- Diagnosis of cervicitis
- Treatment of cervicitis
- Cervicitis and infertility
- Cervicitis and pregnancy
Cervicitis is an inflammatory process that occurs in the cervix. Both the vaginal part of the cervix (exocervix) and the mucous membrane of the cervical canal (endocervix) may be affected. Depending on this, exocervicitis or endocervicitis is diagnosed.
Causes of cervicitis
Cervicitis is a common disease that affects approximately every third woman. This pathology can cause infertility and the development of a number of serious complications during pregnancy.
- Sexually transmitted infectious diseases (chlamydia, gonorrhea, trichomoniasis, mycoplasmosis). Pathogenic microorganisms, penetrating the genital tract, rise up through the vagina and, in the absence of timely treatment, affect the cervix. Further infection of the fallopian tubes (salpingitis) and ovaries (oophoritis) is also possible;
- Infectious diseases caused by opportunistic microorganisms (staphylococcus, streptococcus, E. coli);
- Fungal diseases (candidiasis). Active reproduction of fungi of the genus Candida causes an alkaline environment, which provokes a decrease in local immunity. Damage to the mucous membranes is the cause of the development of vaginitis and cervicitis;
- Bacterial vaginosis (dysbacteriosis) is an inflammatory process of the vaginal mucosa caused by changes in microflora. There is a sharp decrease in the number of lactobacilli and the identification of a large number of polymicrobial anaerobic flora (Klebsiella, Gardnerella, Bacteroides, etc.);
- Damage and trauma to the cervix (surgery, childbirth, artificial termination of pregnancy);
- Diseases of the genitourinary system (pyelonephritis, cystitis);
- Decreased immunity.
The role of cervicitis in obstetric and gynecological pathology
Cervicitis is a total inflammation of the cervix, including inflammation of the mucous membrane of the vaginal part of the cervix (exocervicitis) and the mucous membrane of the cervical canal (endocervicitis). Cervicitis is rarely an isolated condition; as a rule, it is combined with vulvitis and vaginitis, since the woman’s genital organs (vulva, vagina and cervix) form a single ecosystem. Inflammatory processes of the cervix make up a significant proportion of inflammatory diseases of the female genital organs. Cervicitis is most often detected in women of reproductive age (up to 70%), less often during perimenopause. It is quite difficult to establish the true incidence of this pathology, since cervicitis is generally asymptomatic, which does not force patients to see a doctor. In the vast majority of cases, cervicitis is discovered by chance during routine preventive examinations or when women seek treatment for other diseases and syndromes.
Etiology. The mucous membrane of the cervix, as a boundary barrier between the upper genital tract and the external environment, is constantly exposed to damaging factors. Among the latter, sexually transmitted infections have the most aggressive antigenic effect on the cervical mucosa [15]. The etiological structure of cervicitis is constantly changing. In recent years, the number of chlamydial, viral, mycoplasma and mixed infections has increased, the fight against which poses significant difficulties due to the developing resistance of microorganisms to antibiotics and the characteristics of the body's responses. According to various authors, the structure of chronic inflammatory diseases of the cervical canal is currently dominated by cervicitis caused by Chlamydia trachomatis, Neisseria gonorrhoeae, human papillomaviruses and herpes simplex serotype 2 [1, 5, 13]. Among patients with cervical pathology, chlamydia is detected in 40–49% of cases [13]. Cervicitis with trichomoniasis occurs in 5–25% of women, with gonorrhea - in 2%, about 86% of women with chronic cervicitis are infected with human papillomavirus infection (PVI) [6, 16]. It is against the background of a genital infection that inflammatory diseases of the cervix develop, acquiring a chronic, relapsing course. In recent years, the etiology has changed: gram-negative aerobes (Escherichia coli, Proteus, Klebsiella, enterococci) and non-clostridial anaerobes (peptococci, bacteroides) are more often detected. The frequency of viral infections, according to various authors, ranges from 7% to 80% due to difficulties in diagnosis.
Gynecological pathology. It should be remembered that the cervix is the second line of defense of the reproductive system against infections. The mucus secreted by the cervix serves as a biological filter that prevents the penetration of bacterial flora from the vagina into the overlying parts of the reproductive system.
