Use of enterosorbent Polysorb MP in pediatric practice
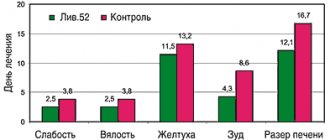
Enterosorption is an integral part of efferent therapy (from the Latin efferens - to remove), that is, a group of therapeutic measures whose ultimate goal is to stop the action of toxins of various origins and their elimination from the body. In addition to enterosorption, this group includes hemodialysis, peritoneal dialysis, plasmapheresis, hemosorption and some others. The basic requirements that enterosorbents must meet are the following: – do not have toxic properties; – be non-traumatic for mucous membranes; – good evacuation from the intestines; – have good functional (sorption) properties; – do not cause dysbacteriosis; – have a convenient dosage form. In Russia, a large number of different enterosorbents are sold and used, based on both wood and chemically synthesized materials. The most successful enterosorbent that meets the above requirements is the domestic silica-based sorbent Polysorb MP, which is produced in the Chelyabinsk region. The drug Polysorb MP is a new generation enterosorbent, created on the basis of natural highly dispersed silica, has multifunctional non-selective sorption properties, is available in powder form, particle size is from 5 to 20 nm. The main purpose of enterosorbents in general and Polysorb MP in particular is the removal of toxins of any origin from the body. In the lumen of the gastrointestinal tract, Polysorb MP binds and removes from the body endogenous and exogenous toxic substances of various natures, including microorganisms and microbial toxins, antigens, food allergens, drugs and poisons, heavy metal salts, radionucleotides, alcohol. Polysorb MP also sorbs some metabolic products of the body, including excess bilirubin, cholesterol and lipid complexes, metabolites of nitrogen metabolism, substances of “average molecular weight” responsible for the development of metabolic toxicosis. Indications for the use of Polysorb MP in pediatrics • Acute intestinal diseases accompanied by diarrheal syndrome (dysentery, salmonellosis, food toxic infections). • Hepatitis of any etiology (viral, toxic, autoimmune). • Endo- and exogenous intoxications of any origin. • Allergic reactions (drug and food allergies, including angioedema, diathesis, eczema, psoriasis, bronchial asthma, obstructive pulmonary diseases). • Chronic renal failure. Polysorb MP is not absorbed in the intestines and is excreted unchanged from the body, due to which it has practically no contraindications for use. This drug causes almost no allergic reactions (only in exceptional cases). Like other enterosorbents, Polysorb MP is used with caution during exacerbation of peptic ulcer disease and bleeding from the gastrointestinal tract. Method of administration and recommended doses The therapeutic dose of Polysorb is 100–200 mg/kg body weight per day. The maximum permissible daily dose for short-term use is 330 mg/kg. The sorbent is taken only in the form of an aqueous suspension. To prepare an aqueous suspension, take the required amount of the drug (1 heaped teaspoon contains 1 g, and 1 heaped tablespoon contains 3 g of the drug), place it in a glass containing 100 ml of water, and mix thoroughly. The resulting suspension of the drug is drunk 1 hour before or 1–2 hours after taking food or other medications. In general, the calculation of the dosage of Polysorb MP is very simple. The average therapeutic dose for an adult is 3–4 tablespoons per day. For children, recalculation is necessary using a table (Table 1). At the Smolensk Medical Academy A.I. Grekova et al. The clinical effectiveness of the enterosorbent “Polysorb MP” was assessed for acute intestinal infections (AIE) in children. AEs occupy one of the leading places in infectious morbidity. 60–65% of all cases of acute intestinal infections are registered among children, with a particularly high incidence in young children (up to 70%). According to the literature, the entire range of modern studies makes it possible to establish the etiology of acute intestinal infections in 56–80% of cases. Etiological agents such as Salmonella, Shigella, Vibrio cholerae cause no more than 10% of all cases of intestinal infections in children in civilized countries. The share of rotavirus infection in the structure of acute intestinal infections ranges from 9 to 73%, and of all children hospitalized for intestinal disorders, it is diagnosed in 20–60%. Changes in the etiological structure and pathogenesis of acute intestinal infections in children (an increase in the number of viral diarrhea), an increase in bacterial resistance to antibacterial drugs, and an increase in recent years in the number of adverse outcomes associated with a burdened premorbid background of patients dictate the need to search for new etiopathogenetic drugs and improve the treatment of patients with acute intestinal infections. The main directions of pathogenetic therapy of acute intestinal diseases accompanied