Relevance
In February 2021, the French National Medical Agency (ANSM) recommended temporarily stopping the use of docetaxel in patients with infiltrative non-metastatic breast cancer.
French pharmacovigilance has previously reported potential serious adverse events associated with the use of Taxam. Taxams (docetaxel and paclitaxel) occupy an important place in the treatment of certain malignant neoplasms, for which there is sometimes no alternative treatment method. This class of drugs, like many others, have severe side effects.
On July 5, 2021, a safety report on the drug was presented on the ANSM website.
Research results
- The results of the studies indicate that serious adverse events such as colitis, septic shock and death remain rare over 20 years of use of the drug (approximately 600,000 patients were treated during this period), their incidence is 1 case per 10,000 patients.
- An analysis of reports to French pharmacovigilance identified 47 deaths associated with enterocolitis or septic shock between 1996 and February 2021. These data were transferred to the European Medicines Agency.
Pharmacological properties of the drug Docetaxel
a cytostatic semi-synthetic agent of the taxoid group, which is obtained from the biomass of yew needles. Promotes the accumulation of tubulin in microtubules and prevents their disintegration, which causes disruption of the mitosis phase and interphase processes in tumor cells. After a single intravenous administration at a dose of 100 mg/m2 of body surface, the maximum concentration in blood plasma is 3.7 μg/ml. The average values of systemic clearance and equilibrium volume of distribution are 21 l/h per 1 m2 and 113 l, respectively. Binding to blood plasma proteins is more than 90%. About 6% of the administered dose is excreted in the urine, 75% in the feces, mainly in the form of metabolites, and a small part is excreted unchanged.
Safety Warnings
- It should be noted that docetaxel and paclitaxel occupy an important place in the treatment of cancer and can significantly reduce mortality.
- ANSM strongly recommends that specialists and patients pay attention to the development of such side effects as neutropenia, enterocolitis, neuropathy and hypersensitivity reactions.
At the same time, the European Pharmacological Regulatory Authority (PRAC) notes that in the last 2 years there has been no increase in the frequency of side effects during docetaxel therapy; in addition, all adverse events recorded in recent years were known earlier. However, a re-discussion of the results is expected in the near future drug safety studies.
It is important to note that French pharmacovigilance plans to study the incidence of adverse events with paclitaxel, which is an alternative to docetaxel in the treatment of breast cancer.
Source:
ANSM. Docetaxel: levée de la recommandation d'éviter son utilisation dans le cancerdu sein et renforcement de l'encadrement des pratiques.
Docetaxel
Treatment with Docetaxel should only be carried out under the supervision of a physician experienced in administering antitumor chemotherapy in a specialized hospital setting.
To prevent hypersensitivity reactions, as well as to reduce fluid retention, all patients receiving Docetaxel (except for patients with prostate cancer, recommendations for premedication for which see below), in the absence of contraindications, before its administration, are premedicated with a glucocorticosteroid, for example, dexamethasone orally at a dose of 16 mg/day (8 mg twice daily) for 3 days, starting 1 day before Docetaxel administration.
In patients with prostate cancer receiving concomitant treatment with prednisone or prednisolone, premedication with dexamethasone at a dose of 8 mg is performed 12, 3 and 1 hour before the start of Docetaxel administration.
To reduce the risk of hematological complications, prophylactic administration of granulocyte colony-stimulating factor (G-CSF) is recommended.
The drug Docetaxel is administered intravenously over 1 hour once every 3 weeks.
Breast cancer (BC)
Adjuvant therapy
For adjuvant therapy of operable breast cancer with regional lymph node involvement and operable breast cancer without regional lymph node involvement, the recommended dose of Docetaxel is 75 mg/m2 1 hour after administration of doxorubicin (50 mg/m2) and cyclophosphamide (500 mg/m2) every 3 weeks ( TAS scheme). A total of 6 cycles (see also further “Dose adjustment during chemotherapy”).