The protective properties of the mucus plug are due to: bactericidal properties; proteolytic activity; immunological activity (mucus contains immunoglobulins of all classes). The presence of cervicitis and ectopia significantly impairs the protective properties of the cervix and contributes to the spread of infection to the overlying sections and the occurrence of inflammatory diseases of the uterus and appendages (IUD). Penetration of infectious agents into the overlying sections occurs with the help of sperm, trichomonas, also with the introduction of an intrauterine device (IUD), induced abortion or other intrauterine interventions. Consequences of undergoing PID include infertility and miscarriage. Often, in 67.7% of cases, inflammatory processes are accompanied by ectopia of the cervix.
Chronic cervicitis, which accompanies most underlying diseases of the cervix, attracts the attention of clinicians, primarily as the basis of malignancy [10]. The process of malignancy is associated with a disruption of the process of reparative regeneration, which, in turn, is largely associated with the dynamics of the chronic inflammatory process. Among sexually transmitted infections, viruses and chlamydia have the greatest modulating effect on the course of reparative regeneration of the cervical mucosa [10]. In patients with chronic exocervicitis, destructive changes in epithelial cells of the endo- and exocervical type progress, affecting the nucleus, organelles and cytoplasmic processes. Intercellular contacts are disrupted, and the sealing of the integumentary epithelium is reduced. With increasing aggressiveness of the damaging effect on the mucous membrane of the cervix (viruses), in patients with chronic exocervicitis, cellular renewal accelerates with a slowdown in cellular differentiation (immature cellular forms appear among cells with signs of maturation). At the same time, the intensity of apoptosis of epithelial cells progressively decreases, which correlates with an increase in atypical changes in stratified squamous epithelium, especially in patients with PVI (virus types 16 and 18).
Obstetric pathology. The problem of cervicitis becomes especially important during pregnancy. In the presence of chronic cervicitis, there is a high probability of miscarriage, premature birth, intrauterine infection of the fetus, and postpartum purulent-septic complications.
In Russia, the incidence of intrauterine infections ranges from 6% to 53%, reaching 70% among premature infants. In the structure of perinatal mortality, the share of intrauterine infection ranges from 2% to 65.6%. There are five main ways of infection entering a pregnant woman’s body: ascending, descending, hematogenous, transdecidual and mixed. The greatest risk is the ascending route of infection, in which infectious agents can penetrate the uterine cavity through the cervical canal. The presence of chronic inflammation in the cervical canal opens the door to infection. With intrauterine infection in the early stages of pregnancy, infectious embryopathies are formed, which are manifested by congenital malformations, primary placental insufficiency, which often ends in spontaneous miscarriage and non-developing pregnancy. Infection in later stages of pregnancy is accompanied by intrauterine growth retardation, the formation of secondary placental insufficiency (often against the background of placentitis), local and generalized infectious lesions of the fetus. Generalized forms of intrauterine infection often develop in the early fetal period (first trimester of pregnancy), since the fetus is not yet able to localize the inflammatory process. In the late fetal period (III trimester), inflammatory changes of a proliferative nature cause narrowing or obstruction of canals and openings, which leads to abnormal development of an already formed organ - pseudodeformities (hydrocephalus, hydronephrosis).
During gestation, the cervix plays the role of a “shutter” that protects the uterine cavity and the fertilized egg from exogenous pathogens. Infectious and inflammatory diseases of the cervix contribute to premature termination of pregnancy due to infection of the amnion, then the chorion (placenta), amniotic fluid and fetus.
Infection of the membranes and waters can occur with an ascending infection. With this type of infection, pathogenic microorganisms, penetrating the amniotic fluid, spread in parallel between the membranes along the chorioamnial space, reaching the basal lamina. Here the pathogen meets a response in the form of leukocyte infiltration. At the same time, a focus of infection forms in the amniotic fluid (avascular and non-reactive environment), and the fetus dies. It can be assumed that the morphological signs of the inflammatory reaction appear secondarily, after the accumulation of the pathogen in the amniotic fluid, when a sufficient dose of bacterial toxins and metabolites penetrates the tissue of the placenta and induces the corresponding pathophysiological mechanism. Apparently, in some cases, inflammatory changes have not yet had time to develop, while infection of the amniotic fluid and fetal death have already occurred [4]. It has been established that the bacterial microflora of the amniotic fluid always coincides with the microorganisms that colonize the cervical canal.
