Fatty liver hepatosis (steatosis) is a primary or secondary pathological syndrome that occupies a leading position in the general structure of hepatopathologies. The main reason for the development of this condition is a metabolic disorder, leading to excessive accumulation of lipids and subsequent degeneration of hepatic parenchyma cells.
Causes of fatty hepatosis
There are three main reasons for the development of hepatic steatosis:
- Obesity. If the body mass index exceeds 30, the likelihood of dystrophy is about 40%.
- Drinking alcoholic beverages. Moreover, hepatosis can occur even in people who drink a little, but every day. There is a direct relationship between the duration of alcohol consumption and the severity of liver dystrophy and, as a consequence, the risk of developing cirrhosis.
- Long-term use of medications with hepatotoxic effects.
Less commonly, hepatosis develops against the background of diseases that occur with metabolic disorders; this category includes hyperlipidemia, hypercholesterolemia, diabetes mellitus, thyrotoxicosis, myxedema, Itsenko-Cushing syndrome, malignant neoplasms, chronic diseases of the gastrointestinal tract, in which the absorption process is disrupted, etc. .
Liver dystrophy can be caused not only by obesity, but also by poor nutrition - overeating, abuse of fatty foods and foods containing hydrogenated fats and simple carbohydrates.
The disease is sometimes diagnosed in people who have a deficiency of enzymes involved in lipid metabolism (hereditary disease).
Most often, more than one factor leads to the development of steatosis. In most cases, there is a multifactorial factor, for example, the consumption of alcohol by a person who is eating poorly or taking toxic medications.
Drugs
Liver problems can develop for more than 10 years and not bother you at all. The average life expectancy with a diagnosis of cirrhosis is 9 years. Therefore, even if you have liver problems, you can fight them. There are about 1000 types of drugs used in hepatology. Therapy not only treats the disease itself, but also supports the liver in order to create the most favorable conditions for recovery. One of these groups of drugs are hepatoprotectors. Hepatoprotectors help restore metabolic processes in the liver, increase the organ’s resistance to destructive factors, normalize functional activity and stimulate regenerative processes in the liver.
Requirements for hepatoprotectors
Since the liver is the organ through which many substances are exchanged, drugs must not only be powerful, but also meet certain safety requirements, as well as:
- well absorbed;
- have a “first pass” effect through the liver;
- have the property of neutralizing or preventing the formation of substances that damage the liver;
- reduce the activity of inflammatory processes;
- slow down scar formation;
- help liver regeneration;
- do not cause rejection in case of liver pathology;
- extensive enterohepatic circulation;
- have no toxic effect.
Despite the fact that the requirements are known, the ideal drug has not yet been created. More than half of the presented products are of plant origin, the rest is divided between phospholipids, synthetic derivatives, organic preparations and amino acids.
Despite the fact that the requirements for liver drugs are known, the ideal one has not yet been created.
Classification
Based on etiology, hepatosis is divided into non-alcoholic fatty liver disease and alcoholic steatosis. The first type of disease is diagnosed in only 7–10% of cases.
Hepatosis occurs:
- primary - caused by metabolic disorders, for example, obesity or hyperlipidemia;
- secondary – due to the impact on the body of external negative factors, which subsequently lead to metabolic disorders, for example, fasting, long-term use of corticosteroids, intestinal resection.
Doctors also take into account the characteristics of fat deposition, according to which hepatosis is divided into:
- diffuse;
- zonal;
- focal disseminated;
- pronounced disseminated.
Why is NAFLD dangerous?
Fatty hepatosis, especially at the very beginning, can be practically asymptomatic, and the existing symptoms are not specific and, thus, make diagnosis difficult. However, you should not relax - diagnosing fatty hepatosis is important for any suspicion of the presence of this disease. Because this disease, developing gradually, practically without manifesting itself clearly, nevertheless increases the risk of cardiovascular death several times - in other words, it increases the risk of developing strokes and heart attacks.4 In addition, advanced fatty hepatosis can ultimately lead to ultimately, to the development of cirrhosis and liver failure. The likelihood of this event is low, however, if it occurs, the consequences can be fatal. The fact is that cirrhosis usually requires organ transplantation, which can be further complicated in the presence of cardio-metabolic disorders and diseases that often accompany fatty hepatosis.3
Stages of development of NAFLD
- 1
Stage of fatty hepatosis (steatosis)
The initial stage of the disease, often asymptomatic
- 2
Non-alcoholic steatohepatitis
Hepatosis with accompanying inflammation of liver cells
- 3
Fibrosis with further transition to cirrhosis
At this stage, liver tissue begins to be replaced by connective tissue, which leads to disruption of the structure and, ultimately, disruption of the organ.3
Symptoms of fatty liver disease
There are no specific signs of fatty liver hepatosis, even when there are already significant morphological changes. This is the insidiousness of the disease and lies a serious danger.