For adjuvant treatment of patients with operable breast cancer with tumor overexpression of HER2, the following doses of Docetaxel are recommended.
Chemotherapy according to the AS TN regimen
-AS (cycles 1-4): doxorubicin (A) 60 mg/m2 followed by cyclophosphamide (C) 600 mg/m2 every 3 weeks, 4 cycles.
-TN (cycles 5-8): docetaxel (T) 100 mg/m2 once every 3 weeks, 4 cycles and trastuzumab (N) administered weekly according to the following schedule:
-cycle 5 (starts 3 weeks after the last AC cycle):
day 1: trastuzumab 4 mg/kg (loading dose),
day 2: docetaxel 100 mg/m2,
days 8 and 15: trastuzumab 2 mg/kg;
-cycles 6-8:
day 1: docetaxel 100 mg/m2 and trastuzumab 2 mg/kg,
days 8 and 15: trastuzumab 2 mg/kg.
- Three weeks after day 1 of cycle 8: trastuzumab 6 mg/kg every 3 weeks. Trastuzumab is administered for a total of 1 year.
Locally advanced or metastatic breast cancer
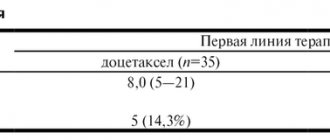
For locally advanced or metastatic breast cancer, docetaxel 75 mg/m2 is administered in combination with doxorubicin 50 mg/m2 as first-line therapy; As a 2nd line therapy, the recommended dose of docetaxel in monotherapy is 100 mg/m2.
For the combination drug Docetaxel plus trastuzumab
The recommended dose of Docetaxel is 100 mg/m2 every 3 weeks with weekly trastuzumab. The initial intravenous infusion of docetaxel is given the day after the first dose of trastuzumab. Subsequent doses of docetaxel are administered immediately after completion of the intravenous infusion of trastuzumab (if the previous dose of trastuzumab is well tolerated). For information on dosage and route of administration of trastuzumab, see the trastuzumab prescribing information.
When combined with capecitabine
The recommended dose of docetaxel is 75 mg/m2 every 3 weeks, and capecitabine is 1250 mg/m2 orally twice daily (within 30 minutes after meals) for 2 weeks followed by a one-week rest period. To calculate the dose of capecitabine according to body surface area, see the capecitabine prescribing information.
Non-small cell lung cancer
In patients who have not previously received chemotherapy, the following treatment regimen is recommended: docetaxel 75 mg/m2 over 30-60 minutes or carboplatin (AUC 6 mg/ml/min) over 30-60 minutes.
For treatment after failure of platinum-based chemotherapy, docetaxel monotherapy at a dose of 75 mg/m2 is recommended.
Metastatic ovarian cancer
For 2nd line treatment of ovarian cancer, a docetaxel dose of 100 mg/m2 every 3 weeks in monotherapy is recommended.
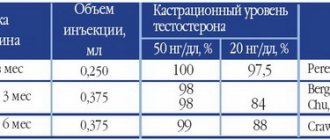
Prostate cancer
For the treatment of patients with prostate cancer, the recommended dose of Docetaxel is 75 mg/m2 once every 3 weeks. Prednisone or prednisolone is prescribed for a long time at 5 mg orally 2 times a day.
Stomach cancer
For the treatment of gastric cancer, the recommended dose of Docetaxel is 75 mg/m2 as a one-hour infusion followed by cisplatin 75 mg/m2 over 1-3 hours (both drugs only on the first day of each chemotherapy cycle). Upon completion of the administration of cisplatin, a 24-hour infusion of fluorouracil 750 mg/m2/day is carried out for 5 days. Treatment is repeated every 3 weeks. Patients should receive premedication with antiemetics and appropriate fluid supplementation (hydration) when receiving cisplatin. To reduce the risk of hematological toxicity (see below, “Dose adjustment during chemotherapy”), administration of G-CSF is indicated for prophylactic purposes.
