Compound
One Bisoprolol tablet contains 0.005 or 0.01 g of bisoprolol fumarate , as well as auxiliary components: magnesium stearate, colloidal silicon dioxide, crospovidone, corn starch (Amylum maydis), microcrystalline cellulose (Cellulose microcrystalline).
For the manufacture of film coating tablets, the following are used: polyvinyl alcohol, titanium dioxide, talc, macrogol, dyes (iron oxide yellow, quinoline yellow, orange yellow).
pharmachologic effect
Bisoprolol (INN - Bisoprolol) belongs to the clinical-pharmacological group “ β1-blockers ”. Its action is aimed at relieving the symptoms of myocardial ischemia (antianginal effect), normalizing the disturbed rhythm of contractions of the heart muscle (antiarrhythmic effect), as well as reducing blood pressure (antihypertensive effect).
Pharmacodynamics and pharmacokinetics
Bisoprolol is a selective β1-blocker and does not have intrinsic sympathomimetic or membrane-stabilizing activity.
Under the influence of low doses of the active substance bisoprolol fumarate in a patient:
- the activity of blood plasma renin (regulating blood pressure and water-salt homeostasis of the proteolytic enzyme) decreases;
- myocardial oxygen demand decreases;
- the excitability and conductivity of the myocardium decreases;
- the frequency of contractions of the heart muscle decreases (both at rest and when under load);
- stimulated catecholamine and the formation of cyclic adenosine monophosphate from adenosine triphosphate ;
- the flow of calcium ions into the intracellular space decreases;
- cardiac output decreases (despite the fact that there is no significant decrease in stroke volume);
- atrioventricular (AV) conduction is inhibited;
- pressure decreases;
- symptoms of myocardial ischemia are relieved.
According to the abstract, Bisoprolol in a dosage significantly higher than the therapeutic one (0.2 grams or more) can cause blockade, including β2-adrenergic receptors, mainly in the bronchi and smooth muscles of the vascular walls .
The drug is absorbed by approximately 80-90%, and the level of absorption does not depend on food intake. The concentration of the active substance in plasma reaches its maximum value 60-180 minutes after taking the tablet.
Bisoprolol fumarate is approximately 30% plasma proteins The substance has the ability to a small extent:
- pass through the placental and blood-brain barriers ;
- penetrate into the milk of a nursing woman.
Approximately half of the dose taken is metabolized in the liver , resulting in the formation of inactive metabolites . The half-life varies from 10 to 12 hours. About 98% is eliminated from the body unchanged in the urine, up to 2% is excreted in bile.
Research results
According to the results of the SDS test, the use of therapy with bisoprolol led to an increase in the duration of development of SDS at the minimum limit of the synchronization range (by 20.9%); a decrease in the synchronization range (by 18.8%) and the RAS index (by 46.3%). These changes indicate a decrease in ASD. As a result of taking sotalol, patients experienced a decrease in the synchronization range (by 9.4%) and the RAS index (by 12.7%); there was no significant change in the duration of development of SDS at the minimum border of the synchronization range. Thus, these changes show a less pronounced decrease in RAS when taking sotalol compared to that in the bisoprolol group (Table 2).
According to the results of echocardiography, during the use of therapy with bisoprolol, the peak velocity of the transmitral diastolic flow E (VE) increased (by 7.8%), the ratio of VE and the peak velocity of the transmitral diastolic flow A (VA) (VE/VA) (by 18.2 %), peak velocity of LV base elevation in early diastole (Ve′) (by 21.1%), deceleration time of transmitral diastolic flow E (DTE) (by 25%); the end-diastolic size (EDD) of the LV decreased (by 7.6%), the anteroposterior size of the left atrium (LA) (by 5.6%), the ratio of VE and Ve′ (VE/Ve′) (by 17.6% ), VA (by 12.6%); LVEF, interventricular septal thickness (IVS) and posterior wall thickness (PV) were not subject to significant changes. The listed changes indicate an improvement in the structural and functional parameters of the myocardium. As a result of therapy with sotalol, VE (by 8.4%), VE/VA (by 20%), Ve′ (by 18.5%), DTE (by 31.7%) increased; LV EDV decreased (by 4.6%), LA anteroposterior size (by 2.4%), VA (by 9.7%), VE/Ve′ (by 20.5%); LVEF, LV PV thickness, and IVS thickness did not change significantly. These changes demonstrate regression of cardiac remodeling processes, which is comparable to that under the action of bisoprolol (Table 3). In both groups, LV isovolumetric relaxation time (IVRT) increased comparablely.