At the initial stage, the following nonspecific symptoms of fatty hepatosis may occur:
- general fatigue, asthenia, decreased ability to work;
- heaviness in the abdomen, stool instability, discomfort in the right hypochondrium, nausea, flatulence, sometimes vomiting;
- weight gain;
- causeless increase in body temperature for a long period of time;
- slight enlargement of the liver;
- skin itching.
As the disease progresses, icteric staining of the mucous membranes and skin is possible. Blood pressure often decreases and fainting occurs. There is a tendency to hemorrhages (increased bleeding).
There are 3 degrees of fatty hepatosis depending on the lesion:
- up to 33% – I degree;
- 33–66% – II degree;
- more than 66% – III degree.
List of medications
Groups of hepatoprotectors are divided depending on their composition.
Group I: milk thistle flavonoids can include both natural extracts from plants and those produced synthetically:
- Legalon;
- Karsil;
- Gepabene;
- Silimar.
These products contain a substance from milk thistle - silymarin (silibinin). It protects and stabilizes cell membranes. Milk thistle has a powerful antitoxic effect and can help with poisoning with toadstool. True, in this case a modification with intravenous administration is used. It also has antioxidant and metabolic effects and accelerates the regeneration of hepatocytes. The formation of scar tissue in the organ slows down.
Cholestasis, that is, obstructed outflow of bile, may be a contraindication for use. If this is ignored, drug congestion may worsen.
Usually the course of treatment is about 4 weeks, then take a break.
Group II: other flavonoids, except milk thistle:
- Katergen;
- Chophytol;
- LIV 52;
- Hepaliv.
Chophytol has a choleretic and hepatoprotective effect due to the content of artichoke leaf extract. It can also reduce the level of “bad” cholesterol in the blood if the level is initially high. The advantages of the drug include its low toxicity.
Liv 52 helps strengthen the liver's defenses against toxins and contains components widely used in Indian medicine. But the use of the drug in the acute inflammatory phase is unsafe and can increase inflammation. Therefore, it is recommended to use the drug when the regeneration phase is active and the liver needs support.
Group III: hepatoprotectors from animal organs:
- Hepatosan;
- Sirepar.
Hepatnosan – dried animal hepatocytes. In the intestines it absorbs toxins. Once digested, the nutritional components of the cells are absorbed and delivered to the liver. They work as protective factors at the level of liver cells and restore the activity of hepatocytes. The drug helps accelerate reparative processes.
Sirepar is a hydrolyzate of cattle liver extract. Contains 10 mg of cyanocobalamin per ml. Promotes liver regeneration and has a cleansing effect. It should not be used during the active phase of the disease, as the inflammatory process may intensify. It is taken for chronic hepatitis and cirrhosis, poisoning with toxins and drugs.
Some drugs should not be used during the active phase of the disease, as the inflammatory process may intensify.
Group IV: drugs containing essential phospholipids:
- Essentiale forte;
- Essliver forte;
- Phosphogliv forte.
Phospholipids, including phosphatidylcholine, are the most important component, from which most of the membranes of the liver cells themselves consist, like bricks. Phospholipids have been isolated and studied for almost 50 years, various experiments have been carried out. By restoring cell membranes, the liver normalizes its function. They are used for a very wide range of diseases. The course of treatment usually lasts about 3 months in the absence of contraindications and undesirable effects.
Funds from other groups not included in the first four:
- Lipoic acid;
- Hepa-mertz;
- Non-steroidal anabolics (methyluracil, sodium nucleinate);
- Ursofalk;
- Heptral.
From this group, we will analyze in detail Ursofalk, as a drug that is widely used among doctors. The active substance (ursodeoxycholic acid) helps protect the organ and has a choleretic effect. Used to dissolve gallstones. Reduces toxic effects on the epithelium of the bile ducts in the liver and hepatocyte membranes. Facilitates the removal of bile from the ducts, thereby facilitating the removal of toxins.
It has contraindications in the form of a non-functioning gallbladder, inflammatory bowel diseases, bile ducts, gallstones with a high calcium content (visible on an x-ray), in general, any conditions that will interfere with the increased outflow of bile from the liver. Also cirrhosis is in the stage of decompensation.
Diagnostics
Diagnosis of the disease is difficult. Firstly, steatosis has no specific symptoms. Secondly, biochemical tests do not show significant changes. Sometimes the activity of serum transaminases increases, but this indicator does not change in all patients with steatosis. In this regard, differential diagnosis with hepatitis, biliary tract obstruction, primary hemochromatosis, and hepatocerebral dystrophy is of primary importance.