Against the background of the action of the extracellular factor of alteration of the epithelial layer (infection with fungi, protozoa, bacteria), there is an activation of local cervical immunity, which generally reflects an adequate reaction of the mucous membrane of the cervix as a barrier organ. Mononuclear phagocytes, natural killer cells, and T-helper cells, which synthesize various cytokines, are attracted to the focus of chronic inflammation [2]. In all stages of pregnancy, in the presence of persistent infection, bacterial products activate type 1 T helper cells (ThI). ThI cells secrete pro-inflammatory cytokines: il-2, il-6, il-12, il-18, TNF-beta, IFN-gamma, through the synthesis of arachidonic acid, the production of prostaglandins (E2 and F2alpha) is enhanced, the latter contribute to the premature rupture of amniotic fluid , myometrial contraction and termination of pregnancy at any stage of gestation.
Diagnostics. Diagnosis of cervicitis is often difficult due to low symptoms even in the acute stage, which often leads to untimely treatment and the transition of the disease into a long-term chronic process, which can occur with exacerbations and is difficult to treat with medication. In addition to a clinical gynecological examination, it is mandatory to perform colposcopy and take smears for oncocytological and bacterioscopic examination. Additional methods are bacteriological cultures followed by cultural examination, immunoenzyme and immunofluorescence research methods, diagnostics using polymerase chain reaction (PCR) and ligase chain reaction (LCR). During pregnancy, it is imperative to clarify the spectrum of etiological factors causing the development of chronic cervicitis in order to carry out etiotropic therapy in order to prevent complications associated with this pathology.
Colposcopic images of exocervicitis make it possible to distinguish between focal and diffuse variants. In this case, colposcopy can help provide preliminary guidance on the nature of the cervical infection. For example, hypertrophic ectopia of the prismatic epithelium and the picture of follicular cervicitis allow one to suspect a chlamydial infection. Increased development of the vascular network in the superficial layers, iodine-negative zones are often observed during viral infection. Flat condylomas are characterized by the presence of areas of acetowhite epithelium, which become visible after a test with acetic acid. The alternation of “rough” zones with a “varnished” surface, the appearance of vessels in the form of “splashes” and “dots” indicate genital candidiasis.
Based on the clinical and morphological picture of the disease, acute and chronic cervicitis are distinguished. The morphological features of cervicitis are determined by the severity of pathological changes in the epithelial and stromal components of the cervix and the nature of the inflammatory process. Acute cervicitis is mainly observed during infection with gonococci, postpartum infection (streptococci and staphylococci), and viral infection. The early stages of the inflammatory process are characterized by vascular congestion, exudative phenomena, and intense infiltration of neutrophilic granulocytes. In epithelial cells, dystrophic changes are observed with vacuolization of the cytoplasm and cell nuclei. Necrosis causes ulceration (cervical erosion), the presence of purulent or serous-purulent exudate on the surface of the exocervix. The reparative process is accompanied by the development of granulation tissue, the appearance on a surface devoid of epithelium of a layer of cylindrical or immature metaplastic cells, which subsequently, as they proliferate and differentiate, form multilayered squamous epithelium [6].
Chronic endocervicitis occurs due to infection of the endocervix, often as a consequence of vaginitis. In this case, the folds of the mucous membrane of the cervical canal are thickened, swollen, there is lymphoid-histiocytic infiltration with an admixture of plasma cells and neutrophilic granulocytes, full-blooded vessels, increased secretion of mucus with rejected dystrophically altered epithelial cells and inflammatory detritus. It should be noted that there is no connection between the structural and functional characteristics of the epithelium and stroma of the cervix and the etiological factor in chronic cervicitis [9]. Against this background, cervical intraepithelial neoplasia (CIN) and, possibly, cervical cancer most often develop [18].
