Even with a varied diet, a person, unfortunately, does not receive the norm of vitamins and microelements. This is especially felt in regions with a sharp and cold climate and food seasonality. For example, in our region, only 3 months a year we can eat clean, fresh vegetables and berries. The sun also doesn’t spoil us all year round, like in the south, for example. Therefore, a lack of vitamin D, poor absorption of calcium, and a lack of omega-3 and 6 are the costs of living in the northern and northeastern parts of Russia, for example, in the Irkutsk region. Taking vitamins becomes a necessity.
Today we’ll talk about magnesium - the main building block for a strong nervous system, the deficiency of which is becoming very common. Which drug is better, what is their feature, how to take magnesium correctly and when a positive effect is achieved.
Compound
Magne B6 tablets contain magnesium lactate dihydrate at a concentration of 470 mg/tablet. (equivalent to 48 grams of Mg++), vitamin B6 (pyridoxine hydrochloride) content - 5 mg.
Heavy kaolin, carboxypolymethylene, sucrose, magnesium in the form of hydrosilicate (talc) and stearate, and acacia gum are used as auxiliary components.
Tablet shell composition: acacia gum, sucrose, titanium dioxide, trace amounts of magnesium hydrosilicate and carnauba wax in powder form.
The oral solution contains 186 mg of magnesium lactate dihydrate and 936 mg of magnesium pidolate (which corresponds to a total Mg++ content of 100 mg), 10 mg of pyridoxine hydrochloride.
Auxiliary components: sodium disulfite and saccharinate, cherry and caramel flavoring, purified water.
Composition of Magnesium B6 Forte (Antistress) tablet: 618.43 mg magnesium citrate, 10 mg pyridoxine hydrochloride, anhydrous lactose, magnesium stearate and hydrosilicate, macrogol 6000, hypromellose, titanium dioxide.
Release form
Pharmacological forms of the drug:
- biconvex oval tablets in a white film shell with a shiny smooth surface (10 pieces in aluminum foil and PVC blisters, 5 blisters per package);
- a transparent, brown solution for oral use with a distinct caramel odor (in 10 ml ampoules, 10 ampoules in a cardboard packaging insert);
- white oval biconvex film-coated tablets (15 pieces in blisters made of aluminum foil and PVC-PE-PVDC, 2 or 4 blisters per package).
Pharmacodynamics and pharmacokinetics
Magnesium (Mg) is an important biogenic element, which is present in significant quantities in all tissues of the body, is a cofactor in most metabolic processes and ensures the normal functioning of cells.
In particular, this element is necessary for the biotransformation of creatine phosphate into ATP - nucleoside triphosphate, which plays the role of a universal energy supplier in living cells of the body.
protein cannot be synthesized normally . The element takes part in muscle contraction (including maintaining the normal function of the heart muscle ), regulates the transmission of impulses in nerve fibers , promotes vasodilation , stimulates the secretion of bile , increases the motor activity of the intestinal tract , which in turn helps remove cholesterol from the body.
Magnesium enters the body with food. Its deficiency can be primary (due to hereditary pathologies) or secondary. Secondary magnesium deficiency is usually associated with:
- with a nutritional disorder (diet poor in vitamins and minerals, exclusively parenteral nutrition, chronic alcoholism);
- with an increase in a person’s need for a microelement during intense physical or mental activity, during periods of intense growth, during pregnancy, during stress, excessive losses of Mg through the kidneys (for example, with chronic pyelonephritis , abuse of diuretics , treatment with cisplatin );
- with impaired absorption of Mg in the gastrointestinal tract due to hypoparathyroidism , chronic diarrhea , etc.
Vitamin B6 (pyridoxine) improves metabolic processes, including in brain tissue. As a result, brain performance increases, mood and memory improve.
In addition, the presence of pyridoxine in the composition of Magne B 6 improves the absorption of Mg from the digestive tract and its distribution in the cells of the body.
If the serum concentration of Mg is in the range from 12 to 17 mg/l, they speak of moderate Mg deficiency. An indicator not exceeding 12 mg/l is evidence of severe microelement deficiency.
No more than half of the Mg dose taken orally is absorbed in the digestive tract 99% of the microelement is located in the intracellular space, while about 66% of intracellular Mg is distributed in bone tissue , the remaining amount is in striated and smooth muscles .
Mg is excreted mainly in the urine (about a third of the dose taken).
pharmachologic effect
Magnesium is an element of vital importance. It must be regularly supplied to the body. The substance takes part in most physiological and biochemical processes, for example:
- muscle contraction processes;
- protein synthesis;
- transport of substances across cell membranes;
- impulse transmission between neurons;
- inhibition of excitation processes in the central nervous system;
- reducing the body's sensitivity to environmental influences and many others.
Magnesium comes from food, but in case of deficiency there can be an imbalance and corresponding consequences.
Vitamin B6 also takes part in a number of vital processes:
- absorption of magnesium by the body;
- activation of protein synthesis;
- transmission of nerve impulses;
- participation in carbohydrate metabolism and others.
The active ingredients of the drug are absorbed in the intestines and enter the bloodstream. They are excreted mainly in urine.
Contraindications
Contraindications to the use of Magne b6 are:
- severe renal failure (conditions in which creatinine does not exceed 30 ml per minute);
- impaired absorption of glucose and galactose , fructose intolerance, sucrose-isomaltase deficiency (only for the tablet form of the drug);
- simultaneous use of the antiparkinsonian drug levodopa ;
- phenylketonuria;
- hypersensitivity to the substances contained in the tablets/solution.
In pediatrics, tablet forms of the drug are prescribed from the age of six; the solution in ampoules is allowed from the age of one.
Due to the risk of developing hypermagnesemia , the drug should be prescribed with caution to persons with moderate renal failure .
Indications and contraindications
The drug is indicated for use in cases of diagnosed deficiency of magnesium and vitamin B6. Deficiency can manifest itself with the following symptoms:
- increased heart rate;
- general weakness and fatigue;
- muscle spasms, pain;
- tingling;
- sleep problems (not too pronounced);
- irritability;
- spasms of the stomach and/or intestines.
In some cases, medication is excluded:
- individual sensitivity to any component;
- severe renal failure;
- children up to 5 years old inclusive;
- fructose carbohydrate intolerance;
- malabsorption of galactose, glucose;
- combination with levodopa.
The tablets can be taken with caution in the presence of kidney failure (moderate stage). The medicine can be used during pregnancy, but should not be taken during breastfeeding.
Instructions for Magne B6 (Method and dosage)
Before taking Magne B6, you should consult your doctor. The average course duration is one month. Treatment is stopped immediately after the Mg concentration in the blood is normalized.
The medicine is taken with meals 2 or 3 times a day.
If the drug is prescribed during pregnancy, the dose is selected individually by the attending physician.
Magne B6 tablets: instructions for use
Magne b6 tablets are taken 6-8 pieces per day.
According to the instructions for use for children, the daily dose for patients over 6 years of age (provided that their body weight exceeds 20 kg) is 4 to 6 tablets.
Instructions for Magne B6 in ampoules
Adults are prescribed the solution to take 3-4 ampoules of 10 ml per day. Before administration, the drug is dissolved in 0.5 glasses of drinking water.
For children over 12 months (if their body weight exceeds 10 kg), Magne B6 in ampoules is prescribed to take 10-30 mg of Mg per kilogram of weight (the indicated dose is contained in 1-4 ampoules of the drug).
