All iLive content is reviewed by medical experts to ensure it is as accurate and factual as possible.
We have strict sourcing guidelines and only link to reputable sites, academic research institutions and, where possible, proven medical studies. Please note that the numbers in parentheses ([1], [2], etc.) are clickable links to such studies.
If you believe that any of our content is inaccurate, out of date, or otherwise questionable, please select it and press Ctrl + Enter.
According to the clinical course, paraproctitis is divided into acute and chronic.
Acute paraproctitis is a purulent inflammation (abscess) of the peri-rectal tissue.
[1], [2], [3], [4], [5], [6], [7], [8], [9]
Symptoms of acute paraproctitis
The disease has a short (no more than 3 days) prodromal period, during which weakness, headache, and general malaise may be observed. Then typical symptoms of paraproctitis appear: chills, fever, pain in the perineum. The severity of clinical symptoms is determined by the reactivity of the body, the type of bacteria that caused the inflammatory process, as well as which of the fascial-cellular spaces is affected. When the cellular spaces of the small pelvis are affected by the type of phlegmon, the clinical picture is dominated by general symptoms caused by intoxication. As the process progresses and an abscess forms, the intensity of the pain increases and it becomes throbbing. Depending on the intensity of the inflammatory process, this period lasts from 2 to 10 days. Then, if surgical treatment is not performed, the inflammation spreads to the adjacent cellular spaces of the pelvis, and the abscess empties into the rectum or onto the skin of the perineum. After opening the abscess, there are 3 possible outcomes:
- recovery;
- formation of rectal fistula (chronic paraproctitis);
- development of recurrent paraproctitis with more or less frequent exacerbations of the inflammatory process.
Chronic paraproctitis is a consequence of acute inflammation. This is a perirectal fistula, formed after spontaneous opening of an abscess or opening it surgically. The internal opening of a fistula is a defect in the rectum. The external opening is located on the skin of the perineum. In some cases, several fistula tracts and several external openings of the fistula can be observed.
Literature
- Dultsev Yu.V., Salamov K.N. Paraproctitis. M.: Medicine 1981. 208 p.
- Kaiser Andreas M. Colorectal surgery. M.: BINOM Publishing House 2011. pp. 473-477.
- Shelygin Yu.A., Blagodarny L.A. Handbook of coloproctology. M.: Litterra 2012. 596 p.
- Zhukov B.N., Isaev V.R., Chernov A.A. Fundamentals of coloproctology for a general practitioner: monograph. Samara, RF: Etching 2009. 218 p.
- Akopyan A.S. and others. Improving the results of treatment of patients with acute paraproctitis // Collection: Problems of coloproctology. M., 2002. Issue. 7. pp. 24-28.
- Slesarenko S.S., Fedorov V.E. Results of surgical treatment of acute paraproctitis // Collection: Current problems of coloproctology. M., 2005. Issue. 8. pp. 125-126.
- Vasilveski CA Anorectal abscesses and fistulas. In: Wolff BG, Fleshman JW, Beck DE, Pemberton JH, Wexner SD, eds. The ASCRS Textbook of Colorectal Surgery. New York: Springer. 2007. R. 192-214.
- Bolkvadze E.E. Complex forms of acute paraproctitis. Literature review // Coloproctology. 2009. 27 (1). pp. 38-46.
- Vorobyov G.I. Basics of coloproctology. M.: Medical Information Agency, 2006. 430 p.
- Orlova L.P. Ultrasonography in the diagnosis of diseases of the rectum and pararectal region: Abstract of thesis. diss. ... doc. honey. Sci. M., 1992. 44 p.
- Santoro GA, Di Falco G. Benign Anorectal Diseases. Diagnosis with Endoanal and Endorectal Ultrasound end New Treatment Options // Springer-Verlag Italia. 2006. 404 p.
- Santoro GA, Fortling B. The advantages of volume rendering in three-dimensional endosonography of the anorectum // Dis Colon Rectum. 2007. 50. R. 359-368.
- Toyonaga T., Tanaka Y., Song J.F. et al. Comparison of accuracy of physical examination and endoanal ultrasonography for preoperative assessment in patients with acute and chronic anal fistula // Tech Coloproctol. 2008. 12. R. 217-223.
