Pharmacological properties of the drug Zofran™
Ondansetron is a potent, highly selective 5HT3 (serotonin) receptor antagonist. The drug prevents and eliminates nausea and vomiting caused by cytotoxic chemotherapy and/or radiation therapy, as well as postoperative nausea and vomiting. The mechanism of action of ondansetron is not fully understood. Perhaps the drug blocks the occurrence of the gag reflex, exerting an antagonistic effect on 5HT3 receptors localized in neurons of both the peripheral and central nervous system. The drug does not reduce the patient's psychomotor activity and does not have a sedative effect. Pharmacokinetics. After oral administration, bioavailability is 60%, and the time to reach maximum concentration in blood plasma is 1.5 hours (after taking 8 g). With intravenous administration, the maximum concentration in the blood plasma is achieved within 10 minutes. The main part of the dose taken is metabolized in the liver. Less than 5% of the drug is excreted unchanged in the urine. The half-life is approximately 3 hours (in elderly patients - 5 hours). Binding to blood plasma proteins is 70–76%. According to clinical studies involving children aged 1–24 months, it was shown that clearance in accordance with body weight in this group of patients was 30% less than in children aged 5–24 months, but comparable to that in children in aged 3–12 years. The half-life in children 1–4 months of age was found to average 6.7 hours, compared with 2.9 hours in children 5–24 months and 3–12 years. There is no need to adjust the dose in children aged 1–4 months, since only a single dose for intravenous administration of the drug is recommended for the treatment of postoperative nausea and vomiting. Differences in pharmacokinetic parameters may be explained in part by the larger volume of distribution of the drug in children aged 1–4 months. In clinical studies in children aged 3–12 years, the absolute values of clearance and volume of distribution of ondansetron after a single IV dose of 2 mg (for children aged 3–7 years) and 4 mg (for children aged 8–12 years) were reduced compared with those doses in adults. Both of these parameters increased linearly depending on body weight, by 12 years they reached the corresponding level of adults and were subsequently the same for different age groups. According to the population analysis, pharmacokinetic parameters in patients aged 1–48 months when administered at an intravenous dose of 0.15 mg/kg body weight every 4 hours 3 times a day will be comparable to those in patients aged 5–24 months and previous studies involving children aged 4–18 and 3–12 years.
Zofran, 2 mg/ml, solution for intravenous and intramuscular administration, 2 ml, 5 pcs.
Zofran is an antiemetic.
Pharmacodynamics
Ondansetron is a selective 5-HT 3 receptor antagonist. Drugs for cytostatic chemotherapy and radiotherapy can cause an increase in the level of serotonin, which, by activating vagal afferent fibers containing 5-HT 3 receptors, causes the gag reflex. Ondansetron inhibits the appearance of the gag reflex by blocking 5-HT 3 receptors at the level of neurons in both the central nervous system and the peripheral nervous system.
Pharmacokinetics
Ondansetron is completely absorbed from the gastrointestinal tract after oral administration and undergoes first-pass metabolism through the liver. Cmax in plasma is reached approximately 1.5 hours after administration. Bioavailability increases slightly with simultaneous food intake, but does not change when taking antacids.
The distribution of ondansetron is the same when administered orally, intramuscularly, and intravenously; T1/2 is approximately 3 hours, in elderly patients it can reach 5 hours, and in case of severe renal failure - 15-20 hours. The volume of distribution when equilibrium concentration is reached is about 140 liters. Plasma protein binding is 70–76%. After rectal administration, ondansetron is detected in plasma within 15–60 minutes. The concentration of the active substance increases linearly, Cmax is reached after approximately 6 hours and is 20–30 ng/ml. The decrease in plasma concentration occurs at a lower rate than after oral administration (due to ongoing absorption). T 1/2 - 6 hours. Absolute bioavailability after rectal administration - 60%.
It is eliminated from the systemic circulation mainly as a result of metabolism in the liver, which occurs with the participation of several enzyme systems. The absence of the CYP2D6 enzyme (sparteine-debrisoquine type polymorphism) does not affect the pharmacokinetics of ondansetron. Less than 5% of the administered dose is excreted unchanged in the urine.
In doses above 8 mg, the blood content increases disproportionately, because when high doses are administered orally, first-pass metabolism through the liver may decrease.
The pharmacokinetic parameters of ondansetron do not change with repeated administration.
In patients with moderate renal failure (creatinine clearance - 15-60 ml/min), both systemic clearance and volume of distribution of ondansetron are reduced, resulting in a small and clinically insignificant increase in its T1/2 (up to 5.4 hours). The pharmacokinetics of ondansetron remains virtually unchanged in patients with severe renal impairment undergoing chronic hemodialysis. In patients with severe liver dysfunction, the systemic clearance of ondansetron is sharply reduced, resulting in an increase in half-life (up to 15–32 hours), and oral bioavailability reaches 100% due to a decrease in first-pass metabolism.
Special patient groups
Floor
The pharmacokinetics of ondansetron depends on the gender of the patients. Women have lower systemic clearance and volume of distribution (indicators adjusted for body weight) than men.
Children and adolescents (ages 1 month to 17 years)
In a clinical study, children aged 1 to 24 months (51 patients) received ondansetron at a dose of 0.1 mg/kg or 0.2 mg/kg before surgery. In patients aged 1 to 4 months, Cl was approximately 30% less than in patients aged 5 to 24 months, but comparable to that in patients aged 3 to 12 years (adjusted for weight). body). T1/2 in the group of patients aged 1–4 months averaged 6.7 hours; in the age groups 5-24 months and 3-12 years - 2.9 hours. In patients aged 1 to 4 months, no dose adjustment is required, since a single intravenous injection of ondansetron is used to treat postoperative nausea and vomiting in this category of patients . Differences in pharmacokinetic parameters are partly explained by the higher volume of distribution in patients aged 1 to 4 months.
In a study of children aged 3–12 years (21 patients) undergoing elective surgery under general anesthesia, the absolute values of Cl and volume of distribution of ondansetron after a single IV dose of 2 mg (3 to 7 years) or 4 mg (from 8 to 12 years) were reduced in comparison with values in adults. Both parameters increased linearly with body weight, with values approaching those in adults at 12 years of age. When correcting clearance and volume of distribution values depending on body weight, these parameters were close in different age groups. A dose based on body weight (0.1 mg/kg, up to a maximum of 4 mg) compensates for these changes and the systemic exposure of ondansetron in children.
A population pharmacokinetic analysis was conducted in 74 patients aged 6 to 48 months who received intravenous ondansetron at a dose of 0.15 mg/kg every 4 hours in 3 doses to relieve nausea and vomiting caused by chemotherapy, and in 41 patients at the age of 1 to 24 months after surgery, who were administered ondansetron in a single dose of 0.1 or 0.2 mg/kg. Based on pharmacokinetic parameters in this population, for patients 1 to 48 months of age, administration of ondansetron IV at a dose of 0.15 mg/kg every 4 hours for 3 doses should result in systemic exposure comparable to that observed with use of the drug in the same doses in children aged 5 to 24 months during surgical interventions, as well as in previous studies in children with cancer (aged 4 to 18 years) and during surgery (aged 3 to 12 years ).
