Compound:
One tablet contains:
active substance
: azithromycin dihydrate in terms of azithromycin 250 mg/500 mg;
Excipients
: lactitol 300.0 mg / 600.0 mg, calcium phosphate dihydrate 59.8 mg / 119.6 mg, corn starch 24.0 mg / 48.0 mg, croscarmellose sodium 20.0 mg / 40.0 mg, magnesium stearate 6.0 mg / 12.0 mg, hypromellose 5.0 mg / 10.0 mg, sodium lauryl sulfate 1.2 mg / 2.4 mg, microcrystalline cellulose to obtain an uncoated tablet weighing 700 mg / 1400 mg;
Excipients of the shell:
hypromellose 9.49 mg/
18.98 mg, titanium dioxide 5.2 mg/10.4 mg, macrogol-4000 3.744 mg/7.488 mg, talc 1.12 mg/2.24 mg, povidone-K17 0.416 mg/0.832 mg, dye tropeolin O 0.030 mg / 0.060 mg to obtain a coated tablet weighing 720 mg / 1440 mg
Description:
Capsule-shaped biconvex tablets, yellow film-coated. On a cross section, two layers are visible, the inner layer is white or almost white.
Pharmacological group:
antibiotic – azalide
ATX code:
J01FA10.
pharmachologic effect
Pharmacological properties
Pharmacodynamics
Azithromycin is a broad-spectrum bacteriostatic antibiotic from the macrolide-azalide group. Has a wide spectrum of antimicrobial action. The mechanism of action of azithromycin is associated with the suppression of protein synthesis in microbial cells. By binding to the 50S ribosomal subunit, it inhibits peptide translocase at the translation stage and suppresses protein synthesis, slowing down the growth and reproduction of bacteria. In high concentrations it has a bactericidal effect.
It is active against a number of gram-positive, gram-negative, anaerobes, intracellular and other microorganisms.
Microorganisms may initially be resistant to the action of an antibiotic or become resistant to it.
Scale of sensitivity of microorganisms to azithromycin (minimum inhibitory concentration (MIC), mg/ml)
| Microorganisms | MIC, mg/l | |
| Sensitive | Sustainable | |
| Staphylococcus | ≤ 1 | ˃ 2 |
| Streptococcus A, B, C, G | ≤ 0,25 | ˃ 0,5 |
| Streptococcus pneumoniae | ≤ 0,25 | ˃ 0,5 |
| Haemophilus influenzae | ≤ 0,12 | ˃ 4 |
| Moraxella catarrhalis | ≤ 0,5 | ˃ 0,5 |
| Neisseria gonorrhoeae | ≤ 0,25 | ˃ 0,5 |
In most cases, sensitive microorganisms:
- Gram-positive aerobes:
- Staphylococcus aureus (methicillin-sensitive)
- Streptococcus pneumoniae (penicillin-sensitive)
- Streptococcus pyogenes
- Gram-negative aerobes:
- Haemophilus influenzae
- Haemophilus parainfluenzae
- Legionella pneumophila
- Moraxella catarrhalis
- Pasteurella multocida
- Neisseria gonorrhoeae
- Anaerobes:
- Clostridium perfringens
- Fusobacterium spp.
- Prevotella spp.
- Porphyromonas spp.
- Other microorganisms:
- Chlamydia trachomatis
- Chlamydia pneumoniae
- Chlamydia psittaci
- Mycoplasma pneumoniae
- Mycoplasma hominis
- Borrelia burgdorferi
Microorganisms that can develop resistance to azithromycin:
gram-positive aerobes:
Streptococcus pneumoniae (penicillin resistant)
Initially resistant microorganisms:
gram-positive aerobes:
Enterococcus faecalis
Staphylococcus (methicillin-resistant staphylococci show a very high degree of resistance to macrolides) gram-positive bacteria resistant to erythromycin
anaerobes
Bacteroides fragilis
Pharmacokinetics
After oral administration, azithromycin is well absorbed and quickly distributed in the body. Bioavailability after a single dose of 500 mg is 37% (the “first pass” effect), the maximum concentration (0.4 mg/l) in the blood is created after 2-3 hours, the apparent volume of distribution is 31.1 l/kg, protein binding plasma inversely proportional to the concentration in the blood is 7-50%. Penetrates through cell membranes (effective against infections caused by intracellular pathogens).
Transported by phagocytes to the site of infection, where it is released in the presence of bacteria. Easily passes histohematic barriers and enters tissues. The concentration in tissues is 10-50 times higher than in plasma, and at the site of infection it is 24-34% higher than in healthy tissues.
Azithromycin has a very long half-life - 35-50 hours. The half-life from tissues is much longer. The therapeutic concentration of azithromycin lasts up to 5-7 days after taking the last dose. Azithromycin is excreted mainly unchanged - 50% by the intestines, 6% by the kidneys. In the liver it is demethylated, losing activity.
Azithromycin Ecomed - Suspension
Home / Ecoanalogues / Azithromycin Ecomed / Suspension
A broad-spectrum antibacterial drug from the group of macrolides-azalides, it acts bacteriostatically. By binding to the 50S ribosomal subunit, it inhibits peptide translocase at the translation stage, suppresses protein synthesis, slows down the growth and reproduction of bacteria, and in high concentrations has a bactericidal effect. Acts on extra- and intracellularly located pathogens. Azithromycin Ecomed can be considered as the drug of choice for patients with an allergy to β-lactam antibiotics in respiratory pathology, especially in people with an increased risk of developing dysbiosis.
Registration number: Trade name of the drug: Azithromycin Ecomed® International non-proprietary or generic name: azithromycin Dosage form: powder for the preparation of a suspension for oral administration. Description: White or yellowish-white powder with a faint fruity odor. Ready suspension: white to light yellow, homogeneous with a faint fruity odor. Pharmacotherapeutic group: antibiotic – azalide. ATX code: J01FA10
Expand all
Composition Expand
5 ml of the finished suspension (one dosage spoon) contains: Active substance: azithromycin dihydrate (in terms of azithromycin) - 100 mg/200 mg; Excipients: lactitol – 200.0 mg/400.0 mg, xanthan gum – 15.0 mg/15.0 mg, crospovidone (Kollidon CL-M) – 65.0 mg/65.0 mg, colloidal silicon dioxide ( aerosil) – 5.5 mg/5.5 mg, anhydrous sodium carbonate – 83.0 mg/83.0 mg, sodium benzoate – 16.5 mg/16.5 mg, titanium dioxide – 10.0 mg/10, 0 mg, strawberry flavor – 55.0 mg/55.0 mg, mint flavor – 0.5 mg/0.5 mg, apple-cinnamon flavor – 27.5 mg/27.5 mg, sucrose – up to 3.75 g/3.75 g.
Pharmacological action Expand
A broad-spectrum antibacterial drug from the group of macrolides-azalides, has a bacteriostatic effect. By binding to the 50S ribosomal subunit, it inhibits peptide translocase at the translation stage, suppresses protein synthesis, slows down the growth and reproduction of bacteria, and in high concentrations has a bactericidal effect. Acts on extra- and intracellularly located pathogens. Microorganisms may be initially resistant to the action of an antibiotic or may acquire resistance to it. Scale of sensitivity of microorganisms to azithromycin (Minimum inhibitory concentration, mg/l): Staphylococcus: sensitive ≥1 mg/l, resistant >2 mg/l; Streptococcus A, B, C, G: sensitive ≤0.25 mg/l, resistant >0.5 mg/l; Streptococcus pneumoniae: sensitive ≥0.25 mg/l, resistant >0.5 mg/l; Haemophilus influenzae: sensitive ?0.12 mg/l, resistant >4 mg/l; Moraxella catarrhalis: sensitive ≤0.5 mg/l, resistant >0.5 mg/l; Neisseria gonorrhoeae: sensitive ≤0.25 mg/l, resistant >0.5 mg/l; Sensitive:
- aerobic gram-positive microorganisms: Staphylococcus aureus (methicillin-sensitive), Streptococcus pneumoniae (penicillin-sensitive), Streptococcus pyogenes;
- aerobic gram-negative microorganisms: Haemophilus influenzae, Haemophilus parainfluenzae, Legionella pneumophila, Moraxella catarrhalis, Pasteurella multocida, Neisseria gonorrhoeae;
- anaerobic microorganisms: Clostridium perfringens, Fusobacterium spp., Prevotella spp., Porphyromonas spp.;
- other: Chlamydia trachomatis, Chlamydia pneumoniae, Chlamydia psittaci, Mycoplasma pneumoniae, Mycoplasma hominis, Borrelia burgdorferi.
Moderately sensitive or insensitive:
- aerobic gram-positive microorganisms: Streptococcus pneumoniae (moderately sensitive or resistant to penicillin).
Resistant:
- aerobic gram-positive microorganisms: Enterococcus faecalis, Staphylococci spp. (methicillin-resistant).
- anaerobes: Bacteroides fragilis group. Streptococcus pneumoniae, beta-hemolytic Streptococcus spp. group A, Enterococcus faecalis and Staphylococcus aureus (including methicillin-sensitive strains), resistant to erythromycin and other macrolides, lincosamides, and resistant to azithromycin.
Pharmacokinetics Expand
After oral administration, azithromycin is well absorbed and quickly distributed in the body. Bioavailability after a single dose of 0.5 g is 37% (the “first pass” effect through the liver), maximum concentration (Cmax) after oral administration of 0.5 g is 0.4 mg/l, time to reach maximum concentration (TCmax) is 2 -3 hours. Concentration in tissues and cells is 10-50 times higher than in serum. The volume of distribution is 31.1 l/kg, binding to plasma proteins is inversely proportional to the concentration in the blood and remains 7-50%. Azithromycin is acid-stable and lipophilic. Easily passes through histohematic barriers, penetrates well into the respiratory tract, internal organs and tissues, including the prostate gland, skin and soft tissues. It is also transported to the site of infection by phagocytes, polymorphonuclear leukocytes and macrophages, where it is released in the presence of bacteria. Penetrates through cell membranes and creates high concentrations in them, which is especially important for the eradication of intracellular pathogens. In foci of infection, the concentration is 24-34% higher than in healthy tissues, and correlates with the severity of the inflammatory process. Remains in effective concentrations for 5-7 days after taking the last dose. It is demethylated in the liver, the resulting metabolites are not active. The metabolism of the drug involves isoenzymes CYP3A4, CYP3A5, CYP3A7, of which it is an inhibitor. Plasma clearance - 630 ml/min: half-life between 8 and 24 hours after administration - 14-20 hours, half-life in the range from 24 to 72 hours - 41 hours. More than 50% of the drug is excreted through the intestines unchanged, 6% - kidneys. Food intake significantly changes pharmacokinetics: Cmax increases (by 31%), the area under the concentration-time curve (AUC) does not change. In elderly men (65-85 years old), the pharmacokinetic parameters do not change; in women, Cmax increases (by 30-50%).