- Buchanan GN, Bartram CI, Williams AB, Halligan S., Cohen CR Value of hydrogen peroxide enhancement of three-dimensional endoanal ultrasound in fistulainano // Dis Colon Rectum. 2005. 48. R. 141-147.
- West RL, Zimmerman DD, Dwarkasing S et al. Prospective comparison of hydrogen peroxide-enhanced three-dimensional endoanal ultrasonography and endoanal magnetic resonance imaging of perianal fistulas // Dis Colon Rectum. 2003. 46. R. 1407-1415.
- Shobeiri SA Practical pelvic floor ultrasonography. A multicompartmental approach to 2D/3D/4D ultrasonography of Pelvic floor // Springer Science+Business Media New York 2014.
- Pescatori M., Regadas FSP, Regadas SMM, Zbar AP Imaging atlas of the pelvic floor and anorectal diseases // Springer-Verlag Italia 2008.
- Tonolini M., Maconi G. Imaging of perianal inflammatory diseases // Springer-Verlag Italia 2013.
- Fillipov D.Yu. Ultrasonography in the diagnosis of acute paraproctitis. Author's abstract. diss. ...cand. honey. Sci. M., 1999. 25 p.
- Stewart LK, McGee J., Wilson SR Transperineal and transvaginal sonography of perianal inflammatory disease // Am. J. Roentgenol. 2001. V. 177 (3). P. 627-632.
Symptoms of chronic paraproctitis
Symptoms of paraproctitis of this form are a consequence of acute. In cases where, when opening the abscess, the internal opening in the rectum is not eliminated, a rectal fistula (chronic paraproctitis) may subsequently form. A rectal fistula is characterized by the presence of one or more external openings in the skin of the perineum near the anus. Pus, sometimes feces and gases can be released from the external openings of the fistula tract.
The general condition of patients with chronic paraproctitis “suffers” little. Pain is not the main symptom of the disease. It appears only when the process worsens. The nature and amount of discharge from the fistula depends on the activity of the inflammatory process. It should be noted that while the fistula is functioning (its external opening is open), relapses of acute paraproctitis rarely occur. At the same time, there is a special form of so-called acute recurrent paraproctitis. With it, a pinpoint internal opening in the rectum can be temporarily closed with a soft scar, and the fistula ceases to function. If the scar is damaged, paraproctitis recurs.
Depending on the location of the fistula tract in relation to the sphincter muscle, 4 types of fistulas are distinguished:
- subcutaneous-submucosal, or intrasphincteric, - the fistulous tract is located under the mucous membrane or in the subcutaneous tissue medially from the sphincter muscle;
- transsphincteric - the fistulous tract is directed from the intestine to the outside through the thickness of the sphincter;
- complex, or extrasphincteric, - the fistulous tract goes around the sphincter from the outside. With this form of fistula, the internal opening is usually located at the upper pole of the sphincter. Complex fistulas can be horseshoe-shaped. In these cases, the internal opening of the fistula, located along the posterior wall of the rectum, gives rise to two fistulous tracts, which open on the skin with two openings on either side of the anus;
- incomplete fistulas have only an internal opening in the rectum and no external opening in the perineum. The source of their formation is often an anal fissure.
The rectum is the final element of the gastrointestinal tract (GIT). Its inner surface is covered with mucous membrane, and on the outside it is surrounded by loose fatty tissue. For various reasons, the organ can become inflamed. If the mucous membrane is inflamed, the disease is called proctitis, if the tissue is inflamed, it is called paraproctitis. In both cases, the patient needs immediate treatment.
Diagnostics
Diagnosis of any type of inflammation of the perirectal tissue includes confirmation of the diagnosis based on existing symptoms, as well as differentiation of pathology from other proctological anomalies:
- teratomas of perirectal tissue;
- abscess of Douglas space;
- rectal tissue cysts;
- osteomyelitis of the lower spine;
- epithelial coccygeal duct;
- tuberculous fistulas and fistulas due to Crohn's disease.
To confirm paraproctitis, in addition to collecting anamnesis and complaints, use:
- laboratory blood test (a purulent process is indicated by an increase in leukocytes, neutrophils and ESR);
- physical examination of the rectum and perianal area (digital examination);
- anoscopy and sigmoidoscopy (these types of studies are not used for acute inflammation due to their pain and risk of sphincter spasm);
- canal probing or fistulography (x-ray contrast study);
- X-ray of the pelvic organs with or without contrast.