Treatment. Therapy for exo- and endocervicitis includes the use of antibacterial, antitrichomoniacal, antichlamydial and other agents, depending on microbiological data and special research methods. Therefore, at present, the gold standard for local treatment of cervicitis of mixed etiology is the use of complex drugs with antimycotic, antiprotozoal and antibacterial effects. Such drugs include Terzhinan, Klion-D, Polygynax (vaginal tablets and capsules), Betadine (vaginal suppositories), Macmiror-complex (vaginal suppositories), Tantum rose (douching solution and powders), etc.
In necessary cases (trichomoniasis, chlamydia, ureaplasma infection, candidiasis), local treatment of cervicitis is supplemented by oral administration of drugs.
In the treatment of chlamydial, ureaplasma, and mycoplasma infections, the drug Sumamed® (azithromycin) has proven itself to be excellent. The ability of azithromycin to accumulate predominantly in lysosomes is especially important for the elimination of intracellular pathogens. It has been proven that phagocytes deliver azithromycin to sites of infection, where it is released during the process of phagocytosis. The concentration of azithromycin in foci of infection is significantly higher than in healthy tissues (on average by 24–34%), and correlates with the degree of inflammatory edema. Despite its high concentration in phagocytes, azithromycin does not have a significant effect on their function. Azithromycin remains in bactericidal concentrations at the site of inflammation for 5–7 days after taking the last dose, which made it possible to develop short (3-day) courses of treatment. In addition, the possibility of using this drug during pregnancy expands the indications for its use. According to a Cochrane review, the microbiological cure rate in pregnant women resulting from the use of all antibiotics specified in the guidelines ranges from 90% [20]. The same review concluded that pregnant women tolerate azithromycin better and therefore treatment with azithromycin may be more effective. The studies conducted did not allow us to conclude that microbiological cure during pregnancy guarantees against subsequent illness in newborns or postpartum manifestations of chlamydial infection in women.
As a result of our study of patients with chronic cervicitis, complicated by termination of pregnancy in the first trimester (n = 20), the following data were obtained: infection of the cervix in patients was of the nature of a mono- and mixed infection. In the form of monoinfection, chlamydia was found in 33.3% of women; mycoplasma in 9.3%; ureaplase in 5%. Among the associations of microorganisms, the most common were: chlamydia, mycoplasma - 26.8%; chlamydia, gardnerella - 12.8%; chlamydia, mycoplasma, ureaplasma - 10.2%; chlamydia, ureaplasma - 6.8%. At the same time, in the majority of patients, ectopia was noted on the vaginal portion of the cervix, which in 1/3 of cases had a recurrent nature after a previous history of destructive therapy. When studying the level of pro-inflammatory cytokines, the following data were obtained: IFN-gamma 114.2 ± 53.4 pkg/ml; il-6 3127 ± 103 pkg/ml; il-2 261.7 ± 51.6 pkg/ml. Considering the nature of the identified microflora in the cervical canal, the high level of pro-inflammatory cytokines, for the purpose of preconception preparation and reducing the duration of therapy, treatment was carried out with Sumamed® 500 mg one hour before meals daily for three days. The criteria for the effectiveness of the treatment was the absence of pathogen DNA in the discharge of the cervical canal. After the therapy, the level of pro-inflammatory cytokines in the mucus of the cervical canal was monitored. The level of IFN-gamma in the main group was 3.8 ± 1.9 pkg/ml, which was significantly (p < 0.0001) lower than before treatment; il-6 2106 ± 170 pkg/ml, which is also significantly (p < 0.001) lower than before treatment; the level of il-2 also decreased significantly to 130 ± 38.5 pkg/ml (p < 0.05). Thus, the treatment contributed to the elimination of the pathogen in the presence of chronic cervicitis and a decrease in the level of proinflammatory cytokines without the use of immunomodulatory therapy.