Instructions for Magne B6 Premium
The tablets are taken with meals. Swallow them whole with a glass of drinking water.
For an adult, the daily dose of Magne B 6 is 3-4 tablets. Children over six years of age (if their weight exceeds 20 kg) should be given 10 to 30 mg/kg/day. (or 2-4 tablets).
Overdose
In patients with normally functioning kidneys, an overdose of magnesium taken orally does not usually cause toxic reactions. In case of kidney failure, excess magnesium can cause poisoning, the symptoms of which are:
- nausea;
- vomit;
- ECG changes;
- decrease in blood pressure;
- hyporeflexia;
- CNS depression;
- disturbances of cardiorespiratory function (up to coma, respiratory paralysis and cardiac arrest);
- anuric syndrome.
The severity of overdose symptoms depends on the concentration of the trace element in the blood.
Treatment involves forced diuresis and rehydration therapy . For renal failure, peritoneal dialysis and hemodialysis are indicated .
Interaction
Due to the fact that pyridoxine (in any quantities) inhibits the activity of levodopa , it is contraindicated to prescribe this drug in combination with Magne B6. This applies to situations when taking levodopa is not combined with taking drugs that suppress the activity of peripheral decarboxylase of aromatic amino acids existing in the L-form.
It is not recommended to take Magne B6 with drugs that contain Ca salts or phosphates (these drugs impair the absorption of Mg in the intestinal tract).
Since Mg preparations reduce the absorption of tetracyclines , at least a three-hour interval should be maintained between their doses.
special instructions
Ampoules with Magne B6 solution are self-breaking (each has 2 marking rings and a break line) and does not require the use of a nail file.
To open the ampoule, take it by the tip, having previously covered it with a piece of fabric, and with a sharp movement break it off first from the pointed end, then from the opposite. The end opened first is directed at an angle into a cup of water so that the tip of the ampoule, which is broken off second, is not above the cup.
After the second tip of the ampoule is broken off, the solution will flow freely into the glass.
Patients with diabetes need to remember that film-coated tablets contain sucrose as an excipient. Therefore, the dosage form that is more preferable for them is a solution that does not contain sugar.
In case of malabsorption syndrome (impaired absorption) and severe magnesium deficiency, treatment should begin with intravenous administration of Mg preparations.
If a patient has a concomitant calcium deficiency, the Mg deficiency is corrected before taking dietary supplements or medications that contain Ca.
The solution contains sulfite, a substance that can cause or intensify hypersensitivity reactions, including anaphylactic reactions (especially in patients at risk).
Taking high (exceeding 200 mg/day) doses of pyridoxine for several months/years can cause the development of sensory axonal polyneuropathy , which is manifested by symptoms such as tremor, numbness and disorders of proprioceptive sensitivity of the distal arms and legs, gradually manifesting sensory ataxia ( imbalance).
Disorders of this kind are usually reversible and disappear after stopping taking vitamins.
Magne B6 oral solution in ampoules 10ml No. 10
Magne B6 solution.
Release forms
Solution.
INN
Magnesium lactate + magnesium pidolate + pyridoxine hydrochloride.
FTG
Magnesium preparation.
Description
Transparent brown liquid with a caramel odor.
Compound
One ampoule (10 ml) contains: Active substances: magnesium lactate dihydrate – 186 mg, magnesium pidolate – 936 mg (total magnesium content (Mg2+) is 100 mg (4.11 mmol)), pyridoxine hydrochloride – 10 mg. Excipients: sodium disulfite (E223), sodium saccharinate (E954), cherry-caramel flavor, purified water. Composition of cherry-caramel flavoring: alcoholates and alcohol tinctures of raspberry, orange, cocoa, black currant, extracts of coffee, Tonka beans, hemanthus and fenugreek, vanillin, ethylvanillin, maltol (E 636), piperonal, oxyphenylone, acetylmethylcarbinol, diacetyl, isoamyl acetate, gamma-nonalactone, ionones, methylisoeugenol, benzoic aldehyde, caramel (E 150), propylene glycol (E 1520). Pharmacotherapeutic group Mineral supplements. Magnesium-based products. ATX code: A12CC.
Pharmacological properties
Pharmacodynamics Physiological aspects: Magnesium is predominantly an intracellular cation. It reduces the excitability of neurons and neuromuscular transmission of excitation, and takes part in many enzymatic processes. Magnesium is an essential element of organs and tissues: bone tissue contains half of the total amount of magnesium contained in the human body. Clinical aspects: Serum magnesium levels: - between 12 and 17 mg/L (1-1.4 mEq/L or 0.5-0.7 mmol/L): indicate mild magnesium deficiency - below 12 mg/L ( 1 mEq/L or 0.5 mmol/L): indicates severe magnesium deficiency. Deficiency can be: - primary, due to a congenital abnormality of magnesium metabolism, - secondary, due to • inadequate intake (severe malnutrition, alcoholism, total parenteral nutrition), • gastrointestinal absorption disorders (chronic diarrhea, gastrointestinal fistula, hypoparathyroidism), • excessive losses at the renal level (tubular disease, significant polyuria, diuretic abuse, chronic pyelonephritis, primary hyperaldosteronism, treatment with cisplatin). Pyridoxine (vitamin B6) is involved in many metabolic processes in the body and in the regulation of nervous system metabolism. The biological properties of pyridoxine are provided by pyridoxal-5-phosphate, which is formed in the body with the participation of the enzyme pyridoxal kinase. Vitamin B6 improves the absorption of magnesium from the gastrointestinal tract and its penetration into cells, which determines the effectiveness of the combination of these substances. Pharmacokinetics Gastrointestinal absorption of magnesium salts occurs partly through a passive mechanism in which the solubility of the salt plays a determining role. The degree of this absorption does not exceed 50%. Excretion occurs primarily through urine.
Indications for use
This medicine contains magnesium and is used to correct a deficiency of this element in the body. A combination of a certain number of the following symptoms may indicate a magnesium deficiency: - Nervousness, irritability, mild anxiety, transient fatigue, mild sleep disturbances, - Signs of anxiety such as gastrointestinal cramps or rapid heartbeat (if the heart is healthy), - Muscle cramps, tingling sensation Prescribing magnesium may help relieve these symptoms. If no improvement is observed after one month of treatment, continuation of monotherapy with this drug is not advisable.
Contraindications
The use of the drug is contraindicated in the following cases: - hypersensitivity to one of the components - severe renal failure with creatinine clearance less than 30 ml/minute - co-administration with levodopa.
