Thrombolytic therapy (TLT) is recognized as one of the 10 greatest achievements in cardiology of the 20th century. [1]. Despite the introduction of primary coronary angioplasty for acute myocardial infarction, thrombolysis does not lose its importance, taking into account the logistical characteristics of our country with long distances to specialized invasive centers. On the contrary, a lot of patients are still left without reperfusion interventions at all, so the problem of introducing thrombolysis continues to be relevant for domestic healthcare.
Some historical aspects
In 1933, W. Tillet et al. discovered the ability of streptococcal cultures to lyse blood clots. This was group A β-hemolytic streptococcus, producing a certain “fibrinolytic” substance, which the authors called “streptococcal fibrinolysin” [2]. In 1945, LR Christensen showed that the human blood plasma contains the enzyme plasminogen, which, under the influence of streptococcal fibrinolysin, which he called streptokinase (SK), is converted into the active fibrinolytic enzyme plasmin [3].
In 1948, S. Sherry et al. reported the first experience of using SC in the clinic for the lysis of purulent pleural exudate containing fibrin films [4]. In 1958, A.P. Fletcher et al. published a report on the first intravenous administration of SA to patients with myocardial infarction [5]. For the first time, it was shown that the use of SC in these patients can reduce mortality, so this is a promising approach to the treatment of patients with acute myocardial infarction (AMI).
In parallel, there were attempts to use not plasminogen activator, but already activated plasmin [6]. Domestic scientists under the leadership of G.V. Andreenko and B.A. Kudryashov created a similar drug called “Fibrinolysin” in 1961, which was used in clinical practice for a long time [7]. Above is the “general” path of development of thrombolytic therapy. Naturally, there were also “dead-end” areas along this path. In particular, in parallel with the study of SA as a thrombolytic by group I. Innerfield, trypsin was actively studied [8]. Animal studies (rabbits and dogs) have shown the thrombolytic effectiveness of trypsin when administered intravenously. At the same time, there was a significant decrease in the concentration of fibrinogen in the blood and an increase in prothrombin time. In addition to the thrombolytic effect, a pronounced anti-inflammatory effect was found. After this, clinical trials were carried out on patients with various diseases: thrombophlebitis, arthritis, strokes, coronary thrombosis. Thrombolysis with trypsin was performed in 538 patients (!) [9]. Incl. There were 7 patients with clinical symptoms of acute coronary syndrome, 3 of them with AMI. Among these patients, one died, the rest showed a significant improvement in their condition, which was accompanied by a decrease in the frequency of angina attacks, positive changes in the ECG and biochemical parameters. Thus, the first administration of thrombolytic to patients with AMI was carried out in 1952 by the group of I. Innerfield. Taking into account the high frequency of side effects, especially with rapid administration, which is required for AMI, trypsin has lost out in comparison with SA and is currently not used as a thrombolytic.
Classification of thrombolytic agents
According to the mechanism of action, all thrombolytic agents can be divided into 3 groups [10]:
Direct fibrinolytics, which directly destroy the fibrin molecule. These include the main natural enzyme of the human thrombolytic system, plasmin, its dosage form fibrinolysin, and some fungal proteases.
Plasminogen activators: SA, staphylokinase, tissue plasminogen activator and urokinase-type plasminogen activator.
Indirect fibrinolytics.
Substances of the third group do not cause direct activation of plasminogen and do not have a direct lysing effect on fibrin. They enhance fibrinolysis relatively gently - through the following mechanisms:
- increasing the biosynthesis of plasminogen or its activators (anabolic steroids, nicotinic acid);
- enhancing the release of plasminogen activators from tissues (histamine, bradykinin, heparin, prostaglandins);
- inactivation of natural fibrinolysis inhibitors;
- specific antibodies, salts of heavy metals;
- changes in the structure of fibrinogen or fibrin (Arvin or Ankrod, defibrase, fibrin-specific antibodies).
Of the drugs of the first group, only fibrinolysin was used in clinical practice. An outstanding achievement of Russian cardiology was the intracoronary administration of fibrinolysin for AMI, which was performed for the first time in the world on June 5, 1975 by cardiologists under the leadership of E.I. Chazov [11]. Currently, as a result of the emergence of new, more effective drugs, fibrinolysin has lost its importance.
Indirect fibrinolytics activate fibrinolysis rather weakly and therefore are not used as thrombolytics, especially in acute thrombosis. Only heparin is widely used, but not as an activator of fibrinolysis, but as an anticoagulant. For drug thrombolysis in myocardial infarction, only plasminogen activators are currently used.
Plasminogen activators, in turn, are divided into thrombolytics:
- 1st generation (fibrin-specific: SC and UK);
- 2nd generation (fibrin-specific: alteplase, prourokinase, recombinant staphylokinase);
- 3rd generation (genetically modified: tenecteplase, Purolase, Fortelysin).
SC: start of multicenter clinical trials
The first of these drugs is considered to be SK. SA forms a complex with plasmin, the molecule of which changes and its active center is exposed. The SC–plasminogen complex plays the role of an enzyme in the further conversion of plasminogen to plasmin, and it activates both fibrin-bound and freely circulating plasminogen molecules. As a consequence, plasmin lyses not only fibrin, but also fibrinogen circulating in the blood, which explains the decrease in fibrinogen during thrombolysis. KS is antigenic, therefore titers of antistreptokinase antibodies quickly increase within several days after administration of the drug, making its repeated use ineffective and unsafe.
The most common side effect/complication of KS is hypotension: a decrease in systolic blood pressure to 80 mm Hg. and lower is observed in 30–40% of patients [12]. This hypotension is not a manifestation of an allergic reaction, much less anaphylaxis, as is sometimes explained. SC is a nonspecific thrombolytic. In parallel with the conversion of plasminogen into plasmin, activation of the kallikrein-kinin system occurs, the conversion of bradykininogen into bradykinin, which reduces blood pressure [13, 14]. Bradykinin completely disappears during a single passage through the pulmonary bed, so this hypotensive effect is short-lived and does not pose a threat to the patient’s life. To relieve it, small doses of mezaton or “renal” doses of dopamine are administered as an infusion.
On the contrary, there is an opinion that a decrease in blood pressure is a marker of the effectiveness of TLT. The more effective TLT, the more not only plasmin, but also bradykinin is formed, the more blood pressure should decrease, although this has not been statistically confirmed.
In the 1960s–1970s. Studies have been conducted to select optimal doses and modes of administration of SA. The most common, “classical” method of introducing SA was proposed in 1981 by R. Schroder et al. and consists of an intravenous infusion of 1.5 million units of SC over 60 minutes [15]. This is how thrombolysis was performed in most studies. In the early 1980s.