The doctor makes the final diagnosis based on a comprehensive examination and a series of tests, including ultrasound and biopsy.
To find out the cause of fatty hepatosis, the level of insulin in the blood, serum glucose concentration, hormonal status, antibodies to cytomegalovirus and hepatitis viruses, markers of autoimmune hepatitis, etc. are determined.
Fatty liver
The article presents the epidemiology, pathophysiology, etiology, clinical signs, differential diagnosis and therapy of fatty liver. Particular attention is paid to the potential pathophysiological mechanisms of the development of fatty infiltration of the liver. Promising directions for the treatment of non-alcoholic steatohepatitis are analyzed, the mechanisms of action of drugs, their effect on biochemical and histological parameters are described.
Rice. 1. Progression of steatosis to cirrhosis – changes in the histological picture of liver tissue
Rice. 2. The influence of adipokines on the development of NAFLD (adapted from [8])
Rice. 3. Morphological criteria for NAFLD
Rice. 4. Characteristics of NASH depending on activity
Rice. 5. Potential pathophysiological directions for NASH therapy (adapted with modifications from [15])
Table. Drug therapy for NASH (adapted from [15] with addition)
Rice. 6. The mechanism of hepatoprotective action of the drug Rezalut® Pro
Fatty infiltration of the liver (liver steatosis, fatty hepatosis) is the accumulation of triglycerides and other fats in liver cells - hepatocytes. The content of fatty acids in hepatocytes depends on the balance between their intake and excretion. In some cases, fatty infiltration causes the death of hepatocytes and progresses to liver inflammation (steatohepatitis) with fibrosis progressing to cirrhosis (Fig. 1).
In Europe, the prevalence of steatosis is 20–30% in the general population and 3–10% in children. The prevalence of non-alcoholic steatohepatitis (NASH) reaches 5% [1]. In the United States, steatosis occurs in approximately 25–35% of the population.
Steatohepatitis may be associated with alcohol-induced or non-alcoholic liver damage. Fatty liver develops in 46–94% of people who abuse alcohol. Routine liver biopsy detects nonalcoholic steatohepatitis (NASH) in 1.2–9% of patients. Non-alcoholic fatty liver disease (NAFLD) develops in more than 80–94% of obese patients. Over 50% of patients undergoing bariatric surgery suffer from NAFLD [2].
A study in Northern Italy found the prevalence of steatosis to be 46.4% in heavy alcohol drinkers (>60 g/day) and 94.5% in obese heavy drinkers [3]. According to studies conducted in Asian countries, NASH and NAFLD can also develop in people with a low body mass index (BMI) [4].
According to the epidemiological study DIREG_L_01903, which included over 30 thousand patients in clinics, NAFLD was registered in 27% of patients in Russia. Non-alcoholic steatosis, steatohepatitis and cirrhosis were detected in 80.3, 16.8 and 2.9% of cases, respectively [5, 6].
Pathophysiology
Potential pathophysiological mechanisms of fatty liver infiltration include [7]:
- decreased activity of mitochondrial beta-oxidation of fatty acids;
- increasing the synthesis of endogenous fatty acids or increasing the delivery of fatty acids to the liver;
- insufficient incorporation or export of triglycerides into very low-density lipoproteins (VLDL).
Pathological changes in patients with alcoholic liver disease (ALD) can be divided into three groups:
- alcoholic fatty liver infiltration (primary steatosis);
- alcoholic hepatitis;
- cirrhosis caused by alcohol intake.
Alcoholic fatty liver disease is an early and reversible consequence of excessive alcohol consumption. It can develop in anyone who drinks more than 60 g of ethanol per day.
Currently, researchers are considering several mechanisms for the development of alcohol-induced fatty liver infiltration. Increases in hepatic glycerol-3-phosphate (3-GP) levels after ethanol ingestion are associated with an increase in the NADH/NAD+ ratio (the reduced/oxidized form of nicotinamide adenine dinucleotide) or an increase in NADH content in liver cells. The higher concentration of 3-GP is the result of improved fatty acid esterification. Increasing the supply of free fatty acids (FFA) to the liver also plays an important role in the development of fatty infiltration. Large amounts of alcohol increase lipolysis by directly stimulating the hypothalamic-pituitary axis and adrenal glands.
In addition, regular intake of alcohol suppresses the oxidation of fatty acids in the liver, which leads to an increased entry of VLDL into the blood. All these mechanisms contribute to the development of hepatic steatosis. Localization of steatosis in the centrilobular zone is the result of a decrease in energy reserves in hepatocytes due to relative hypoxia and changes in lipid metabolism, as well as changes in the redox reaction caused by the preferential oxidation of alcohol in the central zone.