The second direction in the treatment of cervicitis (with chlamydial and viral infections) is the removal of foci of ectopia after preliminary sanitation, which is carried out using chemical and physiosurgical methods (not used during pregnancy). Physiosurgical methods include cryosurgical treatment, laser and electroconization, laser vaporization, and their combination. When carrying out the destruction of a pathologically altered exocervix for the purpose of treatment, it is also necessary to take into account the presence of an inflammatory process. If at the preparatory stage it was not possible to achieve good results in eliminating inflammation, then normal epithelization will not occur on the wound surface after destruction of the cervix for a long time, and this can contribute to the occurrence of complications such as cervical endometriosis, cicatricial changes in the exocervix, strictures of the cervical canal, the appearance of multiple nabothian cysts, exocervicitis, and even their transition to more severe forms of the disease [16, 18].
The third direction in the treatment of cervicitis includes correction of vaginal microbiocenosis (usually carried out after treatment of vaginitis and cervicitis). For chronic chlamydial and viral cervicitis, for the purpose of immunocorrection, a combination of eubiotics is recommended (Hilak-Forte, on tampons, has proven itself better than others) and immunocorrectors (licorice root syrup according to 1 teaspoon orally 3 times + Imudon 2 tablets intravaginally 2 times for 10 days), while optimal changes in local cellular immunity were revealed [6].
The degree of difficulty in choosing an adequate treatment method for cervicitis is due to a number of factors, among which the most important is making the correct etiological diagnosis. Inadequate diagnosis leads to the choice of incorrect treatment, which is overwhelmingly aimed at the destruction of pathologically altered tissues. At the same time, the origin of cervicitis presupposes the choice of pathogenetically substantiated therapy aimed at eliminating the causes of the disease (etiotropic - antimicrobial, anti-inflammatory therapy), the goal of which is to eliminate the inflammatory agent.
Timely and adequate treatment of cervicitis makes it possible to prevent the occurrence of infertility due to infectious pathology of the lower genital tract of a woman, complications associated with pregnancy.
Literature
- Arestova I.M., Zanko S.N., Semenov V.M. Recurrent herpetic infection in reproductive and perinatal pathology. Vitebsk: VSMU, 2003. P. 146.
- Astakhov V. M. State of immunity and psycho-vegetative reactions in women with a history of mixed infection of the genital tract / V. M. Astakhov, V. G. Bylym, V. L. Blednova // Materials of the 4th Ros. forum "Mother and Child". M., 2002. pp. 29–30.
- Belokrinitskaya T. E. Anti-inflammatory cytokines of cervical secretion in cervical epithelial dysplasia / T. E. Belokrinitskaya, Yu. N. Ponomareva, Yu. A. Vitkovsky, M. N. Mochalova, N. M. Ladygina // Materials of the All-Russian Forum “Mother” and a child." M., 2006. P. 331.
- Berlev I.V., Kira I.F. The role of opportunistic microflora in the development of miscarriage in women with vaginal microbiocinosis disorder // Journal of obstetrics and women's diseases. 2002. Issue. 2. T. LI. pp. 33–37.
- Bykovskaya O. V. Immunomodeling therapy for chronic cervicitis caused by urea and mycoplasma infections // Gynecology, 2007, vol. 9. pp. 40–42.
- Vaganova I.G. Apoptosis and proliferation of ectocervix epithelial cells in patients with papillomavirus and chlamydial cervicitis // Questions of Oncology. 2000. T. 46, No. 5. P. 578–582.
- Votrina I. R. An integrated approach to the diagnosis and treatment of cervical pathology in women of reproductive age / I. R. Votrina, A. I. Novikov, E. B. Rudakova, T. I. Dolgikh, G. V. Krivchik, T F. Sokolova, N. G. Gordienko, E. V. Pakhalkova, N. E. Turok // Bulletin of perinatology, obstetrics and gynecology, Omsk. 2004. pp. 167–175.
- Koval E. A. Features of the microbial landscape of the lower parts of the reproductive tract in women with cervical ectopia associated with chronic cervicitis // Materials of the Russian Scientific Forum “Mother and Child”. M., 2005. P. 365.
- Kondrikov N.I. Exo- and endocervicitis: morphological aspects. Polyclinic gynecology. M., 2004. pp. 47–57.
- Kononov A.V. Nomenclature of precancerous lesions of the cervix due to human papillomavirus and chlamydial infections. Omsk 2000. P. 186.