The first multicenter study of the effectiveness of thrombolysis in AMI, known as GISSI-1, was conducted [16]. This Italian study included 11,806 patients with AMI, half of whom received 1.5 million units of SA per hour during the first 12 hours of illness. The end point of the study was mortality.
For the first time it was shown that:
The use of thrombolysis reduces mortality in AMI.
The effectiveness of thrombolysis depends on the time interval between the onset of the disease and the administration of SA. When starting therapy in the first hour of the disease, in the first 2–3 and 3–6 hours, mortality was 8.2, 9.2 and 11.7%, respectively, versus 14.1% in the control group without TLT. It turns out that the earlier TLT begins, the higher its effectiveness.
These findings were fundamentally confirmed in the ISIS-2 study [17]. More than 17 thousand patients were randomized into 4 groups: SK, aspirin, SK + aspirin and control. It turned out that 5-week mortality in the SC group decreased by 25%, in the aspirin group - by 23%, in the SC + aspirin group - by 42%. Those. In addition to confirming the effectiveness of SC, the high effectiveness of aspirin was demonstrated. The results of the above studies have become the evidence base for the modern treatment strategy for AMI: prescribe TLT, aspirin and heparin as early as possible.
A meta-analysis of the results of studies with angiographic control showed that with the introduction of SA, the rate of coronary artery (CA) reperfusion is on average 44% at 60 minutes of treatment, at 90 – 48%, after 3 hours – 72%, and from 24 hours to 21 days – from 75 to 85%, which is statistically significantly higher than in the control group without thrombolysis [18].
SA or alteplase?
Tissue plasminogen activator (tPA), isolated in the early 1980s, is a protein synthesized by vascular endothelial cells. Unlike SK, which activates plasma plasmingogen, causing a systemic lytic state, tPA converts tissue plasminogen into active thrombin only in the presence of fibrin. Thus, it is fibrin-specific and does not have a pronounced systemic effect, although this fibrin-specificity disappears with increasing doses of the drug. During thrombolysis of tPA, active production of thrombin occurs, which determines the mandatory need to combine tPA with intravenous heparin. An industrial product, alteplase, was created using the DNA recombinant method. Unlike SA, it has a short inactivation period. Its half-life is 4–8 minutes, requiring prolonged administration to maintain therapeutic blood concentrations. In the first trials of alteplase for the treatment of AMI, it was prescribed at a total dose of 150 mg over 3 hours, then the regimen was changed to 100 mg over 90 minutes.
In the 1980‑1990s. Comparative studies of SA and alteplase were carried out. Several studies with angiographic control have shown that a 3-hour infusion of alteplase is significantly more likely to cause coronary artery reperfusion at 60 and 90 minutes of thrombolysis compared with SC [19]. Taking into account the important importance of the rate of coronary reperfusion, it was logical to expect a decrease in mortality in the groups with alteplase, but in the studies TIMI-1 (290 patients), GISSI-2 (10,372 patients), ISSIS-3 (41,299 patients) no significant difference was found in mortality between the SA and alteplase groups. And only in the GUSTO-I study, which included 41,021 patients, it was shown that an accelerated regimen of alteplase administration (100 mg in 90 minutes) reduced 30-day mortality compared with SC: 6.3 versus 7.2%, respectively ( p=0.001), i.e. by 0.9% [20]. It would seem that the advantage of alteplase has been proven.
But such an unambiguous assessment of the results is limited by the following circumstances:
A significant difference in mortality was observed only among patients who were treated in the United States. There was no such difference in other countries [21].
More disabling strokes developed in the alteplase group: 0.72 vs. 0.54% (p=0.03). However, the combined end point (death + stroke) in the alteplase group still remained lower: 6.9 versus 7.8% (p = 0.006). An increased incidence of hemorrhagic strokes with the use of fibrin-specific tPA drugs compared with SK was also noted in a more recent meta-analysis [22].
As part of the GUSTO-I study, a substudy was conducted: 2431 patients underwent angiography. It turned out that effective blood flow (according to TIMI 2-3) in the coronary artery by 90 minutes from the start of TLT in the alteplase group was achieved in 81% of cases, and in the SC group - only in 60%. But after 3 hours, the differences in this indicator were no longer detectable: 74 and 76%, respectively [23]. Thus, SA and alteplase open CAs equally often, but alteplase does it a little faster.
The GUSTO-I study examined the cost/effectiveness ratio of thrombolysis with alteplase compared with SA. One year of a patient’s life saved as a result of thrombolysis not with SA, but with alteplase “costs” $32,678 [24]. This ratio is more effective/beneficial for anterior myocardial infarctions and less effective for lower ones.
Thus, the disadvantages of alteplase compared to SK include a high risk of cerebral hemorrhage, the mandatory need for parallel heparin infusion, and high cost. Therefore, when choosing alteplase for thrombolytic therapy, it is necessary to take into account not only its advantages, but also its disadvantages.
Tenecteplase – a drug for bolus administration
To improve the fibrinolytic characteristics of the drug, modifications of the tPA molecule were created using genetic engineering: reteplase (recombinant plasminogen activator, r-PA), lanoteplase (n-PA) and tenecteplase (TNK-tPA). The most successful of them is the drug tenecteplase (Metalise). It is a molecule with a longer plasma half-life, increased fibrin specificity, and greater resistance to plasminogen activator inhibitor type 1 (PAI-1) compared to natural tPA, so the undoubted advantage of tenecteplase is the possibility of its single bolus administration. The ASSENT-1 study determined the most optimal dose of this drug: 30–50 mg, depending on the patient’s weight [25].
The ASSENT-2 study compared alteplase and tenecteplase using this dose. Although the incidence of non-cerebral hemorrhages and the need for blood transfusions was slightly lower in the tenecteplase group than in the alteplase group - 26.4 versus 28.9% (p = 0.0003) and 4.2 versus 5.5% (p = 0.0002), respectively , mortality within 30 days did not differ in both groups: 6.18 and 6.15% in the tenecteplase and alteplase groups, respectively. The frequency of hemorrhagic strokes also did not differ and amounted to 1.78 and 1.66%, respectively. It was concluded that both drugs had the same therapeutic effectiveness, but a simpler method of using the new thrombolytic was noted [26].
Thus, the advantage of the 3rd generation thrombolytics of the tPA group (tenecteplase) is not higher clinical efficacy and safety, but convenience and ease of use. Therefore, this particular drug is positioned as the only special thrombolytic for the prehospital stage.
There have been no multicenter comparative studies of streptokinase and tenecteplase. We conducted a single-center comparative study of these drugs when administered in the prehospital setting [27]. The rate of reperfusion after 90 minutes according to ECG signs was higher in the tenecteplase group: 64 versus 48% (p <0.05). Based on the results of the angiographic-guided GUSTO-1 substudy, it can be assumed that at 3 hours the reperfusion rate would be the same, but according to the recommendations, if thrombolysis is ineffective after 90 minutes, both groups underwent salvage percutaneous coronary intervention. Therefore, mortality did not differ between groups.
