood plasma (23%). The main circulating metabolite was the glucuronide conjugate of palbociclib, although it accounted for only 1.5% of the drug dose in excreta. Palbociclib was extensively metabolized, with unchanged drug accounting for 2.3% and 6.9% of radioactivity in feces and urine, respectively. The major drug metabolite detected in feces was palbociclib sulfamic acid conjugate, accounting for 26% of the drug dose administered. In vitro studies on human hepatocytes, cytosolic and S9 fractions of the liver, as well as with recombinant SULT enzymes showed that the metabolism of palbociclib mainly involves the enzymes CYP3A and SULT2A1.
In patients with advanced breast cancer, the geometric mean apparent oral clearance (CL/F) of palbociclib was 63.1 L/h (CR 29%), and the mean (± standard deviation) plasma T1/2 was 29 h ± 5 h. In 6 healthy male volunteers, following a single oral dose of [14C]-labeled palbociclib, the median total radioactive dose administered was 91.6% cleared in 15 days; the main route of elimination was excretion in feces (74.1% of the dose), and 17.5% in urine. Most of the active substance was excreted in the form of metabolites.
Results from a pharmacokinetic study in patients with varying liver function showed that the unbound AUCinf of palbociclib decreased by 17% in patients with mild hepatic impairment (Child-Pugh class A) and increased by 34% and 77% in patients with liver dysfunction of moderate (Child-Pugh class B) and severe (Child-Pugh class C) severity, respectively, compared with patients with normal liver function. The unbound Cmax of palbociclib increased by 7%, 38% and 72% in mild, moderate and severe liver dysfunction, respectively, compared with patients with normal liver function.
Renal dysfunction.
The results of a pharmacokinetic study in patients with different renal functional status show that the AUCinf value of palbociclib increased by 39%, 42% and 31% in mild (60 ml/min ≤ CL < 90 ml/min), moderate (30 ml/min ≤ CL <60 ml/min) and severe (creatinine clearance <30 ml/min) renal impairment, respectively, compared with patients with normal renal function. Peak palbociclib exposure (Cmax) was increased by 17%, 12%, and 15% in mild, moderate, and severe renal impairment, respectively, compared with subjects with normal renal function.
Preclinical Safety Data
Changes found in target organs of potential relevance to humans in studies of up to 39 weeks in rats and dogs included effects on the hemato-lymphopoietic system and the male reproductive system. Impaired glucose metabolism was associated with changes in the pancreas, with secondary effects on the eyes, teeth, kidneys, and adipose tissue in studies lasting ≥15 weeks in rats, and changes in bone tissue were observed in rats only after 27 weeks of dosing. These systemic toxicities were reported at clinically significant exposures based on AUC data. In addition, effects on the cardiovascular system (prolongation of the QTc interval, decreased heart rate and increased RR interval and systolic pressure) were found in dogs at dosing of 4 times the clinical dose, as determined by Cmax. Reversibility of effects on glucose homeostasis, pancreas, eyes, kidneys and bone tissue after a 12-week after-effect period was not established, while the reported effects on the hemato-lymphopoietic system and the male reproductive system, teeth and adipose tissue were partially or completely reversible .
In a 27-week toxicology study, repeated administration of the drug in rats that had not reached puberty at the start of the study revealed altered glucose metabolism (glucosuria, hyperglycemia, decreased insulin levels) associated with changes in the pancreas (vacuolization of islet cells), eyes (cataract, lens degeneration), kidney (tubular vacuolation, chronic progressive nephropathy) and adipose tissue (atrophy), and these changes were observed more often in males receiving the drug at doses ≥30 mg/kg/day (approximately 11 times the exposure in adult (AUC) at the recommended dose). Some of these changes (glucosuria/hyperglycemia, pancreatic islet cell vacuolation, and renal tubular vacuolation) were observed in a 15-week repeat dose toxicology study in rats, but were of lower incidence and severity. Alterations in glucose metabolism or associated changes in the pancreas, eyes, kidneys, and adipose tissue were not observed in the 27-week repeat dose toxicology study in rats that were sexually mature at the start of the study and in the repeat dose toxicology study for up to 39 weeks. weeks in dogs.
Toxic effects on teeth were observed in rats, independent of changes in glucose metabolism. Palbociclib 100 mg/kg/day for 27 weeks (approximately 13 times adult exposure (AUC) at the recommended dose) resulted in abnormalities in growing incisors (discoloration, ameloblast degeneration/necrosis, mononuclear cell infiltration). cells). Other toxicities potentially significant in pediatric patients have not been studied in young animals.
