Asthenia means weakness that occurs in the absence of exertion, lasts for a long time and does not go away even after a long rest. The main difference between asthenia and physiological fatigue is the ineffectiveness of sleep and its chronic course. In foreign literature, the term “chronic fatigue syndrome” is sometimes used to refer to asthenia.
Every fifth (10-25%) patient seeking medical help complains of asthenia [1]. In many cases, it is possible to establish a connection between asthenia and the effects of pathogenic biological or psychological factors. In particular, asthenia is a characteristic complaint of patients with organic diseases of the brain (chronic cerebrovascular insufficiency, post-traumatic encephalopathy, etc.) [1-3]. Such patients are especially susceptible to rapid mental exhaustion. Prescribing nootropic drugs, normalizing metabolic processes in the central nervous system, improves the well-being of such patients.
In many cases, asthenia is accompanied by mild to moderate cognitive impairment, autonomic dysfunction, emotional disturbances, including severe depression and anxiety. Thus, it was shown that 28% of patients with long-term (more than 6 months) current asthenia develop severe anxiety-depressive syndrome [3]. According to one of the multicenter placebo-controlled randomized studies [4], cytoflavin not only reduced the severity of asthenia in patients with asthenoneurotic syndrome against the background of chronic cerebral ischemia, but also improved cognitive functions and quality of life.
According to research by D.I. Laseeva and O.V. Dikova [5], cytoflavin had a positive effect on the emotional state in patients with eczema. In our previous study [6], we also observed more pronounced positive dynamics in women with depression due to organic brain disease who received cytoflavin as an additional therapy, compared with the control group (the study is being prepared for publication). In addition, in the same group of patients, we observed a normalization of autonomic disorders under the influence of cytoflavin.
Cytoflavin produced by NTFF POLYSAN LLC includes succinic acid, riboxin, nicotinamide and riboflavin, which are important components of normal metabolic processes in the brain. The drug is well tolerated and is used for encephalopathies of various origins (toxic, posthypoxic), for acute and chronic cerebrovascular accidents [7, 8]. In acute conditions, cytoflavin is used intravenously, and in chronic diseases it is prescribed in tablet form, 2 tablets 2 times a day for a course of at least 25 days [3].
The purpose of the study was to study the effect of cytoflavin as an additional therapy in patients with organic emotionally labile (asthenic) disorder.
Material and methods
The present study was observational.
The study included 100 patients, 49 men and 51 women, with organic emotionally labile (asthenic) disorder (F06.6 according to ICD-10), who underwent inpatient treatment at the Scientific and Practical Center for Psychoneurology of the Moscow Department of Health in 2012-2013.
The criteria for inclusion in the study were: severe asthenic disorders (75 or more points on the asthenic state scale) lasting at least 3 months as the main reason for seeking medical help; development of an asthenic state against the background of an organic brain disease due to severe perinatal pathology with developmental delay, chronic cerebral circulatory failure or traumatic brain injury; age over 25 years and under 60 years; complete secondary or higher education; absence of neurometabolic therapy for 3 months before the study. Exclusion criteria were: psychotic disorders or suicidal intentions; uncorrectable visual or hearing impairment; serious neurological or somatic diseases; alcoholism or drug addiction; pregnancy; history of allergic reactions or hypersensitivity to cytoflavin.
All patients were divided into two groups - the main and control groups of 50 people in each. Patients in the main group received cytoflavin in addition to basic therapy.
Cytoflavin was prescribed twice a day, 2 tablets. The duration of therapy was 3-4 weeks. Patients in the control group received only basic therapy. Basic therapy included antidepressants, vascular drugs, and in some cases drugs with sedative and/or antipsychotic effects. All patients were consulted by psychologists and psychotherapists, took courses in hydro- and electrophysiotherapy, received massage of the collar area, and did physical therapy.
Tolerability of cytoflavin was assessed based on side effects in two groups of patients.
All patients underwent an EEG to monitor high-amplitude paroxysmal τ-activity in the central leads or the presence of epileptic brain activity.
The effect of cytoflavin on the symptoms of the disease was assessed by the dynamics of asthenia indicators, the results of cognitive tests, changes in the level of depression, anxiety, autonomic disorders and quality of life after the course of treatment in comparison with the condition of patients in the first days of hospital stay, depending on taking cytoflavin.
The severity of asthenia symptoms was assessed using the asthenic state questionnaire. The technique was developed by L.D. Malkova and adapted by T.G. Chertovaya on the basis of clinical and psychological observations and the MMPI questionnaire. The questionnaire contains 30 questions, the answers to which are ranged from 1 point (no, incorrect) to 4 points (absolutely true). An indicator of 51-74 points is interpreted as mild asthenia, 75-100 points - moderate asthenia, 101-120 points - severe asthenia.