Head and neck cancer
Patients should be premedicated with antiemetics and given adequate hydration (before and after cisplatin administration). The development of neutropenic infections should be prevented. All patients receiving treatment regimens containing Docetaxel received prophylactic antibiotics.
Induction chemotherapy followed by radiation therapy.
For induction therapy for locally advanced unresectable squamous cell carcinoma of the head and neck, the recommended dose of Docetaxel is 75 mg/m2 as a one-hour intravenous infusion followed by cisplatin at a dose of 75 mg/m2 over 1 hour (both drugs are administered only on the first day of each chemotherapy cycle). After this, a continuous intravenous infusion of fluorouracil is carried out for 5 days. This regimen is repeated every 3 weeks for 4 cycles. After chemotherapy, patients should undergo radiation therapy.
Induction chemotherapy followed by chemoradiotherapy
For induction therapy of locally advanced squamous cell carcinoma of the head and neck (technically unresectable, with a low likelihood of surgical cure, or with a decision to preserve the organ), the recommended dose of Docetaxel is 75 mg/m2 as a one-hour intravenous infusion followed by a 0.5 to 3-hour intravenous infusion an infusion of cisplatin 100 mg/m2 (both drugs are administered only on the first day of each chemotherapy cycle) followed by a continuous intravenous infusion of fluorouracil at a dose of 1000 mg/m2/day from days 1 to 4. This treatment regimen is repeated every 3 weeks for a total of 3 cycles. After chemotherapy, patients should undergo chemoradiotherapy. For information about dosage adjustments of cisplatin and fluorouracil, see the instructions for use of these drugs.
Dose adjustment during chemotherapy
General recommendations
Docetaxel should be administered when the peripheral blood neutrophil count is ≥1500/µl. In the case of febrile neutropenia, a decrease in the number of neutrophils < 500 / μl for more than one week, severe or cumulative (increased with repeated administrations) skin reactions, or severe peripheral neuropathy during docetaxel therapy, its dose for subsequent administrations should be reduced from 100 mg /m2 to 75 mg/m2 and/or from 75 mg/m2 to 60 mg/m2. If such reactions persist even at a docetaxel dose of 60 mg/m2, treatment should be discontinued.
Combination therapy including the drug Docetaxel for the treatment of breast cancer
Adjuvant therapy for breast cancer
For patients with breast cancer receiving adjuvant therapy with Docetaxel in combination with doxorubicin and cyclophosphamide (TAC regimen), G-CSF is recommended for primary prevention. For patients who have experienced febrile neutropenia or a neutropenic infection, the dose of Docetaxel should be reduced to 60 mg/m2 in all subsequent cycles. In patients who have developed grade 3 or 4 stomatitis, it is necessary to reduce the dose of docetaxel to 60 mg/m2.
The drug Docetaxel in the chemotherapy regimen AS TN
In operable breast cancer with tumor overexpression of HER2 after an episode of febrile neutropenia or infection during adjuvant therapy according to the AS TN regimen, it is necessary to use G-CSF for prophylactic purposes in all subsequent cycles, and the dose of Docetaxel in the AS TN regimen should be reduced from 100 mg /m2 up to 75 mg/m2.
Since in clinical practice the development of neutropenia was observed during the first cycle of chemotherapy, the neutropenic risk and currently generally accepted recommendations should be taken into account and, if necessary, G-CSF should be used.
In the case of stomatitis of grade 3 or 4 severity, the dose of Docetaxel in the AS TN regimen should be reduced from 100 mg/m2 to 75 mg/m2.
To adjust the dose of trastuzumab, see the information in the trastuzumab prescribing information.
Docetaxel in combination with capecitabine
To adjust the dose of capecitabine when combined with Docetaxel, see the instructions for medical use of capecitabine.
