Home | About us | Delivery | Advertisers | Login | Registration
The pharmacy is closed on Sundays and holidays.
- Medicines
- dietary supplementsVitamins
- Categories from A to Z
- Brands from A to Z
- Products from A to Z
- Medical equipment
- beauty
- Child
- Care
- Honey products appointments
- Herbs and herbal teas
- Medical nutrition
- Journey
- Making medicinesStock
Pharmacy online is the best pharmacy in Almaty, delivering medicines to Almaty. An online pharmacy or online pharmacy provides the following types of services: delivery of medicines, medicines to your home. Online pharmacy Almaty or online pharmacy Almaty delivers medicines to your home, as well as home delivery of medicines in Almaty.
my basket
Apteka84.kz is an online pharmacy that offers its customers medicines, medicinal and decorative cosmetics, dietary supplements, vitamins, baby food, intimate products for adults, medical equipment and thousands of other medical and cosmetic products at low prices. All data presented on the Apteka84.kz website is for informational purposes only and is not a substitute for professional medical care. Apteka84.kz strongly recommends that you carefully read the instructions for use contained in each package of medicines and other products. If you currently have any symptoms of the disease, you should seek help from a doctor. You should always tell your doctor or pharmacist about all the medicines you take. If you feel you need further help, please consult your local pharmacist or contact our GP online or by telephone.
© 2021 Pharmacy 84.
The use of symptomatic slow-acting drugs for osteoarthritis of the joints of the hands
From a modern point of view, osteoarthritis (OA) is one of the most common diseases of the musculoskeletal system and is considered as a heterogeneous group of diseases with different etiologies, but similar biological and morphological features [1]. The number of patients with OA is constantly growing, which is associated with an increase in the life expectancy of the population and the accumulation of risk factors for the disease [2]. This disease is characterized by a steadily progressive course, leading to a deterioration in the quality of life of patients, limiting their physical capabilities and social functions, becoming a cause of disability, which determines the relevance of searching for effective therapy [3]. Chronic pain leads to a decrease in life expectancy by an average of 10–12 years [4]. The problem of pain in OA is not only medical, but also social in nature and affects functional, social activity and life expectancy [5]. The use of nonsteroidal anti-inflammatory drugs (NSAIDs) for OA is associated with the development of NSAID-induced gastropathy, especially in older people. According to randomized clinical trials, ulcerative lesions of the gastrointestinal tract are detected in 15–40% or more of patients regularly taking non-selective NSAIDs for 6 months [6]. Taking NSAIDs aggravates the course of arterial hypertension, reduces the effectiveness of antihypertensive therapy, and can aggravate congestive heart failure [7, 8]. Most NSAIDs are thought to increase cartilage degeneration with long-term use [9–11]. The problem of reducing pain in OA is obvious. Prescribing symptomatic slow-acting drugs can reduce the severity of the main symptoms of the disease and the need for analgesic therapy [12].
Currently, OA of the joints of the hands remains poorly studied in terms of the effectiveness of the drugs used. The prevalence of this type of OA in European countries increases from 10% at the age of 40–49 years, to 92% at the age of over 70 years [3]. Most people aged 55 years and older have radiographic evidence of OA in at least one joint of the hand, and 20% have clinical signs of the disease. EULAR has developed recommendations for the management of patients with OA of the joints of the hands, according to available research. A number of recommendations are associated with the use of local medicinal and non-medicinal local treatment methods, and the use of NSAIDs. Few studies have been carried out using slow-acting drugs, and, in particular, only chondroitin sulfate (CS) has been studied in terms of its structure-modifying effect in OA of the joints of the hands [13]. The effects of glucosamine and diacerein on hand symptoms and joint function have not been studied.
The purpose of the study was to conduct a comparative analysis of the clinical effectiveness of diacerein, glucosamine and chondroitin sulfate in patients with OA of the joints of the hands.
Materials and research methods
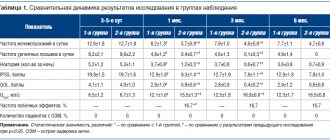
An open comparative controlled randomized 18-month study included 120 women who met the clinical criteria for the diagnosis of osteoarthritis of the hand joints [14]. The study was conducted in accordance with the basic principles of Good Clinical Practice and the Declaration of Helsinki. All patients signed voluntary informed consent, and a positive decision was made by the local ethics committee. Using the adaptive randomization method, all patients were divided into groups: 30 patients (group 1) took diacerein at a dose of 50 mg 2 times a day for 4 months, 30 patients (group 2) took cholesterol 500 mg 2 times a day for 4 months. for 6 months, 30 patients (group 3) took glucosamine sulfate (GS) 1500 mg per day for 3 months. All patients received 2 courses of therapy at intervals of 6 months. A comparison group (4th group) of 30 patients took aceclofenac (Ac) in the required dose. Patients in groups 1–3 were allowed to take aceclofenac as needed. The groups of patients before the start of the study were comparable in terms of main clinical and demographic indicators (p > 0.05) (Table 1).