Urokinase, prourokinase and domestic Purolase
As the name of the drug suggests, urokinase (UK) is produced by kidney cells. It is isolated either from the urine of healthy young people, from human kidney cell culture, or by genetic engineering. UK, like SA, is a fibrin-nonspecific thrombolytic, i.e. activates plasminogen, both adsorbed on fibrin and circulating in the bloodstream, as a result not only fibrin is broken down, but also fibrinogen, which causes the development of a systemic lytic state. Unlike SC, UA directly converts blood plasminogen into plasmin. The half-life of UA is 9–16 minutes. The big advantage of UK over SC is the absence of antibodies to it, i.e. its non-allergenic. Urokinase is a mixture of two forms of the drug: high molecular weight (54 thousand daltons) and low molecular weight (33 thousand daltons). The high molecular weight form consists of two chains: heavy and light; The active site of proteinase is located in the heavy chain. Low-molecular-weight UA, being a cleavage product of high-molecular-weight, consists predominantly of a heavy chain. Despite these differences, their pharmacological (thrombolytic) effects are approximately equivalent [10].
In 1979, another form of the Criminal Code was identified. It has a molecular weight similar to high molecular weight UA, but differs from it in the following properties: 1) has a single-chain structure; 2) exhibits affinity for fibrin. This form of UA was named prourokinase. Most clinical studies with UA are devoted to its use in pulmonary embolism and peripheral thrombosis. Currently, it is practically not used for the treatment of myocardial infarction, probably as a result of the fact that it has no real advantages over SK, except for the lack of antigenicity, and its cost is an order of magnitude higher than that of SK.
Unlike UA, prourokinase has been more widely studied and is used to treat myocardial infarction. Prourokinase was best known abroad under the trade name Saruplase (scu-PA), but when compared with SC (PRIMI and COMPASS studies), Saruplase, with comparable effectiveness, increased the incidence of intracranial hemorrhages. Saruplase also showed no benefit when compared with alteplase (SESAM study). Therefore, this drug is not currently used in clinical practice.
A modified molecule of native prourokinase Purolase was obtained in the genetic engineering laboratory of the Russian Cardiology Research and Production Complex of the Russian Ministry of Health. The result of the change in the amino acid sequence was a 3-fold increase in the half-life of the drug: from 9 to 30 minutes. A Russian multicenter study of Purolaza in AMI was conducted [28]. The study included 237 patients with AMI in the first 6 hours of the disease. After 3 hours from the start of therapy, coronary reperfusion, based on indirect evidence, was achieved in 176 (74%) patients. The incidence of hemorrhagic stroke was 0.4%, and the 30-day mortality rate was 7%. There was no randomized control group with another thrombolytic in this study.
Despite the fact that Purolase has fibrin specificity, when it is administered, signs of systemic fibrinolysis are observed: a significant decrease in the level of fibrinogen (in 28% of patients <1.0 g/l) and α2-antiplasmin. Apparently, these phenomena are associated with the formation of a double-chain form of the molecule lacking fibrin specificity.
Staphylokinase and domestic Fortelysin
Staphylokinase is a protein secreted by some strains of Staphylococcus aureus, which, like SA, is an indirect plasminogen activator. Currently, staphylokinase is produced by the DNA recombinant method, which determines its high cost compared to SA. In 1990 Several small studies have been conducted on the comparative effectiveness of different doses of staphylokinase (10 to 30 g) and alteplase. The rate of CA reperfusion in the staphylokinase group ranged from 50 to 74% at different doses and administration regimens, which was no worse than in the alteplase groups. It was found that staphylokinase is a more fibrin-specific thrombolytic, because Unlike alteplase, after the introduction of which the level of fibrinogen still decreased, after the introduction of staphylokinase there was no such decrease [29–31].
The disadvantage of staphylokinase compared to alteplase is its allergenicity. Therefore, the question immediately arose about overcoming this shortcoming. The latest development in this direction is the creation by domestic scientists of a genetically modified non-immunogenic staphylokinase called “Fortelizin”. A small randomized trial was conducted comparing Fortelisin 15 mg administered over 30 minutes (or two boluses or bolus + infusion) and alteplase. The frequency of coronary reperfusion according to indirect signs at 90 minutes from the start of thrombolysis was absolutely the same in the Fortelysin and alteplase groups: 85% [32]. This study is rightly criticized for the very small number of patients: only 41 patients were examined in the Fortelisin group.
Currently, Fortelizin is registered as a drug for medical use and is even included in the list of vital drugs. To monitor the effectiveness and safety of the drug, a registry was established to collect this information. By the fall of 2014, 675 patients with AMI received thrombolysis with Fortelysin, the rate of coronary reperfusion according to ECG criteria in the form of a decrease in the ST segment≥50% was 74%, mortality within 30 days was 4.4%, hemorrhagic stroke developed in 3 patients, which amounted to 0.44% [33]. However, the methodology for collecting this information and the clinical and anamnestic characteristics of the patients are not presented.
The problem of choosing a drug
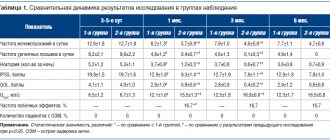
Thus, there are 5 thrombolytics on the domestic market for the treatment of myocardial infarction: SK, alteplase, tenecteplase, Purolase (genetically modified prourokinase) and Fortelysin (genetically modified non-immunogenic staphylokinase). Unlike other drugs, SC is a fibrin-specific thrombolytic. Typically, fibrin-specificity is considered as a drawback of the drug. The goal of thrombolysis is to dissolve the clot, not to reduce fibrinogen levels. It would be logical to expect that fibrin-specific thrombolytics, which preserve fibrinogen levels, should reduce the incidence of hemorrhagic complications, but, on the contrary, tPA drugs - alteplase and tenecteplase - compared to SC, increase the incidence of the most severe complication - intracranial bleeding [20, 22]. In addition, a decrease in the level of fibrinogen, the largest plasma protein, improves the rheological properties of the blood for several hours, ensuring the development of a “systemic lytic state,” which may lead to a slight decrease in the frequency of relapses of the disease. Therefore, it is not possible to unambiguously assess the benefit of fibrin specificity of thrombolytics - tPA drugs. As shown in table. 1, the most fibrin-specific drug is staphylokinase [34], but how this translates into clinical effectiveness is not yet clear.