Progress in studying the pathogenesis of alcoholic steatosis began after the role of peroxisome proliferator-activated receptors (PPAR-alpha), involved in the regulation of hepatic fatty acid metabolism, became clear. Blockade of PPAR-alpha, studied in animal models, as well as ethanol consumption contribute to the development of alcoholic fatty liver.
Serum leptin, a cytokine peptide hormone produced by adipocytes, occupies a special place in the development of steatosis. Hepatic steatosis develops when the effect of leptin decreases due to its deficiency or loss of stability. In patients with alcoholic liver disease, serum leptin levels correlate with the severity of steatosis.
Data from clinical studies support the proinflammatory role of tumor necrosis factor alpha (TNF-alpha) in the early stages of steatosis development, as well as in the progression of steatosis to steatohepatitis.
Visceral adipose tissue secretes a number of proteins—adipokines—that can affect liver function. FFAs play an important role in the development of primary steatosis. Under the influence of adipokines (TNF-alpha), primary hepatosis can progress to NASH with the induction of apoptosis and inflammation. In addition to adiponectin, which can prevent the development of NASH, liver cirrhosis, and even hepatocellular carcinoma (HCC), most adipokines have a negative effect on the course of liver diseases. Increasing BMI may increase the risk of many cancers, including HCC (Fig. 2) [8].
Etiology
The main risk factors for the development of fatty liver are [1]:
- metabolic syndrome (type 2 diabetes mellitus (DM) or impaired glucose tolerance, obesity, dyslipidemia, high blood pressure);
- polycystic ovary syndrome;
- excessive alcohol intake;
- fasting or rapid weight loss, including the effects of gastric bypass (presumably due to the rapid release of large amounts of FFA into the blood);
- parenteral nutrition;
- viral hepatitis B and C, human immunodeficiency virus;
- taking medications (amiodarone, tamoxifen, glucocorticosteroids, tetracycline, estrogens, methotrexate, thallium chloride, etc.);
- metabolic diseases (Wilson-Konovalov disease, glycogenosis; hereditary hemochromatosis, abetalipoproteinemia and hypobetalipoproteinemia; galactosemia, hereditary fructose intolerance; homocystinuria, Refsum disease, systemic carnitine deficiency, tyrosinemia, panniculitis).
Let us list the main risk factors influencing the development of ALD.
Minimum amounts of alcohol consumption associated with an increased risk of ALD range from 40 to 80 g/day over 10–12 years. Genetic factors play an important role in the development of alcoholism. Differences in genetic susceptibility to the development of ALD are mainly associated with structural differences in the main hepatic enzymes involved in alcohol metabolism, such as alcohol dehydrogenase, aldehyde dehydrogenase and cytochrome P-450 CYP4502E1.
The results of a number of studies demonstrate a high prevalence of antibodies to the hepatitis C virus in patients with ALD, as well as in patients with iron overload syndrome.
Obesity and eating habits also influence individual susceptibility to ALD.
Fatty infiltration of the liver can form in patients of all age groups. When it comes to alcoholic steatosis, depending on a person's age, the liver handles alcohol differently. Thus, with age, the toxicity of alcohol increases due to the body’s increased susceptibility. It is believed that this phenomenon is associated with an age-related defect in mitochondrial transport, as well as a decrease in the function of the smooth endoplasmic reticulum and CYP2E1-dependent microsomal ethanol oxidation.
NAFLD is the most common liver disease among adolescents in the United States. Older patients are more likely to develop more severe forms of liver damage. NASH is the third most common chronic liver disease (after hepatitis C and alcohol) in US adults. NASH is probably currently the leading cause of minor elevations in transaminase levels. It has been established that NASH occurs six months after liver transplantation in children and adults [7].
Unlike men, women develop more severe forms of ALD when drinking lower doses of alcohol. Women's increased susceptibility to alcohol may be due to differences in hepatic alcohol metabolism, cytokine production, and gastrointestinal alcohol metabolism. In initial studies involving women with alcoholism, the percentage of patients with NAFLD exceeded 75%, but in subsequent studies it decreased to 50%.
Clinical signs
Drinking moderate or large amounts of alcohol over a short period of time can cause fatty liver disease. Alcohol-induced steatosis is usually asymptomatic. Sometimes severe forms of fatty liver cause general malaise, weakness, anorexia, nausea and abdominal discomfort. Jaundice is present in 15% of hospitalized patients with evidence of fatty liver disease.
A thorough history, especially regarding the amount of alcohol consumed, is very important to determine its role in the etiology of abnormal liver test results. Information received from family members allows us to identify the range of “alcohol” problems. Liver toxicity associated with medications, especially over-the-counter medications, and alternative treatments should be excluded.