Elderly patients
Studies have shown a weak, clinically insignificant, age-dependent increase in T1/2 of ondansetron.
Patients with impaired renal function
In patients with moderate renal impairment (Cl creatinine 15–60 ml/min) with intravenous ondansetron, both systemic clearance and volume of distribution of ondansetron are reduced, resulting in a small and clinically insignificant increase in T1/2 (up to 5.4 h). The pharmacokinetics of ondansetron when administered intravenously remained virtually unchanged in patients with severely impaired renal function on chronic hemodialysis (studies were conducted between hemodialysis sessions).
Patients with liver dysfunction
In patients with severely impaired liver function, the systemic clearance of ondansetron is sharply reduced with an increase in T1/2 to 15–32 hours.
Use of Zofran™
Zofran tablets Nausea and vomiting caused by chemotherapy or radiation therapy Adults The emetogenic potential of cancer therapy varies depending on the dose and combination of chemotherapy and radiation therapy regimens used. Emetogenic chemotherapy and radiation therapy The recommended oral dose of Zofran is 8 mg 1–2 hours before the start of treatment, then 8 mg after 12 hours. To prevent late or delayed vomiting after the first 24 hours, it is necessary to continue further oral administration of the drug at a dose of 8 mg 2 times a day for up to 5 days from the end of chemotherapy. The recommended oral dose is 8 mg 2 times a day. The highly emetogenic therapy Zofran is available in oral and parenteral forms. The recommended oral dose is 24 mg with concomitant oral dexamethasone 12 mg 1 to 2 hours before starting Zofran therapy. To prevent attacks of late or delayed vomiting after the first 24 hours, it is recommended to use Zofran orally at a dose of 8 mg 2 times a day for up to 5 days after the end of chemotherapy. Children Children over the age of 4 years can be prescribed Zofran as a single intravenous injection at a dose of 5 mg/m2 immediately before chemotherapy, followed by oral Zofran at a dose of 4 mg 12 hours after the injection. To prevent vomiting over the next 5 days, Zofran is prescribed orally at a dose of 4 mg 2 times a day. Experience with Zofran in children under 4 years of age is limited. Elderly patients Zofran is well tolerated by patients over 65 years of age. No change in dose, frequency or route of administration is required. Postoperative Nausea and Vomiting Adults To prevent postoperative nausea and vomiting, an oral dose of 16 mg 1 hour before the start of anesthesia is recommended. For the treatment of postoperative nausea and vomiting, Zofran injection is recommended. Children For the prevention and treatment of postoperative nausea and vomiting in children over 4 years of age, Zofran can be prescribed as a slow intravenous injection. Elderly Patients Experience with the use of Zofran for the prevention and treatment of postoperative nausea and vomiting in the elderly is limited, but Zofran is well tolerated in patients over 65 years of age receiving chemotherapy. Patients with Renal Impairment There is no need to change the dosage regimen or route of administration of the drug in patients with impaired renal function. Patients with hepatic impairment In patients with moderate to severe hepatic impairment, the clearance of Zofran is significantly reduced and the serum half-life is increased. For such patients, the maximum daily dose of the drug should not exceed 8 mg. Subjects with impaired sparteine/debrisoquin metabolism The half-life of ondansetron is unchanged in subjects with impaired sparteine/debrisoquin metabolism. In such patients, repeated administration leads to the same drug concentration as in unimpaired metabolism. Therefore, no change in dosage or frequency of drug administration is required. Zofran injection Nausea and vomiting caused by chemotherapy or radiation therapy Adults Zofran injection is used in doses of 8–32 mg/day, recommendations for dose selection are presented below. Emetogenic chemotherapy and radiation therapy The recommended intravenous or intramuscular dose of Zofran is 8 mg as a slow injection immediately before the start of chemotherapy. To prevent attacks of late or delayed vomiting after the first 24 hours, oral or rectal use of the drug is recommended. Highly emetogenic chemotherapy For patients receiving highly emetogenic chemotherapy (eg, high-dose cisplatin), Zofran can be prescribed as a single dose of 8 mg IV or IM immediately before the start of chemotherapy. Doses above 8 mg (up to 32 mg) can only be used as an intravenous infusion in 50–100 ml of physiological solution or other appropriate solvent; infusion duration is at least 15 minutes. Another route of administration is 8 mg of Zofran as a slow IV or IM injection immediately before the start of chemotherapy, followed by 2x IV or IM administration of 8 mg after 2 and 4 hours or by continuous infusion of 1 mg/day. h for 24 hours. The choice of dosage regimen depends on the severity of the emetogenic effect. The effectiveness of Zofran in highly emetogenic chemotherapy can be increased by adding a single intravenous dose of dexamethasone 20 mg before starting chemotherapy. To prevent attacks of late or prolonged vomiting during the first 24 hours, oral or rectal use of the drug is recommended. Children and adolescents (ages 6 months to 17 years) Children with body surface area ≤0.6 m2 are given an initial dose of 5 mg/m2 IV immediately before chemotherapy, followed by oral Zofran 2 mg every 12 hours. Oral use of the drug at a dose of 2 mg 2 times a day can be continued for 5 days after completion of the course of treatment. For children with a body surface area of 0.6–1.2 m2, Zofran at a dose of 5 mg/m2 of body surface can be administered as a single intravenous injection immediately before chemotherapy, followed by the use of Zofran tablets at a dose of 4 mg after 12 hours. Oral use can be continued for up to 5 days after completion of the course of treatment. Children with a body surface area of 1.2 m2 may be given an IV injection at an initial dose of 8 mg immediately before chemotherapy, followed by oral Zofran tablets at a dose of 8 mg after 12 hours. Oral use of 8 mg 2 times a day should be continued for a period of time up to 5 days after completion of the course of treatment. Alternatively, in children over 6 months of age, Zofran at a dose of 0.15 mg/kg (not more than 8 mg) can be given as a single IV injection immediately before chemotherapy, the dose can be repeated every 4 hours, but not more than 3 times. Oral use of 4 mg 2 times a day can be continued for up to 5 days after completion of the course of treatment. Dosages recommended for adults should not be exceeded. Elderly patients Zofran is well tolerated by patients over the age of 65 years, regardless of the dose, frequency and route of administration of the drug. Postoperative Nausea and Vomiting Adults For the prevention of postoperative nausea and vomiting, the recommended dose of Zofran is 4 mg as a single IM or slow IV injection during induction of anesthesia. For the treatment of postoperative nausea and vomiting, a single dose of 4 mg Zofran as an IM or slow IV injection is recommended. Children and adolescents (ages 1 month to 7 years) To prevent and treat postoperative nausea and vomiting in children undergoing surgery under general anesthesia, Zofran can be administered at a dose of 0.1 mg/kg body weight (up to a maximum of 4 mg) by slow intravenous injection before, during and after the onset of anesthesia or after surgery. Elderly Patients Experience with the use of Zofran for the prevention and treatment of postoperative nausea and vomiting in the elderly is limited, but Zofran is well tolerated in patients over 65 years of age receiving chemotherapy.