According to the results of the treadmill test, during therapy with bisoprolol, the maximum load increased (by 11.9%), and the double product decreased (by 17.1%). During sotalol therapy, the maximum load increased (by 14.6%) and the double product decreased (by 16.3%). Thus, both pharmacological treatment regimens increased exercise capacity to the same extent.
According to the results of TSHM, patients taking bisoprolol as part of combination drug therapy showed an increase in the distance traveled (by 14.5%). In 30% of patients there was a decrease in FC of CHF from II to I, in 8% of cases CHF was not registered. Therapy with sotalol led to an increase in the distance traveled (by 16.3%); in 30% of patients the FC of CHF decreased from II to I, in 10% of cases CHF was not registered. Thus, both regimens of pharmacological therapy comparablely reduced the FC of CHF (Table 4).
According to the BP data, target blood pressure values were achieved in 87% of patients taking bisoprolol and in 83% of those taking sotalol.
According to the results of the SM ECG, the use of bisoprolol as part of combined pharmacological therapy made it possible to achieve a decrease in the average heart rate (HR) (by 18.2%), SVT paroxysms (by 69.1%) and the number of supraventricular extrasystoles (by 62.8%). During therapy with sotalol, the average heart rate (by 21.5%), the number of paroxysms of SVT (by 76.4%) and supraventricular extrasystoles (by 79.3%) decreased. The results obtained demonstrate targeted and comparable antiarrhythmic efficacy of combined pharmacological therapy in both groups.
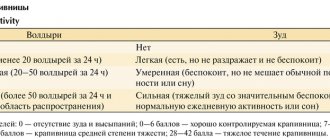
According to the QOL questionnaire for patients with arrhythmia, the sum of negative scores as a result of therapy using bisoprolol decreased by 33%, and during therapy with sotalol - by 47.5%. Obviously, therapy using sotalol improved the quality of life of patients more significantly than using bisoprolol (Table 5).
When using bisoprolol as part of combination pharmacotherapy, side effects occurred in 13% of cases: erectile dysfunction (n=1), dry cough (n=1), drowsiness (n=1), dyspepsia (n=1). During therapy with sotalol, side effects were observed in 17% of cases: dry cough (n=2), drowsiness (n=2), dyspepsia (n=1). These manifestations were mild and transient in nature, which did not require exclusion of patients from the study or discontinuation of therapy.
Contraindications
The use of Bisoprolol is contraindicated in:
- hypersensitivity to the components of the drug;
- hypersensitivity to other β-blockers ;
- acute heart failure (AHF);
- CHF in the stage of decompensation (if the patient requires inotropic therapy);
- shock (including cardiogenic shock);
- syndrome of weakness (dysfunction) of the sinus node;
- pulmonary edema;
- sinoatrial blockade;
- bradycardia (extremely low heart rate, in which the heart rate does not exceed 60 beats per minute);
- 2nd and 3rd degree AV block without pacemaker;
- severe form of arterial hypotension , in which the systolic blood pressure does not exceed 100 mm Hg. Art.);
- severe bronchial asthma;
- noted in the history of COPD ;
- pheochromocytoma (in cases where the patient is not simultaneously prescribed α-blockers );
- poorly controlled diabetes mellitus ;
- metabolic acidosis;
- peripheral circulatory disorders in late stages (for example, with Raynaud's syndrome );
- refractory hypokalemia , hypercalcemia , or hyponatremia ;
- hypolactasia;
- lactase deficiency;
- glucose-galactose malabsorption syndrome.
Due to the fact that there is not enough data on the safety and effectiveness of the drug for patients under 18 years of age, Bisoprolol is not used in pediatrics.
In addition, the drug is not prescribed to patients who are undergoing treatment with MAO inhibitors (with the exception of cases when the patient is prescribed B-type monoamine oxidase inhibitors ).
Possibilities of bisoprolol in the treatment of cardiovascular diseases
In real clinical practice, beta-blockers (BABs) are one of the most widely used drugs in the treatment of cardiovascular diseases (CVD). The issues of choosing BAB still remain relevant.
As is known, beta-1-selective ABs are superior to non-selective ones: they significantly less increase peripheral vascular resistance, to a greater extent reduce the severity of the vasoconstrictor response to catecholamines and, therefore, are more effective in smokers, less likely to cause hypoglycemia in patients with diabetes mellitus (DM), less often cause withdrawal syndrome. Beta-1-selective ABs can be used in patients with obstructive pulmonary diseases; they change the lipid composition of the blood to a lesser extent.
