Do liver steatosis need to be treated?
Very often, routine ultrasound diagnostics of the liver reveal diffuse changes in the liver such as steatosis (fatty hepatosis, fatty infiltration of the liver).
Liver steatosis is a common phenomenon for older people, most often accompanying the aging process, however, recently liver steatosis is also characteristic of young people, and even perhaps without accompanying excess weight? Of course, steatosis is a disease that is expressed in the fact that adipose tissue is formed inside the liver instead of liver tissue , which does not perform the function of the liver and differs from liver tissue in its structure by its high density. With steatosis, the amount of healthy liver gradually decreases and over time, the remaining healthy part will not be able to ensure the vital functions of the body. This stage of the disease is called cirrhosis of the liver and is difficult to treat.
The problem is complicated by the fact that the liver does not hurt, and even if it is seriously damaged, the patient does not have any complaints, with the exception of a possible feeling of heaviness in the right hypochondrium .
Most often, heaviness and discomfort in the right hypochondrium with steatosis, as with other liver pathologies, are caused by an increase in its size.
Types of steatosis
There are two types of steatosis: alcoholic and non-alcoholic. Until the 1980s, experts believed that only chronic alcoholism leads to steatosis. This is how the diagnosis of “alcoholic liver disease” (ALD) appeared. Steatosis is extremely common in Russia and occurs in 90% of alcoholics2. Later, large fat droplets in hepatocytes were discovered in patients with diabetes and obesity. This is how the concept of non-alcoholic steatosis, or non-alcoholic fatty liver disease (NAFLD), which was identified in every third Russian, appeared3.
Causes of liver steatosis
What is the cause of liver steatosis , why, according to statistics from the European Association of Hepatologists, is this disease widespread as an epidemic? The most common opinion is poor nutrition and a sedentary lifestyle. And this is a big mistake. The cause of steatosis is not an unhealthy lifestyle, but hormonal and metabolic changes; this is a disease that, in addition to lifestyle correction, nutrition and physical activity, also requires observation by a hepatologist and endocrinologist!
Who is at risk?
Get checked now for the risks of developing fatty liver disease:
- Obesity, accumulation of fat in the abdominal area. At risk are women with a waist of more than 80 cm and men with a waist of more than 95 cm.
- Hypertonic disease. Pressure above 130/85 mmHg.
- Insulin resistance and diabetes.
- Metabolic disorders.
- Elevated cholesterol and triglyceride levels more than 1.7 mmol/liter.
- Reduced levels of high-density lipoproteins.
- Alcoholism and alcohol abuse.
Treatment of liver steatosis
Like any liver disease in which it is destroyed with a possible outcome in cirrhosis, treatment of steatosis is possible only with medications that act on the cause of the disease. In the case of steatosis, the cause of the disease is metabolic and hormonal disorders , which cause changes in the structure of the liver tissue. Internal fatty liver is always accompanied by a pathological flow of fat into the pancreas, heart and blood vessels, and kidneys. This life-threatening systemic disease is called metabolic syndrome.
Metabolic syndrome is treated by a hepatologist together with an endocrinologist , affecting both the causes of the disease and the consequence - steatosis. The result of treatment is always recovery if treatment is prescribed on time. In addition to drug correction of metabolic disorders, the treatment complex includes recommendations for proper nutrition and physical activity, which on their own, without treatment, do not produce results. The difficulty of treatment is due to the fact that the share of success in treatment depends on the behavior of the patients, which is why the patient’s serious awareness and desire to get results is so important.
Treatment of NAFLD
Medications can help with liver disease, but it is also important to follow your doctor's recommendations for lifestyle changes.
- Play sports. It sounds scary, but you can start by walking briskly for 30 to 40 minutes every day. Then gradually add aerobic (dancing, running), and later strength exercises to strengthen the muscles. Reducing weight by at least three to five percent can already reduce the severity of steatosis3,5. Just make sure that your body weight does not decrease too rapidly; It is enough to lose weight by 0.5–1 kilogram per week3.
- Adjust your diet. Avoid sweet, fatty, fried foods and baked goods. It is best to adhere to the principles of the Mediterranean diet. Add to your diet foods with a high content of plant fiber, fresh vegetables and fruits (taking into account their calorie content), focus on vegetable fats and proteins (nuts, legumes, grains), fish and seafood 3.5.