Zofran instructions for use
Pharmacological action Zofran is a drug from the group of antiemetics. The drug contains the active component ondansetron, a selective blocker of serotonin 5HT3 receptors. The drug has a pronounced antiemetic effect. The mechanism of action of the drug is not fully understood; presumably, the therapeutic effect of the drug is due to the inhibition of serotonin 5HT3 receptors in the central and peripheral nervous system, the stimulation of which occurs during chemotherapy, which increases the release of serotonin. The drug does not have a sedative effect and does not affect the level of prolactin in plasma. After oral administration, the drug is well absorbed from the gastrointestinal tract. Ondansetron is characterized by a first-pass effect through the liver. The peak plasma concentration of the active component is observed 1.5 hours after oral administration of the drug and 6 hours after rectal administration. When taking the drug simultaneously with food, the bioavailability of ondansetron increases. Metabolized in the liver, excreted mainly by the kidneys in the form of metabolites, about 5% of the drug is excreted unchanged by the kidneys. The half-life of the drug reaches 3 hours, in elderly patients - 5 hours, after rectal administration of the drug - about 6 hours (due to longer absorption of the drug in the rectum). In patients with severe renal impairment, the half-life increases to 15-20 hours. The pharmacokinetics of the drug is the same for single and repeated use. In patients with impaired renal function, systemic clearance and volume of distribution of the active component are reduced. The half-life in patients with impaired renal function and creatinine clearance from 15 to 60 ml/min reaches 5.4 hours. In patients on hemodialysis, the pharmacokinetics of the drug corresponds to those in patients with normal renal function. In patients with severe liver dysfunction, there is a decrease in systemic clearance of the active component of the drug, an increase in the half-life (15-32 hours) and oral bioavailability (100%). In women, the systemic clearance and volume of distribution of ondansetron is slightly lower than in men. Indications for use The drug is used for the treatment and prevention of vomiting in patients undergoing cytostatic chemotherapy or radiotherapy. The drug is also prescribed for the prevention and treatment of nausea and vomiting in patients who have undergone surgery. For the treatment of patients in the postoperative period, the drug Zofran in the form of suppositories is not used.
Directions for use Solution for injection The drug is intended for parenteral use. The ampoule with the drug should be opened immediately before use; if not all of the solution is used, the remaining part should be discarded. The prepared solution for infusion can be stored at a temperature of 2 to 8 degrees Celsius for no more than 24 hours. The drug in a dose of 8 mg or less can be administered intramuscularly, intravenously and as an intravenous infusion. If the dose exceeds 8 mg, the drug is administered only as an intravenous infusion. Intramuscularly, the drug is injected slowly into the upper outer quadrant of the gluteal muscle. To prepare a solution for intravenous infusion, the following solvents can be used: 0.9% sodium chloride solution; Ringer's solution; 10% mannitol solution; 5% glucose solution; A solution of 0.3% potassium chloride and 0.9% sodium chloride; A solution of 0.3% potassium chloride and 5% glucose. The drug is stable when used in polyethylene infusion bags and type 1 glass vials. Solutions of the drug in 5% glucose solution or 0.9% sodium chloride solution, as well as solutions of the drug in other compatible solutions for intravenous administration, are stable in polypropylene syringes. It is allowed to simultaneously administer solutions of the drug with a concentration of 16 to 160 μg/ml (8 mg/500 ml and 8 mg/50 ml) through a Y-shaped injector with: Cisplastin (concentration 0.48 mg/ml) for 1-8 hours; 5-fluorouracil (concentration 0.8 mg/ml) at a rate of no more than 20 ml per hour; Carboplatin (concentration 0.18-9.9 mg/ml) for 10-60 minutes; Etoposide (concentration 0.14-0.25 mg/ml) for 30-60 minutes; Ceftazidime (dose 250-2000 mg), dissolved in water for injection according to the instructions, over 5 minutes as an intravenous bolus injection; Cyclophosphamide (dose 100-1000 mg) dissolved in water for injection according to the instructions, over 5 minutes as an intravenous bolus injection; Doxorubicin (dose 10-100 mg) dissolved in water for injection according to the instructions, over 5 minutes as an intravenous bolus injection; The drug can also be mixed in one dropper with dexamethasone phosphate sodium salt (ondansetron dose in solution from 8 μg/ml to 1 mg/ml, dexamethasone phosphate dose in solution from 32 μg/ml to 2.5 g/ml) administration time 50-100 ml of solution not less 15 minutes. The duration of the course of treatment and the dose of the drug are determined by the attending physician individually for each patient. For adults undergoing chemotherapy or radiotherapy for nausea and vomiting, 8 mg of the drug is usually given slowly before starting therapy. If nausea or vomiting continues for more than 24 hours after the start of therapy, patients are prescribed Zofran in oral or rectal dosage forms. Adults receiving highly emetogenic drugs for nausea and vomiting are usually given 8 mg of the drug slowly before starting chemotherapy. Depending on the emetogenicity of the drug, the dose of the drug is increased (maximum dose 32 mg) and administered as an intravenous infusion. In addition, when treating with highly emetogenic drugs, patients may be prescribed ondansetron according to the scheme: 8 mg intravenously slowly before chemotherapy, followed by 2 repeated administrations of 8 mg of the drug at an interval of 2-4 hours. It is also possible to prescribe ondansetron as an intravenous infusion at a rate of 1 mg/hour for 24 hours. To increase the effectiveness of the drug, some patients are prescribed a single intravenous injection of 20 mg of dexamethasone phosphate sodium salt before starting chemotherapy. If nausea or vomiting continues for more than 24 hours after the start of therapy, patients are prescribed Zofran in oral or rectal dosage forms. Before chemotherapy, children are usually prescribed intravenous administration of 5 mg/m2 of the drug. 12 hours after parenteral administration of the drug, 4 mg of ondansetron is usually prescribed orally, 2 times a day. Oral forms of the drug should be taken within 5 days after the end of chemotherapy. Before surgery, adults are usually prescribed 4 mg of the drug intravenously or intramuscularly during induction of anesthesia to prevent nausea and vomiting. For the treatment of vomiting in the postoperative period, adults are usually prescribed a single slow intravenous or intramuscular injection of 4 mg of the drug. Before surgery, children are usually prescribed the drug at a dose of 0.1 mg/kg body weight intravenously to prevent nausea and vomiting during the period of induction anesthesia (it is also possible to administer the drug before or after induction anesthesia). For the treatment of vomiting in the postoperative period, children are usually prescribed a single intravenous slow administration of the drug at a dose of 0.1 mg/kg body weight. The maximum dose of the drug for children with postoperative vomiting is 4 mg of ondansetron. The maximum daily dose of the drug for patients suffering from liver dysfunction is 8 mg. Syrup, film-coated tablets, lingual tablets: The drug is intended for oral use. It is recommended to swallow