One of the most highly cardioselective beta blockers is bisoprolol (Bidop). The affinity of bisoprolol for beta-1 adrenergic receptors is 75 times higher than for beta 2 adrenergic receptors. In a standard dose, the drug has almost no blocking effect on beta-2 adrenergic receptors and is therefore devoid of many undesirable effects. Bisoprolol in therapeutic dosages (2.5–10.0 mg/day) does not cause bronchospasm and does not impair respiratory function in people with chronic obstructive pulmonary disease (COPD). In addition, bisoprolol does not worsen renal function and intrarenal hemodynamics, does not affect carbohydrate metabolism and does not increase the content of cholesterol and lipoproteins in the blood plasma [1].
These properties determine the use of bisoprolol for various CVDs, primarily for arterial hypertension (AH) and coronary heart disease (CHD).
Benefits of bisoprolol for arterial hypertension
The main indications for the use of beta blockers in patients with hypertension are: coronary artery disease, a history of myocardial infarction, chronic heart failure (CHF), tachyarrhythmias, glaucoma [2].
In terms of antihypertensive activity, bisoprolol is not inferior to other beta blockers and is superior to them in a number of indicators. The double-blind randomized BISOMET trial showed that bisoprolol, like metoprolol, reduces blood pressure (BP) at rest, but is significantly superior to metoprolol in its effect on systolic blood pressure and heart rate (HR) during exercise [3]. The pronounced effectiveness of bisoprolol in patients leading an active lifestyle encourages the drug to be prescribed to younger patients with hypertension.
In this regard, we should recall the myths about the effect of beta-blockers on erectile function. Taking beta blockers is often associated with the possibility of sexual dysfunction. With regard to bisoprolol, the absence of a negative effect on sexual function in men has been convincingly proven. This property of bisoprolol increases adherence to treatment in young male patients who begin to suffer from hypertension in the active years of life. In a study by LM Prisant et al. demonstrated that the incidence of sexual dysfunction when taking bisoprolol did not differ from that when taking placebo [4].
When comparing bisoprolol with calcium antagonists (nifedipine) and angiotensin-converting enzyme inhibitors (ACEIs) (enalapril), it was found that it has no less antihypertensive activity. Moreover, in a comparative randomized study, bisoprolol (10–20 mg/day) led to a significant decrease in left ventricular myocardial mass index (LVMI) by 11%, which was identical to the effect of ACEI (enalapril, 20–40 mg/day) [5] .
Another study examined the effectiveness of bisoprolol in doses of 5–10 mg in patients with hypertension and left ventricular hypertrophy (LVH). After 6 months, the LVMM index significantly decreased by 14.6%, the myocardial thickness of the posterior wall of the left ventricle (LV) and interventricular septum by 8% and 9%, respectively, and the volume of cavities and LV ejection fraction did not change. At the same time, the regression of LV hypertrophy could not be explained by the hypotensive effect alone; in 5 patients who did not reach normal blood pressure values, a decrease in LVMM indices was also noted [6].
Assessment of organoprotective properties, including the effect of various antihypertensive drugs on arterial wall stiffness, is currently the subject of active study and debate. Taking into account the discovery of new markers of cardiovascular risk, we present data on the effect of bisoprolol on central pressure, pulse pressure and vascular wall stiffness. The stiffness of the vascular wall is one of the main factors determining pulse blood pressure. Both vascular wall stiffness and pulse pressure are highly correlated with endpoints such as cardiovascular mortality, myocardial infarction, and stroke. Central, or aortic, pulse pressure has an even closer relationship with cardiovascular risk [7].
Bisoprolol at a dose of 10 mg in patients with hypertension led to a significant decrease in pulse wave velocity, as well as an improvement in the elasticity of the brachial artery.
The ADLIB study examined the effects of different classes of antihypertensive drugs (amlodipine 5 mg, doxazosin 4 mg, lisinopril 10 mg, bisoprolol 5 mg and bendroflumethiazide 2.5 mg) on measures of vascular stiffness - central pressure, reflected wave and augmentation index. The most pronounced decrease in blood pressure in the brachial artery was caused by lisinopril and bisoprolol. Bisoprolol, along with lisinopril and amlodipine, reduced central blood pressure. At the same time, bisoprolol had the opposite effect on the augmentation index and reflected wave speed: the augmentation index was higher when using other drugs, and the reflected wave speed was maximum when treated with bisoprolol [8].
It is impossible not to dwell on aspects of the treatment of hypertension in obese patients. Hypertension is diagnosed in 88% of patients with abdominal obesity [9].
Despite the fact that beta blockers belong to the main class of drugs in the treatment of hypertension, obesity and metabolic syndrome are not the primary indication for their use, although the use of beta blockers in obese patients has a pathogenetic justification, given the key role of hyperactivity of the sympathetic nervous system in the development of hypertension in obesity.