Indications for use Expand
Infectious and inflammatory diseases caused by microorganisms sensitive to azithromycin:
- infections of the upper respiratory tract and ENT organs: pharyngitis, tonsillitis, sinusitis, otitis media;
- lower respiratory tract infections: acute bronchitis, exacerbation of chronic bronchitis, pneumonia, incl. caused by atypical pathogens;
- infections of the skin and soft tissues: erysipelas, impetigo, secondary infected dermatoses;
- the initial stage of Lyme disease (borreliosis) – erythema migrans;
Contraindications Expand
Contraindications:
- hypersensitivity to azithromycin (including other macrolides) or other components of the drug;
- severe renal failure (creatinine clearance (CC) less than 40 ml/min);
- severe liver failure (class C on the Child-Pugh scale);
- breast-feeding;
- simultaneous use with ergotamine and dihydroergotamine;
- children up to 6 months;
- sucrase/isomaltase deficiency, fructose intolerance, glucose-galactose malabsorption.
Carefully:
- renal failure (creatinine clearance (CC) more than 40 ml/min);
- liver failure (class A and B on the Child-Pugh scale);
- with arrhythmias or predisposition to arrhythmias and prolongation of the QT interval;
- with the combined use of terfenadine, warfarin, digoxin;
- myasthenia gravis.
Use during pregnancy and lactation Expand
Azithromycin is recommended to be prescribed during pregnancy only in cases where the expected benefit to the mother outweighs the potential risk to the fetus. During treatment with azithromycin, breastfeeding is suspended.
Dosing regimen Expand
Azithromycin Ecomed® in the form of an oral suspension is prescribed to children from 6 months. 3-day course: at the rate of 10 mg/kg 1 time per day (course dose 30 mg/kg). 5-day course: for Lyme disease (borreliosis) for the treatment of stage I (erythema migrans) in children, the dose is 20 mg/kg on the first day and 10 mg/kg from days 2 to 5 of the disease; course dose 60 mg/kg. Method of preparing the suspension The suspension is prepared immediately before use. The powder in the bottle is first shaken, 12 ml of boiled and cooled to room temperature water is added using a dosing syringe, mixed to obtain a homogeneous suspension. To accurately dose the suspension, use a double-sided dosing spoon or syringe, which should be rinsed well with water after each use. After dilution, the prepared suspension should be stored for no more than 5 days in the refrigerator, but not frozen.
Side effect Expand
From the digestive system: nausea, vomiting, diarrhea, abdominal pain, loose stools, flatulence, indigestion, anorexia, constipation, discoloration of the tongue, pseudomembranous colitis, cholestatic jaundice, hepatitis, changes in laboratory parameters of liver function, liver failure, liver necrosis (possibly fatal), hyperbilirubinemia, pancreatitis, fulminant hepatitis. Allergic reactions: itching, skin rashes, angioedema, urticaria, photosensitivity, anaphylactic reaction (in rare cases fatal), erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis. From the cardiovascular system: palpitations, arrhythmia, ventricular tachycardia, increased QT interval, bidirectional ventricular tachycardia, decreased blood pressure. From the nervous system: dizziness/vertigo, headache, convulsions, drowsiness, paresthesia, asthenia, insomnia, hyperactivity, aggressiveness, anxiety, nervousness, fainting, myasthenia. From the senses: tinnitus, reversible hearing loss up to deafness (when taking high doses for a long time), impaired perception of taste and smell, impaired clarity of visual perception. From the hematopoietic organs: thrombocytopenia, neutropenia. Eosinophilia, lymphopenia, hemolytic anemia. From the musculoskeletal system: arthralgia. From the genitourinary system: interstitial nephritis, acute renal failure, increased concentrations of urea and creatinine in the blood plasma. Other: vaginitis, candidiasis, weakness, peripheral edema, malaise.
Overdose Expand
Symptoms: temporary hearing loss, nausea, vomiting, diarrhea. Treatment is symptomatic.
Interaction with other drugs Expand
Antacids (aluminum- and magnesium-containing) do not affect bioavailability, but reduce the concentration of azithromycin in the blood by 30%, so the interval between their administration should be 1 hour before or 2 hours after taking these drugs. When used simultaneously with ergotamine and dihydroergotamine derivatives, the toxic effect of the latter may be enhanced (vasospasm, dysesthesia). When used together with indirect coumarin anticoagulants (warfarin), patients need careful monitoring of prothrombin time. Caution must be exercised when co-administering terfenadine and azithromycin, since concomitant use of terfenadine and macrolides has been found to cause arrhythmia and prolongation of the QT interval. Based on this, the above complications cannot be excluded when taking terfenadine and azithromycin together. When used simultaneously with cyclosporine, it is necessary to monitor the concentration of cyclosporine in the blood. When used simultaneously with digoxin, it is necessary to control the concentration of digoxin in the blood (it is possible to increase the absorption of digoxin in the intestine). When used simultaneously with nelfinavir, it is possible to increase the frequency of adverse reactions of azithromycin (decreased hearing, increased activity of liver transaminases). When used simultaneously with zidovudine, azithromycin does not affect the pharmacokinetic parameters of zidovudine in the blood plasma or the renal excretion of it and its metabolite, glucuronide, but the concentration of the active metabolite of phosphorylated zidovudine in mononuclear cells of peripheral vessels increases. The clinical significance of this fact has not been determined. The possibility of inhibition of the CYP3A4 isoenzyme by azithromycin should be taken into account when used simultaneously with cyclosporine, terfenadine, ergot alkaloids, cisapride, pimozide, quinidine, astemizole and other drugs whose metabolism occurs with the participation of this enzyme. Azithromycin does not affect the blood concentrations of carbamazepine, cimetidine, didanosine, efavirenz, fluconazole, indinavir, midazolam, theophylline, triazolam, trimethoprim/sulfamethoxazole, cetirizine, sildenafil, atorvastatin, rifabutin and methylprednisolone when used simultaneously.
Special instructions Expand
If a dose is missed, the missed dose should be taken as soon as possible, and subsequent doses should be taken 24 hours apart. Azithromycin should be taken 1 hour before or 2 hours after taking antacid medications. Use with caution in patients with moderate hepatic impairment due to the possibility of developing fulminant hepatitis and severe liver failure. If there are symptoms of liver dysfunction (rapidly increasing asthenia, jaundice, darkening of urine, tendency to bleeding, hepatic encephalopathy), azithromycin therapy should be discontinued and a study of the functional state of the liver should be performed. In case of moderate renal failure (creatinine clearance more than 40 ml/min), the use of azithromycin should be carried out under the control of renal function. Concomitant use of azithromycin with ergotamine and dihydroergotamine derivatives is contraindicated due to the possible development of ergotism. When using the drug, both while taking it and 2-3 weeks after stopping treatment, diarrhea caused by Clostridium difficile (pseudomembranous colitis) may develop. In mild cases, it is sufficient to discontinue treatment and use ion-exchange resins (colestyramine, colestipol); in severe cases, replacement of loss of fluid, electrolytes and protein, and the appointment of vancomycin, bacitracin or metronidazole are indicated. Do not use medications that inhibit intestinal motility. Since QT interval prolongation is possible in patients receiving macrolides, caution should be exercised when using azithromycin in patients with known risk factors for QT interval prolongation: advanced age; electrolyte imbalance (hypokalemia, hypomagnesemia); congenital long QT syndrome; heart disease (heart failure, myocardial infarction, bradycardia); simultaneous use of drugs that can prolong the QT interval (including antiarrhythmic drugs of classes IA and III, tricyclic and tetracyclic antidepressants, antipsychotics, fluoroquinolones). When using azithromycin, myasthenic syndrome or exacerbation of myasthenia may develop. Effect on the ability to drive vehicles and machinery During the treatment period, care must be taken when driving vehicles and engaging in other potentially hazardous activities that require increased concentration and speed of psychomotor reactions.
Release form Expand
Powder for the preparation of suspension for oral administration 100 mg/5 ml, 200 mg/5 ml. 16.5 g in 60 ml dark glass bottles with a screw-on plastic cap. One bottle along with a double-sided dosing spoon (small with a capacity of 2.5 ml, large - 5 ml), a syringe for dosing and instructions for use are placed in a cardboard pack.
Expiration date Expand
2 years. Ready suspension – 5 days. Do not use after expiration date.
Storage conditions Expand
In a place protected from moisture and light at a temperature not exceeding 25 ° C. The finished suspension is stored at a temperature from 2? C to 8? C in a tightly closed bottle. Keep out of the reach of children.
Vacation conditions Expand
On prescription.
Owner of the registration certificate Expand
JSC "AVVA RUS", Russia, 121614 Moscow, st. Krylatsky Hills. 30, bldg. 9. Tel. www.avva-rus.ru
Manufacturer/organization receiving claims Expand
JSC "AVVA RUS", Russia, 610044 Kirov, st. Luganskaya, 53A. Tel., www.avva-rus.ru, www.ecoantibiotic.ru Send consumer complaints to the manufacturer.
Share information:
Indications for use
Infectious and inflammatory diseases caused by microorganisms sensitive to the drug:
- infections of the upper respiratory tract and ENT organs: pharyngitis, tonsillitis, sinusitis, otitis media;
- lower respiratory tract infections: acute bronchitis, exacerbation of chronic bronchitis, pneumonia, incl. caused by atypical pathogens;
- infections of the skin and soft tissues: acne vulgaris of moderate severity, erysipelas, impetigo, secondary infected dermatoses;
- the initial stage of Lyme disease (borreliosis) – erythema migrans;
- urinary tract infections caused by Chlamydia trachomatis (urethritis, cervicitis).