Symptoms of liver disease, such as ascites, edema, and jaundice, may occur in patients with cirrhosis that develops as a result of progression of NASH.
Complications of fatty liver
In some cases, prolonged alcohol consumption leads to alcoholic hepatitis or liver cirrhosis. There is an increase in mortality and risk of liver cancer among patients diagnosed with alcoholic fatty liver disease.
In patients with non-alcoholic fatty liver disease, steatohepatitis can progress to cirrhosis with complications (visceral bleeding, ascites, encephalopathy and liver failure). The rate of progression increases with the presence of more than one liver disease (eg, ALD or chronic viral hepatitis). Diabetes and hypertriglyceridemia sometimes lead to the development of liver fibrosis [7].
Differential diagnosis
Differential diagnosis of fatty liver infiltration is carried out with the following diseases:
- alcoholic hepatitis;
- alcoholism;
- alpha-1 antitrypsin deficiency;
- autoimmune hepatitis;
- celiac disease;
- cirrhosis;
- drug-induced hepatotoxicity;
- hemochromatosis;
- hepatitis A, B, C, D, E;
- hyper- and hypothyroidism;
- malabsorption;
- primary biliary cirrhosis;
- primary sclerosing cholangitis;
- enteropathy with large protein loss;
- vitamin A toxicity;
- Wilson-Konovalov disease.
A definitive diagnosis can only be made after liver biopsy and histopathological tests [8]. Attempts are being made to find non-invasive markers of the disease that would allow us to distinguish the stages of liver fibrosis and differentiate fibrosis from NASH and NASH from simple steatosis [9, 10].
Laboratory and instrumental diagnostics
Fatty infiltration is characterized by the following changes in laboratory parameters:
- an increase in the activity of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) by no more than 4–5 times, the AST/ALT index is no more than 1, an increase in ALT activity is more often observed;
- an increase in the activity of alkaline phosphatase (ALP) and gamma-glutamyl transpeptidase (GGTP), usually no more than twice the normal level;
- hypertriglyceridemia, hypercholesterolemia;
- hyperglycemia (impaired glucose tolerance or type 2 diabetes);
- hypoalbuminemia, increased bilirubin levels, thrombocytopenia, increased prothrombin time in patients with advanced stages of NAFLD.
Hepatocellular failure develops only in liver cirrhosis, but hypoalbuminemia in NASH occurs in patients with diabetic nephropathy. Hypergammaglobulinemia and antinuclear antibodies are detected in 10–25% of patients. It should be noted that in patients with NAFLD with histologically verified fatty degeneration without inflammation and damage to hepatocytes, there are practically no clinical and laboratory signs of liver disease. The main differential difference between fatty degeneration and NASH, available in clinical practice, may be the severity of the biochemical cytolysis syndrome. When analyzing laboratory data obtained in specialized clinics, cytolysis is described in 50–90% of NASH patients. More often, ALT activity is higher than AST, but sometimes, especially in patients with transformation into cirrhosis, AST activity is higher. Unlike liver lesions of a different nature, cytolysis in NASH is constant, although fluctuations in ALT levels cannot be ruled out.
The degree of hypertransaminasemia does not correlate with the severity of steatosis and liver fibrosis. The AST level, along with other metabolic factors, is an indicator of insulin resistance. These changes suggest the possibility of using this indicator as an additional marker in patients with insulin resistance. At the same time, a low serum ALT level in combination with a high BMI may indicate the presence of severe fibrosis in NASH. The absence of changes in laboratory parameters characterizing the functional state of the liver (ALT, AST, ALP, GGTP) does not exclude the presence of an inflammatory-destructive process and liver fibrosis.
NASH is characterized by apoptosis of hepatocytes. In late stages of the disease, activated caspases (specifically caspase-3 and caspase-7) cleave the hepatic filament protein cytokeratin-18 (CK-18). Measuring the amount of CD-18 fragments using the immunochemiluminescent method in the blood allows us to differentiate NASH from steatosis and the absence of changes in the liver tissue. The concentration of CK-18 fragments > 395 U/L may indicate the presence of NASH. The specificity and sensitivity of the method are 99.9 and 85.7%, respectively. Increased caspase activity in the blood is an informative predictor of NASH. Moreover, the degree of apoptosis correlates with the severity of steatohepatitis and the stage of fibrosis. The formation of antibodies to caspase-formed CK-18 fragments is an indicator of early cell apoptosis [11]. This non-invasive diagnostic method can assist clinicians in selecting patients for liver biopsy, determining the severity of histological changes in patients with NAFLD, and assessing disease progression and response to treatment.