The fear of prescribing beta blockers to a patient with metabolic syndrome is due to fears of worsening the course of diabetes. BAs have different prodiabetogenic potential. Thus, while taking bisoprolol and nebivolol in patients with hypertension and diabetes, there was no change in blood glucose levels, while treatment with atenolol led to a significant increase in its level. It was found that bisoprolol does not change blood glucose levels in patients with diabetes, and no dose adjustment of hypoglycemic agents is required, which indicates its metabolic neutrality [10].
Studies involving patients with diabetes, conducted with bisoprolol, have shown that, due to its high selectivity, the drug does not have a significant effect on carbohydrate and lipid metabolism and can be used in patients with diabetes.
A positive property of bisoprolol for use in obese patients with hypertension is its unique ability to dissolve in both fats and water (amphiphilicity). Due to its amphiphilic properties, bisoprolol undergoes 50% biotransformation in the liver, the rest is excreted unchanged by the kidneys. Considering the frequent presence of a “compromised” liver in patients with metabolic syndrome in the form of non-alcoholic fatty liver disease, the use of bisoprolol is justified for the treatment of hypertension in this category of patients. Amphiphilicity determines the balanced clearance of bisoprolol, which explains the low likelihood of its interaction with other drugs and greater safety when used in patients with moderate hepatic or renal insufficiency [11].
Polymorbidity and the presence of both COPD and CVD in one patient forces a careful approach to the choice of beta blockers. It has been established that the administration of beta blockers to patients with COPD who have suffered a myocardial infarction reduces the risk of mortality by 40% (compared to a similar group of patients without the use of beta blockers). According to S. Chatterjece, in patients with bronchial asthma, changes in bronchial patency when taking 10 and 20 mg of bisoprolol did not differ significantly from those after placebo [12].
The cardioselective beta blocker bisoprolol in patients with CVD and concomitant COPD does not have a negative effect on bronchial patency and improves the quality of life of patients, while the less selective atenolol and metoprolol worsened airway patency in this category of patients [13].
The use of bisoprolol in various forms of ischemic heart disease
Domestic recommendations for the diagnosis and treatment of coronary artery disease [14] consider beta blockers as first-line drugs for the treatment of various forms of coronary artery disease, including serving as a necessary component in the treatment of patients with a history of myocardial infarction and CHF. It is in these clinical situations that beta blockers can improve the prognosis of patients.
Antianginal properties make it possible to prescribe bisoprolol for the prevention of anginal attacks in patients with stable angina pectoris. The multicenter clinical trial TIBBS (Total Ischemic Burden Bisoprolol Study) demonstrated that bisoprolol effectively eliminates episodes of transient myocardial ischemia in patients with stable angina and increases heart rate variability [15]. This study also showed the effect of bisoprolol on improving the prognosis of coronary artery disease. It has been proven that the incidence of cardiovascular events during bisoprolol therapy is significantly lower than when taking nifedipine and placebo.
It was also found that the antianginal effectiveness of bisoprolol is comparable to atenolol, betaxolol, verapamil and amlodipine. Other studies have shown that bisoprolol is more effective in preventing the occurrence of anginal attacks and increases exercise tolerance to a greater extent than isosorbide dinitrate (used as monotherapy) and nifedipine. In patients with stable angina, bisoprolol can be used in combination with other antianginal agents (in particular, nitrates and calcium antagonists).
It was found that bisoprolol significantly reduces the risk of myocardial infarction and mortality from CVD in patients who underwent surgery on the great arteries. As a means of secondary prevention of myocardial infarction, the use of bisoprolol in stable patients who have suffered a myocardial infarction (starting from 5–7 days of the disease) is justified [16].
Choosing bisoprolol
Considering the wide range of medicines on the Russian market and the need for an adequate choice, the problem of interchangeability of original drugs with generics for economic reasons is very relevant. The main limitation in the widespread use of original medicines is their high cost. On the other hand, the fact that the original drug is highly effective is well known. When choosing a generic, it is necessary to have data on therapeutic bioequivalence to the original drug. To prove therapeutic equivalence, a clinical study of a generic drug is required, with comparative clinical studies performed with the original drug to study its effectiveness and safety.
Let us dwell in more detail on the data from clinical studies involving Russian patients with hypertension and coronary artery disease to evaluate the effectiveness of the drug Bidop (bisoprolol).
In 2012, K.V. Protasov et al. A comparison was made of the clinical effectiveness and safety of the original and generic bisoprolol preparations for patients with hypertension and patients with exertional angina. 30 patients with grade 1–2 hypertension (average age 47 years) were examined. Patients were randomized into the original bisoprolol and Bidop groups, which were prescribed at a starting dose of 5 mg/day. After 6 weeks of treatment and a 2-week washout period, the drug was replaced with an alternative one, after which therapy was continued for up to 6 weeks. The study diagram is presented in Fig.