Precautionary measures
In case of concomitant calcium deficiency, the magnesium deficiency must be corrected before the calcium deficiency is corrected, i.e. before starting to take calcium supplements. In cases of severe magnesium deficiency and malabsorption, the intravenous route of drug administration should be chosen for treatment. This drug is indicated for oral administration. IT CANNOT BE INJECTED! In moderate renal impairment, caution should be exercised to avoid the risk associated with hypermagnesemia. Due to the presence of sucrose, the drug is contraindicated in cases of fructose intolerance, impaired absorption of glucose or galactose, or sucrase-isomaltase deficiency. Use with caution for gastric and duodenal ulcers and coronary heart disease. In case of severe liver damage, pyridoxine in high doses can cause deterioration of liver function. When pyridoxine is used in high doses (> 200 mg/day) for a long time (several months or in some cases years), sensory neuropathy may develop, which is accompanied by symptoms such as numbness and vestibular disturbances, tremors of the distal extremities and gradually developing sensory ataxia (impaired coordination of movements). These disorders are usually reversible and disappear after discontinuation of high doses of vitamin B6. The ampoules contain sulfite, which may cause or worsen allergic-type reactions, including anaphylactic reactions, in patients at risk. Interaction with other medicinal products and other forms of interaction You must systematically inform your doctor about all the medications you are taking. Magnesium, not recommended combinations ■ Phosphorus or calcium salts These drugs inhibit the absorption of magnesium from the intestines. Combinations to consider ■ Oral tetracyclines An interval of at least 3 hours should be maintained between oral tetracyclines and magnesium due to reduced absorption of tetracyclines in the gastrointestinal tract. ■ Oral thrombolytic agents Magnesium weakens their effect. Magnesium reduces iron absorption. Vitamin B6, not recommended combinations ■ Levodopa When used simultaneously with levodopa, the effects of levodopa are reduced or completely inhibited. Vitamin B6, combinations that should be taken into account ■ Hormonal contraceptives When used simultaneously with hormonal contraceptives, the concentration of pyridoxine in the blood plasma may increase. ■ Diuretics When used simultaneously, the effect of diuretics is potentiated. ■ Isonicotin hydrazide, penicillamine, cycloserine When used simultaneously with isonicotin hydrazide, penicillamine, cycloserine, the effectiveness of pyridoxine may be reduced. ■ Phenytoin, phenobarbital When used simultaneously with phenytoin, phenobarbital, a decrease in the concentrations of phenytoin and phenobarbital in the blood plasma is possible.
Pregnancy and breastfeeding
Pregnancy This medicine, if necessary, can be used at any stage of pregnancy. If, during treatment with the drug, you discover that you are pregnant, consult your doctor, who will decide whether you need to continue treatment. Breastfeeding period The use of magnesium and vitamin B6 contained in the drug is considered compatible with the lactation period. Data on this issue are limited by the maximum daily dose of vitamin B6. The recommended dose of vitamin B6 during breastfeeding is no more than 20 mg per day.
Impact on the ability to drive vehicles or other machinery
There are no special recommendations.
Directions for use and doses
This drug is indicated for oral administration. IT CANNOT BE INJECTED! The contents of the ampoules should be diluted in half a glass of water. Adults: 3-4 ampoules per day, divided into 2-3 doses with meals. Children weighing over 10 kg (about 1 year of age and older): 10-30 mg/kg/day (0.4-1.2 mmol/kg/day), that is, 1-4 ampoules per day, divided into 2 -3 doses during meals. If you forget to take Magne B6, do not take a double dose to make up for the missed dose! Treatment should be stopped after normalization of magnesium levels in the blood. ATTENTION: THE AMPOULES ARE SELF-PRESSING, DO NOT REQUIRE THE USE OF A NAILFISH! To open the ampoule, take it by the tip (you can first cover it with a piece of cloth) and break off the tip with a sharp movement. Follow the instructions shown in the picture!
Overdose
Oral overdose of magnesium usually does not cause toxic reactions if the kidneys are functioning normally. However, magnesium poisoning can develop in cases of kidney failure. Toxic effects depend on the level of magnesium in the blood, and their symptoms are as follows: - drop in blood pressure, - nausea, vomiting, - central nervous system depression, impaired reflexes, - ECG changes, - respiratory depression, coma, cardiac arrest and respiratory paralysis, - anuric syndrome . When taking a large dose, there is a risk of anuric syndrome. Treatment: rehydration, forced diuresis. In case of renal failure, hemodialysis or peritoneal dialysis is necessary.
Side effects
Like all medicines, this drug may cause varying degrees of side effects in some people. - diarrhea - abdominal pain - skin reactions - allergic reactions Due to the presence of sodium disulfite (E 223) in this form of the drug (oral solution), there is a risk of allergic reactions, including anaphylactic reactions, and bronchospasm. Reporting Adverse Reactions If you experience any adverse reactions, consult your doctor. This recommendation applies to any possible adverse reactions, including those not listed in the package insert. You can also report adverse reactions to the Adverse Drug Events Information Database, including reports of drug failure. By reporting side effects, you can help provide more information about the safety of the drug.
Storage conditions
Store in a place protected from light at a temperature not exceeding 25 °C. Keep out of the reach of children.
Best before date
3 years. Do not take after the expiration date stated on the package.
Conditions for dispensing from pharmacies
Available without a prescription.
Package
10 ampoules of yellow glass type III, 10 ml capacity, with two or one break line at each of the two ends of the ampoule, along with instructions for use, in a cardboard box.
Buy Magne B6 solution for oral administration in amp. 10 ml in pack No. 10 in the pharmacy
Price for Magne B6 solution for oral administration in amp. 10 ml in pack No. 10
Instructions for use for Magne B6 solution for oral administration in amp. 10 ml in pack No. 10
Analogues of Magne B6
Level 4 ATX code matches:
Magwit
Magne B6 Forte
Vitrum Life
Analogs of Magne B6 are the drugs Magnesium B6 Evalar , Magnelis B6 , Magnikum , Magnistad , Magnefar B6 , Magvit B6 , Beresh Magnesium plus B6 .
The price of analogue tablets is from 150 Russian rubles.
Which is better: Magnelis or Magne B6?
The drug Magnelis B6 is produced by Pharmstandard and, like its analogue Magne B6, is intended to replenish Mg deficiency in the body. The products have a similar composition (Magnelis contains 470 mg Mg lactate and 5 mg pyridoxine , Magna B6 contains 470 mg Mg lactate dihydrate and 5 mg pyridoxine ), the same indications for use and contraindications, and cause similar side effects.
The main differences are the manufacturer and price.
Magne B6 and Magnelis B6 comparison
Let's try to answer the question of what is better Magne B6 or Magnelis B6
As can be seen from the table, both drugs have the same indications, the same recommendations for side effects and, judging by consumer reviews, are generally equally well tolerated if all conditions of administration are met.
But some indicators, as well as the composition of the drugs, are different. The form of the active substance, magnesium, and the excipients differ. The form of magnesium in Magna B6 is lactate dihydrate, in Magnelis it is lactate.
Magnesium lactate is a magnesium salt of natural lactic acid. A dihydrate is a form of a substance (i.e. magnesium lactate) that contains two water molecules attached. Thus, the dihydrate provides the greatest bioavailability and better absorption. In fact, this form allows the molecules of the active substance to separate faster and more easily, attach to transporter substances, reach their destination intact and be absorbed there. But even this fact does not deprive the related drug Magnelis B6 of its beneficial properties and effectiveness.
Moreover, in the line of Magnelis products there is a drug Magnelis Express Calm, which in addition to magnesium contains extracts of hops, valerian, passionflower and folic acid. It has a more pronounced calming effect and helps regulate sleep and wakefulness. In turn, Magne B6 has a solution form that can be given to children from 1 year of age in the presence of hypertension, increased excitability and nervous tension during the adaptation period. Magnelis is acceptable for use by children over 6 years of age. However, before using magnesium in children, you should consult a specialist.
Both drugs in tablet form should be used with caution if you have diabetes, since the tablet shells contain sugar.
When are magnesium supplements prescribed?
- when restoring the nervous system, in the event of any, even seemingly minor, disorders, ranging from mild irritability to severe forms of vegetative-vascular dystonia and cardioneurosis.
- to normalize blood pressure in hypertension.