The severity of depression and anxiety was assessed using the Hospital Depression and Anxiety Scale and the Beck Depression Inventory [9]. The Hospital Scale consists of 14 items, 7 of which assess symptoms of depression and 7 of which assess symptoms of anxiety. The Beck Inventory consists of 21 items assessing symptoms of depression.
Autonomic disorders were assessed using the Autonomic Disorders Scale [10]. The scale consists of 2 parts. The Objective Autonomic Disorders subscale consists of 13 items and is completed by the clinician. The subjective autonomic disorders subscale consists of 11 items and is completed by the patient.
Cognitive function was examined using the Montreal Cognitive Assessment Scale (MoCa) [11]. The scale consists of 12 tasks assessing attention and concentration, memory, visual-constructive skills, abstract thinking, and speech functions. The maximum number of points is 30.
Quality of life was assessed using the SF-36 questionnaire (36-item short form Health Survey) [1, 12]. The questionnaire contains 36 items, on the basis of which 8 subscales are formed: physical functioning, role limitations due to physical problems, physical pain, general health, energy, social functioning, role limitations due to emotional problems, mental health.
Statistical analysis of the obtained data was carried out using the SPSS17 software package. The dynamics of psychological and other indicators were assessed using the Repeated measures ANOVA test, in which the grouping factor was the presence or absence of cytoflavin therapy. Since in a previous study we found differences in the severity of the effect of cytoflavin in men and women [6], in this work we included gender in the analysis as a second grouping factor. If there were between-group differences in testing, baseline test performance was also included in the analysis as a covariate.
Prevention of recurrent stroke
The reasons that led to the occurrence of a stroke most often do not disappear anywhere and continue to affect a person. The risk of recurrent stroke depends on their strength and combinations. Prevention of recurrent stroke is called secondary. List of conditions that people pay attention to first:
- Arterial hypertension is the main risk factor for stroke. It increases his risk by 5 times;
- diabetes;
- smoking;
- coronary heart disease (the risk increases by 2-4 times);
- atrial fibrillation (increases the risk by 3-5 times);
- hyperlipidemia (high levels of “bad” cholesterol);
- thrombocytosis;
- overweight.
Accordingly, it is necessary to correct these conditions and bring them back to normal to reduce the risk of recurrent stroke. Drug therapy is only part of the treatment. Diet, exercise, and giving up bad habits are important.
Antihypertensive drugs
It is recommended to reduce blood pressure, even if it is raised very slightly or within the normal range: “upper” 120-139 mmHg, “lower” 80-89 mmHg. So a decrease of 5 mmHg. helps reduce the development of stroke by 30%.
Diet, exercise, and giving up bad habits are important in preventing a recurrent stroke.
The superiority of some groups of antihypertensive drugs over others has not been proven. When prescribing, the doctor has to take into account the individual characteristics of the patient, compatibility with other drugs, and minimizing side effects. At the same time, for patients after a stroke, it is important not only to reduce blood pressure, but also to stabilize it as much as possible, even if slightly above the target values. For this use:
- Amlodipine - long-acting calcium channel blockers;
- Perindopril, Diroton, Renitek - angiotensin-converting enzyme inhibitors;
- Lozap, Cozaar, Valsartan - sartans, angiotensin receptor blockers;
- Hypothiazide, Indap are diuretics.
Drugs that prevent blood clots
With various arrhythmias, the risk of thrombosis and stroke increases up to 4 times. Anticoagulants and antiplatelet agents can be used to prevent these conditions:
- Warfarin;
- Thrombo ACC;
- Plavix;
- Chimes.
Taking this group of drugs is usually long-term, one might say lifelong.
Statins
They help not only fight atherosclerosis and high cholesterol levels, but also stabilize the surface of already formed plaques, reduce the level of inflammation in the vascular wall, which will also reduce the risk of thrombosis:
- Mertenil;
- Atoris;
- Basil.
Read more about statins in the article.
results
In the table
The characteristics of the patients are presented, including group average indicators on the scales studied.
The distribution of men and women, mean age and level of education did not differ between the groups of patients receiving cytoflavin and the control group.