At baseline, on the 2nd and 6th weeks of therapy, blood pressure, heart rate, and unwanted side effects were recorded, and the results of self-monitoring of blood pressure (SBP) were analyzed. At baseline and at week 6, 24-hour blood pressure monitoring (ABPM) was performed. By the 6th week of treatment, office blood pressure significantly decreased in the original bisoprolol group by 23.0/10.5 mmHg. Art., in the generic group - by 21.2/10.0 mm Hg. Art., intergroup differences are not significant. The target blood pressure level (<140/90 mmHg) was achieved in the first group in 71.4%, in the second - in 64.3% of patients (p = 0.57). The degree of heart rate decrease also did not differ and amounted to 11.8 and 10.1 beats/min.
According to self-control and 24-hour blood pressure monitoring, unidirectional and comparable in severity shifts in mean blood pressure and heart rate were identified. Another fragment of the study, which included 18 patients with stable angina, showed that both bisoprolol drugs had similar antianginal effects, reducing signs of ischemia. It is important to note that the doses of the original and generic drugs when achieving a similar antianginal effect in the same patients did not differ, which indicates the identity of their antianginal properties.
Both drugs were well tolerated. Clinically insignificant bradycardia was recorded in only two patients treated with the original bisoprolol. This indicates that Bidop is quite well tolerated and safe [17].
According to T.K. Chernyavskaya (2012), the drug Bidop turned out to be completely therapeutically equivalent to the original bisoprolol. Thus, in the group of patients with grade 1–2 hypertension, the target blood pressure level was <140/90 mmHg. Art. reached 72% of those receiving original bisoprolol and 72.5% of those receiving Bidop. At the same time, the doses of bisoprolol required to normalize blood pressure were 9.5 mg for the original drug and 9.3 mg for Bidop. Transfer to combination treatment was required in 34% of those receiving original bisoprolol and in 33% of those receiving Bidop. No side effects occurred during 16 weeks of observation in any group of patients. With the same therapeutic efficacy, the cost of Bidop therapy was lower [18].
It can be concluded that the original bisoprolol and the drug Bidop are clinically equivalent in terms of safety, antianginal and antihypertensive effects. This allows doctors and patients to reduce the cost of treatment without reducing the effect.
Conclusion
Bisoprolol is a leader among beta blockers due to its high cardioselectivity, unique amphiphilic properties, metabolic neutrality, high efficiency and the absence of a negative effect on the course of other diseases. It is important for Russian patients to confirm the therapeutic equivalence of the original drug bisoprolol and its generic (Bidop). The antihypertensive and antianginal effectiveness of bisoprolol, reducing the cost of treatment through the use of high-quality generic drugs can significantly increase the adherence of patients with CVD to treatment.
Literature
- The Task Force on Beta-Blockers of the European Society of Cardiology. Expert consensus document on b-adrenergic receptor blockers // Eur Heart J. 2004; 25: 1341–1362.
- Russian Medical Society for Arterial Hypertension (RMAS), All-Russian Scientific Society of Cardiologists (VNOK). Diagnosis and treatment of arterial hypertension. Russian recommendations (fourth revision), 2010.
- Haasis R., Bethge H. Exercise blood pressure and heart rate reduction 24 and 3 hours after drug intake in hypertensive patients following 4 weeks of trearment with bisoprolol and metoprolol: a randomized multicentre double-blind study (BISOMET)//Eur Heart Jour. 1987; 8; 103–113.
- Prisant LM, Weir MR, Frishman WH, Neutel JM, Davidov ME, Lewin AJ Self-Reported Sexual Dysfunction in Men and Women Treated With Bisoprolol, Hydrochlorothiazide, Enalapril, Amlodipine, Placebo, or Bisoprolol/Hydrochlorothiazide // J Clin Hypertens (Greenwich). 1999, July; 1 (1): 22–26.
- Podzolkov V.I., Osadchiy K.K. Rational choice of beta-blocker for the treatment of arterial hypertension: focus on Bisogamma // Breast Cancer. 2008, vol. 16, no. 16, p. 4–8.
- Teresa E., Gonzdlez M., Camacho-Vazquez C., Tabuenca M. Effect of bisoprolol on left ventricular hypertrophy in essential hypertension // Cardiovasc. Drugs ther. 1994, 8, 837–843.
- Asmar R. Effect of antihypertensive agents on arterial stiffness as evaluated by pulse wave velocity: clinical implications // Am. J. Cardiovasc. Drugs; 2001, 1(5): 387–397.