- Stop smoking, alcohol, and sweet carbonated drinks3.5. Drug therapy includes taking hepatoprotectors based on essential phospholipids (EPL). They are embedded in the membranes of liver cells, restore them and protect them from damaging influences8. In addition, EPLs are involved in the processes of normalizing metabolism and help slow down the progression of the disease8.
Weight loss, proper nutrition, and medications can all help with steatosis. But remember that the most important thing when dealing with a disease is its timely detection. Pay close attention to your health and do not forget to get examined regularly.
Necessary examinations for prescribing and monitoring treatment of liver steatosis
To prescribe treatment for liver steatosis, it is necessary to undergo an examination that reveals the degree of liver damage and the severity of metabolic syndrome indicators. The modern equipment of our center allows us not only to detect fatty tissue in the liver, but also to calculate the percentage of normal healthy tissue in the liver and how much non-functioning fatty tissue! This is important for treatment tactics and prognosis for recovery.
The Fibroscan device with an additional sensor for assessing steatosis allows not only to quantify the fatty tissue in the liver according to the degree of steatosis from 0 to 3, but also allows you to measure the result of treatment, which in most cases leads to complete normalization of the liver structure (steatosis 0). Treatment is prescribed individually depending on the examination results. There is no common treatment regimen for all, since metabolic and hormonal disorders can be expressed differently.
Development of steatosis
The main risk factor for developing alcoholic liver disease is chronic alcohol abuse.
In the case of NAFLD, there are many more risk factors2:
- Excess body weight.
- A disorder of lipid metabolism that causes lipid peroxidation and subsequently the development of oxidative stress.
- Insulin insensitivity (insulin resistance) and type 2 diabetes; malabsorption disorders (malabsorption); diseases of the gastrointestinal tract.
- Losing weight too quickly and starving yourself.
- Taking certain medications that can have a toxic effect on the liver: glucocorticosteroids, non-steroidal anti-inflammatory drugs, estrogens, antibiotics, etc.
- Accumulation of copper and iron in the liver due to various metabolic diseases.
Results of treatment of liver steatosis
Patient review:
» Dear Bella Leonidovna!
Dear Nelly Nikolaevna Tsurikova, Mushinskaya Kira Vladimirovna, girls at the reception, ultrasound diagnostic doctor, thank you all so much for organizing the treatment of my illness. You guys work wonders as a team! High-level professionals and people with a capital “P!” I am grateful to fate that I found your clinic, which really saved my life and changed it 180 degrees. Thanks to your efforts, qualifications and attention, I have become a completely healthy person. I lost 23.5 kg in 9 months, my liver has become a real factory that now works perfectly!
In general, I wish your team all the best. Do not stop! You really do a great job for people, help overcome serious illnesses.
On the eve of the New Year 2021, I would like to wish you health, family joys and love too! with best wishes, your patient from Kazan" >>> - Rustem 12/05/2018
Diagnosis of non-alcoholic fatty liver disease
In a biochemical blood test
There is an increase in liver enzymes ALT and AST to 4 norms, alkaline phosphatase to 2 norms.
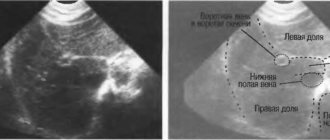
During ultrasound examination (ultrasound)
The information content of the method decreases in obese patients.
Computed tomography (CT)
– allows you to accurately assess the degree
of steatosis
, the sensitivity and specificity of the method is 93-100%.
Magnetic resonance imaging (MRI)
– provides a complete image of the organ in any projection, has a high agreement with the data of histological examination.
Liver elastography
– has higher accuracy in advanced stages of liver damage (fibrosis).
Causes of the disease
Alcoholic liver disease (ALD) develops with regular consumption of toxic doses of alcohol. This is one of the main reasons for the development of chronic liver pathology, from which about 14,000 people die every year in the Russian Federation1. 90% of alcohol abusers have fatty liver disease. This is the first stage of the disease, associated with excessive accumulation of fat in the liver tissue. At the same time, 5-15% of patients develop steatohepatitis and cirrhosis within 20 years1.