The average group indicators of asthenia were: 80.3±2.6 and 82.3±3.8 points in the main and control groups, respectively. However, despite the small differences between the group average indicators, they were significant with less severity of asthenia in the main group. At the same time, the level of depression according to Beck and the severity of autonomic disorders according to a questionnaire filled out by a doctor were greater in the group of patients receiving cytoflavin. Indicators of depression and anxiety, identified using the Hospital Depression and Anxiety Scale, as well as the severity of subjective autonomic disorders did not differ in the study and control groups. The frequency of paroxysmal activity according to EEG examination was low in the examined population of patients with asthenia of organic nature. Thus, paroxysmal τ-activity upon admission was detected in 3 patients receiving cytoflavin and in 5 patients in the control group. During re-examination before discharge, paroxysmal τ-activity was detected in the same 8 patients. Epileptic activity was not detected in any case, either during the initial or re-examination.
Cytoflavin was well tolerated; 16 patients receiving cytoflavin and 15 patients in the control group noted moderate sedative effects of standard antidepressant therapy (drowsiness, mild lethargy, slight dizziness). No other complaints were identified in the group of patients receiving Cytoflavin. There were also no new cases of epileptic activity or paroxysmal high-amplitude activity on the EEG recorded after the course of treatment.
The effect of cytoflavin on the level of asthenia and cognitive functions
After an inpatient course of treatment, the level of asthenia decreased to 57.3±6.8 points in the main group and 58.4±6.8 points in the control group, while the positive dynamics of this indicator was highly reliable ( p
<0.001). At the same time, the magnitude of changes in the severity of asthenia symptoms in accordance with the indicators of the asthenic state questionnaire did not differ in the two groups, either with or without using the baseline level of asthenia as a covariate.
The results of the Montreal Cognitive Impairment Scale tests also significantly improved in both examined groups of patients ( p
<0.001).
However, no effect of the drug was detected in the general group of subjects ( p
= 0.224).
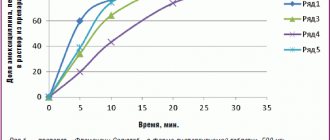
It is important to note that in 53 subjects the total score on the Montreal scale already during the initial examination reached the “ceiling” value of 27 to 30 points, i.e. any dynamics of this indicator during repeated examination was impossible. Accordingly, we re-analyzed the dynamics of the results of the cognitive tests of the Montreal scale depending on the drug intake in a group of 35 patients who completed these tests with a score of 21 to 26 points. A significant improvement in the results of performing cognitive tests before discharge compared to the first days of hospitalization was also found in this group of patients ( p
<0.001). It is important that patients receiving cytoflavin (11 patients) demonstrated a more pronounced improvement in the results of cognitive tests upon re-examination compared to the group of patients (24 people) receiving standard therapy (Fig. 1).
Figure 1. Dynamics of the total score on the Montreal Cognitive Impairment Scale depending on cytoflavin intake. Here and in Fig. 2-4: solid line – main group of patients, dotted line – control group. When excluding from the analysis patients who performed Montreal scale tests at a level of 26 points, this trend reached significance ( p
= 0.009).
Effect of cytoflavin on emotional disorders
In both groups of patients, a decrease in the level of depression on the Beck depression scale was recorded before discharge ( p
<0.001).
A more pronounced decrease in depression was found in the group of patients receiving cytoflavin compared to the control group ( p
= 0.004).
However, patients receiving the drug were significantly different from the control group in higher levels of depression during hospitalization ( p
= 0.011).
Thus, in 8 patients from the main group, depression exceeded 35 points on the Beck scale, while in the control group not a single patient had such a high score. In addition, in 4 patients characterized by very low depression scores on admission (3-6 points), dynamics was impossible. Accordingly, we re-analyzed the effect of cytoflavin on the severity of depression after excluding 8 patients with Beck scale scores of 40-47 (Fig. 2)
.
Figure 2. Dynamics of depression according to the Beck scale depending on cytoflavin intake. The trend toward a more pronounced decrease in depression in patients receiving Cytoflavin compared with the control group remained significant in repeated analysis ( p
= 0.045). It should be noted that the positive effect of cytoflavin on the dynamics of depression was more pronounced in men, but gender differences in this indicator did not reach statistical significance.
Depression and anxiety, as measured by the Hospital Depression and Anxiety Scale, also decreased significantly before discharge in both groups of patients ( p
<0.001), however, the decrease in anxiety level was significantly greater in the group that did not receive cytoflavin (
p
= 0.008) compared with patients treated with cytoflavin
(Fig. 3)
.
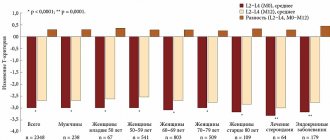
Figure 3. Dynamics of depression and anxiety according to the Hospital Depression and Anxiety Scale depending on cytoflavin intake. The dynamics of anxiety depending on the intake of cytoflavin did not differ between men and women; in other words, a more pronounced decrease in anxiety in patients who did not receive cytoflavin was observed both in the group of men ( p
= 0.043) and in the group of women (
p
= 0.079).