- Leonova M.V. Beta blockers and organ protection for arterial hypertension // Clinical pharmacology and therapy. 2012, 21 (3), p. 26–30.
- Drapkina O. M., Korneeva O. N., Ivashkin V. T. Activation of the sympathetic nervous system in obesity. How to influence energy homeostasis? // Arterial hypertension. 2011, vol. 17, no. 2, p. 102–107.
- Kukes V. G., Ostroumova O. D., Baturina A. M., Zykova A. A. Beta-blockers in the treatment of arterial hypertension in patients with diabetes mellitus: contraindication or drugs of choice? // Rus. honey. magazine 2002; 10: 446–449.
- Semenov A.V., Kukes V.G. Clinical and pharmacological aspects of the use of bisoprolol // RMJ. 2007, vol. 15, no. 15, p. 38–43.
- Ostroumova O. D., Maksimov M. L. Possibilities of using highly selective beta-blockers in patients with concomitant diseases // Consilium Medicum. 2012; (4), No. 1: 721–725.
- Korneeva O. N. The place of beta-blockers in the treatment of obese patients with hypertension // Doctor. 2011, no. 11, p. 38–40.
- Diagnosis and treatment of stable angina. On Sat. "National Clinical Guidelines". MEDI Expo, 2009, p. 35–74.
- Weber F., Schneider H., von Arnim T. et al. Heart rate variability and ischaemia in patients with coronary heart disease and stable angina pectoris; influence of drug therapy and prognostic value. TIBBS Investigators Group. Total Ischemic Burden Bisoprolol Study // Eur Heart J. 1999; 20 (1): 38–50.
- Syrkin A.L., Dobrovolsky A.V. // Russian Medical Journal. 2010. No. 22. pp. 1352–1355.
- Protasov K.V., Dzizinsky A.A., Shevchenko O.P. et al. Antianginal and antihypertensive effectiveness of bisoprolol: comparison of generic Bidop with the original drug // Pharmateka. 2012, no. 17, p. 57–63.
- Chernyavskaya T.K. Fundamentals of optimal choice among interchangeable drugs in the treatment of cardiovascular diseases // Systemic hypertension. 2012, No. 1, p. 29–32.
O. N. Korneeva, Candidate of Medical Sciences
GBOU VPO First Moscow State Medical University named after. I. M. Sechenova Ministry of Health of the Russian Federation, Moscow
Contact information about the author for correspondence
Side effects
Taking Bisoprolol may be accompanied by:
- dizziness and headaches ;
- feeling tired ;
- feeling of a rush of blood to the face;
- sleep disorders;
- mental disorders (usually depression , less often - hallucinations );
- paresthesia of the limbs and a feeling of cold in them;
- decreased secretion of tear fluid;
- development of conjunctivitis ;
- abdominal pain, nausea , vomiting ;
- diarrhea or, conversely, constipation ;
- muscle weakness;
- increased convulsive muscle activity;
- symptoms of bronchial obstruction (in patients who are predisposed to this);
- increased sweating ;
- violation of potency;
- bradycardia;
- orthostatic hypotension;
- AV conduction disorders.
In some cases, the course of heart failure may worsen with the development of peripheral edema .
In patients with impaired blood supply to the lower extremities , which is accompanied by intermittent claudication, as well as in patients diagnosed with Raynaud's syndrome , the main symptoms of these diseases may increase.
The possibility of decreased glucose tolerance cannot be ruled out, mainly in patients with concomitant diabetes mellitus (including latent diabetes , which is characterized by the complete absence of any manifestations of this disease).
Bisoprolol film-coated tablets 2.5 mg 30 pcs. in Kaliningrad
Bisoprolol is taken orally
, in the morning on an empty stomach, once, without chewing, with a small amount of liquid. The tablets should not be chewed or crushed into powder.
Treatment of arterial hypertension and angina pectoris
In all cases, the regimen and dosage are selected by the doctor for each patient individually, in particular, taking into account the heart rate and therapeutic response.
For arterial hypertension and coronary heart disease, the usual initial dose is 5 mg 1 time per day.
If necessary, the dose is increased to 10 mg 1 time per day. In the treatment of arterial hypertension and angina pectoris, the maximum daily dose is 20 mg 1 time / day.
It is possible to divide the daily dose into 2 doses.
Treatment of stable chronic heart failure
The standard treatment regimen for CHF includes the use of angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor antagonists (in case of intolerance to ACE inhibitors), beta-blockers, diuretics and, optionally, cardiac glycosides.
Initiation of treatment for CHF with bisoprolol requires a special titration phase and regular medical monitoring.
The precondition for treatment with bisoprolol is stable chronic heart failure without signs of exacerbation.