Based on the fact that alteplase is a more effective thrombolytic than SA, opens the coronary artery faster, but more often causes intracranial bleeding, a differentiated approach to prescribing these drugs has been proposed in the literature [35]. According to him, alteplase is more indicated for young patients in the first hours of a large, especially anterior, AMI: these patients have a low risk of hemorrhagic stroke and the greatest benefit from rapid reperfusion. SC is indicated for elderly patients with hypertension and a history of cerebrovascular accident, especially several hours after the onset of a small inferior myocardial infarction: these patients have an increased risk of hemorrhagic stroke, and the benefit of rapid reperfusion is no longer so significant, and may even be questionable. In such a situation, the risk of thrombolysis may outweigh the benefit, so it is preferable to use a safer thrombolytic agent. The risk of hemorrhagic complications can be further reduced by reducing the dose of SA to 750 thousand units. According to our data, administration of this dose of SA over 5–10 minutes does not reduce the frequency of reperfusion, but only accelerates it [12].
The main indicators of the effectiveness and safety of thrombolytics from the above literature sources, as well as current rounded wholesale prices are presented in Table. 2.
Because these data are from different studies and registries with different patient inclusion and reperfusion criteria, direct comparison is not valid. This especially applies to Purolase and Fortelysin, which do not have a large evidence base comparable to other thrombolytics, therefore the data presented on their effectiveness and safety should be considered as preliminary, which require further clarification and confirmation. Despite this, the incidence of intracranial bleeding against the background of Purolase and Fortelysin looks very encouraging: it is significantly lower compared to tPA drugs and even lower than in the SC group. If this is confirmed by further collection of material, it will be possible to claim that these are the safest thrombolytics. In addition, it can be stated that the presented drugs differ only slightly in their effect on mortality (except for the mortality rate on Fortelysin, which is doubtful). In order to prove a difference in this indicator, enrollment of several tens of thousands of patients is required (as in the GUSTO-1 study comparing CK and alteplase). Fibrin-nonspecific SC is currently used less frequently and is more difficult to work with due to the frequent development of hypotension, but it retains its place in clinical recommendations [36]. Given its benefits regarding the risk of hemorrhagic stroke, there is no reason to completely abandon this drug, especially in patients at increased risk for this severe complication.
Prehospital thrombolysis requires a drug administered as a single bolus. So far, only tenecteplase satisfies this requirement.
A multicenter study is currently underway to examine the effectiveness of administering the full dose of Fortelisin 15 mg as a single bolus [37]. The comparison drug is tenecteplase in a dose calculated according to body weight, according to the instructions. If the study result is positive for Fortelisin, another drug for prehospital thrombolysis may appear in clinical practice, which is significantly cheaper.
The federal list of vital drugs currently includes alteplase, prourokinase (in Russia - Purolase) and a recombinant protein containing the amino acid sequence of staphylokinase (i.e. Fortelysin, since it does not have an international name), so the selling price for them is limited [38]. As presented in table. 2, prices for thrombolytic drugs differ by an order of magnitude. Significantly cheaper than all SCs. Despite its disadvantages compared to other thrombolytics, it appears that SK is not so much worse than other drugs as it is cheaper, taking into account the minimal difference between SK and tPA in terms of the effect on mortality.
Thus, domestic cardiology has the opportunity to select a thrombolytic for use in clinical practice for AMI. This choice depends on the intended route of administration, the risk of hemorrhagic stroke, and the cost of the drug. But the most important thing that doctors on duty and health care managers should remember is that the very fact of performing thrombolysis with any thrombolytic is much more important for the outcome of the disease than the choice of thrombolytic drug!
No conflict of interest is declared.
Fibrinolytic drugs
Home Medical Encyclopedia Medicines Medicines that primarily affect tissue metabolic processes
ALTEPLASE
Synonyms: Actilyse.
Pharmachologic effect. Recombinant human plasminogen activator (a blood protein involved in the regulation of blood coagulation), which is part of the drug, is a glycoprotein (complex protein), which, after systemic administration, is in the plasma in an inactive form until it binds to fibrin (an insoluble protein formed in blood clotting process). Once activated, the drug activates the transition from plasminogen to plasmin and leads to the dissolution of the fibrin clot, thereby increasing fibrinolysis (dissolution of the blood clot) only in the thrombus tissue.
Indications for use. Acute arterial and venous thrombosis (formation of a blood clot in a vessel).
Method of administration and dose. Administered intravenously over 1-2 minutes at a dose of 10 mg, then dropwise over 3 hours at a dose of 90 mg (in this case, 50 mg is administered over 60 minutes, and the remaining 40 mg is administered over the 2nd and 3rd hours from speed 20 mg/h).
If bleeding occurs due to an overdose of the drug, a transfusion of fresh frozen plasma or fresh blood is indicated; In addition, fibrinolysis inhibitors (drugs that inhibit the dissolution of a blood clot) can be used.
Side effect. Nausea, vomiting, fever, allergic reactions in the form of urticaria, headaches, rarely - bleeding, reperfusion arrhythmias (heart rhythm disturbances as a result of restoration of blood flow through the arteries of the heart).
Contraindications. Hemorrhagic diathesis (increased bleeding), bleeding, previous surgery or injury less than a week old, malignant arterial hypertension (persistent rise in blood pressure, difficult to treat), bacterial endocarditis (disease of the internal cavities of the heart due to the presence of bacteria in the blood), acute pancreatitis ( inflammation of the pancreas), complicated diabetes mellitus, sickle cell anemia (a hereditary disease characterized by increased breakdown of sickle-shaped red blood cells and the presence of functionally defective hemoglobin (oxygen carrier) in them), childhood, pregnancy, breastfeeding, hypersensitivity to the drug. The drug is prescribed with caution to patients with concomitant pulmonary diseases, as well as to patients over the age of 75 years.
Release form. Dry substance for infusion of 0.02 g and 0.05 g in bottles in a package of 1 piece complete with solvent.
Storage conditions. List B. In a cool place.
STREPTODECASA FOR INJECTION (Streptodecasum pro injectionibus)
It belongs to the group of “immobilized” (fixed on a polymer carrier) enzymes and is an activator of the human fibrinolytic (blood clot-dissolving) system, modified by a water-soluble polymer matrix of a polysaccharide nature.
Pharmachologic effect. It has thrombolytic activity (dissolves a blood clot), converts blood plasminogen into plasmin and inactivates its inhibitors, and has a prolonged (long-lasting) fibrinolytic effect.
Indications for use. Acute peripheral arterial thrombosis (formation of a blood clot in an artery) or thromboembolism (blockage of a vessel by a blood clot), except in cases where emergency surgery is indicated; peripheral phlebothrombosis (blockage of a vein with a blood clot), acute thromboembolism in the pulmonary artery system or in cases of recurrent thrombosis of its small branches (recurrent blockage of a blood vessel with a blood clot); thrombosis of the central vein and retinal artery; acute myocardial infarction on the 1st-2nd day of the disease or its recurrent course (reappearance of signs of the disease), with rethrombosis after thrombectomy (re-occlusion of a vessel with a blood clot after its removal).