Diagnostic data helps to detect a purulent focus and all its ducts in order to choose the right treatment tactics.
Causes of inflammation of the rectum
Diseases may be of an allergic nature. But more often they are caused by opportunistic bacteria, which are constantly present inside the organ and lead to inflammation only in the presence of provoking factors. Less commonly, viruses that enter the intestinal tissue with the blood. The inflammatory process can be a consequence of sexually transmitted infections.
- frequent constipation/diarrhea;
- poor nutrition;
- weakened immune system;
- undergoing radiation therapy;
- taking antibacterial drugs.
The diseases often occur in patients suffering from food allergies, Crohn's disease, and ulcerative colitis. Hemorrhoids and anal fissures contribute to their occurrence. Pathologies can develop as a complication of sepsis, influenza or sore throat.
Reasons for development
There are many factors that can contribute to the development of pathology. Among them:
- Frequent bowel disorders or constipation
- Infectious bowel diseases, E. coli
- STD
- Haemorrhoids
- Traumatization of the rectum
- Untreated anal fissures
- Colitis
- Crohn's disease
- Decreased immunity
- Poor nutrition – predominance of fatty and spicy foods in the menu
- Alcohol abuse
- Specific physical activity, lifting heavy objects
- Failure to comply with hygiene standards
The combination of reasons determines the main category of patients of the proctologist - most often men aged 25-50 years turn to the doctor with paraproctitis.
Symptoms of acute proctitis and paraproctitis
Pathologies develop as an acute inflammatory process. Its clinical picture is identical in both cases. This is due to the close proximity of the mucous membrane and fiber of the rectum.
Local symptoms
- constipation/diarrhea;
- fecal incontinence;
- discharge of mucus, pus, and sometimes blood from the anus;
- a feeling of empty bowels and a constant desire to go to the toilet;
- itching and pain around the anus, aggravated by defecation;
- pain on the left side of the abdomen, in the perineum (sometimes radiating to the genitals or lower back).
General symptoms
- weakness;
- headache;
- skin rashes;
- loss of appetite;
- weight loss;
- aches and pain in muscles;
- increase in body temperature to +38…+39 o C, chills.
What is the treatment for paraproctitis?
Treatment of paraproctitis involves making an incision in the skin near the anus to remove pus from the infected cavity and reduce the pressure inside it. Quite often this can be done on an outpatient basis using local anesthesia. Treatment of large or deep abscesses may require hospitalization in a specialized hospital that can provide adequate pain relief during surgery. Hospitalization is indicated for patients with a tendency to serious infectious complications (patients with diabetes mellitus and decreased immunity). Conservative (non-surgical) treatment with antibiotics alone is not as effective as drainage (removing pus). This is due to the fact that antibiotics cannot penetrate the abscess cavity and act on the purulent contents located there.
Possible consequences
Lack of treatment for acute proctitis leads to the disease becoming chronic. Against this background, anal fissures often appear, and the inflammation spreads to the fatty tissue and causes paraproctitis. All this provokes the formation of malignant tumors in the tissues of the rectum.
Paraproctitis is accompanied by the formation of a large amount of pus. This usually leads to the formation of a fistula, which finds its outlet near the anus. Sometimes the abscess breaks through. Then the purulent masses spread in the abdominal cavity, causing peritonitis and involving other organs in the inflammatory process. This can lead to blood poisoning (sepsis).
Prognosis and prevention
With timely treatment, the prognosis for recovery is good. In the absence of medical care, acute forms of paraproctitis always progress to the chronic stage, and they are complicated by the spread of infection, purulent melting and necrosis of the pelvic organs, and sepsis.
To prevent paraproctitis, careful hygiene of the perianal area, adherence to PN standards to maintain normal stools, as well as timely treatment of proctological diseases are recommended.
How are pathologies treated?
Despite the similarity of clinical manifestations, proctitis and paraproctitis are treated differently. Treatment of inflammation of the mucous membrane is conservative. If the inflammatory process affects the intestinal tissue, surgical intervention is required.
Conservative therapy
The goal of therapy is to stop the inflammatory process. For this, the patient is prescribed antibiotics (Ceftriaxone, Medaxone) and antimicrobial agents (Biseptol, Bactrim). To rinse the rectum, enemas are done with Collargol, furatsilin solution or warm chamomile infusion. When the symptoms of inflammation decrease, sitz baths in a weak solution of potassium permanganate and oil microenemas are additionally prescribed.