Treatment of CHF with bisoprolol begins in accordance with the following titration scheme. This may require individual adaptation depending on how well the patient tolerates the prescribed dose, i.e. The dose can only be increased if the previous dose was well tolerated.
To ensure the dosage regimen indicated below, it is possible to prescribe bisoprolol drugs in the dosage form of “2.5 mg tablets” with a score or “5 mg tablets” with two marks (to obtain dosages of 1.25 mg, 2.5 mg and 3.75 mg ).
The recommended starting dose is 1.25 mg (1/2 2.5 mg tablet) once daily.
Depending on individual tolerance, the dose should be gradually increased to 2.5 mg, 3.75 mg (11/2 tablets of 2.5 mg), 7.5 mg (3 tablets of 2.5 mg or 11/2 tablets of bisoprolol 5 mg) and 10 mg once a day.
Each subsequent dose increase should be carried out at least two weeks later.
If increasing the dose of the drug is poorly tolerated by the patient, a dose reduction may be possible.
The maximum recommended dose for CHF is 10 mg of bisoprolol once a day.
During titration, regular monitoring of blood pressure, heart rate and the severity of CHF symptoms is recommended.
Worsening of the symptoms of CHF is possible from the first day of using the drug. If the patient does not tolerate the maximum recommended dose of the drug, a gradual dose reduction is possible. During the titration phase or after it, a temporary worsening of CHF, arterial hypotension or bradycardia may occur. In this case, it is recommended, first of all, to adjust the doses of concomitant therapy drugs. It may also be necessary to temporarily reduce the dose of bisoprolol or discontinue it.
After stabilization of the patient's condition, the dose should be re-titrated or treatment should be continued.
Special patient groups
Impaired kidney or liver function:
- Mild or moderate hepatic or renal impairment usually does not require dose adjustment.
- In severe renal impairment (creatinine clearance less than 20 ml/min.) and in patients with severe liver disease, the maximum daily dose is 10 mg.
Increasing the dose in such patients should be carried out with extreme caution.
To date, there is insufficient data regarding the use of bisoprolol in patients with CHF associated with type 1 diabetes mellitus, severe renal and/or liver dysfunction, restrictive cardiomyopathy, congenital heart defects or heart valve disease with severe hemodynamic disturbances. Also, sufficient data have not yet been obtained regarding patients with CHF with myocardial infarction within the last 3 months.
Bisoprolol tablets, instructions for use (Method and dosage)
The dosage of the drug is selected individually. The tablets are taken in the morning, before meals, without chewing. The course of treatment begins by prescribing 0.005 grams to the patient, which is taken once. For patients whose blood pressure is slightly elevated, the starting dose is 0.0025 grams per day.
In cases where this is necessary, the dose is doubled. The dosage regimen remains the same.
The highest daily dose is 0.02 grams; for patients with renal dysfunction , which is characterized by a decrease in creatinine clearance (CC) below 20 ml per minute, the highest dose should be half that (0.01 grams per day).
Exceeding the prescribed average daily dose is allowed in extreme cases. The drug is usually used for a long time.
Elderly patients do not need dose adjustment.
The instructions for use of Bisoprolol-Ratiopharm are identical to the instructions for use of Bisoprolol-Lugal and the instructions for use of Bisoprolol-Teva . Bisoprolol-Prana and other bisoprolol preparations are taken according to the same regimen
Beta-blockers (BABs) are one of the main groups of drugs used in the treatment of cardiovascular diseases (CVD). Experts from international and Russian recommendations have included beta blockers in the list of drugs for the treatment of patients with arterial hypertension (AH), acute coronary syndrome, chronic coronary heart disease (CHD), cardiac arrhythmias, and chronic heart failure (CHF). Large international randomized studies have proven the high effectiveness of beta blockers for hypertension (MRS, IPPPSH, HAPPHY, MAPHY). In Russian recommendations for the diagnosis and treatment of hypertension, beta blockers are included in the main groups of drugs for the treatment of this disease, since they have a proven ability to reduce cardiac mortality. BBs are the drugs of choice for patients with hypertension who have suffered a myocardial infarction, as well as for patients with concomitant stable angina, heart rhythm disturbances, CHF, glaucoma, and pregnancy.
Currently, more than 100 beta blockers have been synthesized, but no more than 30 drugs from this group are used in clinical practice.
BBs differ in cardioselectivity, intrinsic sympathetic activity, lipophilicity, membrane-stabilizing properties, duration of action, and routes of elimination. BBs with additional characteristics were synthesized, in particular the properties of vasodilators and antioxidants (carvedilol, nebivolol).