- Kostava M.N. The role of inflammatory processes of the genital organs in the pathology of the cervix. Polyclinic gynecology. M. 2004. pp. 48–53.
- Klinyshkova T.V. Features of the cervico-vaginal ecosystem in cervicitis // Problems of ecology and public health. Omsk 2000. pp. 12–13.
- Kurbanbekova D. S. Features of the management of patients with pathological processes in the cervix associated with chlamydial infection / D. S. Kurbanbekova, D. K. Nazhmutdinova, M. P. Akhmetova // Russian Bulletin of Obstetrics and Gynecology. No. 1. 2003.S. 40–42.
- Manukhin I. B. Vaginal microbiocenosis and pathology of the cervix. Possibilities for correcting dysbiotic conditions / I. B. Manukhin, G. N. Minkina, V. S. Kalinina // Polyclinic gynecology. M., 2004. pp. 38–44.
- Novikov A.I., Kononov A.V., Vaganova I.G. Sexually transmitted infections and exocervix. M., 2002. 200 p.
- Prilepskaya V.N. Diseases of the cervix, vagina and vulva. M. 1999. P. 426.
- Prilepskaya V.N. Diseases of the cervix, vagina and vulva. Polyclinic gynecology / V. N. Prilepskaya, A. E. Golubenko // M., 2004. P. 9–29.
- Prilepskaya V.N. Pathology of the cervix /V. N. Prilepskaya, N. I. Kondrikov, E. V. Gogaeva // Practical gynecology. M., 2006. pp. 16–28.
- Rudakova E. B. Inflammatory diseases of the cervix and infertility /E. B. Rudakova, E. G. Khilkevich, S. A. Mukanova // Genital infections and pathology of the cervix. M., 2004. pp. 152–164.
- May W., Gulmezoglu AM, Ba-Thike K. Antibiotics for incomplete abortion. Cochrane Database of Systematic Reviews 2007, Issue 4. Art. No.: CD001779. DOI: 10.1002/14651858.CD001779.pub2.
Yu. I. Tirskaya*, Candidate of Medical Sciences E. B. Rudakova* , Doctor of Medical Sciences, Professor I. A. Shakina* O. Yu. Tsygankova** * Omsk State Medical Academy, Omsk ** BUZOO "KMHC-MZOO ", Omsk
Key words: chronic cervicitis, squamous metaplasia, pelvic inflammatory diseases, intrauterine infection, miscarriage
Symptoms of cervicitis
There are a number of signs to suspect cervicitis. These include:
- Discharge from the genital tract that is mucous or purulent in nature. The characteristics of the discharge are determined by the cause of cervicitis. So, if the disease is caused by gonococci, the discharge becomes yellowish, if trichomonas, it becomes foamy.
- Periodic pain in the lower abdomen, which can be either dull, pulling or sharp, cutting in nature
- Painful sensations and bloody discharge after sexual intercourse
- Pain when urinating
- Burning and cutting in the external genital area
However, in some cases the clinical picture is blurred, and the woman, as a rule, does not see a doctor. This is very dangerous, because... if left untreated, the inflammatory process begins to spread to surrounding tissues.
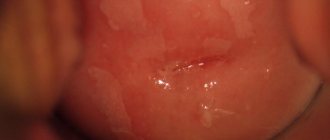
During the examination, pathological changes in the cervix are revealed, which also vary depending on the causative agent of the infection. Thus, trichomonas cervicitis is characterized by the presence of small hemorrhages, gonorrheal cervicitis is characterized by looseness and hyperemia of the cervix with areas of ulceration, candidal cervicitis is characterized by alternating areas with a rough and very smooth (varnished) surface.
Inflammation of the cervix during pregnancy
Cervicitis occurs in two out of three pregnant women at different stages of gestation. The disease is acute, not only the vaginal wall becomes inflamed, but also the labia. Women complain of burning, itching in the perineum, and discomfort. Inflammation of the cervix during pregnancy is one of the factors of miscarriage, so it is necessary to consult a doctor as soon as possible.
Cervicitis in this case is chronic. A woman may not be aware of inflammation until pregnancy, when the pathology manifests itself against the background of natural immunodeficiency.