Effect of cytoflavin on autonomic disorders
The severity of objective and subjective autonomic disorders significantly decreased in the examined group of patients with emotionally labile disorder after an inpatient course of treatment compared to the period before treatment ( p
<0.001).
Patients treated with cytoflavin showed a tendency towards a more pronounced normalization of autonomic functions according to the corresponding questionnaire compared to patients not treated with cytoflavin ( p
= 0.076). This trend was expressed to the same extent in both the subgroup of men and the subgroup of women.
As noted above, autonomic disorders, as examined by a physician, were significantly more pronounced in the group of patients receiving Cytoflavin. However, as can be seen in Fig. 4
, there were no intergroup differences in the dynamics of objective symptoms of autonomic dysfunction depending on the intake of cytoflavin (
p
= 0.24).
Figure 4. Dynamics of autonomic disorders according to the questionnaire by A.M. Vein depending on the intake of cytoflavin.
Effect of cytoflavin on quality of life
Group mean scores on all 8 SF-36 subscales improved at re-examination compared with examination at admission ( p
<0.001), but these changes did not depend on cytoflavin intake.
Discussion
The results of the study indicate that cytoflavin at a dose of 4 tablets per day (in 2 doses) has a positive effect on cognitive functions in patients with organic brain damage. Data from a previous study [6] regarding the positive effect of cytoflavin on depressive symptoms in patients with severe asthenia were confirmed. At the same time, in contrast to a multicenter study that included patients with cerebrovascular disease [4], we did not detect an additional effect of cytoflavin on the overall positive dynamics of asthenic symptoms in patients with emotionally labile disorder. We observed a pronounced regression of asthenia symptoms regardless of cytoflavin intake. It should be noted that the average age of the examined patients was significantly lower compared to the specified multicenter study [6], which included patients with cerebrovascular disease and demonstrated a more pronounced reduction in asthenia during treatment with cytoflavin. It can be assumed that the effectiveness of cytoflavin manifests itself mainly in patients with reduced neurotrophic resources. Indirect confirmation of this hypothesis is a more pronounced improvement in cognitive status while taking cytoflavin in patients with cognitive impairment compared to the control group in our study.
In patients treated with cytoflavin, a significantly more pronounced decrease in the Beck depression score and normalization of autonomic regulation were found compared to the control group. Interestingly, in our previous study involving patients with organic depression, a similar effect of cytoflavin was observed only in a subgroup of women. In the present study, the effect of cytoflavin was more pronounced in the subgroup of men with emotional labile disorder compared to the subgroup of women. Our data are consistent with previous experimental and clinical studies demonstrating the antidepressant effect of nootropics [13–15]. Numerous neuroimaging and experimental studies have revealed a deficit in neurotrophic processes in patients with chronic depression, leading to hypotrophic changes in the frontal cortex and other brain structures in such patients [16-18]. Thus, the effectiveness of prescribing cytoflavin as an additional method of treating depression seems pathogenetically justified.
It is well known from clinical practice that most nootropic drugs have a stimulating effect on the functions of the central nervous system. It is likely that the stimulating effect of cytoflavin was the reason for less regression of anxiety symptoms in the group of patients receiving the drug compared to the control group. Accordingly, the possibilities and limitations of nootropic therapy in patients with anxiety disorders require further research.
Thus, the data from the present observational study indicate that cytoflavin is well tolerated by patients with organic emotionally labile (asthenic) disorder and helps to normalize cognitive functions, mood and autonomic regulation in such patients. The effectiveness of cytoflavin as a treatment for asthenia in young patients requires further research.
Stroke and rehabilitation
Stroke is an acute disease that is associated with circulatory disorders and is manifested by such symptoms from the nervous system as:
- motor, speech, sensory, coordination, visual and other disorders;
- general cerebral disorders: changes in consciousness, headache, vomiting for more than 24 hours;
- death in a short period of time.
There are 2 main forms of stroke:
- ischemic (when some part of the brain stops receiving oxygen for various reasons, for example, blockage of the lumen of a vessel with a blood clot);
- hemorrhagic (when a vessel ruptures, blood permeates the brain tissue and non-traumatic damage or subarachnoid hemorrhage occurs).
Rehabilitation after a stroke begins as early as possible. An integrated approach to treatment combines drug therapy, physiotherapy, and training to restore lost functions. There are 3 main areas in pharmacotherapy:
- prevention of relapse, that is, repeated stroke. Typically, 1 in 10 people will have another stroke in the first year;
- treatment of individual symptoms;
- pathogenetic treatment.