Recently, with the development of laboratory research methods, a set of computational tests has appeared to determine the degree of histological activity in the most common forms of liver diseases. Such tests include FibroMax. It is represented by five calculation algorithms:
- FibroTest, including ActiTest: liver fibrosis is diagnosed, displaying the stage of fibrosis (F0–4) and the degree of necroinflammatory process (A0–3) according to the international METAVIR system;
- SteatoTest: fatty liver degeneration (liver steatosis) is diagnosed mainly due to disturbances in the levels of ALT and GGTP;
- AshTest: ASH is diagnosed in people who abuse alcohol;
- NashTest: Diagnoses NASH in patients with excess body weight, insulin resistance, diabetes mellitus or hyperlipidemia.
When conducting tests, mathematical formulas are used to check each parameter. Each parameter separately serves as an indicator of the condition of the liver. The calculations also take into account the age, weight, height and gender of the patient.
Diagnostic tests make it possible to obtain an accurate quantitative and qualitative assessment of fibrosis, steatosis and necroinflammatory changes in the liver at all stages, regardless of location.
FibroTest, SteatoTest and NeshTest are used for non-invasive diagnosis of NAFLD.
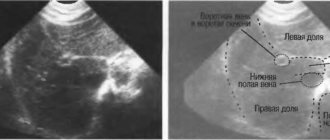
If the patient is asymptomatic, liver function tests are abnormal, and histological examination of the liver tissue is not available, ultrasound can be an inexpensive and reliable method for diagnosing hepatic steatosis, especially in the presence of one or more risk factors for NASH. In addition, ultrasound allows you to monitor the dynamics of the disease.
There are four main ultrasound signs of liver steatosis:
- distal echo attenuation;
- diffuse hyperechogenicity of the liver parenchyma (“bright liver”);
- increased echogenicity of the liver compared to the kidneys;
- blurred vascular pattern.
The gold standard for diagnosing and staging NAFLD remains a liver puncture biopsy, since the main liver tests used in clinical practice are nonspecific and do not always correlate with histological changes (damage, inflammation, fibrosis).
Mandatory indications for biopsy:
- age over 45 years and cytolysis of unknown etiology;
- a combination of cytolysis of unknown etiology with at least two manifestations of metabolic syndrome, regardless of age.
Liver biopsy is not indicated in cases where serum aminotransferase levels are normal. Morphological examination allows us to determine the degree of NASH activity and the stage of liver fibrosis. Using the E. Brunt classification [12], it is possible to verify NAFLD more accurately and make a differential diagnosis of NASH with other diffuse liver lesions, including severe ASH (Fig. 3).
E. Brunt's classification allows one to assess the degree of steatosis, the activity of inflammation and the stage of liver fibrosis based on the severity of morphological signs, which is very important for making a diagnosis by a practicing physician (Fig. 4).
Therapy for NAFLD
In most patients, NAFLD is characterized by a long-term, stable, asymptomatic course. Based on modern concepts, special pharmacotherapy is indicated only for patients with a progressive course of the disease or a high risk of its development. Obesity, type 2 diabetes, hyperlipidemia are the main conditions associated with the development of NAFLD. Therefore, treatment and/or prevention of such conditions should be aimed [13]:
- to prevent progression of the disease to the stage of liver cirrhosis and hepatocellular failure;
- reducing the severity of insulin resistance;
- decreased activity of serum transaminases;
- reducing the severity of liver steatosis;
- improving quality of life.
For successful treatment of NAFLD, modification of the patient’s lifestyle, especially weight loss in obesity, is extremely important. The patient should be warned about the undesirability of complete fasting, as well as the imposition of ileojejunal anastomosis. The fact is that rapid weight loss (500–1000 g per week) aggravates the manifestations of NASH. It is advisable to combine balanced diet therapy with restriction of fats and carbohydrates and adequate physical activity. It is also necessary to completely stop drinking alcohol.
Drug therapy is indicated if the patient has histologically confirmed NASH. US guidelines for the treatment of NAFLD suggest the use of vitamin E because there is evidence that it may improve liver histology. The possibility of treating patients with biopsy-proven NASH with pioglitazone is being considered. However, it should be noted that the long-term efficacy and safety profile of therapy were not assessed in the majority of patients participating in clinical trials involving the treatment of NASH with pioglitazone [14].
In Fig. Figure 5 presents the potential pathophysiological effects of NAFLD therapy currently being studied. The development of hepatic steatosis and steatohepatitis is a multimodal process, so several treatment methods are being studied - thiazolidinedione therapy, diet, exercise, and the use of rimonabant, which can have pleiotropic effects in the treatment of NAFLD.
Table [15] presents medications that can currently be used in the treatment of NASH. It should be noted that drug treatment methods for NASH continue to improve.