Method of administration and dose. Intravenously. Streptodecase is administered intravenously in a bolus, usually at an initial dose of 300,000 FU (test dose), then an hour later, in the absence of side effects, an additional 2,700,000 FU (total dose of 3,000,000 FU) is administered additionally in a bolus (within 1-2 minutes) at the rate of 300 000-600,000 FU per minute.
In these doses, the drug causes a significant and long-term increase in fibrinolytic activity of the blood, an increase in the content of stasminogen activator and plasmin, and has a pronounced therapeutic effect.
Streptodecase in therapeutic doses has little effect on blood coagulation parameters.
To prevent rethrombosis (re-occlusion of a vessel by a blood clot), combination therapy with streptodecase and heparin is advisable. Starting from the end of the 1st day after the administration of a therapeutic dose of streptodecase (3,000,000 FU), heparin is administered at the rate of 40,000 units per day (10,000 units every 6 hours) for 7-10 days.
Repeated administration of streptodecase is permissible no earlier than after 3 months. after treatment according to the specified regimen and only after studying the titer of streptococcal antibodies. If necessary, repeated administration is usually carried out after 6 months.
For the treatment of retinal vein thrombosis, it is proposed to administer streptodecase retrobulbarly (behind the eyeball) at 30,000 - 50,000 FU in 0.2-0.3 ml of isotonic sodium chloride solution at intervals of 5 days. In the intervals between injections, heparin and dexamethasone are administered retrobulbarly (see pages 448, 583).
Side effect. Allergic reactions are possible (chills, fever, headache, hyperemia /redness/, urticaria, lower back pain, etc.), and when combined with heparin - hemorrhagic complications: (bleeding, formation of hematomas: limited accumulation of blood in tissues / bruise/), hematuria (blood in urine), etc.
Contraindications. Hemorrhagic diathesis (increased bleeding), bleeding, peptic ulcer of the stomach and duodenum, for 4 days. after surgery and childbirth, acute streptococcal infection, sepsis (blood infection by microbes from the focus of purulent inflammation), endocarditis (disease of the internal cavities of the heart), acute inflammatory diseases of the abdominal organs (pancreatitis, cholecystitis, appendicitis, etc.), pregnancy up to 18 weeks. , high arterial hypertension (high blood pressure), active tuberculosis process, malignant neoplasms, allergies to fibrinolytic drugs in the past; diabetes mellitus, bronchiectasis with a pronounced destructive process (bronchial disease associated with the expansion of their lumen, accompanied by destruction of the bronchi), cirrhosis of the liver, kidney stones in the acute stage, severe atherosclerosis.
Release form. Lyophilized (dehydrated by freezing in a vacuum) powder of 1,500,000 FU (fibrinolytic units) in 10 ml bottles in a package of 2 bottles.
Storage conditions. List B. At a temperature not higher than +10 °C.
STREPTOKINASE
Synonyms: Avelizin, Streptase, Cabikinase.
Pharmachologic effect. Activates the fibrinolytic (blood clot dissolving) enzyme system, breaks down the fibrin contained in blood clots, resulting in thrombolysis (blood clot dissolution).
Indications for use. Embolism (blockage) of the pulmonary artery and its branches; thrombosis (formation of a blood clot in a vessel) of arteries and embolism of peripheral arteries with conservative (non-surgical) treatment; thrombosis of superficial and deep veins of the extremities; acute myocardial infarction during the first 12 hours; blockage of blood vessels in the retina of the eye.
Method of administration and dose. Streptokinase is administered intravenously, and, if necessary, intra-arterially.
It is usually administered intravenously at an initial dose of 250,000 IU (IU) in 50 ml of isotonic sodium chloride solution over 30 minutes (30 drops per minute). This dose usually causes the onset of lysis (dissolution) of the clot. Then the administration of streptokinase is continued at a dose of 100,000 IU per hour. The total duration of administration is, as a rule, 16-18 hours. Subsequent treatment is carried out with heparin and indirect anticoagulants.
With extensive arterial and venous thrombosis, long-term administration of streptokinase is sometimes necessary.
Intra-arterial administration of streptokinase is used in the acute period of myocardial infarction (initial dose 20,000 IU; maintenance dose - 2000-4000 IU per minute for 30-90 minutes).
In all cases, the administration of streptokinase should be started as early as possible, since the best effect is observed with fresh blood clots.
Treatment with streptokinase is carried out under the control of thrombin time (an indicator of blood clotting) and the level of fibrinogen in the blood (one of the blood clotting factors).
Side effect. Nonspecific reactions to protein are possible; headache, nausea, slight chills; allergic reactions; hematomas (limited accumulation of blood in the tissue /bruise/) with intramuscular injections; bleeding after puncture (piercing with a needle). To prevent allergic reactions, it is recommended to administer 50 mg of prednisolone intravenously simultaneously with streptokinase.'
Contraindications. Hemorrhagic diathesis (increased bleeding), recent bleeding, severe hypertension (persistent rise in blood pressure), streptococcal sepsis (blood infection by microbes / streptococci / from the focus of purulent inflammation), stomach ulcer, septic endocarditis (disease of the internal cavities of the heart due to the presence of microbes in the blood) , severe diabetes, pregnancy. The drug should be used with caution in severe liver and kidney diseases, and in active tuberculosis.
Release form. In bottles of 100,000, 250,000, 750,000 and 1,500,000 IU of streptokinase.
Storage conditions. In a cool place.
UROKINASE
Synonyms: Ukidan.
Pharmachologic effect. Fibrinolytic (blood clot dissolving) agent. Breaks down blood clots by activating plasminogen, which is an inactive precursor of plasmin (a protein that breaks down clotted blood clots).
Indications for use. Thromboembolic occlusive vascular diseases (vein thrombophlebitis /inflammation of the vein wall with blockage/, embolism /blockage of the pulmonary artery), the formation of local thrombi (blood clots) in arteriovenous hemodialysis shunts (special devices worn by patients for periodic connection to the machine " artificial kidney") or intravenous cannulas (devices for intravenous infusions), some forms of chronic meningitis (myelomeningocele /spina bifida/), coronary thrombosis (formation of a blood clot in the artery of the heart), bleeding in the anterior chamber of the eye and vitreous body.
Method of administration and dose. The average dose is 1000-2000 IU/kg/hour; when used within 24 hours, generalized proteolysis (enzymatic breakdown of proteins) does not occur, but fibrinolysis (dissolution of the blood clot) is ensured at the level of the blood clot; treatment continues until the blood clot is disobliterated (complete restoration of blood flow in a vessel previously blocked by a blood clot) in combination with heparin therapy. In the case of pulmonary embolism, arterial ischemia (arterial thrombosis), myocardial infarction, urokinase can be administered in situ (artery affected by a thrombus) at a dose of 1000-2000 IU/kg/hour; for severe pulmonary embolism - 15,000 IU/kg/hour in the form of a single injection lasting 10 minutes. In some cases - with thrombosis of shunts (formation of a blood clot in special devices worn by the patient for periodic connection to the artificial kidney apparatus), bleeding in the anterior chamber of the eye - local installations (instillations) of 5000-30,000 IU are used.