by diarrhea syndrome: – detoxification; – correction of water and electrolyte disorders; – correction of motor-secretory disorders of the gastrointestinal tract; – correction of intestinal microflora disorders; – strengthening of reparative processes in the colon mucosa; – enterosorption. Enterosorption in infectious diseases is not only a pathogenetic method of therapy, but also an etiological one, since sorbents are capable of absorbing not only endo- and exotoxins of pathogens, but also fixing pathogens of a bacterial and viral nature on their surface, thus excluding them from the pathological process. The ability of enterosorbents to bind endo- and exotoxins of pathogens makes a significant contribution to the detoxification of the macroorganism. On the Russian pharmaceutical market, different groups of enterosorbents are represented by activated carbons, lignins, ion exchange resins, which have very different clinical effects, and sometimes unpleasant organoleptic properties (hydrolytic lignin). They have different levels of solubility and have different aromatic fragrances, which is important when used in children with allergy pathology and, of course, a possible traumatic effect on the intestinal mucosa. In this regard, the problem of producing new enterosorbent drugs that meet modern requirements, especially when used in children, remains relevant. The drug Polysorb MP is produced from finely dispersed silicas and meets all the basic requirements for enterosorbents: it is non-toxic, does not injure the gastrointestinal mucosa, is easily evacuated from the gastrointestinal tract, and has good sorption and organoleptic properties. Purpose of the work: to evaluate the clinical effectiveness of the enterosorbent drug “Polysorb MP”, to improve the pathogenetic therapy of acute intestinal infections in children accompanied by diarrhea syndrome. Materials and methods: for 2005–2006. 65 children who were undergoing inpatient treatment at the City Clinical Hospital No. 1 of Smolensk in department No. 5 (intestinal infections) were examined. To assess the effectiveness of the drug, clinical data were used to assess the phenomena of intoxication (duration of nausea, vomiting, loss of appetite), the severity of clinical signs of the disease (feverish period, abdominal syndrome, duration of diarrhea, the presence of pathological impurities in the stool), laboratory assessment of the isolation of pathogens - bacteriological and serological methods. Two groups of children were identified: study group “A” – 35 children who received, along with traditional basic (including specific antibacterial or antiviral) therapy, the enterosorbent drug “Polysorb MP”, and control group “B” – 30 children who received traditional basic (including specific antibacterial or antiviral) therapy. In terms of age structure, children under 5 years of age predominated in both groups (Fig. 1). In the etiological structure of both groups, the predominance of rotavirus infection was noted. Thus, in the study group there were 18 children (51.4%) with rotavirus infection, in the control group there were 13 children (43.3%) (Fig. 2). In terms of severity, a predominance of moderate forms was noted in both groups (Fig. 3). Assessment of intoxication syndrome. The disappearance of intoxication symptoms in the study group was completely noted on the 4th day with maximum extinction on days 1–2; in the control group, intoxication symptoms persisted until the 7th day with maximum extinction on days 2–4 (Fig. 4) . Dynamics of abdominal syndrome. Abdominal syndrome was relieved in the study group mainly by the 3rd day, in 25% of the control group it persisted until the 4th day (Fig. 5). Stool dynamics in the study group: in the vast majority, stools became formed by the 3rd day; in the control group, in 3.3% of cases, they remained liquid until the 8th day of illness. In the study group, pathological impurities disappeared by the end of 2–3 days, in the control group they persisted until 5 days (Fig. 6). When analyzing the data obtained, the dynamics presented in tables 1 and 2 were noted. In group “A”, in 2 cases of shigellosis (Shigella Flexner 2a was isolated), control stool cultures after therapy were negative. Of the 18 cases of rotavirus infection (laboratory confirmed), rotavirus was not isolated in control stool tests. In group “B”, in 2 cases of shigellosis, Shigella Flexneri 2a was isolated, in control cultures after therapy the result was negative. Of the 13 cases of rotavirus infection (laboratory confirmed), 5 cases had a positive control stool test for rotavirus. In both groups, 15 children were diagnosed with ACI, which was not laboratory confirmed. The development of adverse reactions and manifestations of hypersensitivity to the enterosorbent used in sick children have not been recorded. Thus, the data obtained indicate that: 1. When using the enterosorbent Polysorb MP in children with acute intestinal intoxication, rapid dynamics of relief of intoxication symptoms, normalization of stool character and the disappearance of pathological impurities were noted in comparison with the control group. 