film-coated tablets whole, without chewing or crushing, with the required amount of liquid. It is recommended to keep the lingual tablets in the mouth until completely dissolved (1-2 minutes) and then swallow. It is recommended to take the syrup undiluted; dosing the drug in syrup form is done using a special measuring spoon, which is included in the pack along with the bottle. The duration of the course of treatment and the dose of the drug are determined by the attending physician individually for each patient. For adults undergoing chemotherapy or radiotherapy, nausea and vomiting are usually prescribed 8 mg of the drug 1-2 hours before the start of therapy. After which the drug is re-administered 12 hours later at a dose of 8 mg. To prevent late vomiting, adults are usually prescribed 8 mg of the drug 2 times a day. The drug should be taken within 5 days after completing chemotherapy or radiotherapy. For adults receiving therapy with highly emetogenic drugs, for nausea and vomiting, 24 mg of the drug is usually prescribed in combination with 12 mg of dexamethasone phosphate sodium salt 1-2 hours before the start of chemotherapy. To prevent late vomiting, 8 mg of ondansetron 2 times a day is usually prescribed 24 hours after the first dose of the drug. The drug should be taken within 5 days after the end of chemotherapy. Children are usually prescribed parenteral administration of the drug before chemotherapy. 12 hours after parenteral administration of the drug, 4 mg of ondansetron is usually prescribed orally, 2 times a day. The drug should be taken within 5 days after the end of chemotherapy. Before surgery, adults are usually prescribed 16 mg of the drug once 60 minutes before the start of general anesthesia to prevent nausea and vomiting. For the treatment of vomiting in the postoperative period, it is recommended to use the drug in the form of a solution for parenteral administration. Rectal suppositories: The drug is intended for rectal use. The duration of the course of treatment and the dose of the drug are determined by the attending physician individually for each patient. For adults undergoing chemotherapy or radiotherapy, for nausea and vomiting, 1 suppository of the drug is usually prescribed 1-2 hours before the start of therapy. To prevent late vomiting, adults are usually prescribed 1 suppository of the drug once a day. The drug should be used within 5 days after completing chemotherapy or radiotherapy. For adults receiving therapy with highly emetogenic drugs, for nausea and vomiting, 1 suppository of the drug is usually prescribed 1-2 hours before the start of chemotherapy. To enhance the therapeutic effect of the drug, a single intravenous injection of 20 mg of dexamethasone phosphate sodium salt is prescribed before starting chemotherapy. For the prevention of late vomiting, adults are usually prescribed 1 suppository of the drug 1 time per day 24 hours after the first dose of the drug. The drug should be used within 5 days after the end of chemotherapy.
Side effects When using the drug, patients experienced the development of the following side effects: From the gastrointestinal tract: nausea, vomiting, stool disorders, hiccups, increased activity of liver enzymes, dry mouth. When using the drug in the form of suppositories, a burning sensation in the anal area may occur. From the central and peripheral nervous system: headache, dizziness, convulsions. From the cardiovascular system: flushing of the face and upper body, cardialgia, heart rhythm disturbances, decreased blood pressure, bradycardia. Allergic reactions: skin rash, itching, urticaria, bronchospasm, Quincke's edema, anaphylactic shock. Others: blurred vision, increased creatinine levels in the blood; when using the drug in the form of an injection solution, pain, irritation and the development of an inflammatory process at the injection site are possible.
Contraindications Increased individual sensitivity to the components of the drug. The drug is not used for the treatment of women during pregnancy and lactation. The drug Zofran in the form of suppositories is not used to treat children under the age of 18 years; the drug in the form of syrup and lingual tablets is not prescribed to children under the age of 2 years. The drug in the form of lingual tablets is not prescribed to patients suffering from phenylketonuria. The drug should be prescribed with caution to patients with increased individual sensitivity to other drugs from the group of 5HT3 receptor inhibitors, as well as patients with subacute intestinal obstruction and elderly patients. The drug in the form of a solution for parenteral use should be prescribed with caution to patients suffering from impaired cardiac conduction and rhythm, as well as impaired water and electrolyte balance.
Pregnancy At the moment, there are no reliable data on the safety of ondansetron for the fetus. During animal studies of the drug, no mutagenic, teratogenic or embryotoxic effects of ondansetron were observed. The attending physician can prescribe the drug Zofran to women during pregnancy for health reasons. If it is necessary to use the drug during lactation, you should consult with your doctor and decide whether to interrupt breastfeeding.
Drug interactions There were no pharmacokinetic interactions of the drug with other drugs. Phenytoin, rifampicin, carbamazepine and other drugs that inhibit or induce liver enzymes, when used in combination with the drug, can affect its metabolism and change plasma concentrations of ondansetron. Medicines that alter the activity of liver enzymes should be used with caution in combination with ondansetron.
When used in combination, the drug reduces the effectiveness of tramadol. The drug in the form of a solution for parenteral use is compatible with dexamethasone phosphate, saline, 5% glucose solution, 0.3% potassium chloride and 0.9% sodium chloride solution, 0.3% potassium chloride and 5% glucose solution, as well as Ringer's and 10% mannitol solution. The drug should not be administered in the form of a solution for parenteral use in the same syringe or dropper with other drugs other than those listed above.
Overdose There is currently insufficient data on overdose of Zofran. When using excessive doses of the drug in patients, the risk of developing and the severity of side effects increases. There is no specific antidote. In case of drug overdose, symptomatic therapy is indicated. In case of an overdose of the drug, it is not recommended to use ipecac, due to the low probability of its effectiveness in case of an overdose of ondansetron.
Release form: Film-coated tablets, 5 pieces in a blister pack, 2 blister packs in a cardboard box. Lingual tablets, 10 pieces in a blister pack, 1 blister pack in a cardboard box. Syrup 50 ml in dark glass bottles, 1 bottle in a cardboard box. Solution for injection, 2 or 4 ml in ampoules, 5 ampoules in a cardboard box. Rectal suppositories, 1 piece in a blister pack, 1 or 2 blister packs in a cardboard box.
Storage conditions It is recommended to store the drug in a dry place away from direct sunlight at a temperature of 15 to 30 degrees Celsius. It is recommended to store the bottle of syrup for oral use in an upright position. The shelf life of the drug in tablet form is 3 years. The shelf life of the drug in the form of lingual tablets is 2 years. The shelf life of the drug in syrup form is 3 years. The shelf life of the drug in the form of suppositories is 3 years. The shelf life of the drug in the form of a solution for parenteral use is 3 years. The shelf life of the prepared infusion solution is no more than 24 hours at a temperature of 2 to 8 degrees Celsius.