During pregnancy, the concentration of antiurokinase bodies gradually increases towards childbirth, making treatment
ineffective. Special observation is required if the patient has diabetes, accompanied by severe retinopathy (non-inflammatory lesions of the retina). If it is necessary to combine this drug with heparin, it should be administered sequentially at a certain time interval. If it is necessary to simultaneously administer urokinase with sodium heparinate in solution, a pH (an indicator of the acid-base state) should be created more than 5.0, and with calcium heparinate - 5.0-7.0.
Side effect. The development of shock, changes in liver tests, nausea, vomiting, loss of appetite, fever, chills, headache, lethargy, in case of an overdose of the drug - bleeding.
Contraindications. Hemorrhagic stroke (acute cerebrovascular accident resulting from rupture of blood vessels in the brain), bleeding or risk of bleeding, recent intracranial surgery, hemostasis deficiency (impaired function of the blood coagulation system), recent biopsy (tissue sampling for morphological studies) of any organ, severe arterial hypertension (persistent rise in blood pressure), severe liver or kidney failure. Relative contraindications: recent surgery, recent arterial puncture (puncture), inaccessible to local compression (local compression), pregnancy.
Release form. Bottles containing 5000, 25,000, 100,000, 250,000, 500,000, 1,000,000 IU of urokinase complete with solvent bottles.
Storage conditions. In a dry, cool place.
FIBRINOLYSIN (Fibrinolysinum)
Dry protein preparation of a natural enzyme isolated from donor blood plasma.
Pharmachologic effect. A physiological component of the body's natural anticoagulant system, the basis of which is the ability to dissolve fibrin threads.
Indications for use. Thromboembolism (blockage of blood vessels with a blood clot) of the pulmonary and peripheral arteries, thromboembolism of cerebral vessels, fresh myocardial infarction, acute thrombophlebitis (inflammation of the vein wall with blockage), exacerbation of chronic thrombophlebitis.
Method of administration and dose. Intravenously (drip) in an isotonic solution of sodium chloride (100-160 units of the drug in 1 ml of solution) with the addition of heparin (up to 20,000 - 40,000 units).
Side effect. Nonspecific reactions to protein (hyperemia/redness/ of the face, pain along the vein, pain behind the sternum and in the abdomen, chills, fever, urticaria, etc.).
Contraindications. Hemorrhagic diathesis (increased bleeding), bleeding, open wounds, peptic ulcer of the stomach and duodenum, nephritis (inflammation of the kidney), fibrinogenopenia (low levels of fibrinogen in the blood - one of the blood clotting factors), tuberculosis (acute form), radiation sickness.
Release form. In bottles of 20,000 units.
Storage conditions. At temperatures from +2 to +10 °C.
CELIASE (Celyasa)
A drug containing the enzyme streptokinase. Obtained from a culture of group C beta-hemolytic streptococcus.
Pharmachologic effect. Celiase activates the fibrinolytic proenzyme contained in the blood (a protein involved in the dissolution of a blood clot) - plasminogen, which is converted into plasmin. Penicast penetrates the thrombus (blood clot) and causes its dissolution.
Indications for use. Systemic and local arterial and venous thrombosis (formation of a blood clot in a vessel). The drug is most effective when used in the first 7 days of the disease.
Method of administration and dose. Intravenous drip or intra-arterial. The contents of the ampoule are dissolved in 1-2 ml of solvent (complete dissolution occurs within 1-2 minutes, the presence of suspensions, turbidity, and sediment is not allowed). Reopolyglucin, isotonic sodium chloride solution, and 5% glucose solution are used as solvents. After complete dissolution, the contents of the ampoule are transferred with a syringe into a bottle with one of the solvents listed above. The solution retains specific activity for 24 hours.
Celease treatment is carried out according to a special regimen only in a hospital setting (in a hospital).
Side effect. Resorptive fever (a sharp increase in body temperature associated with the entry into the bloodstream of thrombus breakdown products). Possible reactions in the form of hyperthermia (fever), chills, headache, pain in the lumbar region, nausea,
caused by the presence of a heterogeneous (foreign) protein in the preparation.
Contraindications. Diseases and conditions predisposing to bleeding: hemorrhagic diathesis (increased bleeding), ulcerative lesions of the gastrointestinal tract, severe forms of sepsis (blood poisoning by microbes from the focus of purulent inflammation), hemorrhagic stroke (acute cerebrovascular accident resulting from rupture of cerebral vessels), tuberculosis lungs with cavernous process, active rheumatic process and other infections caused by streptococci; acute alcohol intoxication (alcohol poisoning), early (up to 3 days) postoperative, postpartum period, pregnancy. Persistent arterial hypertension (persistent rise in blood pressure). In severe forms of diabetes mellitus, the use of celiac is possible only for health reasons.
Release form. In ampoules in lyophilized form (powder dehydrated by freezing in a vacuum) 250,000 ME each, 10 pieces in a package.
Storage conditions. List B. At temperatures from +2 °C to +10 °C.
| print version | This information is not a guide to self-treatment. A doctor's consultation is required. |
The importance of antifibrinolytic drugs in the prevention of obstetric hemorrhage
The authors of the article presented literature data on the state of hemostasis during pregnancy and the prevention of obstetric hemorrhage. The authors used the drug Tranexam as a means of controlling fibrinolytic activity. Observations have shown that this drug is an effective way to limit intra- and postnatal blood loss.
The significance of drugs of antifibrinolytic action in the prevention of obstetric hemorrhage
The authors presented the data of the literature as hemostasis in pregnancy and prevention of obstetric hemorrhage. As a means of controlling fibrinolytic activity, the authors used "Tranexam". Observations showed that the drug is an effective way of limiting intra-and postnatal bleeding.
The priority task of modern obstetrics is to protect the health of the mother and fetus. Of particular importance in this regard is the prevention of dangerous life-threatening complications of pregnancy and childbirth, among which obstetric hemorrhages occupy one of the leading places. The frequency of bleeding averages 2-3% of the total number of births and has had a slight downward trend in the last decade. However, the percentage of massive blood loss does not decrease, and it is they that largely determine the structure of maternal mortality, appearing as its main cause in 20-25%, as a competing cause in 42%, as a background pathology in 78% [1, 2 , 3].