2. Against the background of the therapy, the study group achieved better sanitation of the intestines from pathogenic pathogens (for rotavirus infection). 3. The therapeutic effect of the drug Polysorb is associated with a reduction in the duration of the infectious disease, length of hospital stay, and a lower cost (compared to analogues), which suggests a possible positive economic effect. 4. The enterosorption method using the drug “Polysorb MP” can be recommended for the treatment of acute intestinal infections in children with intoxication and diarrhea syndrome. In many countries of the world, including Russia, allergic diseases and associated gastrointestinal pathology occupy a fairly large share among childhood diseases. The prevalence of various clinical forms of food allergies in Chelyabinsk is, according to our data (research by the Department of Childhood Diseases No. 1 during 1990–1997), about 10%, and gastrointestinal pathology - 32.2%. This determines great interest in various areas of therapy, methods of complex treatment of allergic diseases, as well as those occurring in combination with damage to the gastrointestinal tract. Despite clear advances in understanding these diseases and the increasing production of drugs, the problems of choosing the necessary drug and determining the minimum drug correction sometimes become crucial. The diversity of the clinical picture and outcomes of allergic diseases is often due to the concentration of biologically active substances and the severity of intestinal dysbiosis (ID). In the fight against these phenomena, an inorganic sorbent, Polysorb MP, can be successfully used. Without having a resorptive effect, it has unique sorbing properties. Polysorb MP promotes the binding and removal of many biologically active substances (histamine, serotonin, bradykinin, etc.), thus reducing the intensity of allergic inflammation in tissues. This ensures the antiallergic effect of the drug. The presence of DC, even subcompensated forms, often causes the presence of incomplete digestion products in the intestine. They, in turn, support the clinical manifestations of food allergies, since they themselves can be allergens, and at the same time increase inflammatory changes in the gastrointestinal mucosa due to direct irritant effects. We used Polysorb MP in the early childhood pathology department (35 children), gastroenterology (22 children) and allergology (34 children) departments of the children's clinic. In the early childhood pathology department, a course of treatment with Polysorb MP was mainly given to children with acute allergic reactions (AAR) and DC. The group of children with OAD consisted of 19 people (54% of the total number of children). Of these, generalized urticaria was observed in 10 children (28.5%), angioedema in 5 (14.2%), a combination of urticaria and angioedema in 4 children (14.3%). It should be noted that all children received standard proven therapy (diet, antihistamines, enzymes, biological products, hormones for severe damage). In addition, they were prescribed Polysorb MP. Treatment was carried out with a 3–5% aqueous suspension at a dose of 200 mg per 1 kg of body weight per day until the clinical symptoms subsided. In general, clinical manifestations decreased significantly on the second day of administration of this drug. Moreover, “fresh” allergic reactions (no more than a day old) tended to more quickly regress the main symptoms. This can be explained by the binding of the incorporated allergen from the intestinal lumen before it enters the bloodstream. In a comparative analysis of 23 case histories of children with OAR for 1996 (before the use of Polysorb MP), it was noted that the subsidence of clinical symptoms in children receiving Polysorb was observed on average 3.8 ± 0.4 days earlier than in children who received only standard therapy. In only one child with severe manifestations of food allergy, which occurred like giant urticaria, the clinical effect occurred much later, although it should be noted that he had a weak effect from the usually effective massive hormonal therapy. Apparently, this is due to the individual characteristics of the course of OAR in a given child. For the treatment of DC, 16 (45.7%) children received Polysorb. The drug was prescribed upon admission of children to the department as initial therapy for a course of 7–10 days; We used a 3–5% aqueous suspension at the rate of 100 mg of the drug per 1 kg of child weight. At the same time, the children received the usual standard therapy. Polysorb MP was taken 2 hours after taking food and other medications. In some children with a relapsing course of the disease, repeated courses of treatment were used with a break of 2 weeks. DC was characterized mainly by subcompensated forms: a change in the number and appearance of E. coli