Azithromycin Pharmland tablets p/o 500 mg No. 3x2
Name
Azithromycin Pharmland tablet p/o 500 mg in container pack No. 3x2
Description
Tablets 500 mg: pink, oblong, biconvex, film-coated, scored on one side.
Main active ingredient
Azithromycin
Release form
Film-coated tablets
Dosage
500mg
Indications for use
Treatment of infectious diseases caused by microorganisms sensitive to Azithromycin:
- Upper respiratory tract infections (acute and chronic bacterial pharyngitis/tonsillitis, sinusitis, acute otitis media);
- Lower respiratory tract infections (acute bacterial bronchitis, exacerbation of chronic bronchitis, community-acquired bacterial pneumonia, including those caused by atypical pathogens);
- infections of the skin and soft tissues (uncomplicated forms of achne vulgaris, chronic migratory erythema (initial stage of Lyme disease), erysipelas, impetigo, secondary pyodermatoses);
- Sexually transmitted infections (urethritis, cervicitis);
- Diseases of the stomach and duodenum associated with Helicobacter pylori.
Directions for use and doses
Take Azithromycin strictly as prescribed by your doctor. If you are not sure about something, ask again. Azithromycin is taken orally, without chewing, 1 time per day, one hour before meals or two hours after meals, since food affects the absorption of Azithromycin. Usual dose for adults and children weighing ? 45 kg: 500 mg 1 time per day for 3 days. For various diseases, the doctor may prescribe doses and treatment regimens that differ from the above. If you are not sure about something, ask again. Carefully read the dosage instructions on the package, this will help you take the required number of tablets. Continue treatment as prescribed by your doctor, even if you feel better. If there is no improvement after completing the prescribed course of treatment, consult a doctor.
Use during pregnancy and lactation
If you are pregnant (or think you may be pregnant), or breastfeeding, be sure to consult a physician before use. Effect on the ability to drive a car and use machinery. Does not affect the ability to drive a car or use machinery.
Precautionary measures
If you have any liver, kidney or heart problems; If you are taking ergot alkaloid derivatives: ergotamine, dihydroergotamine; If you are pregnant or breastfeeding.
Interaction with other drugs
- Ergot alkaloid derivatives: ergotamine, dihydroergotamine;
- warfarin or other medicines to reduce blood clotting;
- Cyclosporine (for immunosuppression);
- Antacids (to reduce stomach acidity);
- Digoxin (to treat heart failure);
- Terfenadine (to treat allergic reactions).
Tell your doctor if you are taking any other medicines not listed on this list.
Contraindications
- you are allergic to Azithromycin, other macrolide antibiotics (erythromycin, clarithromycin) or to any other component of the drug;
- If you take ergot alkaloid derivatives: ergotamine, dihydroergotamine (ergotoxicity may develop).
Compound
Each Azithromycin tablet contains 250 mg or 500 mg of the active substance azithromycin and excipients: sodium starch glycolate, microcrystalline cellulose, talc, sodium lauryl sulfate, magnesium stearate, corn starch; shell – Opadry II pink (polyvinyl alcohol, macrogol, titanium dioxide, talc, red charm (E 129), tartrazine (E 102)). This medicine belongs to the group of macrolide antibiotics. Antibiotics inhibit the growth of microorganisms that cause infections.
Overdose
If the number of tablets per day you take is more than the number recommended by your doctor, or your child swallows the tablets, contact your doctor or call an ambulance.
Side effect
If any of the following symptoms occur during treatment with Azithromycin, stop taking the medication immediately and contact your doctor:
- Loose stools for a long time, possibly with blood or mucus in it. Loose stools may appear even two months after taking Azithromycin;
- Sudden wheezing, difficulty breathing, swelling of the face or difficulty swallowing, rash, itching, especially all over the body. These symptoms may indicate an allergic reaction;
- Severe skin disorders with blistering on the skin, mouth, lips, eyes or genitals. These are symptoms of a rare allergic reaction called toxic epidermal necrolysis;
- fast or irregular heart rhythm;
- Low blood pressure.
The most common side effects when taking Azithromycin (affect 1 in 10 people):
- Stomach cramps;
- Weakness;
- Stool disorder.
Common side effects when taking Azithromycin (occur less than 1 in 10 people):
- Dizziness, headache;
- Numbness, tingling;
- Weakness, indigestion;
- Loss of appetite, taste disturbance;
- Visual and hearing impairment;
- rash or peeling skin;
- Joint pain;
- Low number of lymphocytes, high number of eosinophils in the blood;
- Fatigue, weakness.
Other rarer side effects of Azithromycin (occurring in less than one in 100 people):
- Fungal diseases of the mouth or genitals;
- Low number of leukocytes, neutrophils in the blood;
- Allergic reactions of varying severity;
- blisters on the skin, mouth, lips, eyes, or genitals;
- Skin sensitivity to sunlight;
- Nervousness;
- Decreased sensitivity;
- Deterioration of hearing, circles before the eyes;
- Palpitations, chest pain;
- Constipation or stomach pain, accompanied by loose stools and fever;
- Inflammation of the liver and changes in liver tests;
- General weakness;
- Swelling;
- General discomfort;
- Changes in blood tests.
Be sure to consult your doctor if any of these symptoms appear, if they persist and bother you, or if you experience any other symptoms that are unusual and not described in this leaflet!
Storage conditions
Store in a place protected from moisture and light at a temperature not exceeding 25°C. Keep out of the reach of children.
Buy Azithromycin Pharmland tablet p/o 500 mg in container pack No. 3x2 in the pharmacy
Price for Azithromycin Pharmland tablet p/o 500 mg in container pack No. 3x2
Instructions for use for Azithromycin Pharmland tablet p/o 500 mg in container pack No. 3x2
Carefully
- myasthenia gravis;
- mild to moderate liver dysfunction;
- mild to moderate renal dysfunction (creatinine clearance more than 40 ml/min);
- in patients with the presence of proarrhythmogenic factors (especially in elderly patients): with congenital or acquired prolongation of the QT interval, in patients receiving therapy with antiarrhythmic drugs of classes IA (quinidine, procainamide), III (dofetilide, amiodarone and sotalol), cisapride, terfenadine, antipsychotics drugs (pimozide), antidepressants (citalopram), fluoroquinolones (moxifloxacin and levofloxacin), with disturbances in water and electrolyte balance, especially in the case of hypokalemia or hypomagnesemia, with clinically significant bradycardia, cardiac arrhythmia or severe heart failure;
- simultaneous use of terfenadine, warfarin, digoxin, cyclosporine.
Directions for use and doses
Azithromycin Ecomed® is taken orally, without chewing, 1 time per day, regardless of meals. The drug is taken at least 1 hour before or 2 hours after meals.
Adults (including elderly people) and children over 12 years of age weighing over 45 kg.
For infections of the upper and lower respiratory tract, ENT organs, skin and soft tissues: 0.5 g per day for 3 days (course dose – 1.5 g).
For moderate acne: 0.5 g per day for 3 days, then 0.5 g once a week for 9 weeks. The first weekly tablet should be taken 7 days after taking the first daily tablet (8th day from the start of treatment), the subsequent 8 weekly tablets should be taken at intervals of 7 days. Course dose 6.0 g.
For migratory erythema: 1 time per day for 5 days, 1st day 1.0 g, then from 2nd to 5th day 0.5 g. Course dose 3.0 g.
For urinary tract infections caused by Chlamydia trachomatis (urethritis, cervicitis): 1.0 g once.
When used in patients with mild renal impairment, no dose adjustment is required.
When used in patients with mild to moderate liver dysfunction, no dose adjustment is required in elderly patients.
Elderly patients: no dose adjustment is required. Caution should be exercised in elderly patients with persistent proarrhythmogenic factors due to the high risk of developing arrhythmias, including arrhythmias.
Side effect
The frequency of side effects is classified in accordance with WHO recommendations: very often - at least 10%; often - at least 1%, but less than 10%; infrequently - not less than 0.1%, but less than 1%; rarely - not less than 0.01%, but less than 0.1%; very rarely - less than 0.01%; unknown frequency—cannot be estimated from available data.
Infectious diseases:
uncommon - candidiasis, incl. mucous membrane of the oral cavity and genitals, pneumonia, pharyngitis, gastroenteritis, respiratory diseases, rhinitis; unknown frequency - pseudomembranous colitis.
From the blood and lymphatic system:
uncommon - leukopenia, neutropenia, eosinophilia; very rarely - thrombocytopenia, hemolytic anemia.
Metabolism and nutrition:
infrequently - anorexia.
Allergic reactions:
uncommon - angioedema, hypersensitivity reaction; unknown frequency - anaphylactic reaction.
From the nervous system:
often - headache; infrequently - dizziness, disturbance of taste, paresthesia, drowsiness, insomnia, nervousness; rarely - agitation; unknown frequency - hypoesthesia, anxiety, aggression, fainting, convulsions, psychomotor hyperactivity, loss of smell, perversion of smell, loss of taste, myasthenia gravis, delirium, hallucinations.
From the side of the organ of vision:
infrequently - visual impairment.
Hearing and labyrinth disorders:
uncommon - hearing loss, vertigo; unknown frequency - hearing loss, incl. deafness and/or tinnitus.
From the cardiovascular system:
infrequently - palpitations, flushing of the face; unknown frequency - decreased blood pressure, increased QT interval on ECG, ari, ventricular tachycardia.
From the respiratory system:
infrequently - shortness of breath, nosebleeds.
From the gastrointestinal tract:
very often - diarrhea; often - nausea, vomiting, abdominal pain; uncommon - flatulence, dyspepsia, constipation, gastritis, dysphagia, bloating, dry oral mucosa, belching, ulcers of the oral mucosa, increased secretion of the salivary glands; very rarely - change in tongue color, pancreatitis.
From the liver and biliary tract:
uncommon - hepatitis; rarely - impaired liver function, cholestatic jaundice; unknown frequency - liver failure (in rare cases with death, mainly due to severe liver dysfunction); liver necrosis, fulminant hepatitis.
For the skin and subcutaneous tissues:
uncommon - skin rash, itching, urticaria, dermatitis, dry skin, sweating; rarely - photosensitivity reaction; unknown frequency - Stevens-Johnson syndrome, toxic epidermal necrolysis, erythema multiforme.
From the musculoskeletal system:
uncommon - osteoarthritis, myalgia, back pain, neck pain; unknown frequency - arthralgia.