The largest number of obstetric hemorrhages occurs in the placenta and early postpartum period, they account for more than 80% of the total. The reasons for them are different - violation of the separation and discharge of the placenta, trauma to the soft tissues of the mother, hypotension of the uterus. At the present stage of development of science, it is becoming increasingly clear that, along with traditional causes, disturbances in the hemostasis system play a significant role in the genesis of bleeding, and this applies not only to massive bleeding, but also to pathological blood loss of moderate volume.
The importance of the quality of thrombus formation at the placental site is evidenced by the cardinal adaptive changes that the hemostatic system undergoes during pregnancy and childbirth. Their goal is to achieve a state of structural and chronometric hypercoagulation, capable of stopping bleeding from the uteroplacental arteries in the shortest possible time [4, 5, 6].
Adaptation of the hemostatic system during pregnancy, aimed at increasing coagulation potential, is systemic in nature and affects all parts of the hemostatic balance. The change in primary (vascular-platelet) hemostasis consists of an increase in the absolute number of platelets (at the same time, due to hemodilution, their relative concentration may decrease slightly), an increase in the functional activity of the plates (increased adhesiveness and aggregation, the ability to activate and degranulate). The dynamics of plasma (secondary) hemostasis parameters are associated primarily with an increase in the content of fibrinogen, the amount of which in the body increases by more than 2-3 times. Also, on average, the concentration and activity of most other plasma factors increases by 100-200%.
The anticoagulant (anticoagulant) system, represented by the antithrombin-heparin complex, is characterized by a slight decrease in the synthesis of AT111 with a simultaneous increase in its activity. This combination makes it possible to effectively control the coagulation cascade, but may demonstrate its inconsistency in conditions of excessive coagulation against the background of various pathologies, both obstetric and extragenital.
In general, despite the obvious activation of hemostasis in pregnant women, their thrombophilia remains only potential and is not accompanied by either thrombogenesis or a violation of the rheological properties of the blood.
To stop subsequent bleeding, along with systemic events, local processes that occur directly in the area of damage to the epithelial cover of the uterus - on the placental site - are also of great importance. When the placenta is separated, coagulation is highest here. The placenta and decidual tissue contain an excess of thromboplastic substances (tissue factors), which create optimal conditions for local thrombus formation. Coagulation of blood flowing from the uterus during the passage of the placenta occurs 10 times faster than blood taken simultaneously from a finger. Retroplacental blood clots 12 times faster than capillary blood taken from a finger.
In ensuring the reliability and durability of fibrin clots, the fibrinolytic system plays an important role. Fibrinolysis reflects a complex reaction between the components of the body's plasmin system (plasminogen, plasmin, activators and inhibitors of fibrinolysis proenzymes) and fibrin. In order to prevent delayed bleeding, which is possible at the stages of tissue repair of the placental site, the activity of this part of the hemostatic balance in pregnant women is deeply depressed. It is known that progesterone is involved in the suppression of fibrinolytic activity, which helps to increase the concentration of fibrinolysis inhibitors. However, the main source of protease activator inhibitors is the placenta. The concentration of PAI 1 (plasminogen activator inhibitor) in its tissue exceeds the plasma level by 11 times, PAI 2 by 260 times, respectively [7, 8, 9, 10].
Inhibition of fibrinolytic activity during pregnancy has a deep physiological meaning. This is due to the fact that the tissues of the uterus (endometrium, myometrium), as well as the perimetrium of a non-pregnant woman, have a high plasminogen-activating ability and are significantly superior to other tissues with similar properties (adrenal glands, lymphatic glands, prostate, lung, aorta, kidney). The feasibility of activating fibrinolysis in the uterine cavity (both during menstruation and in the first phase of the cycle) is undeniable from the point of view of preventing the formation of blood clots and the development of intrauterine adhesion. This process is stimulated by estrogens. It has been established that excessive activation of local fibrinolytic activity is accompanied by various pathological conditions of the reproductive system (inflammatory diseases of the upper genital tract, uterine bleeding of various origins, dyshormonal conditions, uterine fibroids, endometriosis). Thus, the uterus tends to respond with proteolytic events in response to a variety of stimuli, and in this regard, suppression of fibrinolytic activity during the stages of gestation is a necessary protective measure. However, there are a number of situations when, for various reasons, the fibrinolytic link of hemostasis in pregnant and postpartum women does not demonstrate suppression, but increased activity. In these cases, clinical manifestations in the form of bleeding are inevitable, which are, of course, coagulopathic in nature and require appropriate specific therapy.
It must be taken into account that activation of fibrinolytic activity can be both systemic and local in nature [11, 12, 13].
Systemic activation of fibrinolysis is observed in acute and fulminant DIC syndrome (with massive bleeding, severe gestosis, eclampsia, premature placental abruption, septic conditions, amniotic fluid embolism, catastrophic form of aPL syndrome, as well as in the presence of a dead fetus in the uterus).
Local activation of fibrinolysis occurs much more often. It occurs in chronic disseminated intravascular coagulation syndrome (preeclampsia, autoimmune processes, infectious pathology), intrauterine infection during pregnancy or childbirth, and uterine hypotension. Patients with a history of inflammatory processes of the endo- and myometrium, hormonal disorders before pregnancy, endometriosis, uterine fibroids, abnormal uterine bleeding before pregnancy, congenital and acquired disorders of hemostasis of a coagulopathic nature are at risk.
Women with the listed complications are traditionally at risk for bleeding in the postpartum period. But usually a threat of uterine hypotension is implied. However, this contingent primarily needs measures aimed at preventing blood loss associated with increased fibrinolytic activity. For these purposes, it is advisable to use drugs that have the properties of protease inhibitors, that is, antifibrinolytic agents, whose safety and effectiveness are confirmed by evidence-based medicine. In particular, a systematic review by the Cochrane Association (2007) based on the results of 211 randomized controlled trials (20,781 participants) showed that fibrinolysis inhibitors significantly reduce the amount of blood loss and the need for transfusions, their use is not accompanied by an increase in the incidence of thrombotic complications and deaths.
Tranexamic acid (“Tranexam”), a synthetic amino acid and a competitive inhibitor of plasminogen, acts as a means of professionally controlling fibrinolytic activity. According to the mechanism of action, tranexamic acid is similar to e-aminocaproic acid, but is 10-20 times more effective [7, 12].
Tranexamic acid blocks lysine-binding sites in plasminogen, as a result of which the latter cannot bind to fibrin and exert its lytic effect.
A feature of Tranexam, unlike other hemostatic agents, is the low risk of thrombotic complications. Back in the 60s of the last century, studies conducted in Scandinavia showed that over a period of over 19 years, on the example of 238,000 women, there was no increase in the incidence of thrombotic complications compared to the usual level among patients of the same age. It is very important that the suppression of the formation of kinins and other active peptides by Tranexam has an anti-inflammatory and anti-allergic effect [7].