When using Docetaxel in combination with capecitabine, if grade 2 toxicity occurs for the first time and persists at the start of the next cycle, the next treatment cycle may be delayed until the toxicity is reduced to grade 0 to grade 1, with 100% of the original dose administered during the next treatment cycle. doses. In patients with recurrent grade 2 toxicity or first grade 3 toxicity at any time during the cycle, treatment is delayed until toxicity has decreased to grade 0-1, then treatment with Docetaxel is resumed at a dose of 55 mg/m2.
If any subsequent toxicity occurs or any grade 4 toxicity occurs, docetaxel should be discontinued.
Combination therapy, including the drug Docetaxel, for non-small cell lung cancer, the drug Docetaxel in combination with cisplatin or carboplatin
In patients who initially received docetaxel 75 mg/m in combination with cisplatin or carboplatin and whose platelet count in the previous cycle decreased to 25,000/μL, or in patients who developed febrile neutropenia, or in patients with severe non-hematological toxicity , the dose of docetaxel in subsequent cycles should be reduced to 65 mg/m2.
To adjust the dose of cisplatin, see the instructions for use of cisplatin.
Docetaxel in combination with cisplatin and fluorouracil for gastric cancer and head and neck cancer
Patients receiving Docetaxel in combination with cisplatin and fluorouracil should receive antiemetics and adequate fluid supplementation (hydration) in accordance with current generally accepted recommendations. To reduce the risk of complicated neutropenia, G-CSF should be used.
If, despite taking G-CSF, episodes of febrile neutropenia, prolonged neutropenia or neutropenic infection occur, the dose of Docetaxel is reduced from 75 to 60 mg/m2. With the subsequent development of episodes of complicated neutropenia, it is recommended to reduce the dose of Docetaxel from 60 mg/m2 to 45 mg/m2. With the development of grade 4 thrombocytopenia, it is recommended to reduce the dose of Docetaxel from 75 mg/m2 to 60 mg/m2. Subsequent cycles with docetaxel are possible when neutrophil counts > 1500/µl and platelet counts > 100,000/µl. If these toxic manifestations persist, treatment should be discontinued.
Recommended dose adjustments for toxicity in patients receiving Docetaxel in combination with cisplatin and fluorouracil (FU):
| Toxicity | Correction of dosage regimen |
| Diarrhea grade 3 | First episode: reduce FU dose by 20%. Repeated episode: reduce Docetaxel dose by 20%. |
| Diarrhea grade 4 | First episode: reduce the dose of Docetaxel and FU by 20%. Repeated episode: stop treatment. |
| Stomatitis/mucositis grade 3 | First episode: reduce FU dose by 20%. Repeated episode: Stop FU only in all subsequent cycles. Third episode: reduce the dose of Docetaxel by 20%. |
For recommendations on dosage adjustments of cisplatin and fluorouracil, see their prescribing information.
In patients with head and neck squamous cell carcinoma who develop complicated neutropenia (including prolonged neutropenia, febrile neutropenia, or infection), prophylactic use of G-CSF is recommended in all subsequent cycles (eg, days 1 to 15 of the cycle).
Special patient groups
Children
The safety and effectiveness of Docetaxel in children have not been studied. There is limited experience with docetaxel in children. The effectiveness and safety of Docetaxel for nasopharyngeal cancer in children and adolescents from 1 month to 18 years have not yet been established. Docetaxel has not been used in children for the following indications: breast cancer, non-small cell lung cancer, prostate cancer, gastric cancer and head and neck cancer, with the exception of poorly differentiated nasopharyngeal cancer (types I and II).
Elderly patients
Based on population pharmacokinetic analysis data, there are no special instructions for the use of Docetaxel in the elderly. In patients 60 years of age and older, when Docetaxel is combined with capecitabine, a 25% reduction in the dose of capecitabine is recommended (see instructions for use of capecitabine).