Composition of 1 ml of injection solution contains: Ondansetron dihydrate hydrochloride (in terms of ondansetron) – 2 mg; Excipients.
1 film-coated tablet of Zofran 4 contains: Ondansetron dihydrate hydrochloride (in terms of ondansetron) – 4 mg; Excipients.
1 film-coated tablet of Zofran 8 contains: Ondansetron dihydrate hydrochloride (in terms of ondansetron) – 8 mg; Excipients.
1 lingual tablet of the drug Zofran 4 contains: Ondansetron dihydrate hydrochloride (in terms of ondansetron) – 4 mg; Excipients, including lactose.
1 lingual tablet of the drug Zofran 8 contains: Ondansetron dihydrate hydrochloride (in terms of ondansetron) – 8 mg; Excipients, including lactose.
5 ml of syrup contains: Ondansetron dihydrate hydrochloride (in terms of ondansetron) – 4 mg; Excipients.
1 rectal suppository contains: Ondansetron dihydrate hydrochloride (in terms of ondansetron) – 16 mg; Excipients.
Pharmacological group Medicines used to treat malignant neoplasms Medicines used to correct the side effects of anticancer drugs Antiemetics
Active ingredient: ondansetron
Side effects of Zofran™
They are classified according to organs and systems and the frequency of their occurrence. By frequency they are divided into the following categories: very often (≥1/10), often (≥1/100, but ≤1/10), infrequently (≥1/1000, but ≤1/100), rarely (≥1/10 000, but ≤1/1000), very rare (≤1/10,000, including isolated cases). Immune system: rarely , including anaphylaxis. Nervous system: very often - headache, often - movement disorders (including extrapyramidal disorders, such as oculogyric crisis, dystonic reactions) and dyskinesia without persistent clinical consequences, convulsions, rarely - dizziness during rapid intravenous administration of the drug. Organ of vision: rarely - transient visual disturbances (blurred vision), most often with rapid intravenous administration, very rarely - transient blindness, mainly with intravenous administration. In most cases, blindness disappears within 20 minutes after the end of the drug administration. As a rule, most patients receive chemotherapy with cisplatin. Some reports believed that cases of transient blindness were of cortical origin. Cardiovascular system: infrequently - arrhythmias, pain in the heart region (with ST ), bradycardia, hypotension, often - a feeling of warmth or flushing of the face. Respiratory system and chest organs: infrequently - hiccups. Gastrointestinal tract: often - constipation. Hepatobiliary system: uncommon - transient asymptomatic increase in transaminase activity in the blood serum. These cases occur primarily in patients receiving cisplatin chemotherapy. General disorders: often - local reactions in the injection area.
Special instructions for the use of Zofran™
When treating patients with manifestations of hypersensitivity to other selective 5HT3 receptor antagonists, hypersensitivity reactions were observed. Because ondansetron impairs intestinal motility, patients with signs of subacute intestinal obstruction should be closely monitored while using Zofran. Zofran solution ampoules do not contain preservatives and should be used immediately after opening; the remaining unused solution should be destroyed. Ampoules containing Zofran solution cannot be autoclaved. Compatibility with other solutions for intravenous administration. Solutions for intravenous administration should be prepared immediately before infusion. However, it has been established that ondansetron solution remains stable for 7 days at room temperature (up to 25 ° C) in daylight or in the refrigerator when dissolved in the following media: sodium chloride solution 0.9%; glucose solution 5%; manitol solution 10%; Ringer solution; potassium chloride solution 0.3%; sodium chloride solution 0.9%; solution of potassium chloride 0.3%. A study was carried out on the compatibility of the drug with polyvinyl chloride bottles and infusion systems. It has been established that ondansetron remains stable when using polyethylene and glass vials. Ondansetron in 0.9% sodium chloride or 5% glucose solution has been shown to remain stable in polypropylene syringes. It has also been proven that stability in polypropylene syringes is maintained when ondansetron is diluted with other recommended solutions. If long-term storage of the drug is necessary, dissolution should be carried out under appropriate aseptic conditions. Compatibility with other drugs Zofran can be used as an intravenous infusion at a rate of 1 mg/hour. Through an X-like injector, together with Zofran, at a concentration of ondansetron from 16 to 160 mcg/ml (that is, 8 mg/500 ml or 8 mg/50 ml, respectively), you can administer: • cisplatin at a concentration of up to 0.48 mg/ml for 1–8 hours; •5-fluorouracil in concentrations up to 0.8 mg/ml at a rate of no more than 20 ml/h (higher concentrations of 5-fluorouracil may cause precipitation of ondansetron). 5-fluorouracil infusion solution may contain up to 0.045% magnesium chloride in addition to other compatible excipients; •carboplatin at a concentration of 0.18–9.9 mg/ml for 10–60 minutes; •etoposide at a concentration of 0.14–0.25 mg/ml for 30–60 minutes; •ceftazidime in a dose of 250 mg to 2 g, dissolved in water for injection (for example, 2.5 ml per 250 mg or 10 ml per 2 g of ceftazidime), as an IV bolus injection over 5 minutes; •cyclophosphamide in a dose of 100 mg to 1 g, dissolved in water for injection (5 ml per 100 mg of cyclophosphamide), as an IV bolus injection over 5 minutes; •doxorubicin at a dose of 10–100 mg, dissolved in water for injection (5 ml per 10 mg of doxorubicin), as an IV bolus injection over 5 minutes; dexamethasone at a dose of 20 mg as a slow intravenous injection over 2–5 minutes (with simultaneous administration of 8 mg or 32 mg of ondansetron dissolved in 50–100 ml of injection solution) over approximately 15 minutes. Special warning When treating patients with manifestations of hypersensitivity to other selective 5HT3 receptor antagonists, hypersensitivity reactions have been observed. Very rarely, and mainly with intravenous use of Zofran, temporary ECG changes are noted, including prolongation of the QT . Because ondansetron impairs intestinal motility, patients with signs of subacute intestinal obstruction should be closely monitored while using Zofran. During pregnancy and breastfeeding. The safety of Zofran during pregnancy in humans has not been established. In experimental studies on animals, Zofran did not disrupt the development of the embryo or fetus and did not affect the course of pregnancy, pre- and postnatal development. However, since animal studies are not always predictive in humans, Zofran is not recommended for use during pregnancy. In experimental studies, ondansetron has been shown to be excreted into the breast milk of animals. If it is necessary to prescribe the drug during breastfeeding, breastfeeding should be stopped. Impact on the ability to drive vehicles and operate machinery. In psychomotor tests, ondansetron does not affect driving or operating machinery and does not have a sedative effect.
Depending on the timing and mechanism of development, there are three types of nausea and vomiting caused by cytostatic treatment:
- Acute – develops in the first 24 hours.
- Delayed - develops in the days following the first day.
- Previous – develops before cytostatic treatment.