The effectiveness of Tranexam is directly related to the choice of an adequate dose of the drug. The plasma concentration of tranexamic acid sufficient for prophylactic purposes is 30-50 mcg/ml. To obtain this concentration of the drug, it is recommended to adhere to certain prescribing regimens. In particular, the prevention of postpartum hemorrhage is proposed to be carried out according to the following protocol:
At the beginning of the first stage of labor - from 750 mg per os (up to 20-25 mg/kg). Then every 4 hours 500 mg. The total dose is up to 2 g.
In the high-risk group - 500 mg intravenously at the beginning of the first stage of labor (before surgery), then 500 mg per os every 4 hours.
The use of lower doses is inappropriate from a pharmacodynamics point of view, clinically ineffective and, in fact, discredits the method.
We conducted a clinical trial to evaluate the effectiveness of the drug "Tranexam" for the specific prevention of bleeding in women in the early postpartum period. The study included 236 pregnant women aged 19 to 42 years with one or more risk factors for bleeding:
- third or more births,
- gestosis,
- autoimmune processes,
- large fetus, polyhydramnios, multiple births,
- infectious pathology during pregnancy (signs of intrauterine infection, recurrent infections of the lower genital tract, urinary tract infections),
- abnormalities of labor,
- clinical and anamnestic markers of coagulopathies, isocoagulation state,
- history of inflammatory diseases of the upper genital tract, including after childbirth and abortion,
- history of abortions and miscarriages,
- uterine bleeding of various origins, including after childbirth and abortion,
- uterine fibroids.
The study was single-blind, placebo-controlled. By randomization with stratification by parity, the patients were divided into 2 groups: 1st - main (121 women) and 2nd - comparison group (115 women). All women of group 1 in the first stage of labor or before cesarean section were given specific bleeding prophylaxis with Tranexam according to the above regimens. The indication for intravenous administration of the drug was the presence of 3 or more risk factors, as well as delivery by cesarean section (planned or emergency). There were 36 such patients (29.8%). In group 2, women received a placebo during childbirth, including those who had a high risk of bleeding (32 women in labor - 27.8%). Prevention of hypotonic bleeding was performed in all women of both groups using generally accepted methods using uterotonic drugs. The volume of blood loss during childbirth was determined for each patient using gravimetric methods. The frequency of pathological blood loss was assessed.
The results of the study showed that women of group 1, who gave birth naturally, had an average blood loss of 201.5 ± 25.3 ml. It is important that this indicator did not show significant differences even in those patients whose risk of bleeding was assessed as high. The amount of blood they lost averaged 237.6 ± 40.8 ml, versus 192.3 ± 28.6 ml for the rest of this group (excluding those who gave birth surgically), p = 0.06. 22 women (18.2%) delivered by caesarean section either planned or emergency according to maternal or fetal indications. The average intraoperative blood loss was 480.2 ± 62.3 ml. Bleeding in the afterbirth and early postpartum period occurred in 4 postpartum women of group 1 (3.3%), which in frequency corresponds to the population average. In 2 observations it was hypotonic in nature, as could be judged by clinical symptoms and the rapid and stable effect of uterotonic drugs. In one case, bleeding was associated with retention of parts of the placenta in the uterine cavity, and in another, with injury to the soft tissue of the woman’s birth canal. The average blood loss was 548.3 ± 76.6 ml. In all cases, the women’s condition was not disturbed, there were no signs of hemodynamic suffering, standard therapy to stop bleeding and replenish blood volume was effective.
In group 2, whose patients received placebo, the average blood loss during conservative delivery was 339.2 ± 40.1 ml, which was 1.68 times higher than in group 1 (p = 0.02). At the same time, in women who had a high risk of bleeding based on a combination of signs, the average blood loss was 376.6 ± 32.5 ml, significantly exceeding this figure in postpartum women with a lower degree of risk (respectively 302.2 ± 25.1 ml, p = 0 ,04). The volume of blood loss during cesarean section also differed in comparison with group 1; it amounted to 610.6 ± 50.4 ml and was 1.3 times higher than in women who received Tranexam intravenously as a preventive measure (p = 0.05). Bleeding complicated the course of the afterbirth and postpartum period in 8 women (6.9%). This figure is 2 times higher than in group 1, however, to confirm the statistical significance of the differences and overcome type 2 error, it is necessary to increase the sample. A significant percentage of bleeding that developed in women who received prophylaxis with uterotonic drugs indirectly indicates the role of other causes of bleeding, not related to uterine hypotension, and first of all, this refers to the possibility of disturbances in local hemostasis with activation of proteolytic activity, so characteristic of endocrine tissues. and myometrium.
Thus, it is necessary to take into account the features of the physiological mechanisms of adaptation of the fibrinolytic system in pregnant women, as well as the significance of violations of these mechanisms in the genesis of obstetric hemorrhage. Specific prevention with an antifibrinolytic drug, Tranexam, is an effective way to limit intra- and postnatal blood loss, and the accumulated experience allows us to classify this drug as the first choice drug for the prevention of obstetric hemorrhage and recommend it for widespread use in practice.
L.I. Maltseva, T.P. Zefirova, I.V. Abdullina
Kazan State Medical Academy
Maltseva Larisa Ivanovna - Doctor of Medical Sciences, Professor, Head of the Department of Obstetrics and Gynecology No. 1
Literature:
1. Kickler T. General principles of treatment of bleeding. Cowless surgery on the threshold of the 21st century - a modern view of transfusion therapy 04/19/1999.
2. Lanir N. et al. Best Pract Res Clin Haematol-2003 -16(2),183-95.
3. Tengborn L. Treatment of Hemophilia 2007; 42:15.
4. Coolman M. et al. Eur J Obstet Gynecol Reprod Biol. 2006; 128(1-2): 22-8.
5. Deitcher S., Gardner J. Clinics in Liver Disease 2007; 3:1:83-96.
6. O'Riordan MN et al. Best Pract Res Clin Obstet Gynaecol. 2003; 7(3): 385-96.
7. Tingborn L. Fibrinolysis inhibitors in the treatment of hemorrhagic disorders. Treatment of hemophilia 200; 42.
8. Shevchenko Yu.L. and others. Blood-saving effect of tranexamic acid. Farmoteka 2008; 16:17-25.
9. Demers C. et al. Int. J. Gynaecol. Obstet. 2006; 95:1:75-87.
10. Mackman N. Thromb Vasc Biol. 2004; 24(6): 1015-22.
11. Soma H. The significance of fibrinolysis in abortion. J Tokyo Med Coll 1970; 28: 343-50.
12. Svanberg L., Astedt B., Nilsson IM Abruptio placentae — treatment with the fibrinolytic inhibitor tranexamic acid. Acta Obstet Gynecol Scand 1980; 59: 127-30.
13. Uszyński M. et al. Gynecol Obstet Invest. 2001; 52(3): 189-93.