- to eliminate heart pain and heart rhythm disturbances. If the cause of heart ailments lies not in a functional disorder, but in a serious heart disease, then the supplement is prescribed in combination with other medications.
- for the treatment of muscle cramps, including in children
- with poor and imaginative nutrition, diets, increased physical activity.
Benefits of magnesium
- Helps absorb calcium, activates vitamin D in the kidneys, which is necessary for the health of the skeletal system.
- Metabolizes carbohydrates and glucose, therefore reduces the risk of type 2 diabetes.
- Reduces fat deposits on artery walls, reduces the risk of coronary artery calcification.
- Magnesium therapy reduces the likelihood of developing migraines.
- Reduces premenstrual symptoms.
- Promotes weight loss due to its influence on hormonal levels and its participation in the synthesis of female hormones.
- The presence of magnesium in the body can change the types of bacteria present in the intestines.
Magne B6 for children
Magnesium is very important for children because it participates in various biochemical reactions of the body, improves the absorption of calcium and the tone of the walls of blood vessels, and normalizes the conduction of nerve impulses in the brain.
Magnesium deficiency is very closely related to stress. Experts consider Mg deficiency and stress to be interdependent processes that can aggravate each other.
Both acute and chronic stress lead to depletion of the intracellular Mg pool and its loss in the urine. This is due to the fact that in a stressful situation the body releases more adrenaline and norepinephrine , which contribute to the elimination of Mg from cells.
Magnesium deficiency often leads to a decrease in the ability to concentrate, memory impairment, convulsive seizures , impairment of consciousness and the coordination sphere (usually this manifests itself in the form of nystagmus, ataxia, tremor ). Some children develop paresthesias and increased tendon reflexes .
In children of all ages, Mg deficiency (as well as stress) provokes an increase in blood pressure - one of the significant components of stress and changes the cerebroreactive reactivity of blood vessels towards a constrictor response.
Biochemical and clinical-neuropsychological studies, as well as reviews of Magne B6 for children, confirm that taking Mg drugs can curb the rise in blood pressure, increase stress resistance, improve behavior, memory and attention, normalize sleep, reduce anxiety, the level of synkinesis and aggression.
In accordance with the instructions, in pediatric practice the solution is prescribed from the age of one year, tablets - after 6 years, however, in the presence of neurological disorders, Magne B6 can be used from the first days of life. The dosage for an infant is calculated depending on his body weight.
It is very important that the composition of the drug (both in the form of a solution and in the form of tablets) includes organic Mg salts - lactate, citrate and pidolate - which are characterized by high bioavailability and practically do not cause side effects.
Magne B6 Forte, which is based on Mg citrate, is recommended for use in children with oxalaturia and acidosis , as well as in children with a shift towards acidosis : the drug is used to compensate for rapid nervous and mental exhaustion in patients with a neuroarthritic type of constitution and for the prevention of urolithiasis .
Use of magnesium in obstetrics
Magnesium is one of the vital microelements, the fourth most abundant cation in the body and is found mainly in bone, muscle and nerve tissues. Less than 1% of the total magnesium in the body is found in plasma and red blood cells. About 60% of magnesium contained in plasma is in an ionized state, and the rest is associated with albumin or complexed with ions - mainly citrate and phosphate [15].
Magnesium is involved in the regulation of metabolic processes in the body: in energy (complexation with ATP and activation of ATPases, oxidative phosphorylation, glycolysis), plastic (synthesis of protein, lipids, nucleic acids) and electrolyte metabolism. In addition, it is a cofactor for many enzymes, acts as a calcium antagonist, and takes part in the relaxation of muscle fibers other than the heart muscle. Magnesium also reduces platelet aggregation ability, maintains normal transmembrane potential in electrically excitable tissues, and affects the endothelium, which plays a key role in vascular homeostasis, in particular, through the production of nitric oxide and participation in the control of platelet aggregation. It has been proven that magnesium ion deficiency increases the activity of thromboxane A2, which is accompanied by damage to the vascular wall. The protective effect of magnesium on neurons is manifested by inhibition of calcium channels and antagonism with the N-methyl-D-aspartic acid receptor [15].
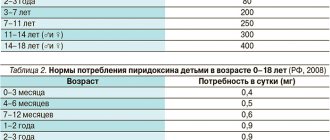
Numerous units of measurement of magnesium dose are used in foreign literature (table). The daily requirement for magnesium is 350 mg for men and 280 mg for women and increases during pregnancy and lactation by at least one and a half times (360–400 mg/day).
During breastfeeding, for the normal development of the growing body of a newborn, the concentration of magnesium in breast milk should be 30–40 mg/l [15]. The richest magnesium crops are grains, legumes, greens, nuts, and chocolate. The absorption of magnesium from food products is 30–35%.
Regulation of magnesium levels depends on renal excretion. Excess plasma calcium and magnesium activates the calcium receptor in the kidneys and thereby increases diuresis to remove excess of both ions. Thus, magnesium leads to an increase in its own clearance with normal renal function.
The generally accepted plasma magnesium level is 0.75–1.0 mmol/L. However, magnesium is an intracellular ion, so its deficiency in the body can be present even with normal and elevated plasma magnesium levels [15].
It was found that magnesium levels decrease during pregnancy, reaching a minimum value at the end of the first trimester, partly due to dilution and release into the extracellular space and partly due to absolute magnesium deficiency. Magnesium deficiency has numerous consequences, including chronic fatigue, delirium, weakness and seizures, impaired glucose metabolism, a variety of arrhythmias, vascular disorders and disturbances of electrolyte metabolism, especially potassium. The immediate manifestations of magnesium deficiency most often include a rapidly developing lack of magnesium in the body, which leads to a state of increased nervous excitability of the cell. Clinically, it manifests itself as muscle twitching and cramps, most often in the calf muscles, which is a common problem during pregnancy. Arrhythmia in pregnant women is also often associated with magnesium deficiency. Magnesium deficiency during pregnancy increases the risk of insulin resistance and diabetes. Magnesium deficiency during pregnancy can lead to the development of placental insufficiency, preeclampsia due to spasm of the uterine arteries, and fetal growth restriction syndrome [15]. Magnesium also has a significant effect on the condition of connective tissue. During pregnancy, prolonged magnesium deficiency can provoke the development of stretch marks in the chest and abdomen in a woman during a period of rapid breast growth and an enlarged uterus. Childbirth in women with magnesium deficiency is more often complicated by perineal ruptures [5, 8].
In obstetrics, magnesium is used for two main purposes - as a tocolytic in the form of magnesium sulfate (or magnesium chloride in solutions for IM and IV infusions) and as replacement therapy for nutritional support and balanced diet. A rational, balanced diet is an essential basis for bearing a healthy fetus and giving birth to a healthy child.
In the absence of diseases of the gastrointestinal tract, eubiosis of the intestinal flora and the absence of genome polymorphisms associated with severe disorders of magnesium metabolism, the daily requirement for magnesium can be met with a balanced diet. The required amount is calculated based on the following indicator: 5 mg/kg/day. Some people need more magnesium due to significant losses. Children require 5 to 10 mg/kg/day; pregnant women (or nursing mothers) - 10–15 mg/kg/day; women with established magnesium deficiency also require 10–15 mg/kg/day. To select a diet, you should take into account the quantitative content of magnesium in food and its bioavailability. Thus, fresh vegetables, fruits, herbs (parsley, dill, green onions, etc.), and new crop nuts have the maximum concentration and activity of magnesium.