Each type of nausea and vomiting has its own mechanisms of development, which leads to different approaches and principles for their prevention and treatment.
One of the main mechanisms for the development of acute nausea and vomiting after antitumor treatment is the release of serotonin (5-hydroxytryptamine or 5-HT) when cytostatics act on the mucous membrane of the small intestine (the main reservoir of this mediator). The released serotonin further stimulates specific 5-HT3 receptors in the trigger zone of the central nervous system, impulses from which are transmitted to the vomiting center, which leads to the development of nausea and vomiting. In addition, the effect of serotonin is realized through its effect on peripheral receptors of the vagus nerve with subsequent transmission to the vomiting center. In addition to serotonin, other receptors (for example, dopamine and neurokinin) are also involved in the genesis of acute vomiting. The mechanisms of development of delayed nausea and vomiting are less well understood, but it is known that serotonin plays a much smaller role in them. Preceding nausea and vomiting is a situationally conditioned reaction that develops as a conditioned reflex, mainly in patients who previously had inadequate control of acute and delayed nausea and vomiting [1].
Without adequate antiemetic therapy, some cytostatics can cause vomiting in more than 90% of patients (highly emetogenic chemotherapy) or in 30–90% of patients (moderately emetogenic chemotherapy). Of the highly emetogenic drugs in clinical practice, the most commonly used are cisplatin ≥ 50 mg/m2, cyclophosphamide ≥ 1500 mg/m2, dacarbazine; from moderately emetogenic - doxorubicin ≥ 60 mg/m2, carboplatin, oxaliplatin, epirubicin, ifosfamide, cyclophosphamide ≤ 1500 mg/m2, cisplatin ≤ 50 mg/m2.
Acute nausea and vomiting
The creation of antiemetic drugs from the group of 5-HT3 receptor antagonists has made a real revolution in the prevention and treatment of acute nausea and vomiting caused by cytostatic therapy. The first such antiemetic to demonstrate clinical effectiveness was Zofran (ondansetron), which is the most studied and widely used drug in this group in the world. When studying new antiemetic drugs, many clinical studies use Zofran as the standard antiemetic therapy.
Studies that first proved the high effectiveness of Zofran were conducted in the early 1990s. In these studies, Zofran was used intravenously either at a dose of 32 mg once before the administration of cytostatics, or 8 mg (0.15 mg/kg) 3 times a day (30 minutes before the administration of chemotherapy, 4 hours and 8 hours after administration first dose). Early studies showed a highly significant benefit of Zofran over placebo, making further placebo-controlled studies unethical.
In the early 1990s. Zofran has been used as monotherapy. During this period, many studies were conducted to find the optimal dose of the drug. Due to the low toxicity of Zofran, the doses used varied widely (8–32 mg), and the main task of the researchers was to determine not the maximum tolerated dose, but the smallest clinically effective dose. In a study by Beck et al. in a sample of 699 patients receiving high (more than 100 mg/m2) or moderate doses (50–70 mg/m2) of cisplatin, it was shown that Zofran at a dose of 32 mg, administered once IV before cisplatin, was more effective than Zofran in dose 8 mg. The rate of achieving complete control of acute vomiting when using Zofran at these doses in the group of patients receiving high doses of cisplatin was 48 versus 35%, and in the group receiving medium doses – 73 and 50%, respectively. The failure rate of antiemetic therapy (more than 5 episodes of vomiting in the first 24 hours) also varied significantly: 20 and 34%, respectively, with high doses of cisplatin, 9 and 23% with medium doses. Also in this study, a single intravenous dose of 32 mg of Zofran was shown to be equally effective compared with its 3-fold administration of 8 mg with an interval of 4 hours [2].
At the same time, in the studies of Seynayeve et al. [3] and Ruff et al. [4] Zofran 32 mg was not shown to be superior to 8 mg. Thus, in the study [3], 535 patients who received cisplatin at a dose of 50–120 mg/m2 were randomized: group 1 – Zofran 8 mg IV + 24-hour infusion 1 mg/hour, group 2 – Zofran 32 mg IV /in once and group 3 – Zofran 8 mg intravenously once. Complete and almost complete control of acute vomiting (less than 2 episodes) were achieved in 74, 78 and 74% of cases, respectively.
In addition to the injectable form of Zofran, its tablet form is widely used to control acute nausea and vomiting. Thus, in a study by Needles et al. compared the effectiveness of different doses of Zofran administered orally in highly emetogenic chemotherapy containing cisplatin at a dose of ≥ 50 mg/m2: group 1 - 8 mg 2 times a day, group 2 - 24 mg once and group 3 - 32 mg once. Control of acute vomiting was achieved in 55, 66 and 55% of cases, respectively, and control of acute nausea in 36, 56 and 50%. Based on this, as well as a number of other studies, it was concluded that the most adequate dose for highly emetogenic chemotherapy is 24 mg orally once 30 minutes before cisplatin administration [5]. At the same time, when conducting moderately emetogenic chemotherapy, the administration of Zofran at a dose of 8 mg 2 times a day allows for complete control of acute vomiting in 61% of cases, which is no worse, and according to some data, even more effective than the oral administration of Zofran 8 mg 3 times a day.
However, at the moment, the control of acute nausea and vomiting achieved with the use of Zofran in monotherapy (complete control in 40-50% of cases, more than 5 episodes - no control - in 14-21%) cannot be considered satisfactory. A large number of studies have been conducted showing that the addition of corticosteroids to 5-HT3 receptor antagonists leads to a potentiation of the antiemetic effect of the latter: the rate of complete control of nausea and vomiting during highly emetogenic chemotherapy increases to 75–85% (Table 1) [6–8].
These studies showed that the use of corticosteroids can increase the antiemetic effectiveness of any dose of Zofran. Based on this, it is now believed that they should be prescribed in any case where the emetogenic potential of chemotherapy makes the use of 5-HT3 antagonists necessary. Due to minimal mineralocorticoid activity, dexamethasone is most widely used in clinical practice. For antiemetic purposes, corticosteroids are prescribed in a short course, which makes the development of their side effects unlikely. However, we should not forget about adequate antihypertensive therapy in patients with arterial hypertension and the need for strict control over blood glucose levels in patients with diabetes mellitus.
At the same time, a number of researchers still continue to use Zofran in mono mode. Thus, in a recent comparative study examining the effectiveness of a new 5-HT3 receptor antagonist, palonosetron, in moderately emetogenic chemotherapy in the control group (standard antiemetic treatment), Zofran was used at a dose of 32 mg IV once before the administration of chemotherapy. In all study groups, prophylactic use of corticosteroids was not permitted. Despite the fact that only 18% of patients included in the study received cisplatin-containing therapy, complete control of acute vomiting in the Zofran group was achieved in only 68.6% of patients [15]. Such effectiveness, comparable or even inferior to the effectiveness of controlling acute vomiting in patients receiving high doses of cisplatin during prophylaxis with the combination of Zofran + dexamethasone, cannot be considered adequate in accordance with modern standards.