Atrophic cervicitis
In addition to infection by various types of microorganisms and injury to the cervix, atrophic cervicitis can be caused by prolapse of the vagina and cervix, a decrease in estrogen levels during menopause, and the use of certain contraceptives, which, for example, include chemical spermicides. As a rule, atrophic cervicitis develops as a result of a long (chronic) course of the pathological process. The mucous membrane of the cervix becomes thinner and ulcers form on it.
Treatment at the IPF Clinic
First of all, it is necessary to eliminate the infection and associated diseases. Treatment of chronic cervicitis can sometimes take a very long time.
To treat cervicitis, antifungal, antibacterial, and antiviral agents are used. These are broad-spectrum medications. Sometimes medications are prescribed that boost immunity and restore intestinal microflora. Local remedies are also used, mainly creams and suppositories.
Local treatment may also involve the use of dimethyl sulfoxide 3%, which is used to treat the cervix; solutions of chlorophyllipt and silver nitrate are often used.
The chronic form is not very effective in treating conservatively. Surgical methods are often used. This:
- Cryodestruction
- Diathermocoagulation
- Laser therapy
The treatment process must be constantly monitored using a colposcope and various tests.
If the infection that caused the disease is sexual, it is necessary that the partner also undergo treatment.
Is it possible to cure chronic cervicitis? Yes, if you go to a good hospital that specializes in cervical problems. You can defeat the disease in Kyiv at the IPF clinic. Here they will help you get rid of acute and chronic forms. Highly qualified doctors will select a treatment method that is suitable for the patient. Specialists will offer not only conservative methods, but also modern methods of surgical interventions on the cervix. And affordable prices will please any woman.
Diagnosis of cervicitis
Diagnosis of cervicitis involves:
- examination of the patient by an obstetrician-gynecologist in the speculum, which allows identifying pathological changes in the visible part of the cervix
- conducting an extended colposcopy - examination of the cervix under significant magnification, allowing a detailed examination of the affected areas, determining the nature of the changes, including through special tests
- Ultrasound of the pelvic organs
- obtaining laboratory test results that allow identifying the type of pathogen, selecting the most effective drug for treatment, and identifying changes at the cellular level.
Classification
Of primary importance in the classification of chronic cervicitis is the division of the disease according to the main causative factor. In accordance with this, they distinguish:
- Specific infectious chronic cervicitis. Caused by chronic infection of the cervix with causative agents of chlamydia, gonorrhea, viruses and other pathogens, which are characterized by a unique clinical picture.
- Nonspecific infectious chronic cervicitis. The development of the disease in this case is caused by nonspecific pyogenic cocci and intestinal flora. These pathogens do not have specific features; the clinical picture may vary.
- Non-infectious chronic cervicitis. Microbes are not involved in the occurrence of this form; it is caused by foreign bodies and allergic reactions.
Classification according to the nature of the cervical lesion is of secondary importance. It can be diffuse, when pathological changes affect almost the entire surface of the cervix, and focal, when there are several affected areas and they are “scattered” over the surface of the organ.
Also in the context of classification, concepts such as exocervicitis, endocervicitis and cervicitis may appear. These terms characterize the localization of the pathological process on the cervix. With exocervicitis, the outer part of the cervix is affected, with endocervicitis - the inner part. In both cases, the nature of the lesion is superficial. When they talk about cervicitis, they mean deep damage down to the muscle layer.
If you are diagnosed with chronic cervicitis, you need to be examined by a gynecologist every six months. Photo: imagepointfr / Depositphotos
Treatment of cervicitis
Treatment of cervicitis depends on the reasons that caused it and on the duration of the inflammatory process. Taking antibacterial, antiviral, and antifungal drugs may be indicated. In addition, immunostimulants and vitamin complexes can be prescribed. Vaginal dysbiosis requires restoration of normal microflora. If the basis of cervicitis is a hormonal imbalance, the doctor may recommend replacement therapy. Chronic cervicitis is much less treatable. In some cases, surgical treatment (laser therapy, diathermocoagulation, etc.) may be used.
Why is cervical inflammation dangerous?