When preparing products for storage (drying, drying, canning, etc.), the concentration of magnesium decreases slightly, but its bioavailability drops sharply. It should be noted that magnesium deficiency is less common in summer and manifests itself more easily than in winter [7]. In the same type of product, the concentration of magnesium can vary significantly. Treatment with mineral water with magnesium ions and salts is of particular importance when preparing a dietary correction. Waters containing a significant amount of magnesium include “Batalinskaya” (Mg - 1.52 g/l), “Donat”, “Slovenia” (Mg - 1.26 g/l), water from the Lysogorsk well, “Pyatigorsk” (Mg - 0.65 g/l), water from the Kuka resort (well No. 27, Mg - 0.23 g/l), as well as Crimean Narzan and Kislovodsk Narzans. All other waters tend to have a very low magnesium content.
It should be noted that almost all vitamin and mineral complexes for pregnant women contain magnesium in low-access and poorly absorbed inorganic magnesium compounds. Recently proposed natural preparations for the correction of calcium and magnesium, obtained from animal bones and dolomite flour, oyster shells, shells, have not been sufficiently studied; there is no data on adequate purification of these preparations from harmful impurities, in particular from lead. And pregnant women should not use biologically active food supplements that do not have special recommendations for pregnant women. The prescription of magnesium preparations is a kind of replacement therapy and is carried out to correct its normal level and restore physiological processes in which magnesium takes an active part [7]. According to evidence-based medicine, intravenous use of magnesium sulfate in significant dosages or over a certain period of time can be very unsafe for both mother and child, so the issue of oral use of magnesium during pregnancy in the form of its various preparations remains relevant. The drugs of choice for the treatment of chronic magnesium deficiency and long-term prevention of pregnancy complications are oral dosage forms.
Nutritional correction with organic magnesium preparations is considered as an independent type of metabolic replacement therapy and is not mixed with the administration of high doses of magnesium sulfate for tocolytic purposes. To provide nutritional support in pregnant women and children with magnesium deficiency, various drugs have been developed. One of these drugs, widely used in obstetrics and gynecology, is a combination preparation of second-generation organic magnesium salt (lactate or pidolate) and vitamin B6 (pyridoxine). The first generation of magnesium preparations includes inorganic compositions: magnesium oxide, sulfate, chloride, etc.; the second - organic compounds: magnesium lactate, pidolate, orotate, glycinate, asparaginate, citrate, ascorbate [4, 7]. The bioavailability of organic magnesium salts is almost an order of magnitude higher than that of inorganic ones. Thus, the bioavailability of lactate, citrate and orotate is several times (5–6 times) higher than that of magnesium sulfate. Magnesium pidolate, citrate, gluconate, and aspartate also have a higher excretory capacity (in urine) than inorganic salts. Inorganic magnesium salts are less well tolerated and more often cause dyspeptic complications (diarrhea, vomiting, abdominal cramps). Organic magnesium salts are not only much better absorbed, but also easier to tolerate by patients and less likely to cause side effects from the digestive tract.
Treatment will be more effective if both magnesium and a magnesium fixative are administered simultaneously: B vitamins (B6 or B1); glycine, orotic acid. Pyridoxine is a good magnesium fixative because it improves the bioavailability of magnesium, magnesium forms well-absorbed complexes with the vitamin, in addition, vitamin B6 promotes the penetration of magnesium into cells and its preservation within cells. In addition, vitamin B6 and magnesium deficiencies are often combined with each other and have a similar clinical picture. It is also important that vitamin B6 forms a biocoordination bond with four magnesium atoms at once, which improves its bioavailability. In combination with magnesium, pyridoxine penetrates much better through the lipid layer of the membrane of any cells.
There are several galenic forms that are well absorbed in the intestines, released in the form of drugs: magnesium citrate, magnesium gluconate, magnesium orotate, magnesium thiosulfate, magnesium lactate and magnesium pidolate. The content of elemental magnesium in dosage forms varies. For example, magnesium gluconate, 0.5 g tablets contains 27 mg; magnesium citrate, effervescent tablets 0.15 g - 24.3 mg; magnesium orotate, tablets 0.5 g - 32.8 mg; magnesium thiosulfate, tablets 0.5 g - 49.7 mg; magnesium lactate – 48 mg [9].
According to a number of authors, undesirable manifestations of a combined deficiency of pyridoxine and magnesium appear already in the first trimester of pregnancy, and the administration of magnesium supplements to pregnant women, starting from the 4th–5th week of pregnancy, leads to a significant decrease in the level of spontaneous miscarriages [5–7]. Hypomagnesemia leads to fetal growth retardation due to insufficient transfer of magnesium from mother to fetus through the placenta, as well as due to impaired circulating plasma volume and the need for protein synthesis. In addition to protein deficiency, magnesium deficiency in the fetus leads to disruption of cellular energy metabolism and increased transmembrane metabolism.
Data from a meta-analysis of five placebo-controlled studies on the use of 2nd generation organic magnesium salts (magnesium lactate and magnesium citrate at a dose of 150 mg, 2 times a day) in pregnant women represent a high level of confidence. An objective and independent analysis has proven complete safety and high effectiveness for relieving calf muscle cramps (5 mmol in the morning and 10 mmol in the evening) [30].
A Cochrane study conducted to evaluate the effect of magnesium supplementation during pregnancy on pregnancy outcome and maternal and fetal health included 7 studies (2689 women). A pooled analysis of a cluster-design study found that magnesium supplementation before 25 weeks' gestation (compared with placebo) reduced the incidence of preterm birth (RR 0.73; 95% CI 0.57–0.94) and birth defects. low body weight (OR 0.67; 95% CI 0.46–0.96). Moreover, these women were less likely to be hospitalized (RR 0.66; 95% CI 0.49–0.89) and less likely to have antepartum hemorrhage (RR 0.38; 95% CI 0.16–0.90). In the remaining six studies, the differences in the effects of magnesium and placebo were not statistically significant. Therefore, the effectiveness of magnesium supplementation requires further investigation using studies with high quality design [2].
Another common use of magnesium in obstetrics is its use as a tocolytic. A number of studies of magnesium have shown advantages over sympathomimetics [16], but in other studies the results were opposite [28] or comparable [19] when comparing maternal and fetal risk and side effects. A number of studies have carried out a comparative assessment of the tocolytic activity of magnesium sulfate and nitric oxide donors (nitrates): the antispasmodic activity of magnesium turned out to be higher [23]. However, not all studies have proven the effectiveness of magnesium sulfate therapy in preventing preterm birth.
To evaluate the effectiveness and safety of magnesium sulfate in women with threatened preterm labor, a meta-analysis was conducted in the Cochrane database, analyzing 23 studies that included more than 2000 women. Only 9 studies met the criteria for high quality. The analysis revealed that magnesium sulfate does not slow down or prevent premature birth, but its use is associated with a lack of a positive effect on morbidity and an increase in neonatal mortality. It was concluded that further, larger and higher-quality studies are needed to seriously assess morbidity and mortality, as well as compare different drug administration regimens [1, 2, 22].