From the kidneys and urinary tract:
uncommon - dysuria, pain in the kidney area; unknown frequency - interstitial nephritis, acute renal failure.
From the genital organs and breast:
infrequently - metrorrhagia, testicular dysfunction.
Other:
uncommon - asthenia, malaise, feeling of fatigue, facial swelling, chest pain, fever, peripheral edema.
Laboratory data:
often - a decrease in the number of lymphocytes, an increase in the number of eosinophils, an increase in the number of basophils, an increase in the number of monocytes, an increase in the number of neutrophils, a decrease in the concentration of bicarbonates in the blood plasma; infrequently - increased activity of AST, ALT, increased concentration of bilirubin in the blood plasma, increased concentration of urea in the blood plasma, increased concentration of creatinine in the blood plasma, change in the potassium content in the blood plasma, increased activity of alkaline phosphatase in the blood plasma, increased chlorine content in the blood plasma, increased blood glucose concentration, increased platelet count, increased hematocrit, increased plasma bicarbonate concentration, change in plasma sodium content.
Azithromycin ecomed 100mg/5ml 16.5g powder for suspension for oral administration
pharmachologic effect
Antibiotic – azalide.
Composition and release form Azithromycin ecomed 100 mg/5 ml 16.5 g powder for the preparation of suspension for oral administration
Suspension - 5 ml:
- Active ingredient: azithromycin dihydrate - 104.82 mg (in terms of azithromycin - 100.00 mg);
- Excipients: lactitol - 200.00 mg; sodium carbonate anhydrous - 83.00 mg; crospovidone (kollidon CL-M) - 65.00 mg; strawberry flavoring - 55.00 mg; sodium benzoate - 16.50 mg; xanthan gum - 15.00 mg; apple flavoring - 13.75 mg; cinnamon flavoring - 13.75 mg; titanium dioxide - 10.00 mg; colloidal silicon dioxide - 5.50 mg; mint flavor - 0.50 mg; sucrose to weight - 3.75 g.
16.5 g in 60 ml dark glass bottles with a screw-on plastic cap with a silica gel insert.
1 bottle along with a syringe for dosing and instructions for use is placed in a cardboard pack.
Description of the dosage form
White or yellowish-white powder with a faint fruity odor. Ready suspension: white to light yellow, homogeneous with a faint fruity odor.
Directions for use and doses
Orally (the method of administration is determined by the release form), 1 time per day, 1 hour before or 2 hours after meals.
After taking the drug, the child must be offered to drink a few sips of water so that he can swallow the remainder of the suspension.
Before each dose of the drug, it must be shaken thoroughly until a homogeneous suspension is obtained. If the required volume of suspension has not been taken within 20 minutes after shaking, the suspension should be shaken again, the required volume taken and given to the child.
For infections of the upper and lower respiratory tract, ENT organs, skin and soft tissues.
At the rate of 10 mg/kg body weight 1 time per day for 3 days (course dose 30 mg/kg).
For precise dosing of azithromycin in accordance with the child’s body weight according to the scheme:
- Body weight 10-14 kg - Dose of 100 mg of azithromycin (2.5 ml suspension) per 1 dose.
- Body weight 15-24 kg - Dose of 200 mg of azithromycin (5.0 ml suspension) per 1 dose.
- Body weight 25-34 kg - Dose of 300 mg of azithromycin (7.5 ml suspension) per 1 dose.
- Body weight 35-44 kg - Dose of 400 mg of azithromycin (10.0 ml suspension) per 1 dose.
- Body weight of at least 45 kg - Dose of 500 mg of azithromycin (12.5 ml of suspension - corresponds to the dose for adult patients) per 1 dose.
Children weighing up to 10 kg should take azithromycin in powder form to prepare an oral suspension with a concentration of 100 mg/5 ml.
To accurately dose azithromycin according to the child's body weight, use the following regimen:
- Body weight 5 kg - Dose of 50 mg of azithromycin (2.5 ml suspension) per 1 dose.
- Body weight 6 kg - Dose of 60 mg of azithromycin (3.0 ml suspension) per 1 dose.
- Body weight 7 kg - Dose of 70 mg of azithromycin (3.5 ml suspension) per 1 dose.
- Body weight 8 kg - Dose of 80 mg of azithromycin (4.0 ml suspension) per dose.
- Body weight 9 kg - Dose of 90 mg of azithromycin (4.5 ml suspension) per 1 dose.
- Body weight 10 kg - Dose of 100 mg of azithromycin (5 ml suspension) per 1 dose.
For pharyngitis/tonsillitis caused by Streptococcus pyogenes, azithromycin is used at a dose of 20 mg/kg/day for 3 days (course dose 60 mg/kg). The maximum daily dose is 500 mg.
For Lyme disease (the initial stage of borreliosis) - erythema migrans.
On the 1st day at a dose of 20 mg/kg/day, then from the 2nd to the 5th day at a dose of 10 mg/kg/day (course dose 60 mg/kg).
In case of impaired renal function.
In patients with GFR (glomerular filtration rate) 10-80 ml/min, no dose adjustment is required.
In case of liver dysfunction.
When used in patients with mild to moderate liver dysfunction, no dose adjustment is required.
Elderly patients
No dose adjustment is required. In elderly patients, special caution is recommended when using azithromycin due to the possible presence of proarrhythmogenic factors that may increase the risk of developing cardiac arrhythmia and arrhythmias.
Pharmacodynamics
A broad-spectrum antibacterial drug from the group of macrolides-azalides, has a bacteriostatic effect. By binding to the 50S ribosomal subunit, it inhibits peptide translocase at the translation stage, suppresses protein synthesis, slows down the growth and reproduction of bacteria, and in high concentrations has a bactericidal effect. Acts on extra- and intracellularly located pathogens.
Microorganisms may be initially resistant to the action of an antibiotic or may acquire resistance to it.
Scale of sensitivity of microorganisms to azithromycin (Minimum inhibitory concentration, mg/l):
- Microorganism Staphylococcus - MIC Sensitive ≤ 1 mg/l; Stable > 2 mg/l;
- Microorganism Streptococcus A, B, C, G - MIC Sensitive ≤ 0.25; Stable > 0.5 mg/l;
- Microorganism Streptococcus pneumoniae - MIC Sensitive ≤ 0.25; Stable > 0.5 mg/l;
- Microorganism Haemophilus influenzae - MIC Sensitive ≤ 0.12; Stable > 4 mg/l;
- Microorganism Moraxella catarrhalis - MIC Sensitive ≤ 0.5; Stable > 0.5 mg/l;
- Microorganism Neisseria gonorrhoeae - MIC Sensitive ≤ 0.25; Persistent > 0.5 mg/l.
Sensitive
Aerobic gram-positive microorganisms: Staphylococcus aureus (methicillin-sensitive), Streptococcus pneumoniae (penicillin-sensitive), Streptococcus pyogenes.
Aerobic gram-negative microorganisms: Haemophilus influenzae, Haemophilus parainfluenzae, Legionella pneumophila, Moraxella catarrhalis, Pasteurella multocida, Neisseria gonorrhoeae.
Anaerobic microorganisms: Clostridium perfringens, Fusobacterium spp., Prevotella spp., Porphyromonas spp..
Other: Chlamydia trachomatis, Chlamydia pneumoniae, Chlamydia psittaci, Mycoplasma pneumoniae, Mycoplasma hominis, Borrelia burgdorferi.
Moderately sensitive or insensitive
Aerobic gram-positive microorganisms: Streptococcus pneumoniae (moderately sensitive or resistant to penicillin).
Stable
Aerobic gram-positive microorganisms: Enterococcus faecalis, Methicillin-resistant strains of Staphylococcus aureus.
Anaerobes: Bacteroides fragilis group; Streptococcus pneumoniae, beta-hemolytic Streptococcus spp. group A, Enterococcus faecalis and Staphylococcus aureus (including methicillin-sensitive strains), resistant to erythromycin and other macrolides, lincosamides, and resistant to azithromycin.
Pharmacokinetics
After oral administration, azithromycin is well absorbed and quickly distributed in the body. Bioavailability after a single dose of 0.5 g is 37% (the “first pass” effect through the liver), maximum concentration (Cmax) after oral administration of 0.5 g is 0.4 mg/l, time to reach maximum concentration (TCmax) is 2 -3 hours. Concentration in tissues and cells is 10-50 times higher than in serum. The volume of distribution is 31.1 l/kg, binding to plasma proteins is inversely proportional to the concentration in the blood and amounts to 7-50%. Azithromycin is acid-stable and lipophilic. Easily passes through histohematic barriers, penetrates well into the respiratory tract, internal organs and tissues, including the prostate gland, skin and soft tissues. It is also transported to the site of infection by phagocytes, polymorphonuclear leukocytes and macrophages, where it is released in the presence of bacteria. Penetrates through cell membranes and creates high concentrations in them, which is especially important for the eradication of intracellular pathogens.
In foci of infection, the concentration is 24-34% higher than in healthy tissues and correlates with the severity of the inflammatory process. Remains in effective concentrations for 5-7 days after taking the last dose.
It is demethylated in the liver, the resulting metabolites are not active. The metabolism of the drug involves isoenzymes CYP3A4, CYP3A5, CYP3A7, of which it is an inhibitor. Plasma clearance - 630 ml/min: half-life between 8 and 24 hours after administration - 14-20 hours, half-life in the range from 24 to 72 hours - 41 hours. More than 50% of the drug is excreted through the intestines unchanged, 6% - kidneys.
Food intake significantly changes pharmacokinetics: Cmax increases (by 31%), the area under the concentration-time curve (AUC) does not change.
In elderly men (65-85 years old), the pharmacokinetic parameters do not change; in women, Cmax increases (by 30-50%).