According to Russian recommendations for the diagnosis and treatment of NAFLD, therapy is selected taking into account the impact of risk factors on the disease. For drug therapy of NAFLD it is proposed to use:
- drugs for weight loss (orlistat);
- drugs that increase insulin sensitivity (metformin);
- essential phospholipids;
- ursodeoxycholic acid;
- ademetionine;
- vitamin E.
For the treatment of conditions accompanying NAFLD, it is advisable to use lipid-lowering (statins) and antihypertensive (hydrophilic angiotensin-converting enzyme inhibitors) drugs.
In recent years, particular importance has been attached to the use of drugs that combine hepatoprotective and hypocholesterolemic effects in patients with NAFLD. Such a drug is Rezalut® Pro. The mechanism of its hepatoprotective action is presumably provided by the incorporation of polyunsaturated phospholipids (PL) into defects in the hepatocyte membrane, which helps restore the structure of liver cells (Fig. 6). In this way, the transport of substances across the cell membrane is normalized and the function of hepatocytes is restored.
In addition to the hepatoprotective effect characteristic of all drugs based on PL, the drug Rezalut® Pro is characterized by a hypocholesterolemic effect. Its achievement was made possible by optimizing the composition of the drug. The composition of the drug Rezalut® Pro includes polyunsaturated fatty acids - linoleic acid - omega-6 and linolenic acid - omega-3 in a ratio of 10:1.
The results of studies of the drug Rezalut® Pro confirmed the properties of essential FL: during therapy, the manifestations of cytolytic syndrome in patients with NASH decreased. In addition, the presence of this additional property allows us to recommend the hepatoprotector Rezalut® Pro as a hypocholesterolemic agent for patients with high cholesterol levels in the blood [16].
Rezalut® Pro is a representative of the latest generation of phospholipid drugs. It is produced using modern technology: a full cycle of oxygen-free production and packaging in sealed capsules. This allows you to preserve all the specified beneficial properties of FL and avoid the addition of dyes, stabilizers and flavors. In this case, the drug exhibits the basic properties of essential PL. According to accumulated clinical and experimental data, phospholipids:
- form the lipid bilayer of cell membranes, determining membrane properties such as fluidity and flexibility, thereby ensuring the permeability and barrier functions of cell membranes;
- are able to directly integrate into the structure of cell membranes, replacing defects;
- participate in normalizing the lipid profile and reducing fatty infiltration of hepatocytes;
- have an antioxidant effect (able to block free radicals by breaking double bonds);
- stabilize the physicochemical properties of bile;
- have an antifibrotic effect due to the effect on stellate (collagen-producing) cells of the liver (the introduction of phospholipids reduces the level of activation of stellate cells and, consequently, the production of procollagen);
- have anti-inflammatory properties: they reduce the level of activation of Kupffer cells and increase the synthesis of anti-inflammatory cytokines - interleukin-1b and TNF-alpha.
The presented methods for treating fatty liver and NASH are aimed at the main factors in the development of this disease. Treatment of NAFLD is aimed at eliminating or reducing insulin resistance, oxidative stress, diabetes mellitus, hyperlipidemia, obesity and liver fibrosis. The main treatments include diet, exercise, surgery and medication. Although there is no cure-all for NAFLD, comprehensive treatment can be effective.
Thus, early diagnosis of fatty liver and identification of risk factors for unfavorable course of the disease are extremely important when choosing an adequate treatment method that prevents further progression of the disease to NAFLD. In this regard, all patients with metabolic syndrome who are at high risk of developing NAFLD and especially NASH should be examined to assess the condition of the liver. The most informative methods for such assessment are liver ultrasound with biopsy. The main directions in the treatment of fatty liver are weight loss through lifestyle changes, therapy using insulin sensitizers, hepatoprotectors with antioxidant and hypocholesterolemic effects (for example, the drug Rezalut® Pro).
Treatment of fatty hepatosis
Treatment of fatty hepatosis is usually complex, including diet therapy, drug therapy and physical therapy.
Diet plays an important and sometimes paramount role in the treatment of steatosis. Sometimes, to cure the first stage, it is enough to follow a diet. Thanks to a significant limitation of fat consumption, healthy cells, and there are more than 66% of them, independently remove the fat present in the liver. But even in the later stages, nutritional correction is a prerequisite. It is recommended to steam food, eat more greens, vegetables and low-fat dairy products, eggs, cereals, and vegetarian dishes.
The cause of its occurrence directly affects how fatty hepatosis is treated.
Weight loss is a necessary condition for obese patients. As a rule, this helps to get rid of insulin resistance, which leads to normalization of carbohydrate and lipid metabolism. But there is one important nuance here - you should not lose weight too quickly (up to 600 g per week is allowed), otherwise there is a risk of progression of fatty hepatosis.