strains with altered properties, the identification of opportunistic flora in quantities exceeding 103–105 (staphylococcus, Klebsiella, Proteus, Candida, etc.) against the background of a decrease in bifid flora. At the same time, 6 children (37.5%) had unstable stools, and 10 children (62.5%) had constipation. When monitoring the results of bacteriological examination of feces after treatment, the high effectiveness of Polysorb MP was noted against opportunistic flora (reduced inoculation in 70% of cases), as well as E. coli with altered properties (43%). At the same time, in 80% of cases there was a decrease or complete absence of bifid flora. It seems that courses of treatment with Polysorb must be alternated with the prescription of biological products appropriate to the child’s age. It is important to note the normalization of the frequency and nature of stool in children during treatment with Polysorb. In the gastroenterology department, Polysorb MP was used to treat DC, but in children with chronic enterocolitis. Despite some differences in the nature of bacteriograms with infants (a larger percentage of seeding of opportunistic flora), in general, the same trends towards faster intestinal sanitation against the background of a remaining deficiency of bifid flora were noted. This pathology is characterized by persistent persistence of opportunistic flora. The results obtained indicate the advisability of using Polysorb MP in patients with chronic inflammatory bowel diseases, along with conventional methods of treating this pathology. In the allergy department, enterosorption with Polysorb was carried out for children of the older age group. The drug was prescribed for emergency indications to patients with OAR, starting from the first hours from the moment of admission to the department. The results obtained are statistically comparable with the data on the effectiveness of Polysorb in children of the younger age group with a similar pathology. Thus, the inorganic sorbent Polysorb is a highly effective drug for the treatment of allergic diseases associated with food sensitization, as well as DC. The effect we obtained gives reason to assume the possibility of a wider use of polysorb in chronic inflammatory diseases of the gastrointestinal tract and allergic diseases with various types of sensitization, as well as with combined gastrointestinal and allergic pathology.
Literature 1. “Enterosorbent Polysorb MP, methodological recommendations for clinical use” CJSC “Polisorb” Chelyabinsk 2007 2. “Modern view of the problem of enterosorption. Optimal approach to drug selection” N.I. Ursova, A.V. Gorelov. Russian Medical Journal No. 19 2006 3. “Infectious toxicoses in children” Uchaikin V.F., Molochny V.P. Moscow 2002
Nosological classification (ICD-10)
- A05.9 Bacterial food poisoning, unspecified
- B19 Viral hepatitis, unspecified
- K59.1 Functional diarrhea
- K63.8.0* Dysbacteriosis
- N18 Chronic renal failure
- R17 Unspecified jaundice
- T50.9 Other and unspecified drugs, medicinal products and biological substances
- T50.9.0* Alkaloid poisoning
- T51 Toxic effects of alcohol
- T56.9 Toxic effect of unspecified metal
- T65.9 Toxic effects of unspecified substance
- T78.4 Allergy, unspecified
- Y57 Adverse reactions during therapeutic use of other and unspecified drugs and medications
- Y97 Factors associated with environmental pollution
- Z57 Occupational exposure to hazards
Release form
Powder for the preparation of suspension for oral administration. 1/2/3/6/10/12 g in disposable bags made of label paper with a thermal layer. 1/2/3/4/5/10/30/50/100 disposable bags per cardboard box. It is allowed to place disposable bags directly into group packaging.
50 g in double PE bags or 5/10 kg in double PE bags (for hospitals). Packages of 50 g are placed in a cardboard box.
Also 12/15/20/25/30/35/40/45/50 g in polystyrene, PE or PET jars, sealed with lids made of similar materials. The jar is placed in a cardboard box or packed in shrink film in packs of 5 and 10 pcs.
Symptoms
The incubation period ranges from several hours to three days. Some time after infection, the patient begins to feel weak, nauseated, and the temperature rises. Then vomiting begins, it can be either single or multiple. In children, the symptoms are more pronounced and they suffer more severely from the disease. Then abdominal pain begins, which is accompanied by stool disturbances: at first it becomes mushy, then develops into diarrhea. After a few hours, the patient feels dry mouth - this is the first sign of dehydration. The patient loses weight, this is especially pronounced in children under one year old. Dehydration causes dry, cracked lips and sunken eyes. If the patient does not urinate after 6 hours, then this is a dangerous symptom of dehydration. If a child suffers a severe illness, it is best to hospitalize him. In a hospital setting, there are more opportunities to bring the child out of this state: droppers are used to eliminate dehydration.