A special place in the list of indications for treatment with magnesium preparations is occupied by eclampsia - a severe multiple organ disorder of unknown etiology. The pathogenesis of eclampsia is complex, insufficiently studied and includes such links as endothelial dysfunction, impaired rheological properties of blood, and generalized vasoconstriction. The mechanisms of action of magnesium sulfate in eclampsia include suppression of the synthesis of thromboxane A2 and antagonism with calcium, leading to vascular dilatation, improvement of blood flow in the “mother-placenta-fetus” system and cerebral circulation [13, 18], another possible mechanism of action of magnesium sulfate is an increase in the level of calcitonin in the blood serum, which is reduced in women with preeclampsia [1, 14].
The effect of magnesium therapy in the treatment of eclampsia and a significant reduction in maternal mortality were shown in the famous randomized, placebo-controlled MAGPIE trial, in which magnesium treatment halved the risk of developing eclampsia in the absence of significant adverse reactions [20].
When comparing magnesium therapy and its effectiveness relative to anticonvulsants (diazepam, phenytoin, lytic cocktail), a large number of studies have demonstrated the effectiveness of magnesium sulfate in the prevention and treatment of eclampsia in comparison with other anticonvulsants [21, 25]. Thus, according to five studies that included observations of 1236 women [30], it was shown that magnesium therapy leads to a significant reduction in the frequency of seizures compared to diazepam and, as a result, leads to a decrease in maternal mortality. When comparing the effect of magnesium therapy and lytic mixtures, the advantage of magnesium sulfate was also shown, since it was more effective in preventing repeated convulsive seizures, inhibited respiratory function to a lesser extent and more effectively eliminated cases of ongoing seizures, in addition, with its use, cases of perinatal mortality [27].
The advantages of magnesium sulfate in comparison with calcium antagonists in moderate preeclampsia were also revealed, while in severe preeclampsia, nimodipine improved cerebral circulation to a greater extent than magnesium sulfate [12]. The standard dosage of magnesium as an anticonvulsant involves a loading dose of 4 g IV and 10 g IM, followed by either 5 g IM every 4 hours or a maintenance IV infusion of 1–2 g/hour. However, there is evidence of the effectiveness of lower, even half doses of the drug in preventing seizures and reducing mortality from 16% to 8% [11]. Patients receiving low maintenance doses of magnesium (2 g/hour) had a lower incidence of side effects compared with those receiving 5 g/hour [1, 29].
It is known that low levels of intracellular magnesium can contribute to the development of arterial hypertension in pregnant women. This is the basis for the use of magnesium in isolated hypertension in pregnant women, although it is not a drug for the treatment of arterial hypertension. The hypotensive activity of magnesium is comparable to methyldopa [1, 10, 17, 24].
Magnesium deficiency is also associated with sudden infant death syndrome (SIDS). SIDS may be caused by a decrease in thermoregulatory mechanisms in brown adipose tissue, leading to a change in temperature point. There are two forms of the pathological process. The hypothermic form can be caused by a functional deficiency of brown adipose tissue, and the hyperthermic form is associated with hyperfunction of the thermogenesis system. Some forms of SIDS can develop as a result of chronic magnesium deficiency in the mother, causing chronic deficiency of this microelement in the newborn and leading to impaired thermoregulation and changes in the temperature point. Prevention of SIDS caused by magnesium deficiency in a newborn can be carried out using magnesium replacement therapy in the mother [15].
With the exception of hypothyroidism, renal and adrenal insufficiency, as well as dehydration, hypermagnesemia in pregnant women is an iatrogenically provoked condition in which it is necessary to exclude the use of magnesium-containing antacids to reduce increased gastric acidity, as well as intravenous administration of magnesium sulfate. Contraindications to magnesium therapy in pregnant women include ketoacidosis, diabetic nephropathy, proliferating nephropathy in diabetes mellitus, renal and adrenal insufficiency. Moreover, renal failure in a pregnant woman (if it is impossible to organize monitoring of magnesium concentration in the blood in the mode of one measurement every two hours) is an absolute contraindication, including for the use of magnesium-containing drugs of the 2nd generation for oral administration. Intravenous administration of magnesium sulfate solutions for oliguria (with creatinine clearance below 20 ml/min), bradycardia, hereditary myopathies in a pregnant woman, thrombophilia, thrombocytopenia is contraindicated [1, 15].
In Russia, intramuscular administration of some magnesium preparations is widespread, but in developed countries it is not used for ethical reasons due to severe pain at the injection site and the possibility of developing an abscess [3, 4]. Parenteral magnesium therapy is indicated only in severe cases of magnesium deficiency, for the treatment of severe complications (preeclampsia) or urgent conditions (threatened miscarriage). On the other hand, magnesium preparations for oral administration are considered primarily as an effective nutritional correction and vitamin and mineral therapy, and not a first-line treatment for severe pregnancy complications.
Thus, there is currently a large amount of data on the possibilities of using magnesium preparations in obstetric practice. Accumulated experience shows that chronic magnesium deficiency can lead to serious pregnancy complications and adverse outcomes in the mother, fetus and newborn and should be compensated in advance, without waiting for the development of urgent situations, by taking special magnesium preparations. The use of magnesium preparations is justified in cases of threatened miscarriage and premature birth, in the treatment and prevention of preeclampsia. At the same time, it should be recognized that there are controversial issues regarding many aspects of the use of magnesium in obstetric practice, and not all existing practical recommendations are confirmed from the standpoint of evidence-based medicine.
Literature
- Alekseeva O.P., Klemenov A.V., Guseva O.I. et al. Magnesium in the pathology of pregnancy and childbirth // Breast cancer. 2004. No. 1, p. thirty.
- Pregnancy and childbirth. Cochrane manual. Under. ed. Sukhikh G.T.M.: Logosphere, 2010. P. 410.
- Gromova O. A. Vitamins and microelements in preconception, during pregnancy and in nursing mothers. Clinical pharmacology. UNESCO training programs, Manual for doctors. Ed. V. M. Sidelnikova. M., 2006. 124 p.
- Gromova O. A. Magnesium and pyridoxine: basic knowledge. ProtoTip, 2006. 234 p.
- Kosheleva N. G. The role of hypomagnesemia in obstetric pathology and methods of its correction // Vestn. Ross. assoc. obstetricians-gynecologists. 1999. No. 1. p. 42–46.
- Kosheleva N. G., Arzhanova O. N., Pluzhnikova T. A. Miscarriage: Etiopathogenesis, diagnosis, clinic and treatment, St. Petersburg, 2003, 70 p.
- Sidelnikova V. M. Use of the drug Magne B6 in the miscarriage clinic // Obstetrics and Gynecology, 2002, No. 6, p. 47–48.
- Vidal Directory. Medicines in Russia: Directory. M.: AstraPharmServis, 2008, 1488 p.
- Chekman I. S., Gorchakova N. A., Nikolai S. L. Magnesium in medicine. Kishinev. 101 p.
- Adam B., Malatyalioglu E., Alvur M., Talu C. Magnesium, zinc and iron levels in pre-eclampsia // J Matern Fetal Med 2001; 10 (4): 246–250.
- Begum R., Begum A., Bullough CH, Johanson RB Reducing maternal mortality from eclampsia, using magnesium sulphate // Eur J Obstet Gynecol Reprod Biol. 2000; 92(2):223–224.
- Belfort MA, Saade GR, Yared M. et al. Change in estimated cerebral perfusion pressure after treatment with nimodipine or magnesium sulfate in patients with preeclampsia // Am J Obstet Gynecol. 1999; 181(2):402–407.
- Belfort MA, Anthony J., Saade GR, Allen JC A comparison of magnesium sulfate and nimodipine for the prevention of eclampsia // N Engl J Med. 2003; 348(4):304–311.