Indications for use Azithromycin ecomed 100 mg/5 ml 16.5 g powder for the preparation of suspension for oral administration
Infectious and inflammatory diseases caused by microorganisms sensitive to azithromycin:
- infections of the upper respiratory tract and ENT organs: pharyngitis, tonsillitis, sinusitis, otitis media;
- lower respiratory tract infections: acute bronchitis, exacerbation of chronic bronchitis, pneumonia, incl. caused by atypical pathogens;
- infections of the skin and soft tissues: erysipelas, impetigo, secondary infected dermatoses;
- initial stage of Lyme disease (borreliosis) – erythema migrans (erythema migrans)/
Contraindications
- Hypersensitivity to azithromycin (including other macrolides) or other components of the drug;
- severe renal failure (creatinine clearance (CC) less than 40 ml/min);
- severe liver failure (class C on the Child-Pugh scale);
- breast-feeding;
- simultaneous use with ergotamine and dihydroergotamine;
- children up to 6 months;
- sucrase/isomaltase deficiency, fructose intolerance, glucose-galactose malabsorption;
- hypersensitivity to erythromycin; ketolides.
With caution: pregnancy, myasthenia gravis, mild to moderate liver dysfunction, mild to moderate renal dysfunction (creatinine clearance more than 40 ml/min), diabetes mellitus, in patients with the presence of proarrhythmogenic factors (especially in elderly patients): with congenital or acquired prolongation of the QT interval, in patients receiving therapy with antiarrhythmic drugs of classes IA (quinidine, procainamide), III (dofetilide, amiodarone and sotalol), cisapride, terfenadine, antipsychotic drugs (pimozide), antidepressants (citalopram), fluoroquinolones (moxifloxacin and levofloxacin), with disturbances in water and electrolyte balance, especially in the case of hypokalemia or hypomagnesemia, with clinically significant bradycardia, cardiac arrhythmia or severe heart failure; simultaneous use of digoxin, warfarin, cyclosporine.
Application Azithromycin ecomed 100mg/5ml 16.5g powder for the preparation of suspension for oral administration during pregnancy and breastfeeding
Pregnancy
During pregnancy, azithromycin is used only if the expected benefit to the mother outweighs the potential risk to the fetus.
Breastfeeding period
During breastfeeding, it is used only if the expected benefit to the mother outweighs the potential risk to the child. If it is necessary to use azithromycin during breastfeeding, it is recommended to stop breastfeeding.
special instructions
If you miss one dose of azithromycin, the missed dose should be taken as soon as possible, and subsequent doses should be taken at intervals of 24 hours.
Azithromycin should be taken at least one hour before or two hours after taking antacids.
Azithromycin should be used with caution in patients with mild to moderate hepatic impairment due to the possibility of developing fulminant hepatitis and severe hepatic failure.
If there are symptoms of liver dysfunction, such as rapidly increasing asthenia, jaundice, dark urine, bleeding tendency, hepatic encephalopathy, azithromycin therapy should be discontinued and a study of the functional state of the liver should be performed.
In case of impaired renal function: in patients with GFR (glomerular filtration rate) 10-80 ml/min, no dose adjustment is required; azithromycin therapy should be carried out with caution under monitoring the state of renal function.
As with the use of other antibacterial drugs, during therapy with azithromycin, patients should be regularly examined for the presence of non-susceptible microorganisms and signs of the development of superinfections, including fungal ones.
Azithromycin should not be used in longer courses than indicated in the instructions, since the pharmacokinetic properties of azithromycin allow us to recommend a short and simple dosage regimen.
There is no data on a possible interaction between azithromycin and ergotamine and dihydroergotamine derivatives, but due to the development of ergotism with the simultaneous use of macrolides with ergotamine and dihydroergotamine derivatives, this combination is contraindicated.
With long-term use of azithromycin, the development of pseudomembranous colitis caused by Clostridium difficile, both in the form of mild diarrhea and severe colitis, is possible. If antibiotic-associated diarrhea develops while taking azithromycin, as well as 2 months after the end of therapy, clostridial pseudomembranous colitis should be excluded. Do not use drugs that inhibit intestinal motility.
When treated with macrolides, including azithromycin, prolongation of cardiac repolarization and QT interval was observed, increasing the risk of developing cardiac arrhythmias, including arrhythmias, which can lead to cardiac arrest.
Caution should be exercised when using azithromycin in patients with the presence of proarrhythmogenic factors (especially in elderly patients), including congenital or acquired prolongation of the QT interval, in patients taking antiarrhythmic drugs of classes IA (quinidine, procainamide), III (dofetilide, amiodarone and sotalol), cisapride, terfenadine, antipsychotics (pimozide), antidepressants (citalopram), fluoroquinolones (moxifloxacin and levofloxacin), with fluid and electrolyte imbalance, especially in the case of hypokalemia or hypomagnesemia, with clinically significant bradycardia, cardiac arrhythmia or severe heart failure .
The use of azithromycin may provoke the development of myasthenic syndrome or cause an exacerbation of myasthenia gravis.
Impact on the ability to drive vehicles and operate machinery
During the treatment period, care must be taken when driving vehicles and engaging in other potentially hazardous activities that require increased concentration and speed of psychomotor reactions.
Overdose
Symptoms: temporary hearing loss, nausea, vomiting, diarrhea.
Treatment is symptomatic.
Side effects Azithromycin ecomed 100mg/5ml 16.5g powder for suspension for oral administration
Infectious and parasitic diseases - uncommon: candidiasis, including oral mucosa, vaginal infection, pneumonia, fungal infection, bacterial infection, pharyngitis, gastroenteritis, respiratory diseases, rhinitis; unknown frequency: pseudomembranous colitis.
Disorders of the blood and lymphatic system - uncommon: leukopenia, neutropenia, eosinophilia; very rarely: thrombocytopenia, hemolytic anemia.
Metabolic and nutritional disorders - uncommon: anorexia.
Immune system disorders - uncommon: angioedema, hypersensitivity reaction; unknown frequency: anaphylactic reaction.
Nervous system disorders - often: headache; uncommon: dizziness, disturbance of taste, paresthesia, drowsiness, insomnia, nervousness; rarely: agitation; unknown frequency: hypoesthesia, anxiety, aggression, fainting, convulsions, psychomotor hyperactivity, loss of smell, perverted sense of smell, loss of taste, myasthenia gravis, delirium, hallucinations.
Visual disorders - often: visual impairment.
Hearing disorders and labyrinthine disorders - uncommon: hearing loss, vertigo; unknown frequency: hearing impairment, including deafness and/or tinnitus.
Cardiovascular system disorders - uncommon: palpitations; very rarely: arrhythmia; unknown frequency: increased QT interval on the electrocardiogram, ari, ventricular tachycardia.
Vascular disorders - uncommon: flushing of blood to the face; unknown frequency: decreased blood pressure.
Disorders of the respiratory system, chest and mediastinal organs - uncommon: shortness of breath, nosebleeds.
Gastrointestinal disorders - very common: diarrhea; often: nausea, vomiting, abdominal pain; uncommon: flatulence, dyspepsia, constipation, gastritis, dysphagia, bloating, dry oral mucosa, belching, ulcers of the oral mucosa, increased secretion of the salivary glands; very rarely: discoloration of the tongue, pancreatitis.
Disorders of the liver and biliary tract - uncommon: hepatitis; rarely: impaired liver function, cholestatic jaundice; unknown frequency: liver failure (in rare cases, fatal, mainly due to severe liver dysfunction); liver necrosis, fulminant hepatitis.
Disorders of the skin and subcutaneous tissues - uncommon: skin rash, itching, urticaria, dermatitis, dry skin, sweating; rarely: photosensitivity reaction; unknown frequency: Stevens-Johnson syndrome, toxic epidermal necrolysis, erythema multiforme, drug rash with eosinophilia and systemic manifestations (DRESS syndrome).
Musculoskeletal and connective tissue disorders - uncommon: osteoarthritis, myalgia, back pain, neck pain; unknown frequency: arthralgia.
Renal and urinary tract disorders - uncommon: dysuria, pain in the kidney area; unknown frequency: interstitial nephritis, acute renal failure.
Disorders of the genital organs and mammary gland - infrequently: metrorrhagia, impaired testicular function.
General disorders and administration site conditions - uncommon: swelling, asthenia, malaise, feeling tired, facial swelling, chest pain, fever, peripheral edema.
Impact on the results of laboratory and instrumental studies - often: decreased number of lymphocytes, increased number of eosinophils, increased number of basophils, increased number of monocytes, increased number of neutrophils, decreased concentration of bicarbonates in the blood plasma; uncommon: increased activity of aspartate aminotransferase, alanine aminotransferase, increased concentration of bilirubin in blood plasma, increased concentration of urea in blood plasma, increased concentration of creatinine in blood plasma, change in potassium content in blood plasma, increased activity of alkaline phosphatase in blood plasma, increased chloride content in blood plasma , increased blood glucose concentration, increased platelet count, decreased hematocrit, increased plasma bicarbonate concentration, change in plasma sodium content.
Drug interactions
Antacids (aluminum and magnesium containing) do not affect bioavailability, but reduce the concentration of azithromycin in the blood by 30%, so the interval between their administration should be 1 hour before or 2 hours after taking these drugs.
When used simultaneously with ergotamine and dihydroergotamine derivatives, the toxic effect of the latter may be enhanced (vasospasm, dysesthesia).
When used together with indirect coumarin anticoagulants (warfarin), patients need careful monitoring of prothrombin time.
Caution must be exercised when co-prescribing terfenadine and azithromycin, since it has been found that the simultaneous use of terfenadine and macrolides causes arrhythmia and prolongation of the QT interval. Based on this, the above complications cannot be excluded when taking terfenadine and azithromycin together.
When used simultaneously with cyclosporine, it is necessary to monitor the concentration of cyclosporine in the blood. When azithromycin and cyclosporine are used simultaneously, a dose adjustment of cyclosporine is necessary. When used simultaneously with digoxin, it is necessary to control the concentration of digoxin in the blood (it is possible to increase the absorption of digoxin in the intestine). The simultaneous use of azithromycin (1200 mg) and nelfinavir (750 mg 3 times a day) causes an increase in the equilibrium concentration of azithromycin in the blood plasma; no clinically significant side effects were observed and no dose adjustment of azithromycin is required when used simultaneously with nefinavir.
When used concomitantly with zidovudine, azithromycin has little effect on the pharmacokinetics, including renal excretion, of zidovudine or its glucuronide metabolite.
Azithromycin weakly interacts with cytochrome P450 isoenzymes; it has not been revealed that azithromycin is involved in pharmacokinetic interactions similar to erythromycin and other macrolides; azithromycin is not an inducer or inhibitor of the cytochrome P450 isoenzyme.