Delayed nausea and vomiting
The use of a combination of 5-HT3 receptor antagonists with corticosteroids has significantly solved the problem of acute nausea and vomiting. At the same time, delayed nausea and vomiting still pose a serious clinical problem.
In the prevention and treatment of this complication, 5-HT3 receptor antagonists have much less effectiveness, which, according to most studies, is comparable to the effectiveness of standard doses of metoclopramide [16]. Currently, corticosteroids are considered the key drugs for the prevention of delayed nausea and vomiting [17–19], and 5-HT3 receptor antagonists or metoclopramide lead to only a slight increase in their effectiveness (Table 2).
As noted above, in combination with dexamethasone, the effectiveness of metoclopramide and 5-HT3 receptor antagonists is comparable, and the choice of drug to add to dexamethasone should be based on cost and tolerability. The recommended dose of Zofran for the prevention of delayed nausea and vomiting is 8 mg 2 times a day for 2–5 days.
At the same time, as follows from the data presented, not all patients receiving cisplatin-containing therapy can achieve control of delayed nausea and vomiting even by prescribing a combination of dexamethasone + a 5-HT3 receptor antagonist. One of the proposed mechanisms for the development of vomiting is the effect of neurokinin substance P on specific NK1 receptors in the central nervous system. Randomized trials have shown that NK1 receptor antagonists increase the control of acute delayed-onset nausea and vomiting [21, 22]. In this regard, the triple combination (substance P antagonist + 5-HT3 receptor antagonist + corticosteroid) in the latest MASCC consensus of 2004 is recognized as the standard of adequate antiemetic therapy for highly emetogenic chemotherapy.
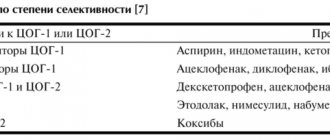
Based on the conclusions of a number of consensus conferences, the following principles for the prevention and treatment of nausea and vomiting have been developed and adopted, depending on the degree of emetogenicity of chemotherapy (Table 3).
Given the controversy surrounding the doses and schedules of Zofran used to prevent nausea and vomiting during highly and moderately emetogenic chemotherapy, several consensus conferences have been held and concluded that a dose of 8 mg i.v. is adequate for the prevention of acute vomiting. once in combination with dexamethasone. However, according to NCI recommendations and the official labeling for Zofran in the US, a dose of 32 mg IV once or 8 mg 3 times IV, with or without dexamethasone, should be used. These data are presented in more detail in Table. 4 and .
It is extremely important to prescribe adequate antiemetic prophylaxis from the first course of chemotherapy, since patients who experienced nausea and vomiting during the first administration of cytostatics significantly increase the risk of developing these complications in the future [1].
Previous nausea and vomiting
According to the results of the analysis conducted by Burish et al., previous nausea and vomiting by the time they received the 4th course of chemotherapy was observed in 30% of patients [23]. Symptoms may occur outside the clinic, in the clinic, when talking about chemotherapy, or when the patient experiences specific smells and tastes. Antiemetic drugs used to treat acute and delayed nausea and vomiting are usually ineffective in cases of pre-existing nausea and vomiting. To treat pre-existing nausea and vomiting, foreign guidelines recommend the use of suggestive methods - psychotherapy, relaxation, hypnosis, as well as drugs from the benzodiazepine group [24, 25]. The main method of preventing pre-existing nausea and vomiting is adequate control of acute and delayed nausea and vomiting from the first course of chemotherapy.
Nausea and vomiting due to radiation
Depending on the risk of nausea and vomiting, radiation therapy is recommended to be divided into highly emetogenic (total therapeutic irradiation of the body, irradiation of the upper half of the body, irradiation of the entire abdomen and retroperitoneum), moderately emetogenic (irradiation of the lower half of the chest or epigastric region, irradiation of the pelvis, irradiation of the lower half body), and low-emetogenic (irradiation of the head, neck, extremities) [26]. In highly emetogenic radiotherapy, 5-HT3 receptor antagonists are the drugs of choice [27]. At the same time, unlike chemotherapy, radiation therapy is usually carried out over a long period of time (weeks), which makes the use of non-injectable forms of drugs preferable. Due to the availability of a variety of dosage forms (see below), Zofran is perhaps the most optimal 5-HT3 receptor antagonist for the prevention of nausea and vomiting during highly and moderately emetogenic radiotherapy. For use for this purpose, Zofran (in tablets or lingual tablets) at a dose of 8 mg 3 times a day can be recommended.
Nausea and vomiting during multi-day chemotherapy courses
When using multi-day regimens, the main problem on the first day is acute vomiting, and subsequently delayed nausea and vomiting become more important. The most optimal option for multi-day highly or moderately emetogenic chemotherapy is the administration of a 5-HT3 receptor antagonist (Zofran) in combination with dexamethasone throughout the entire treatment period (prevention of acute vomiting) followed by the use of dexamethasone for the prevention of delayed vomiting [28].
Refractory nausea and vomiting
Despite advances in modern antiemetic therapy, some patients still experience nausea and vomiting during radiation and chemotherapy. The most obvious reason for this may be non-compliance with recommendations (inadequate dose of 5-HT3 receptor antagonists, lack of corticosteroids in the antiemetic regimen, etc.). Usually this problem is quite easily solved and requires only antiemetic therapy to generally accepted standards. If the patient is already receiving adequate therapy, the likelihood of selecting an effective antiemetic combination is low. Various studies have suggested the following approaches: administration of an additional dose of a 5-HT3 receptor antagonist, use of another drug from this group in subsequent cycles of chemotherapy, sedation [29–32]. The use of these methods made it possible to achieve an antiemetic effect in 30–33% of patients who had not previously responded to standard antiemetic therapy. At the same time, they cannot be recommended as standards due to the small number of patients included in the studies.
Special dosage forms of Zofran
In addition to the traditional forms of Zofran (tablets and ampoules), oncologists also have non-parenteral forms of the drug such as lingual tablets and suppositories, which have certain advantages.
Thus, lingual tablets are absorbed by the oral mucosa within a few seconds, which ensures a faster onset of effect. This advantage allows the widespread use of Zofran lingual tablets in patients with impaired swallowing. LeBourgeois JP et al. showed the effectiveness of this form of Zofran in patients receiving radiation therapy. In this study, patients were randomized into 3 groups: patients of the first group received lingual Zofran tablets at a dose of 8 mg every 12 hours, the second - at a dose of 16 mg every 12 hours, and the third - placebo. There were no statistically significant differences in effectiveness between the two treatment groups. At the same time, patients who received lingual tablets (regardless of the dose) were statistically significantly less likely to report vomiting during radiation therapy compared to the placebo group [33].