All patients were women. The average age and length of illness did not differ significantly. Most patients in the groups had a nodular form of OA with symptoms of synovitis. In all groups, the isolated form of OA of small joints of the hands predominated, predominantly radiological stage II. All patients showed clinical activity of the disease and a decrease in the functional capabilities of the joints. Inclusion criteria were: a reliable diagnosis of OA of the joints of the hands, intensity of joint pain > 40 mm on a visual analogue scale (VAS), the need to take NSAIDs, the absence of clinically significant disorders of liver and kidney function, and signed informed consent. The study did not include patients with heart, renal and liver failure, type 1 diabetes mellitus, exacerbation of gastric and duodenal ulcers, as well as patients who received symptomatic slow-acting drugs at the time of inclusion in the study or 6 months before. actions.
To assess the effectiveness of therapy, we studied the severity of pain, stiffness, dysfunction in joints according to VAS, and assessed the Dreiser and AUSCAN functional indices. The need for NSAIDs was determined to assess the effect of therapy on the course of the disease. The dynamics of the indicators were assessed after 1 month, then every 3 months; radiography of the joints was carried out at baseline and after 18 months.
Statistical processing of the material was carried out using a specialized statistical package SPSS 17.0. In groups, the arithmetic mean (M), standard deviation (σ), mean error of the arithmetic mean (m), and confidence interval were calculated. When comparing indicators in groups, Student's t-test, χ2, was used. The study of the dynamics of the studied parameters during treatment was carried out using paired Student's t-test, χ2. In all cases, the null hypothesis was rejected at p < 0.05.
Results and its discussion
A positive effect of therapy on the symptoms of the disease was noted in all groups: pain, stiffness decreased and joint function improved (Tables 2–5). However, the time of onset of the clinical effect and its severity in the groups were different. The use of diacerein and GS led to a statistically significant improvement in the studied parameters by the 3rd month of observation (p < 0.05–0.01) (Table 2–5). The use of cholesterol statistically significantly (p < 0.05) improved clinical indicators only by the 6th month of taking the drug.
A decrease in the Dreiser index by the 18th month was noted in group 1 by 49%, in group 2 by 42%, in group 3 by 35%, in group 4 by 38% (p < 0.05 –0.01). A decrease in pain according to the AUSCAN scale by the 18th month was noted in all groups: in the 1st and 2nd groups the decrease in pain was 49% and 47.5%, respectively, in the 3rd group - 36%, and in the 4th group group 23.5% (p < 0.05). The stiffness index on the AUSCAN scale by the 18th month decreased by 51% in the diacerein and cholesterol group (p < 0.05), and in the HS group by 35% (p < 0.05). The functional activity of joints improved by the end of observation in the diacerein group by 53%, in the CS group by 50%, and in the HS group by 41% (p < 0.05–0.01). The effect of diacerein and CS lasted for 6 months; in HS, the effect “slipped away” 3 months after therapy. In all groups, the need for NSAIDs significantly decreased (p < 0.05–0.01). By the 18th month, in the diacerein group the dose of aceclofenac decreased by 87.4%, in the 2nd group by 86%, in the 3rd group by 78.5%. In group 4, a gradual decrease in the consumed dose by 54.2% was noted. The therapy allowed us to discontinue aceclofenac in 23% of patients in group 1, in 25% in group 2, and in 16.6% in group 3. 77% of patients in group 1, 75% in group 2, 83.3% in group 3, and 38% in group 4 were able to reduce NSAID intake by ≥ 50%. By the 18th month, 62% of patients in group 4 were taking the same dose of aceclofenac. Assessing the tolerability of the study drugs, it was noted that most often adverse events were recorded when taking aceclofenac - in 53% of cases: 26.6% of patients had epigastric pain, 16.6% had dyspepsia, and 10% had an increase in transaminases. Side effects in the CS and HS groups occurred equally (20%), in the diacerein group - 30% of cases. When taking diacerein, epigastric pain and increased transaminases occurred equally (in 6.6% of patients), and diarrhea was observed in 16.6% of patients. When taking cholesterol, 13.3% of patients experienced epigastric pain and 6.6% dyspepsia. During GS therapy, diarrhea and dyspepsia occurred equally (10%). In all cases of side effects, the drugs were discontinued.