- Halhali A., Wimalawansa S. J., Berentsen V. et al. Calcitonin gene- and parathyroid hormone-related peptides in preeclampsia: effects of magnesium sulfate // Obstet Gynecol. 2001; 97(6):893–897.
- James MFM Magnesium in obstetrics. Best Pract & Res Clin Obst & Gyn. Vol. 24, Iss. 3, 2010, p. 327–337.
- Katz VL, Farmer RM Controversies in tocolytic therapy // Clin Obstet Gynecol. 1999; 42(4):802–819.
- Kisters K., Barenbrock M., Louwen F. et al. Membrane, intracellular, and plasma magnesium and calcium concentrations in preeclampsia // Am J Hypertens. 2000; 13(7):765–769.
- Li S., Tian H. Oral low-dose magnesium gluconate preventing pregnancy induced hypertension // Zhonghua Fu Chan Ke Za Zhi. 1997;32(10):613–615.
- Macones GA, Sehdev HM, Berlin M. et al. Evidence for magnesium sulfate as a tocolytic agent // Obstet Gynecol Surv. 1997; 52(10):652–658.
- The Magpie Trial Collaboration Group. Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomized placebo-controlled trial // Lancet. 2002; 359(9321): 1877–1890.
- Manyemba J. Magnesium sulphate for eclampsia: putting the evidence into clinical practice // Cent Afr J Med. 2000; 46 (6): 166–169.
- Matsuda Y., Kouno S., Hiroyama Y. et al. Intrauterine infection, magnesium sulfate exposure and cerebral palsy in infants born between 26 and 30 weeks of gestation // Eur J Obstet Gynecol Reprod Bio. 2000;91(2):159–164.
- Morgan PJ, Kung R., Tarshis J. Nitroglycerin as a uterine relaxant: a systematic review // J Obstet Gynaecol Can. 2002; 24 (5): 403–409.
- Qi Q., Li W., Wang Z. Magnesium and calcium concentration of peripheral serum and mononuclear cells in patients with pregnancy induced hypertension // Zhonghua Fu Chan Ke Za Zhi. 1997; 32 (1): 15–18.
- Raman NV, Rao CA Magnesium sulfate as an anticonvulsant in eclampsia // Int J Gynaecol Obstet. 1995; 49(3):289–298.
- Roffe C., Sills S., Crome P., Jones P. Randomised, cross–over, placebo controlled trial of magnesium citrate in the treatment of chronic persistent leg cramps // Med Sci Monit. 2002; 8 (5): 326–330.
- Sawhney H., Vasishta K., Rani K. Comparison of lytic cocktail and magnesium sulphate regimens in eclampsia: a retrospective analysis // J Obstet Gynaecol Res. 1998; 24 (4): 261–266.
- Surichamorn P. The efficacy of terbutaline and magnesium sulfate in the management of preterm labor // J Med Assoc Thai. 2001; 84(1):98–104.
- Terrone DA, Rinehart BK, Kimmel ES et al. A prospective, randomized, controlled trial of high and low maintenance doses of magnesium sulfate for acute tocolysis // Am J Obstet Gynecol. 2000; 182(6):1477–1482.
- Young GL, Jewell D. Interventions for leg cramps in pregnancy // Cochrane Database Syst Rev. 2002, 1.
R. G. Shmakov , Doctor of Medical Sciences E. S. Polushkina Scientific Center for Obstetrics, Gynecology and Perinatology named after. V. I. Kulakova , Moscow
Contact information for authors for correspondence
Magne B6 during pregnancy
Why Magne B6 during pregnancy?
Magne b6 is prescribed quite often during pregnancy. It is advisable to use the drug in pregnant women when:
- hypertonicity of the uterine muscles threatening spontaneous miscarriage ;
- Mg deficiency confirmed by test results .
Clinical experience with the use of Mg preparations and doctors’ reviews of Magne B6 indicate that prescribing the drug for uterine hypertonicity allows you to quickly and effectively calm the nervous system, as well as relieve spasms and tension in the muscles.
The main reason for the increased tone of the uterine muscles is the calcium contained in the muscle fibers. Mg has the ability to reduce its amount and thereby promote muscle relaxation.
During the period of bearing a child, the female body requires more magnesium than usual. If the microelement is not supplied to it from the outside in the required doses, the fetus begins to draw Mg from the mother’s body, which significantly affects the health and well-being of the pregnant woman. Once the mother's Mg reserves are depleted, the condition of the fetus will also begin to deteriorate.
Magnesium deficiency causes poor development of blood vessels in the placenta, which leads to malnutrition of the fetus and the threat of miscarriage.
Contraindications
The instructions for the drug indicate that contraindications to its use are fructose intolerance , severe renal failure , allergic reactions to the substances contained in the tablets/solution.
How to take MagneB6 during pregnancy?
The dosage of Magne B6 during pregnancy is usually as follows: 2 tablets with each of the main meals (morning, lunch and evening). Thus, the dose of Magne B 6 for a pregnant woman is 6 tablets per day, and the dosage regimen does not change depending on the stage of pregnancy.
In the 1st and 2nd trimesters, the use of the drug is advisable if there is a threat of miscarriage. In the third trimester, a woman usually experiences an increased feeling of discomfort, night cramps and swelling.
Magnesium deficiency can lead to increased secretion of aldosterone and the development of edema. Delayed removal of fluid from the body, in turn, provokes an increase in blood pressure , which is very dangerous both during pregnancy and during childbirth.
The duration of treatment can range from 2 weeks to 9 months. After childbirth, the drug is stopped, since it tends to penetrate into the milk of a nursing woman.
Reviews from specialists and clinical experience with the use of Magne B6 during pregnancy indicate that the drug does not have an adverse effect on the process of prenatal development or fetotoxic effect. However, the drug can only be used if indicated and only on the recommendation of a doctor.
Magne B6 forte for magnesium and vitamin B6 deficiency tablets No. 40
A country
Hungary
The country of production may vary depending on the batch of goods. Please check with the operator for detailed information when confirming your order.
Compound
1 tablet contains the core of the tablet: active ingredients: magnesium citrate - 618.43 mg, which corresponds to 100 mg of magnesium (Mg++), pyridoxine hydrochloride - 10.00 mg; excipients: lactose - 50.57 mg, macrogol-6000 - 120.00 mg, magnesium stearate - 1.00 mg. Tablet shell: hypromellose 6 mPa.s - 14.08 mg, macrogol-6000 - 1.17 mg, titanium dioxide (E 171) - 4.75 mg, talc - traces. Description Oval, biconvex, white film-coated tablets. At the fracture, two layers are visible: a white shell and a white tablet mass. Release form: Film-coated tablets. 15 or 20 tablets in a blister made of PVC-PE-PVDC/aluminum foil. 2 or 4 blisters of 15 tablets each, 2 or 3 blisters of 20 tablets each, along with instructions for use in a cardboard box.