Toxic doses of alcohol for the liver are considered to be 30 g in terms of pure ethanol for men and 20 g for women3. To imagine how many alcoholic drinks we are talking about, you need to understand that every 100 g of 40° alcoholic drink contains 40 g of ethanol.
Non-alcoholic fatty liver disease (NAFLD) usually develops in patients with overweight/obesity and type II diabetes mellitus. The diagnosis of NAFLD is a diagnosis of exclusion, and is made when all other possible liver pathologies, such as viral hepatitis or alcoholic liver disease, have been excluded. NAFLD can also progress sequentially from steatosis (fatty degeneration) to steatohepatitis, and then to fibrosis and cirrhosis4.
The prevalence of NAFLD is constantly growing: today it is up to 37% (on average among adult patients who consult a doctor)5.
Alcoholic and non-alcoholic steatohepatitis have different risk factors, but the main stages of their development are similar. The initial stage in both cases is steatosis, that is, the accumulation of fatty droplets in the liver tissue. Then an inflammatory process occurs with the destruction of liver cells and steatohepatitis develops. The next stage is the formation of connective tissue in place of dead hepatocytes, which changes the structure of the liver, which can subsequently cause disruption of its function.
Alcohol abuse and obesity are two independent risk factors causing steatosis. When exposed to both factors, the risk of developing the disease increases almost 2 times: for example, in the Dionysos study (Dionysos study, 1994), according to biopsy data in obese individuals, steatosis was observed in 46% of cases, and in the presence of both factors - in 95%7 .
Both diseases are characterized by a poor prognosis: with alcoholic liver disease, the likelihood of developing cirrhosis in ALD is 10 times higher6, while in NAFLD the risk of developing cardiovascular diseases is several times higher4.
Diagnostics
Laboratory changes
are also nonspecific4,5:
- Changes in laboratory parameters characteristic of cytolysis (destruction of liver cells): as a rule, in patients with non-alcoholic fatty liver disease, there is a predominance of ALT (alanine aminotransferase) over AST (aspartate aminotransferase), and in alcoholic liver disease, on the contrary, an excess of AST levels is observed (usually the ratio AST/ALT above 2). However, the degree of increase in AST and ALT activity does not correlate with the severity of steatosis, steatohepatitis or liver fibrosis: the absence of an increase in AST and ALT enzymes can be observed in 80% of patients with NAFLD8.
- It is possible to increase the activity of alkaline phosphatase and gammaglutamyl transpeptidase (GGTP). Changes in these indicators are also not specific, can be caused by various reasons and do not always indicate the development of cholestasis (stagnation of bile). Thus, GGTP most often increases due to alcohol consumption.
Instrumental diagnostics can
include4,5:
- Ultrasound of the abdominal cavity. Ultrasound signs of steatosis include, first of all, increased echogenicity (the phenomenon of “bright white liver”), heterogeneity of the structure of organ tissues, and blurred vascular patterns and signal attenuation may also be observed.
- If necessary, a CT scan, MRI of the liver, or a liver biopsy may be performed. A biopsy is the “gold standard” for diagnosing liver diseases, which makes it possible to evaluate changes in liver tissue at the microscopic level, that is, to evaluate the morphological picture of the disease. However, this method is associated with certain risks and is an invasive procedure, so it is used less frequently.
Why is fatty liver disease dangerous?
Without treatment, liver steatosis threatens to develop severe complications. They are presented:
- fibrosis. As the cells die, they are gradually replaced by connective fibers, which is accompanied by scarring of the organ. Against this background, the functioning of the liver rapidly deteriorates;
- disruption of the production and movement of bile through the excretory ducts, as a result of which cholestasis develops and the digestion process is disrupted;
- steatohepatitis, which is characterized by inflammation of the liver tissue against the background of its fatty degeneration.
Separately, we should highlight cirrhosis, which is dangerous due to its manifestations. Against the background of protein deficiency, there is a deficiency of coagulation factors, which is fraught with massive bleeding. In addition, esophageal veins undergo varicose changes. They become crimped and their walls become thinner. The patient begins to experience severe swelling of the extremities. Fluid accumulates not only in tissues, but also in cavities (pleural, abdominal), which is accompanied by symptoms characteristic of pleurisy and ascites.
Provided proper treatment and compliance with all medical recommendations, it is possible to slow down the progression of the disease and significantly improve a person’s general condition.