Conclusion
Our data regarding GS and diacerein confirm the literature data. Although their effectiveness has not been evaluated in OA of the hand joints, their effectiveness in reducing pain in OA of the knee and hip joints has been shown in many clinical studies [15, 16]. CS was studied in 2 clinical studies for hand OA, which showed the effectiveness of the drug in preventing radiological progression. But these data are contradictory. No effect on disease symptoms or joint dysfunction has been reported [17].
Thus, therapy with repeated courses of diacerein, HS and cholesterol for OA of the joints of the hands has a symptomatic effect: it reduces pain, stiffness, improves joint function, and reduces the need for NSAIDs. Diacerein and CS, compared to GS, have a more persistent and pronounced effect. CS and GS, in comparison with diacerein, are less likely to cause side effects.
Literature
- Balabanova R. M., Kaptaeva A. K. Arthrodarin - a new drug for pathogenetic therapy of osteoarthritis // Scientific and practical rheumatology. 2009. No. 2. P. 49–53.
- Alekseeva L. I. Symptomatic slow-acting drugs in the treatment of osteoarthritis // Consilium medicum. 2009. No. 11 (9). pp. 100–104.
- Alekseeva L. I., Chichasova N. V. Use of piascledine for osteoarthritis of the hands // Pharmateka. 2010. No. 10. P. 48–55.
- Mozgovaya E. E., Zborovskaya I. A. Osteoarthrosis is the most common disease of the joints // Medicine Bulletin. 2012. No. 7. P. 33–40.
- Chichasova N.V. The problem of pain in osteoarthritis // Attending Physician. 2007. No. 2. P. 50–56.
- Nasonov E. L., Karateev A. E. Use of non-steroidal anti-inflammatory drugs. Clinical recommendations // Russian Medical Journal. 2006. No. 25. pp. 1769–1778.
- Savenkov M.P., Brodskaya S.A. et al. The influence of non-steroidal drugs on the antihypertensive effect of ACE inhibitors // Russian Medical Journal. 2003. No. 19. pp. 56–59.
- Warksman JC Nonselective nonsteroidal anti-inflammatory drugs and cardiovascular risk: are they safe? // Ann Rharmacother. 2007. Vol. 41. P. 63–73.
- Badokin V.V. Non-steroidal anti-inflammatory drugs in the treatment of osteoarthritis // Modern rheumatology. 2009. No. 1. P. 33–35.
- Chichasova N.V. Treatment of osteoarthritis: the effect of various anti-inflammatory drugs on cartilage // Russian Medical Journal. 2005. No. 8. pp. 539–543.
- Chichasova N.V., Imametdinova G.R., Igolkina E.V. Approaches to the treatment of pain taking into account the mechanisms of its development // Modern rheumatology. 2013. No. 1. P. 59–66.
- Lygina E.V. Chondroprotectors in the treatment of osteoarthritis // Modern rheumatology. 2012. No. 2. P. 59–65.
- Rovetta G., Monteforte P., Molfetta G. A two-year study of chondroitin sulfate in erosive osteoarthritis of the hand behavior of erosions osteophytes pain and hand dysfunction // Drug. Exp. Clin. Res. 2004. Vol. 30 (1). P. 11–16.
- Key provisions of the EULAR recommendations for the management of patients with osteoarthritis of the hand. 2010.
- Bartels EM, Bliddal H, Schondorff PK et al. Symptomatic efficacy and safety of diacerein in the treatment of osteoarthritis: a meta-analysis of randomized placebo-controlled trials // Osteoarthritis Cartilage. 2010. Vol. 18. No. 3. R. 289–296.
- McAlindon TE et al. Glucosamine and chondroitin for treating symptoms of osteoarthritis. A systematic quality assessment // JAMA. 2000. Vol. 283. P. 1469–1475.
- Leeb BF, Schweizer M. A meta-analysis of chondroitin sulphate in the treatment of osteoarthritis // J. Rheumarol. 2006. Vol. 27. P. 205.
E. A. Leushina1 O. V. Simonova, Doctor of Medical Sciences, Professor
State Budgetary Educational Institution of Higher Professional Education Kirov State Medical Academy of the Ministry of Health of the Russian Federation, Kirov
1 Contact information