Neutropenia has occasionally been observed with concomitant use of azithromycin and rifabutin, although neutropenia has been associated with the use of rifabutin; a causal relationship between the use of the combination of azithromycin and rifabutin and neutropenia has not been established.
Azithromycin does not affect the blood concentrations of carbamazepine, cimetidine, didanosine, efavirenz, fluconazole, indinavir, midazolam, theophylline, triazolam, trimethoprim/sulfamethoxazole, cetirizine, sildenafil, atorvastatin, rifabutin and methylprednisolone when used simultaneously.
There have been isolated case reports of rhabdomyolysis in patients taking azithromycin and statins concomitantly.
Interaction with other drugs.
Antacids
Antacids do not affect the bioavailability of azithromycin, but reduce the maximum blood concentration by 30%, so the drug should be taken at least one hour before or two hours after taking these drugs and eating.
Cetirizine
Concomitant use of azithromycin with cetirizine (20 mg) for 5 days in healthy volunteers did not lead to pharmacokinetic interaction or a significant change in the QT interval.
Didanosine (dideoxyinosine)
The simultaneous use of azithromycin (1200 mg/day) and didanosine (400 mg/day) in 6 HIV-infected patients did not reveal any changes in the pharmacokinetic indications of didanosine compared to the placebo group.
Digoxin (P-glycoprotein substrates)
Simultaneous use of macrolide antibiotics, incl. azithromycin, with P-glycoprotein substrates such as digoxin, leads to increased concentrations of P-glycoprotein substrate in the blood serum. Thus, with the simultaneous use of azithromycin and digoxin, it is necessary to take into account the possibility of increasing the concentration of digoxin in the blood serum.
Zidovudine
The simultaneous use of azithromycin (single dose of 1000 mg and multiple doses of 1200 or 600 mg) has a minor effect on pharmacokinetics, incl. renal excretion of zidovudine or its glucuronide metabolite. However, the use of azithromycin caused an increase in the concentration of phosphorylated zidovudine, a clinically active metabolite in peripheral blood mononuclear cells. The clinical significance of this fact is unclear.
Azithromycin interacts weakly with isoenzymes of the cytochrome P450 system. Azithromycin has not been shown to participate in pharmacokinetic interactions similar to erythromycin and other macrolides. Azithromycin is not an inhibitor or inducer of cytochrome P450 isoenzymes.
Ergot alkaloids
Given the theoretical possibility of ergotism, the simultaneous use of azithromycin with ergot alkaloid derivatives is not recommended.
Pharmacokinetic studies were conducted on the simultaneous use of azithromycin and drugs whose metabolism occurs with the participation of isoenzymes of the cytochrome P450 system.
Atorvastatin
Concomitant use of atorvastatin (10 mg daily) and azithromycin (500 mg daily) did not cause changes in atorvastatin plasma concentrations (based on HMG-CoA reductase inhibition assay). However, in the post-marketing period, isolated case reports of rhabdomyolysis have been received in patients receiving concomitant azithromycin and statins.
Carbamazepine
Pharmacokinetic studies involving healthy volunteers did not reveal a significant effect on the plasma concentrations of carbamazepine and its active metabolite in patients receiving concomitant azithromycin.
Cimetidine
Pharmacokinetic studies of the effect of a single dose of cimetidine on the pharmacokinetics of azithromycin did not reveal changes in the pharmacokinetics of azithromycin, provided that cimetidine was used 2 hours before azithromycin.
Indirect anticoagulants (coumarin derivatives)
In pharmacokinetic studies, azithromycin did not affect the anticoagulant effect of a single 15 mg dose of warfarin administered to healthy volunteers. Potentiation of the anticoagulant effect has been reported after simultaneous use of azithromycin and indirect anticoagulants (coumarin derivatives). Although a causal relationship has not been established, the need for frequent monitoring of PT should be considered when using azithromycin in patients receiving indirect oral anticoagulants (coumarin derivatives).
Cyclosporine
In a pharmacokinetic study involving healthy volunteers who took azithromycin (500 mg/day once) orally for 3 days, followed by cyclosporine (10 mg/kg/day once), a significant increase in plasma Cmax and AUC0-5 of cyclosporine was detected. . Caution is advised when using these drugs together. If simultaneous use of these drugs is necessary, it is necessary to monitor the concentration of cyclosporine in the blood plasma and adjust the dose accordingly.
Efavirenz
Concomitant use of azithromycin (600 mg/day once) and efavirenz (400 mg/day) daily for 7 days did not cause any clinically significant pharmacokinetic interaction.
Fluconazole
Concomitant use of azithromycin (1200 mg once) did not change the pharmacokinetics of fluconazole (800 mg once). The total exposure and T1/2 of azithromycin did not change with simultaneous use of fluconazole, however, a decrease in Cmax of azithromycin was observed (by 18%), which was not clinically significant.
Indinavir
The simultaneous use of azithromycin (1200 mg once) did not have a statistically significant effect on the pharmacokinetics of indinavir (800 mg 3 times a day for 5 days).
Methylprednisolone
Azithromycin does not have a significant effect on the pharmacokinetics of methylprednisolone.
Nelfinavir
The simultaneous use of azithromycin (1200 mg) and nelfinavir (750 mg 3 times a day) causes an increase in the Css of azithromycin in the blood serum. No clinically significant side effects were observed, and no dose adjustment of azithromycin is required when used concomitantly with nelfinavir.
Rifabutin
The simultaneous use of azithromycin and rifabutin does not affect the concentration of each drug in the blood serum. Neutropenia has sometimes been observed with simultaneous use of azithromycin and rifabutin. Although neutropenia has been associated with the use of rifabutin, a causal relationship between the use of the combination of azithromycin and rifabutin and neutropenia has not been established.
Sildenafil
When used in healthy volunteers, there was no evidence of the effect of azithromycin (500 mg/day daily for 3 days) on the AUC and Cmax of sildenafil or its main circulating metabolite.
Terfenadine
Pharmacokinetic studies have not provided evidence of an interaction between azithromycin and terfenadine. There have been isolated cases reported where the possibility of such an interaction could not be completely excluded, but there was no concrete evidence that such an interaction occurred. It has been found that the simultaneous use of terfenadine and macrolides can cause arrhythmia and prolongation of the QT interval.
Theophylline
No interaction has been detected between azithromycin and theophylline.
Triazolam/midazolam
Significant changes in pharmacokinetic parameters with simultaneous use of azithromycin with triazolam or midazolam in therapeutic doses were not detected.
Trimethoprim/sulfamethoxazole
Concomitant use of trimethoprim/sulfamethoxazole with azithromycin did not show a significant effect on Cmax, total exposure or renal excretion of trimethoprim or sulfamethoxazole. Azithromycin serum concentrations were consistent with those found in other studies.
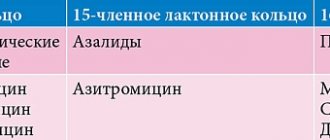
New directions for the clinical use of azithromycin in pediatric practice
Azithromycin (Sumamed®), the first representative of the group of semi-synthetic 15-membered macrolide antibiotics (azalides), has been used in clinical practice since 1991 and is one of the most frequently prescribed drugs in many countries around the world. Thus, according to the information and analytical company IMS Health (2009), 53.8 million prescriptions for azithromycin were written in the USA (5th place among all drugs) [1]. Azithromycin is currently approved by the US Food and Drug Administration (FDA) for use in adults and children over 6 months of age for the treatment of infections caused by susceptible pathogens, including respiratory tract infections ( IDP) [2]. Azithromycin has high activity against both typical and atypical bacterial pathogens of IDP, and its pharmacokinetic properties allow it to create maximum concentrations in infected tissues. The main indications for use of the drug are acute otitis media, acute bacterial rhinosinusitis, community-acquired pneumonia and acute streptococcal tonsillitis/pharyngitis, scarlet fever, skin and soft tissue infections (erysipelas, impetigo, secondary infected dermatoses). To date, a number of clinical studies have been conducted confirming the effectiveness of azithromycin in other nosological forms, which will be discussed in this review.
Recurrent respiratory tract infections
Traditionally, it was believed that most cases of so-called acute respiratory infections (ARI), acute bronchitis and laryngotracheitis are caused by viruses and do not require antibiotics. However, recently more and more information has appeared about the role of bacterial pathogens (such as Mycoplasma pneumoniae, Chlamydia pneumoniae) in the etiology of such infections, especially in young people without concomitant pathology [3, 4] and in children [5]. Thus, the frequency of infection caused by C. pneumoniae and M. pneumoniae in acute respiratory infections is, on average, up to 10% during non-epidemic periods and can reach 25–50% during epidemic outbreaks [3]. Undoubtedly, macrolides are the drugs of choice for the treatment of infections allegedly caused by “atypical” pathogens (chlamydia and mycoplasmas).
In a study performed by S. Esposito et al. [6], the role of M. pneumoniae and C. pneumoniae in the development of acute respiratory infections in children with recurrent UTIs, as well as the ability of specific antibacterial therapy to reduce the incidence of relapses, was studied. The study involved 353 frequently ill children (FCI) aged 1 to 14 years; The control group consisted of 208 healthy children. NPCs were randomized to treatment with symptomatic therapy alone or symptomatic therapy with azithromycin (10 mg/kg/day 3 days a week for 3 weeks). Infections caused by “atypical” pathogens were diagnosed in 54% of children and only in 3.8% of children in the control group (p < 0.0001). Short-term (within 1 month) clinical effect was more often observed in patients receiving azithromycin, but the differences were statistically significant only in the group of patients with infection caused by “atypical” pathogens. A long-term clinical effect (over 6 months) was observed significantly more often in patients with PBD during treatment with azithromycin, regardless of the etiology of recurrent IDPs. The authors believe that “atypical” bacteria may play a role in the occurrence of recurrent respiratory tract infections in children and long-term therapy with azithromycin can significantly improve the course of an acute episode and reduce the risk of relapses [6].
In another study of 1,706 children aged 6 months to 14 years with recurrent respiratory tract infections (≥ 8 episodes of acute respiratory infections per year if the child was < 3 years of age and ≥ 6 episodes per year if the child was ≥ 3 years of age) , it was shown that, regardless of age and clinical diagnosis, the administration of macrolides to patients with recurrent respiratory tract infections led to statistically greater both short- and long-term clinical effectiveness of therapy compared with beta-lactams (p < 0.0001) or the administration of only symptomatic therapy (p < 0.0001) [5].