One study, which included 427 patients receiving moderately emetogenic chemotherapy including cyclophosphamide, showed that when Zofran was prescribed in lingual form, 8 mg 2 hours before the start of chemotherapy, then 8 mg every 12 hours for 3 days, the frequency of complete and partial antiemetic control (64 and 14%) was comparable to that in the group of patients receiving Zofran tablets in a similar regimen (63 and 17%). Complete control of vomiting within 3 days was comparable in both groups (64 and 63%, respectively) [34].
Recommendations for the use of lingual tablets.
- To control acute vomiting during moderately emetogenic chemotherapy - 8 mg 2 times a day (1-2 hours before the administration of chemotherapy and 12 hours later).
- For the prevention of delayed nausea and vomiting - 8 mg 2 times a day for 5 days.
- To prevent nausea and vomiting during moderate and highly emetogenic radiation therapy - 8 mg 2 times a day (before the radiation therapy session and 12 hours after it).
- Prevention of postoperative nausea and vomiting - 16 mg once before the start of anesthesia or 8 mg 1 hour before anesthesia + 8 mg 8 and 16 hours after surgery.
Another special non-injectable form of Zofran is suppositories. It has been shown that during moderately emetogenic therapy, the administration of Zofran in suppositories (16 mg 2 hours before the start of chemotherapy, then once a day for 3 days) allows achieving complete antiemetic control on the first day in 73–87% of patients compared to 81–92 % when using Zofran tablets (8 mg 2 hours before chemotherapy, then 8 mg every 12 hours for 3 days) [35, 36]. Moreover, the maximum concentration of the drug in the blood is observed after 3.5 hours and is maintained at a high level for quite a long time. This allows the use of Zofran in suppositories once a day to prevent delayed nausea and vomiting.
Recommendations for the use of suppositories.
- To control acute nausea and vomiting during moderately emetogenic chemotherapy - 16 mg 1 hour before the administration of cytostatics.
- To control delayed nausea and vomiting - 16 mg once a day for 5 days.
Prevention and treatment of postoperative nausea and vomiting
Although most cases of nausea and vomiting in oncological practice are caused by chemotherapy or radiation therapy, we should not forget that surgical interventions with general anesthesia can also lead to the development of these complications.
Unlike other antiemetics from the group of 5-HT3 receptor antagonists, only Zofran (in the form of syrup, injections, tablets or lingual tablets) is recommended for the prevention of postoperative nausea and vomiting, not only at high, but also at low risk of its development. In the preoperative period, Zofran can be prescribed either in oral or injectable form. In the postoperative period, Zofran is prescribed only in the form of injections, which reduces the risk of developing repeated episodes of nausea and vomiting.
The official instructions for Zofran (for the USA) recommend a single dose of 4 mg Zofran IV immediately before the start of anesthesia (studies have not shown the benefit of 8 mg) or 16 mg orally. To prevent repeated episodes of nausea and vomiting in the postoperative period in patients who have not received preoperative prophylaxis and have already noted episodes of vomiting, a single intravenous administration of Zofran at a dose of 4 mg is recommended.
Use of Zofran in pregnant women
A recent study by Einarson A. [37] showed that the use of Zofran as an antiemetic drug during toxicosis of pregnancy does not increase the risk of developing serious fetal malformations. Considering that currently antitumor treatment does not require mandatory termination of pregnancy, the data obtained allow us to recommend Zofran as an antiemetic drug in this category of patients.
Thus, Zofran (ondansetron) is an effective and safe antiemetic from the group of 5-HT3 receptor antagonists, and thanks to the availability of new dosage forms (lingual tablets, syrup, suppositories), it can be conveniently used in almost any clinical situation.
Drug interactions Zofran™
Ondansetron does not accelerate or inhibit the metabolism of other drugs when used simultaneously. Special studies have shown that ondansetron does not interact with alcohol, temazepam, furosemide, tramadol and propofol. Ondansetron is metabolized by a variety of liver cytochrome P459 enzymes: CYP 3A4, CYP 2D6 and CYP 1A2. Due to the diversity of ondansetron metabolic enzymes, inhibition or reduction in the activity of one of them (for example, genetic deficiency of CYP 2D6) is under normal conditions compensated by other enzymes and will have no or negligible effect on total creatinine clearance. Phenytoin, carbamazepine and rifampicin In patients receiving therapy with drugs that are potential inducers of CYP 3A4 (for example, phenytoin, carbamazepine and rifampicin), the clearance of ondansetron increases and its concentration in the blood decreases. Tramadol According to a small number of clinical studies, ondansetron may reduce the analgesic effect of tramadol.
Zofran
Zofran is an original brand drug from the British pharmaceutical concern GlaxoSmithKline (currently produced by subsidiaries in Canada, Germany, France, Poland and Russia), which is based on the pharmacologically active substance ondansetron, which has a pronounced antiemetic effect. Negative physiological phenomena such as nausea and vomiting are frequent accompaniments of cytostatic therapy. They arise due to the massive release of serotonin under the influence of antitumor drugs on the mucous membrane of the small intestine (this, as is known, is the main “storage” of serotonin). Secreted serotonin activates specific 5-HT3 receptors located in the so-called trigger zone of the central nervous system, from where nerve impulses are transmitted to the vomiting center of the medulla oblongata. So, in short, the mechanism of development of nausea and vomiting is described. There is also a peripheral way of potentiating the gag reflex - through the effect on the receptors of the vagus nerve. The creation of the drug Zofran, which is an antagonist of 5-HT3 receptors, produced, if not a sensation, then a very loud resonance: after all, a new way to prevent and relieve nausea and vomiting, which is a side effect of chemotherapy, has appeared. Zofran is by far the most researched and widely used drug in its pharmacological group.
Clinical trials that confirmed the high effectiveness and favorable safety profile of Zofran were first conducted in the 90s of the last century. At the same time, this drug was first used as part of antiemetic monotherapy.
However, it was later found that the combination of glucocorticosteroids with 5-HT3 receptor antagonists enhances the antiemetic effect of the latter. Moreover, as studies show, an increase in antiemetic effectiveness occurs with the use of any doses of Zofran.
Zofran is available in five dosage forms: film-coated tablets; lozenges, syrup, injection solution and rectal suppositories. Such a wide arsenal of dosage forms gives doctors the opportunity to use, depending on the situation, the advantages of each of them. For example, lozenges are absorbed in the oral cavity literally in seconds, which determines the rapid occurrence of the pharmacological effect. This dosage form may be used in patients who have difficulty swallowing. Another non-injectable form of Zofran that is of particular interest is suppositories. The peak concentration in the blood of the active substance when used is observed after 3.5 hours and subsequently remains at a given level for quite a long time, which makes it possible to resort to zofran once a day in order to prevent delayed nausea and vomiting. In contrast to other representatives of the glorious tribe of 5-HT3 receptor antagonists, zofran is the only drug recommended for use in the prevention of nausea and vomiting after surgical interventions with a low risk of their development. Before surgery, the drug can be prescribed in any dosage form, and in the postoperative period, to prevent recurrence of vomiting, the optimal dosage form is injection.