Patients with liver failure
Based on the pharmacokinetic data obtained for docetaxel in monotherapy at a dose of 100 mg/m2, in patients with ALT and/or AST activity > 1.5 ULN or alkaline phosphatase activity > 2.5 ULN, the recommended dose of Docetaxel is 75 mg/m2 . In patients with an increase in the concentration of bilirubin in the blood (> 1 ULN) and/or with an increase in the activity of ALT and AST (> 3.5 ULN) in combination with an increase in the activity of alkaline phosphatase (> 6 ULN), a dose reduction cannot be recommended and not Docetaxel should be used without strict indications. The combination of Docetaxel with cisplatin and fluorouracil in the treatment of patients with gastric cancer was not used in patients with increased ALT and/or AST activity (> 1.5 ULN) in combination with increased alkaline phosphatase activity (> 2.5 ULN) and increased bilirubin concentrations in the blood (> 1 ULN).
In such patients, no dose reduction can be recommended and docetaxel should not be used unless strictly indicated.
There are currently no data regarding the use of Docetaxel in combination with other drugs in patients with impaired liver function.
Patients with impaired renal function
There are no data on the use of docetaxel in patients with severe renal impairment.
Preparation of infusion solution
Concentrate for preparing solution for infusion 20 mg/0.5 ml:
the actual content in the bottle is 24.4 mg/0.61 ml, which allows you to compensate for the loss of liquid when preparing a pre-mixed solution due to foaming, adhesion to the walls of the bottle and the presence of “dead space”. Thus, excess drug in the vial ensures that after reconstitution of its contents with the supplied diluent, the minimum volume of premixed solution drawn up will be 2 ml containing 10 mg/ml docetaxel, corresponding to 20 mg (the dose indicated on the vial label).
Concentrate for solution for infusion 80 mg/2 ml:
the actual content in the vial is 94.4 mg/2.36 ml, which makes it possible to compensate for liquid losses during the preparation of a pre-mixed solution due to foaming, adhesion to the walls of the vial and the presence of “dead space”. Thus, the excess drug in the vial ensures that, after diluting its contents with the supplied diluent, the minimum volume of the premixed solution drawn up will be 8 ml containing 10 mg/ml docetaxel, corresponding to 80 mg (the amount indicated on the vial label),
a) Preparation of a pre-mixed solution of Docetaxel (with a docetaxel concentration of 10 mg/ml)
The concentrate for preparing a solution for infusion of the drug Docetaxel must first be diluted in the supplied solvent. If the bottles with the drug and solvent were stored in the refrigerator, then before dilution they must be kept at room temperature (below 25 ° C) for 5 minutes. The entire contents of the bottle with the solvent are drawn under aseptic conditions using a needle into a syringe (the bottle is placed slightly at an angle) and injected into the bottle with Docetaxel.
After removing the needle, the contents of the bottle with the resulting mixture are mixed by turning the bottle upside down for 45 s (do not shake!) and left for 5 minutes at room temperature, after which the solution is checked for homogeneity and transparency (the presence of foam even after 5 minutes is the norm from - for the content of polysorbate 80 in the composition of the drug). The premix contains docetaxel at a concentration of 10 mg/ml and should be used immediately to prepare an infusion solution.
b) Preparation of solution for infusion.
The required volume of pre-mixed solution according to the required dose is injected into an infusion bag or bottle containing 250 ml of 5% dextrose solution or 0.9% sodium chloride solution. If the required dose of docetaxel exceeds 200 mg, it should be diluted in a larger volume of solution for infusion so that the docetaxel concentration does not exceed 0.74 mg/ml. The contents of the infusion bag or bottle should be mixed using a rotational motion. Infusion of the resulting solution should be carried out no later than 4 hours after preparation (including 1 hour of administration) when stored at room temperature (below 25 ° C) and normal lighting conditions. Docetaxel premixed solution and solution for infusion, like any other parenteral drug, must be inspected before administration; If there is sediment, the solution should be destroyed.
Residues of the drug and all materials used for its dilution and administration should be disposed of in accordance with standard regulations.