Pharmacological properties
Pharmacodynamics Magnesium is a vital element that is necessary for the normal functioning of cells and is involved in most metabolic reactions. In particular, it is involved in the regulation of the transmission of nerve impulses and muscle contraction. 1/3 of the amount of magnesium contained in the body accumulates in bone tissue. The body receives magnesium through food. A lack of magnesium in the body can be observed when the diet is disrupted, when the need for magnesium increases, or when there is an imbalance in the intake, metabolism and excretion of magnesium (for example, with increased physical and mental stress, stress, during pregnancy, when using diuretics). Pyridoxine (vitamin B6) is involved in many metabolic processes and helps improve the absorption of magnesium from the gastrointestinal tract and its penetration into cells. Serum magnesium levels: - between 12 and 17 mg/L (1 - 1.4 mEq/L or 0.5 - 0.7 mmol/L): indicate mild magnesium deficiency; - below 12 mg/L (1 mEq/L or 0.5 mmol/L): indicate severe magnesium deficiency. Pharmacokinetics Gastrointestinal absorption of magnesium salts occurs partly through a passive mechanism in which the solubility of the salt plays a determining role. The degree of this absorption does not exceed 50%. Excretion occurs mainly by the kidneys.
Indications for use
Established magnesium deficiency, isolated or associated with other deficiency conditions, accompanied by symptoms such as increased irritability, minor sleep disturbances, gastrointestinal cramps, rapid heartbeat, increased fatigue, muscle pain and spasms, and a tingling sensation in the muscles. If after a month of treatment there is no improvement in these symptoms, continuing treatment is not advisable.
Contraindications
Hypersensitivity to any of the components of the drug. Severe renal failure (creatinine clearance less than 30 ml/min). Phenylketonuria. Age up to 6 years (efficacy and safety have not been established). Hereditary galactosemia, glucose and galactose malabsorption syndrome, or lactase deficiency (due to the presence of lactose in the drug). Concomitant use of levodopa (see “Interaction with other drugs”). With caution: Moderate renal failure (risk of developing hypermagnesemia). Use during pregnancy and breastfeeding Pregnancy Clinical experience with the drug in a sufficient number of pregnant women has not revealed any adverse effects on the occurrence of fetal malformations or fetotoxic effects. The drug Magne B6® forte can be used during pregnancy only if necessary, on the recommendation of a doctor. Breastfeeding period Taking into account that magnesium passes into breast milk, if it is necessary to take the drug, it is recommended to stop breastfeeding.
Mode of application
The tablets should be taken whole with a glass of water. Adults: 3-4 tablets per day, divided into 2-3 doses, with meals. Children over 6 years of age (weighing about 20 kg): 10-30 mg/kg/day (0.4–1.2 mmol/kg/day), i.e. children over 6 years of age (weighing about 20 kg) 2- 4 tablets per day, divided into 2-3 doses, with meals. Typically the duration of treatment is one month.
Side effect
Immune system disorders: Very rare (Gastrointestinal disorders: Unknown frequency (it is not possible to estimate the frequency of occurrence based on available data): diarrhea, abdominal pain, nausea, vomiting, flatulence.
Overdose
Symptoms With normal renal function, an overdose of magnesium when taken orally does not usually lead to toxic reactions. However, in case of renal failure, magnesium poisoning may develop. Symptoms of overdose, the severity of which depends on the concentration of magnesium in the blood: decreased blood pressure; nausea, vomiting; depression of the central nervous system, decreased reflexes; changes in the electrocardiogram; respiratory depression, coma, cardiac arrest and respiratory paralysis; anuric syndrome. Treatment Rehydration, forced diuresis. In case of renal failure, hemodialysis or peritoneal dialysis is necessary.
Interaction
Contraindicated combinations With levodopa: the activity of levodopa is inhibited by pyridoxine (unless taking this drug is combined with taking inhibitors of peripheral aromatic L-amino acid decarboxylase). Any amount of pyridoxine should be avoided unless levodopa is taken in combination with peripheral aromatic L amino acid decarboxylase inhibitors. Not recommended combinations The simultaneous use of drugs containing phosphates or calcium salts may impair the absorption of magnesium in the intestine. Combinations that should be taken into account When prescribing tetracyclines orally, it is necessary to maintain an interval of at least three hours between ingestion of tetracycline and Magne B6 forte, since magnesium preparations reduce the absorption of tetracyclines.
special instructions
The tablets are intended only for adults and children over 6 years of age. In case of moderate renal failure, the drug should be taken with caution due to the risk of developing hypermagnesemia. If calcium and magnesium are deficient at the same time, the magnesium deficiency should be corrected before taking calcium supplements or dietary supplements containing calcium. When pyridoxine is used in high doses (more than 200 mg per day) for a long time (over several months or in some cases years), sensory axonal neuropathy may develop, which is accompanied by symptoms such as numbness and impaired proprioceptive sensitivity, distal tremor limbs and gradually developing sensory ataxia (impaired coordination of movements). These disorders are usually reversible and disappear after stopping taking vitamin B6. Impact on the ability to drive vehicles and engage in other potentially hazardous activities No effect. There are no special recommendations.
Reviews of Magna B6
Reviews from doctors about Magna B6 are positive: experts consider this remedy to be indispensable in conditions where the patient’s body suffers from magnesium deficiency . It is especially important for children and during pregnancy. In addition, Mg preparations are the core of neurorehabilitation and therapeutic measures for pathologies such as attention deficit in children and hyperactivity.
Prescribing Magne B6 to children - reviews from doctors and mothers confirm this fact - can significantly improve the general condition of the child, reduce his aggressiveness, increase attentiveness, improve behavior, and school performance.
Magne b6 helps to normalize the magnesium balance and, consequently, the physiological processes occurring in the body, in particular, the processes that ensure the normal functioning of the heart, as well as the nervous and vascular systems, creating an optimal background for pharmacotherapy in adults and children.
Since the drug contains Mg in organic form and in an acceptable dosage, its use is usually not associated with side effects.
As an alternative to Magne B6, to correct magnesium deficiency, the patient may be prescribed Magnesium B6 Evalar , Magnistad , Magnelis B6 .
Magnesium for health
Magnesium is an essential trace element that is directly involved in the functioning of the nervous system. Regulates cellular metabolism, ensures the transmission of nerve impulses between muscles and the brain. A sufficient amount of this element in the body helps to more easily endure stress and shock, not experience muscle tone and spasms, and regulate mood and emotions.
Magnesium is extremely important for women's health during pregnancy. Regulates endocrine functions. Magnesium is best absorbed only in combination with vitamin B6 or pyridoxine. Therefore, it is required to be present in magnesium preparations.
The main symptoms of magnesium deficiency in the body:
- headache;
- tachycardia;
- arrhythmia;
- muscle cramps;
- irritability;
- insomnia;
- premenstrual syndrome;
- "lazy bowel" syndrome;
- anxiety and neurasthenic disorders;
- photosensitivity and sensitivity to noise;
- hypertension;
- increased level of platelets in the blood.
Price Magne B6
Cost of the drug in Russian pharmacies
The price of Magne B6 tablets No. 50 is from 280 rubles, the price of Magne B6 in ampoules No. 10 is from 360 rubles.
Price Magne b6 in Ukraine
The average price of tablets No. 50 is 140 UAH; you can buy a solution for about 70 UAH.
Despite the fact that Magne B6 belongs to the category of over-the-counter products, you should consult your doctor before purchasing the drug (especially for children and during pregnancy).
- Online pharmacies in RussiaRussia
- Online pharmacies in UkraineUkraine
ZdravCity
- Magne B6 forte tab.
p/o captivity. 40pcs Hinoin Pharmaceutical and Chemical Products Plant CJSC RUR 609 order
Pharmacy Dialogue
- Magne B6 (tab.vol. No. 180) Quinoin Plant Pharm. and Khim.prod. JSC
RUB 1,218 order
show more