For alcoholic fatty degeneration, successful treatment is only possible with complete abstinence from alcohol. Patients are recommended to consult a narcologist.
Lipotropic drugs for fatty hepatosis are prescribed to accelerate the removal of fat from the liver. This category includes drugs that normalize cholesterol and lipid metabolism, promote fat oxidation and its mobilization from the liver: lipoic acid, essential phospholipids, folic acid, B vitamins.
To prevent the destruction of cell membranes and stimulate the regeneration of hepatocytes, hepatoprotective drugs are prescribed for fatty liver hepatosis: betaine, taurine, ursodeoxycholic acid, glutargin, phosphatidylcholine,
Tablets containing ursodeoxycholic acid often prescribed for fatty hepatosis: Livodexa, Grinterol, Urdoxa, Ursodez, Ursoliv, Ursofalk, Exchol, Ekurochol.
Thiazolidinediones and biguanides are used to eliminate insulin resistance.
The utilization of fatty acids is improved by physical exercise, so it is recommended for all patients with this disease.
Dietary recommendations
There is no diet that suits everyone without exception. Patients with fatty hepatosis first of all need to reduce the calorie content of their daily diet. One of the recommendations may be advice on limiting the consumption of foods rich in saturated fatty acids and replacing them with foods containing monounsaturated or polyunsaturated fats (milk, olive oil, fish oil).
Nutritional balance
The main parts of food are proteins, fats, carbohydrates, water, minerals and vitamins, which must be strictly balanced. The ratio between proteins, fats and carbohydrates should be 1:1:4.
Animal proteins should make up about 60% of the total protein. Of the total fat, 20-25% should be vegetable oils as a source of polyunsaturated fatty acids.
The balance of carbohydrates is expressed in the ratio of starch, sugar, fiber and pectin. Sugars should be represented by fruits, berries, dairy products, and honey. It is extremely important to maintain a balance of vitamins and minerals, which must be supplied to the body daily in accordance with daily requirements.
Diet
This is the number of meals and the interval between them during the day. For healthy people 3-4 times a day at 4-5 hour intervals. For some concomitant diseases, such as obesity, it is necessary to eat 5-6 times a day.
Nutrition for liver diseases
The diet for fatty hepatosis should be gentle and create maximum liver rest. It is necessary to reduce the amount of fat and enrich the diet with foods that are sources of complete proteins and vitamins, reduce the sugar content and increase the amount of fluid. Meals should be frequent and in small portions. It is necessary to exclude fatty meats, smoked meats, spices, spicy, rich dough. Alcohol is absolutely prohibited.
To find a diet that is right for you, consult your doctor.
up
Fatty hepatosis of pregnant women
Separately, there is hepatic steatosis, which occurs without a significant cause in women bearing a child. Acute fatty hepatosis of pregnancy is diagnosed in one out of 13,000 women. 20–25% of cases end in death, according to foreign authors, and up to 60%, according to domestic sources.
The disease progresses quickly, over 2–3 weeks. Occurs mainly in late pregnancy - 32–36 weeks. The exact cause of this pathology has not yet been established.
Symptoms that may indicate acute fatty hepatosis in pregnant women: excessive vomiting, severe nervous disorders, general weakness, drowsiness.
The only treatment method is emergency delivery. Within 5 weeks after birth, the disease regresses.
Prevention
Preventive measures include:
- proper nutrition, in particular limiting fatty, spicy, fried and smoked foods;
- moderation in the consumption of alcoholic beverages;
- taking medications correctly;
- regular physical activity.
Fat accumulation is often caused by excess weight due to a sedentary lifestyle. Scientists have proven that if you eat only fast food for 4 weeks, this disease will almost certainly occur. Student volunteers took part in the experiment. Moreover, the first signs appeared after 1 week of such nutrition. Therefore, nutrition and weight control are of great importance.
For prevention, hepatoprotectors should be used, especially during periods of increased load on the liver, for example, with prolonged alcohol consumption, antibiotic treatment, and following a diet aimed at weight loss.
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Ultrasound of the abdominal organs (liver, gall bladder, pancreas, spleen) | 3 800 |
| Liver elastography (shear wave method) | 4 000 |
| MSCT of the abdominal cavity and retroperitoneal space of the abdomen | 6 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Frequently asked questions about fatty liver disease
Which doctor should I contact?
A hepatologist specializes in liver diseases.
How to determine fatty hepatosis?
Unfortunately, the disease has no specific symptoms. A comprehensive examination allows you to identify deviations.
Can hepatic steatosis be cured?
With proper and timely therapy, changes in the liver are reversible. The main thing is to strictly follow all the doctor’s instructions, stick to your diet, and give up alcohol and “harmful” foods.