Palbociclib was evaluated for carcinogenicity in a 6-month transgenic mouse study and a 2-year rat study. No adverse effects associated with carcinogenicity were observed in transgenic mice at doses of 60 mg/kg/day (the no observed adverse effect [NOEL] dose was approximately 11 times the human dose used in standard practice, based on AUC). Neoplastic effects observed with palbociclib included an increase in central nervous system microglial cell tumors in males at 30 mg/kg/day; females did not experience the development of any neoplasms when using the drug in doses up to 200 mg/kg/day. The NOEL for the carcinogenic effect of palbociclib was 10 mg/kg/day (approximately 2 times the dose used in standard human clinical practice, based on AUC) and 200 mg/kg/day (approximately 4 times the dose used in standard clinical practice in humans). clinical practice in humans, based on AUC) in males and females, respectively.
Palbociclib induced micronuclei through an aneugenetic mechanism in Chinese hamster ovary cells in vitro and in the bone marrow of male rats when administered at doses of 100 mg/kg/day or more. The drug concentration that did not cause an observed adverse effect was 7 times higher than the drug concentration in humans when used at standard clinical doses, based on AUC.
Based on non-clinical studies in rats and dogs, palbociclib is believed to be capable of interfering with reproductive function and fertility in men.
The following effects have been associated with palbociclib on the testes, epididymis, prostate and seminal vesicle:
- decrease in organ weight, atrophy, degeneration, hypospermia, the appearance of intracordial cellular detritus, decreased concentration and motility of sperm, decreased sperm secretion. These events were observed in rats and/or dogs at exposures subtherapeutic or 7 times or more greater than human clinical exposures determined based on AUC, respectively.
Partial reversibility of the effects on the male reproductive organs was observed in rats and dogs after a 4- and 12-week withdrawal period, respectively. Despite documented changes in male reproductive organs, no effects on mating or fertility were observed in male rats at exposure doses equal to 13 times the clinical exposure dose on a human basis based on AUC.
Palbociclib is a reversible inhibitor of cyclin-dependent kinases 4 and 6, which are both involved in cell cycle regulation. Therefore, it may have a risk of harm to the fetus if used during pregnancy. Palbociclib has been shown to be fetotoxic in pregnant animals. In rats, an increased incidence of skeletal changes (increased frequency of appearance of ribs on the seventh cervical vertebra) was observed at a specific dose of ≥100 mg/kg/day. A decrease in fetal body weight was observed when the mother received a toxic dose of 300 mg/kg/day in rats (3 times the human clinical exposure determined based on AUC, respectively), and an increase in the incidence of skeletal changes, including the appearance of small phalanges on the anterior extremities, was observed when the mother received a toxic dose of 20 mg/kg/day in rabbits (4 times the human clinical exposure determined based on AUC, respectively). In animal reproductive studies, administration of palbociclib to pregnant female rats and rabbits during organogenesis caused embryofetal toxicity at maternal exposure levels ≥4 times the exposure achieved at human clinical doses (based on AUC).
Manufacturer Palbocent
The manufacturer of Palbocent is the large pharmaceutical company Incepta Pharmaceuticals Limited. The pharmaceutical giant's headquarters is located in Dhaka, Bangladesh. The company's activities are based on the production and sale of generic medicinal products. Incepta's product range includes antitumor, antiviral agents and medications for the treatment of the consequences of injuries and diseases. Medicines are available in various pharmaceutical forms - from tablets to ointments. The current chairman of the pharmaceutical company is Abdul Muqtadir.
the drug Palbocent in a stationary pharmacy in Russia. Wholesale supplies of medicines from the state of Bangladesh are not carried out. But the pharmaceutical giant operates under an international license. This allows you to purchase the company’s products legally in most of the world.
You can order the drug via the Internet . To avoid buying counterfeits, purchasing potent drugs from unofficial sellers is not recommended. When purchasing medicines on the InApteka website, the client will receive certificates confirming the quality and authenticity of the goods.
Reviews of the drug Palbocent
Before purchasing an antitumor drug, you should pay attention to reviews from other patients. Having learned the opinion of those who have undergone therapy, you can prepare in advance for the specifics of treatment and decide on the choice of the manufacturer of the medicine.
Most reviews of Palbocent are positive. As advantages of therapy, patients note improvement in the dynamics of the disease, reduction in tumor size and stable remission.
A negative aspect of taking Palbociclib is the side effects, as patients call them on thematic forums and on social networks. Side effects can be quite severe, so it is important that treatment is carried out under the strict supervision of a specialist.