Prolonged cough and whooping cough
Prolonged cough is one of the common reasons for visits to pediatricians, the most likely cause of which may be whooping cough. The incidence of whooping cough remains high despite the availability of an effective and safe vaccine. Serologically confirmed Bordetella pertussis infection is detected in 37% of cases of cough lasting more than 2 weeks after an acute respiratory infection [12]. Another 12.9% of children with prolonged cough were diagnosed with M. pneumoniae infection [12]. Thus, in approximately half of cases of prolonged cough due to infectious causes, there are indications for the prescription of antibacterial drugs (ABPs) from the macrolide group.
The drug of choice for the treatment and post-exposure prophylaxis of whooping cough is erythromycin, which is prescribed for 14 days [13]. However, despite the effectiveness of erythromycin therapy, the need for use 4 times a day and a fairly high incidence of adverse drug reactions from the gastrointestinal tract were the reason for the low compliance with the recommended 14-day course [14]. In recent decades, in vitro studies have demonstrated the activity of azithromycin against B. pertussis, and clinical studies have confirmed the effectiveness of this drug (table).
According to the results of a Cochrane systematic review of the use of antibiotics for the treatment and prevention of pertussis, which included 12 randomized controlled trials (total number of participants 1720), a 3-day course of azithromycin therapy was not inferior in effectiveness to a 14-day course of erythromycin treatment in terms of clinical and microbiological effectiveness, as well as the frequency of microbiological relapses of infection [13]. Currently, azithromycin is included in the recommendations of the US Centers for Disease Control and Prevention (CDC) for the treatment of whooping cough. It must be prescribed to children under 6 months at a dose of 10 mg/kg once a day for 5 days; for children over 6 months - 10 mg/kg on the first day (but not more than 500 mg), then 5 mg/kg (days 2–5 of therapy) [14].
Cat scratch disease
Cat scratch disease was first described in 1931, but its causative agent, Bartonella henselae, was identified only in 1983, which is associated with significant difficulties in cultivating this pathogen [15]. The disease is widespread and most often affects children and young people, but can also occur in adult patients. Typical manifestations in individuals without immunodeficiency include the appearance after 3–10 days of a red-brown, painless papule at the site of injury caused by the animal. After 1–3 weeks, unilateral regional lymphadenopathy develops. The disease progresses slowly. The condition of patients is usually satisfactory, with mild nonspecific symptoms such as general malaise, loss of appetite, abdominal pain, and muscle or joint pain. In 25% of cases the disease is asymptomatic. The diagnosis is established based on medical history (contact with cats and the presence of scratches) and serological testing - determination of IgG class antibodies to B. henselae in a titer of more than 1:256. The duration of the infectious process usually does not exceed 6 months [15].
Although cat scratch disease tends to be self-limiting in immunocompetent individuals and recovery occurs within 2–3 months without treatment, accelerated resolution of lymphadenopathy (within 1 month) has been shown when treated with a short course of azithromycin [16–18]. In children, azithromycin is prescribed for 5 days at a dose of 10 mg/kg on the first day, and in the next 4 days at a dose of 5 mg/kg [18, 19].
It should be noted that other antibacterial drugs potentially active against B. henselae include rifampicin, doxycycline, gentamicin, co-trimoxazole and ciprofloxacin (monotherapy or combination of two drugs) [15, 20]. Some of them are not approved for use in pediatrics, others are characterized by an unfavorable safety profile, therefore, when treating children, it is advisable to give preference to azithromycin [21].
Intestinal infections
The limited possibilities of antibacterial therapy for intestinal infections in children and the increasing resistance of pathogens to ALD dictate the need to search for new approaches to the treatment of shigellosis in children [22]. One of the new directions is to study the effectiveness of azithromycin in this nosological form, which is based on pharmacokinetic and pharmacodynamic data and clinical experience with the use of azithromycin in adults [23, 24]. The first successful clinical studies of its effectiveness against shigellosis in children were also conducted.
During an outbreak of shigellosis in Israel in 2003, 73 people were infected, of whom 83% were children aged 6 months to 18 years. All children with shigellosis confirmed by a positive fecal culture were prescribed nalidixic acid at a dose of 55 mg/kg/day in 4 doses orally for 5 days. Since diarrhea persisted in 25 children by the time the course of its use was completed, it was decided to replace nalidixic acid with azithromycin, which was administered orally at a dose of 10 mg/kg/day for 3 days. In all (100%) children taking azithromycin, diarrhea was relieved 48 hours after the start of therapy, while in the group receiving only nalidixic acid, diarrhea was relieved in only 65% of children [25].
Another study, conducted between 1998 and 2000, included 75 children aged 6 months to 5 years diagnosed with shigellosis. Patients were randomized into two groups: the first received cefixime at a dose of 8 mg/kg/day (maximum dose 400 mg/day) for 5 days, the second received azithromycin at a dose of 12 mg/kg on the first day (maximum dose 500 mg). ), then 6 mg/kg (maximum 250 mg/day) over the next 4 days. The therapy was clinically effective in 93% of patients in the first group and in 78% in the second (p = 0.1, that is, the differences are not significant). The average duration of diarrhea from the start of treatment averaged 2.5 days in the first group and about 4 days in the second. Eradication of the pathogen on the 3rd day of therapy was achieved in 59% of patients taking cefixime and in 93% of patients taking azithromycin; these differences were statistically significant. On the 7th day, a positive bacteriological result was obtained in one child from the azithromycin group and in two children from the cefixime group [26].
Thus, the results of the described studies demonstrate the clinical and microbiological effectiveness of azithromycin for shigellosis in children. The simple dosing regimen, rapid rate of clinical improvement, and sufficient eradication of Shigella, most likely due to high intracellular concentrations of azithromycin, warrant further studies aimed at confirming the validity of this therapeutic strategy.
Chlamydial infection in newborns
Chlamydia trachomatis is the most common pathogen of sexually transmitted infections in the United States. Perinatal transmission of C. trachomatis usually occurs during natural childbirth, but the infection can also be secondary, resulting from damage to the membranes of the fetus, direct contamination of the nasopharynx and lungs of the newborn. Cases of chlamydial infection in newborns after cesarean section have been described. 35–50% of newborns whose mothers are infected with chlamydia develop conjunctivitis and 11–20% develop pneumonia. Chlamydial infection is the most common cause of neonatal conjunctivitis, occurring between the 5th and 12th day of life.
Because chlamydia spreads through the tear duct and into the nasopharynx, at least 33% of newborns develop chlamydial pneumonia. In cases where there are no signs of conjunctivitis, pneumonia develops in 11–20% of newborns from infected and untreated mothers [27]. C. trachomatis can also cause subacute afebrile pneumonia in children 1–3 months of age.
The US Centers for Disease Control and Prevention (CDC) recommends the use of erythromycin base or ethyl succinate at a dose of 50 mg/kg/day orally in 4 divided doses for 14 days for the treatment of chlamydial conjunctivitis and pneumonia in newborns. However, attention is drawn to the possibility of a serious undesirable effect of erythromycin in children under 6 weeks of age - hypertrophic pyloric stenosis, which occurs 8 times more often in children receiving erythromycin orally (but not topically) between the 3rd and 13th days of life [ 28–30]. This phenomenon is presumably based on the well-known prokinetic properties of erythromycin. The risk of developing pyloric stenosis when using other macrolides (azithromycin, clarithromycin) has not been established. Although data regarding the use of azithromycin in the treatment of chlamydial infection in newborns are limited, there is evidence of the effectiveness of a short course of azithromycin at a dose of 20 mg/kg/day once daily orally for 3 days for the treatment of chlamydial infection in newborns, i.e. it may be a safer alternative to erythromycin [31, 32]. It should be noted that no other macrolide antibiotic (except for the above-mentioned erythromycin, which has a questionable safety profile in this category of patients) has official approval for use in newborns and children in the first months of life for the treatment of chlamydial infection.
Acne
Acne is the most common dermatological problem in teenagers and young adults. Over the past decades, it has been proven that the systemic use of ABP plays a major role in the treatment of acne patients who have inflammatory elements. In some cases, systemic antibiotic therapy leads to side effects, which contributes to a decrease in patient compliance. Considering the fact that the commonly prescribed systemic antibiotics for acne are tetracyclines, and this group of antibacterial drugs is characterized by a not entirely favorable safety profile, it is advisable, especially in adolescents, to search for safer alternative antibiotics for use. Azithromycin has anti-inflammatory properties and prevents the growth of Propionibacterium acnes, a major pathogen involved in the pathogenesis of the inflammatory process in acne [33].
According to an open multicenter non-comparative study performed in patients with stage II inflammatory forms of acne vulgaris, the use of azithromycin at a dose of 500 mg per day for 3 consecutive days per month for 3 months led to a statistically significant decrease in the number of inflammatory elements in various areas of the face [ 33].
In another study in 57 patients aged 13 to 41 years with moderate acne, long-term (12 weeks) use of azithromycin at a dose of 500 mg 3 times a week demonstrated high (80.7%) clinical efficacy and good tolerability (undesirable drug reactions were recorded in 11.3% of patients), on the basis of which the authors conclude that the use of azithromycin is effective, safe and highly compliant for moderate forms of acne vulgaris in both adolescents and adult patients [34].
A separate open-label, non-comparative study of the effectiveness of azithromycin was conducted in 52 Italian adolescents with moderate to severe papulopustular forms of acne. Azithromycin was prescribed at a dose of 500 mg 3 times a week for 8 weeks without concomitant local treatment. 90.4% of patients showed significant improvement (a decrease of more than 20% in the number of inflammatory elements) within the first 4 weeks of treatment. All patients completed the 8-week course of treatment. The most pronounced skin cleansing was observed by the 8th week of treatment in 61.5% of patients. The effect persisted for 4 months after completion of azithromycin. The drug was well tolerated—adverse events were noted in only 3 patients (5.6%) [35].
Another randomized, double-blind, controlled clinical trial conducted in Iran compared the efficacy and safety of azithromycin and doxycycline in the treatment of moderate acne and examined the effect of patient age on treatment outcomes [36]. The study involved 100 patients with moderate forms of acne vulgaris who sought outpatient care at a dermatology clinic. Patients were randomized into 2 groups A and D: group A received azithromycin at a dose of 500 mg per day for 4 consecutive days per month for 3 consecutive months; patients in group D took doxycycline at a dose of 100 mg per day for 3 consecutive months. As it turned out, both ABPs were comparable in clinical efficacy and safety in moderate forms of acne, but doxycycline was statistically significantly more effective in patients over the age of 18 years [36].