Treatment of proctitis includes diet. The patient is recommended to exclude fatty, spicy, spicy foods, alcohol, and high-fiber foods from the diet. After recovery, he is advised to consume more dietary fiber along with fruits, vegetables and grains to prevent constipation.
Surgical intervention
Paraproctitis requires emergency surgery. It is carried out immediately after diagnosis using general anesthesia. During this procedure, the abscess is opened, its contents are removed, and the cavity is washed with an antiseptic solution.
To prevent relapse and complications, the operated patient is prescribed a course of antibiotics. Wounds are treated daily with antiseptics or antimicrobial agents. In the postoperative period, it is necessary to follow a diet. It prohibits the consumption of foods that cause gas formation and contain large amounts of fiber, spicy and fatty foods.
If symptoms of proctitis and paraproctitis appear, contact your doctor. An experienced proctologist will see you, make an accurate diagnosis and prescribe effective treatment. If necessary, you will receive emergency care immediately after diagnosis.
Diet
After surgery, nutrition should be “gentle”. Therefore, it is important to follow several main principles of the regime. The main thing is to choose the right foods that will ensure normal bowel movements and prevent the development of constipation.
Global Clinic specialists recommend including the following products in your diet:
- vegetables, steamed (with this cooking option you can retain the maximum amount of nutrients) or boiled;
- fresh fruits and herbs (it is recommended to exclude dill and fennel);
- fermented milk products (kefir, soft cheeses, low-fat cottage cheese);
- chicken fillet and white turkey meat, as well as veal;
- rye bread bread and crackers;
- soft-boiled eggs;
- cereals: buckwheat, pearl barley, millet;
- rosehip decoction;
- weak teas with the addition of lemon balm, chamomile or mint.
During the rehabilitation period, it is necessary to eat a variety of foods in small quantities - this will ensure that the body receives the maximum amount of nutrients.
Paraproctitis – anal fistula (rectal fistula)
Acute or chronic purulent “melting” of tissue in the anal area, leading to the formation of a fistula canal and, accordingly, a fistula opening. The main diagnostic signs of this serious disease are complaints of pain in the anus, the presence of a fistula opening and discharge from it, including purulent discharge, and swelling of the perineum.
Making a diagnosis by a proctologist is not difficult.
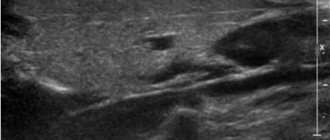
To clarify the nature and location of the fistula tract, an instrumental examination is carried out - anoscopy or retroromanoscopy, ultrasound or MRI.
Rehabilitation after paraproctitis removal
You need to spend several days in the hospital. In the early postoperative period after removal of a rectal fistula, there is a pronounced pain syndrome, an increase in body temperature and a deterioration in general health are possible. If possible, unpleasant symptoms are relieved. A course of antibiotics is required, usually intramuscularly.
One of the main aspects is hygiene. The wound healing process can be complicated by hair growing in the anal area. They need to be shaved or cut off so that there are no problems with treating the wound. Depilatory creams cannot be used. After each bowel movement, you need to thoroughly clean the anal area not only with toilet paper, but also with a disinfectant. You can do sitz baths with disinfectants or herbs. When going to the toilet there may be minor discharge and slight bruising. If the bleeding is severe, you should immediately consult a doctor.
An important part of rehabilitation is nutrition. Salty and spicy foods, sour foods, fresh fruits, alcohol, and sweet carbonated drinks should be excluded from the diet. There should not be “harmful” foods in the diet, that is, semi-finished products, chips, fast food. To improve the digestion process, you need to eat as much cereal as possible, dishes high in dietary fiber, and drink more clean water.
Every day after surgery to remove a rectal fistula, it is necessary to clean the sutures and make dressings. Sutures are usually treated with Chlorhexidine or antibacterial ointments. One of the best is Levomekol. Additionally, agents that accelerate healing are used. In some cases, physical therapy is prescribed to speed up recovery. These are magnetic therapy and UV irradiation.
Our surgery center features:
- more than 15 highly qualified surgeons on staff;
- the latest equipment;
- postoperative recovery of patients within 1 day.