Self-medication risks complications, so only a doctor should decide how to treat a woman. If the patient does not seek help in a timely manner, acute cervicitis becomes chronic. A woman faces consequences such as erosion, miscarriage, and spread of the inflammatory process to the appendages. The risk of developing cancer increases. Chronic cervicitis leads to the formation of adhesions and infertility. Patients often experience chronic pelvic pain, menstrual irregularities and other manifestations that reduce quality of life.
Cervicitis and pregnancy
Of course, it is best to undergo a course of treatment for cervicitis at the stage of preparation for pregnancy. The fact is that cervicitis, diagnosed already in the gestational period, poses a danger to the health and life of the unborn child. The pathogen can ascend into the amniotic fluid and cause infection of the fetus. In the early stages, when the formation of organs and body systems occurs, infection can cause developmental defects. If the fetus is infected at a later stage, developmental delays may occur.
Cervicitis can cause isthmic-cervical insufficiency (ICI), which threatens termination of pregnancy in the 2nd and 3rd trimester. Also, with cervicitis, the risk of premature birth and the birth of a child with low body weight is increased.
Women diagnosed with cervicitis are more likely to develop complications in the postpartum period. Treatment of cervicitis during pregnancy is prescribed by an obstetrician-gynecologist based on the results of the examination, taking into account concomitant pathologies. Monitoring the condition of the expectant mother and baby should be carried out by a qualified obstetrician-gynecologist with extensive experience in managing complicated pregnancies.
If you have any questions related to cervicitis, you can ask them to the doctors at Nova Clinic. You can make an appointment with a gynecologist-reproductologist or obstetrician-gynecologist by calling the phone number listed on the website or using the booking button.
Sources
- Iqbal U, Wills C. Cervicitis. 2021 Jul 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID: 32965864.
- Gynecology: textbook for medical universities / E. K. Ailamazyan. - St. Petersburg. : SpetsLit, 2013. - 2nd ed., revised. and additional — 415 p. : ill.
- Guide to outpatient care in obstetrics and gynecology / Academician. RAMS V.I. Kulakov, prof. V.N. Prilepskaya, prof. V.E. Radzinsky
- Savelyeva I.V., Polyanskaya I.B., Galyanskaya E.G., Shevlyagina L.S., Shirokova O.V., Gimp M.V., Florov A.Yu., Nikerina N.I. On the issue of improving treatment outcomes for chronic cervicitis // MS. 2021. No. 13.
- Atabieva D.A., Chilova R.A., Gadaeva I.V., Pikuza T.V., Odnokopytny A.V. Treatment of chronic cervicitis in pregnant women // Volgograd Medical Scientific Journal. 2015. No. 1 (45).
- Unanyan Al, Sidorova I. S., Arakelov S. E., Polonskaya L. S., Kossovich Yu. M., Kadyrova A. E., Baburin D. V. Chronic cervicitis and chronic endometritis: general aspects of pathogenesis and pathogenetic therapy // MS. 2013. No. 4-2.
- Serdyukov S.V., Novikov E.I., Glukhovets B.I., Kravchenko P.B. The significance of chronic cervicitis in the termination of pregnancy in the 1st trimester // Zh. obstetrics. and wives disease.. 2009. No. 5.
- Mattson SK, Polk JP, Nyirjesy P. Chronic Cervicitis: Presenting Features and Response to Therapy. J Low Genit Tract Dis. 2016 Jul;20(3):e30-3. doi: 10.1097/LGT.0000000000000225. PMID: 27243142.
Disease prevention
Cervicitis is treatable. You can completely get rid of it if you use the right tactics and follow your doctor’s advice. If you do not start the disease in an acute form, but immediately take specific therapeutic measures, the disease can be defeated at the initial stage.
Prevention of the disease involves following the rules of personal hygiene, having one partner who is healthy and regularly undergoes examination. It is also important to remember to use a condom in case of casual sex, eat right, have a healthy lifestyle and regularly see a doctor. It is also important to remember that a woman must have healthy intestinal microflora and good immunity, which must be strengthened. It’s also a good idea to get tested for serious diseases (syphilis, hepatitis) at least once a year. All these measures will help avoid this unpleasant disease.