Thus, azithromycin, according to a number of clinical studies, has demonstrated high efficacy and a favorable safety profile in the treatment of acne in adolescents and young adults.
Conclusion: Thus, Sumamed® (azithromycin) has high activity against both typical and atypical bacterial pathogens of the respiratory tract, and its pharmacokinetic properties allow it to create maximum concentrations in infected tissues. This is one of the effective and most convenient ABPs used in outpatient practice. Based on the presented data, we can conclude that, along with the well-known traditional indications for the use of azithromycin, there are a number of promising areas for its clinical use in pediatrics, including a fairly wide range of additional clinical conditions for which reliable data on effectiveness have already been obtained and the safety of azithromycin. All this opens up new possibilities for its use in respiratory medicine for recurrent URIs, prolonged cough, chlamydial infection in newborns, as well as acne, cat scratch disease, and intestinal infections.
Literature
- Bartholow M. Top 200 Prescription Drugs of 2009 // Pharmacy Times. May 11, 2010.
- Langtry HD, Balfour JA Azithromycin: a review of its use in pediatric infectious diseases // Drugs 1998; 56:273–297.
- Blasi F. Atypical pathogens and respiratory tract infections // Eur Respir J 2004; 24: 171–181.
- Gonzales R., Sande MA Uncomplicated acute bronchitis // Ann. Intern. Med. 2001; 135(9):839–840.
- Principi N., Esposito S., Cavagna R. et al. Recurrent respiratory tract infections in pediatric age: a population-based survey of the therapeutic role of macrolides // J Chemother 2003; 15(1):53–9.
- Esposito S., Bosis S., Faelli N. et al. Role of atypical bacteria and azithromycin therapy for children with recurrent respiratory tract infections // Pediatr Infect Dis J 2005; 24 (5): 438–444.
- Aoyama T., Sunakawa K., Iwata S. et al. Efficacy of short-term treatment of pertussis with clarithromycin and azithromycin // J Pediatr 1996; 129:761–764.
- Bace A., Zrnic T., Begovac J. et al. Short-term treatment of pertussis with azithromycin in infants and young children // Eur J Clin Microbiol Infect Dis 1999; 18(4):296–298.
- Bace A., Kuzmanovic N., Novac D. Clinical comparative study of azithromycin and erythromycin in the treatment of pertussis - preliminary results // ICMAS-5, Jan 26–28, Seville, 2000: abstract # 36.
- Pichichero ME, Hoeger WJ, Casey JR Azithromycin for the treatment of pertussis // Pediatr Infect Dis J 2003; 22 (9): 847–9.
- Langley JM, Halperin SA, Boucher FD et al. Azithromycin is as effective as and better tolerated than erythromycin estolate for the treatment of pertussis // Pediatrics 2004; 114:96–101.
- Wang K., Chalker V., Bermingham A. et al. Mycoplasma pneumoniae and respiratory virus infections in children with persistent cough in England: a retrospective analysis // Pediatr Infect Dis J. 2011; 30 (12): 1047–1051.
- Altunaiji S., Kukuruzovic R., Curtis N., Massie J. Antibiotics for whooping cough (pertussis) // Cochrane Database Syst Rev. 2005; (1): CD004404.
- Tiwari T., Murphy TV, Moran J. National Immunization Program, CDC. Recommended antimicrobial agents for the treatment and postexposure prophylaxis of pertussis: 2005 CDC Guidelines // MMWR Recomm Rep 2005; 54 (RR-14): 1–16.
- Windsor JJ Cat-scratch disease: epidemiology, aetiology and treatment // Br J Biomed Sci 2001; 58 (2): 101–110.
- Batts S., Demers DM Spectrum and treatment of cat-scratch disease // Pediatr Infect Dis J 2004; 23 (12): 1161–1162.17.
- Vincent JM, Demers DM, Bass JW Infectious exanthems and unusual infections // Adolesc Med 2000; 11 (2): 327–58.
- Bass JW, Freitas BC, Freitas AD et al. Prospective randomized double blind placebo-controlled evaluation of azithromycin for the treatment of cat-scratch disease // Pediatr Infect Dis J 1998; 17(6):447–452.
- Estrada D. Azithromycin and cat-scratch disease // Infect Med 1998; 15 (8): 517.
- Conrad DA Treatment of cat-scratch disease // Curr Opin Pediatr 2001; 13(1):56–9.
- Klotz SA, Ianas V., Elliott SP Cat-scratch Disease // Am Fam Physician. 2011; 83 (2): 152–5.
- Jain SK, Gupta A, Glanz B et al. Antimicrobial-resistant Shigella sonnei: limited antimicrobial treatment options for children and challenges of interpreting in vitro azithromycin susceptibility // Pediatr Infect Dis J 2005; 24(6):494–497.
- Windsor JJ Cat-scratch disease: epidemiology, aetiology and treatment // Br J Biomed Sci 2001; 58 (2): 101–110.W.
- Bhattacharya SK, Sur D. An evaluation of current shigellosis treatment // Expert Opin Pharmacother 2003; 4(8):1315–1320
- Vincent JM, Demers DM, Bass JW Infectious exanthems and unusual infections // Adolesc Med 2000; 11 (2): 327–58.
- Basualdo W., Arbo A. Randomized comparison of azithromycin versus cefixime for the treatment of shigellosis in children // Ped Infect Dis J 2003; 22: 374–377.
- Popovich DM, McAlhany A. Practitioner care and screening guidelines for infants born to Chlamydia-positive mothers // NBIN 2004; 4 (1): 51–55.
- Hauben M., Amsden GW The association of erythromycin and infantile hypertrophic pyloric stenosis: causal or coincidental? // Drug Saf 2002; 25 (13): 929–942.
- Cooper WO, Griffin MR, Arbogast P. et al. Very early exposure to erythromycin and infantile hypertrophic pyloric stenosis // Arch Pediatr Adolesc Med 2002; 156(7):647–650.
- Mahon BE, Rosenman MB, Kleiman MB Maternal and infant use of erythromycin and other macrolide antibiotics as risk factors for infantile hypertrophic pyloric stenosis // J Pediatr 2001; 139(3):380–384.
- Workowski KA, Berman SM Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2006 // MMWR Recomm Rep. 2006; 55(RR-11):1–94.
- Zar HJ Neonatal chlamydial infections: prevention and treatment // Paediatr Drugs 2005; 7 (2): 103–110.
- Antonio JR, Pegas JR, Cestari TF, Do Nascimento LV Azithromycin pulses in the treatment of inflammatory and pustular acne: efficacy, tolerability and safety // J Dermatolog Treat. 2008;19(4):210–5.
- Innocenzi D., Skroza N., Ruggiero A. et al. Moderate acne vulgaris: efficacy, tolerance and compliance of oral azithromycin thrice weekly for // Acta Dermatovenerol Croat. 2008;16(1):13–8.
- Bardazzi F., Savoia F., Parente G. et al. Azithromycin: a new therapeutical strategy for acne in adolescents // Dermatol Online J. 2007; 13(4): 4.36.
- Babaeinejad S., Khodaeiani E., Fouladi RF Comparison of therapeutic effects of oral doxycycline and azithromycin in patients with moderate acne vulgaris: What is the role of age? // J Dermatolog Treat. 2011; 22 (4): 206–10.
I. V. Andreeva, Candidate of Medical Sciences O. U. Stetsyuk, Candidate of Medical Sciences
Research Institute of Antimicrobial Chemotherapy of the State Budgetary Educational Institution of Higher Professional Education of the State Medical Academy of the Ministry of Health and Social Development of Russia, Smolensk
Contact information for authors for correspondence
special instructions
If you miss one dose, the missed dose should be taken as soon as possible, and subsequent doses should be taken at intervals of 24 hours.
The drug should be taken at least one hour before or two hours after taking anatacid medications.
The drug should be used with caution in patients with mild to moderate liver dysfunction due to the possibility of developing fulminant hepatitis and severe liver failure.
If there are symptoms of liver dysfunction, such as rapidly increasing asthenia, jaundice, darkening of urine, tendency to bleeding, hepatic encephalopathy, drug therapy should be stopped and a study of the functional state of the liver should be performed.
In case of mild to moderate renal dysfunction (creatinine clearance more than 40 ml/min), azithromycin therapy should be carried out with caution under monitoring the state of renal function.
As with the use of other antibacterial drugs, during therapy with azithromycin, patients should be regularly examined for the presence of non-susceptible microorganisms and signs of the development of superinfections, including fungal ones.
The drug should not be used for longer courses than indicated in the instructions, because The pharmacokinetic properties of azithromycin allow us to recommend a short and simple dosage regimen.
There is no data on a possible interaction between azithromycin and ergotamine and dihydroergotamine derivatives, but due to the development of ergotism with the simultaneous use of macrolides with ergotamine and dihydroergotamine derivatives, this combination is not recommended.
With long-term use of azithromycin, the development of pseudomembranous colitis caused by Clostridium difficile, both in the form of mild diarrhea and severe colitis, is possible. If antibiotic-associated diarrhea develops while taking the drug, as well as 2 months after the end of therapy, clostridial pseudomembranous colitis should be excluded.
When treated with macrolides, incl. azithromycin, prolongation of cardiac repolarization and QT interval was observed, increasing the risk of developing cardiac arrhythmias, incl. ari.
Caution should be exercised when using the drug in patients with the presence of proarrhythmogenic factors (especially in elderly patients): with congenital or acquired prolongation of the QT interval, in patients taking antiarrhythmic drugs of classes IA (quinidine, procainamide), III (dofetilide, amiodarone and sotalol), cisapride, terfenadine, antipsychotics (pimozide), antidepressants (citalopram), fluoroquinolones (moxifloxacin and levofloxacin), with fluid and electrolyte imbalance, especially in the case of hypokalemia or hypomagnesemia, with clinically significant bradycardia, cardiac arrhythmia or severe heart failure.
The use of azithromycin may provoke the development of myasthenic syndrome or cause an exacerbation of myasthenia gravis.