The mechanisms of action of beta blockers in hypertension are not fully understood. BBs reduce minute blood volume due to negative ino- and chronotropic effects, reduce the release of norepinephrine from neurons due to blockade of presynaptic β2-adrenergic receptors, and reduce stimulation of postsynaptic β-adrenergic receptors and the sympathoadrenal system (SAS). The binding of beta blockers to myocardial β1-adrenergic receptors, competitive with catecholamines, increases their density, as a result of which the direct cardiotoxic effect of catecholamines is suppressed and the sensitivity of cardiomyocytes to β-adrenostimulation is restored. BBs restore the sensitivity of baroreceptors to changes in blood pressure (BP). Blockade of renal β-adrenergic receptors inhibits renin secretion and secondarily inhibits the synthesis of angiotensin II and aldosterone.
A decrease in the activity of the SAS and the renin-angiotensin-aldosterone system (RAAS) during beta blocker therapy prevents the development of hypertrophy and apoptosis of cardiomyocytes, the accumulation of collagen in the myocardium, and promotes regression of already developed left ventricular (LV) myocardial hypertrophy.
BBs reduce heart rate (HR), lengthen diastole, and improve myocardial perfusion. Drugs from the beta blocker group increase oxygen delivery to the myocardium by increasing collateral blood flow and its redistribution in favor of the ischemic layers of the myocardium. BB block β1-adrenergic receptors and reduce the formation of cAMP stimulated by catecholamines, reduce the intracellular content of calcium ions, weaken the proliferation of cardiac tissue cells, increase the expression of Mg-ATPase mRNA of the sarcoplasmic reticulum calcium pump and α-myosin heavy chain mRNA, which leads to improved diastole of cardiomyocytes.
BBs reduce the frequency of recurrent myocardial infarction, which is associated with their effect on the triggers of coronary plaque damage: vascular wall tension, platelet activity, and blood pressure levels. Due to the negative inotropic effect, beta blockers reduce the rate of blood expulsion from the left ventricle, reduce the transstenotic pressure gradient in the coronary arteries, preventing damage to the atherosclerotic plaque.
Long-term use of beta blockers in hypertensive patients with CHF leads to an increase in LV ejection fraction by an average of 5–9%. The increase in cardiac output during treatment with negatively acting inotropic agents is due to the inhibition of increased activity of the SAS and RAAS, a decrease in the calcium content of cardiomyocytes, limiting the processes of apoptosis, increasing diastolic relaxation of the heart, and reducing the zone of hibernating myocardium [1].
For a long time, the position of beta blockers in the treatment of hypertension seemed indisputable. At the same time, a meta-analysis conducted by H. Litchell in 1992 showed an increase in insulin resistance during therapy with propranolol, atenolol, and pindolol. B. Carlberg's meta-analysis included 9 studies using atenolol, of which 5 (17,071 patients) compared atenolol with other antihypertensive drugs, and 4 (6825 patients) compared it with placebo. It was found that in patients with hypertension, atenolol, compared with placebo, does not reduce the risk of myocardial infarction (relative risk [RR] = 0.99), total (RR = 1.01) and cardiovascular mortality (RR = 0.99). Atenolol was shown to be significantly less effective in comparison with angiotensin-converting enzyme inhibitors (ACEIs) and calcium antagonists in reducing the risk of death (RR = 1.13), stroke, and mortality from CVD with equal antihypertensive effectiveness.
In 2005, another meta-analysis by LH Lindholm was published, which included 14 randomized studies (105,951 patients). BBs were compared with diuretics, ACE inhibitors, calcium antagonists and angiotensin II receptor blockers. It has been shown that treatment of patients with beta blockers leads to an increase in the RR of stroke by 16% compared to other groups of antihypertensive drugs.
Previously obtained data on the insufficient effectiveness of beta blockers in hypertension required further clarification. In 2009, a meta-analysis of 147 studies was published, which included a total of data on 464 thousand patients taking drugs from various groups of antihypertensive drugs. In terms of their effect on the incidence of coronary artery disease and strokes, beta blockers did not differ from diuretics, ACE inhibitors, and angiotensin II receptor blockers, but were inferior to calcium antagonists in terms of reducing the risk of stroke. The incidence of coronary complications was lower when beta blockers were used by patients with hypertension and concomitant coronary artery disease.
The results obtained in meta-analyses served as the basis for discussing the feasibility of using beta blockers in hypertension. In the British guidelines for the treatment of hypertension, beta-blockers are ranked 4th among other antihypertensive drugs. In the European recommendations of 2009, the attitude towards beta blockers is quite restrained. It is believed that beta blockers should not be used among patients with hypertension with metabolic syndrome, obesity, carbohydrate metabolism disorders, and a high risk of developing diabetes mellitus. Experts of the Russian Society of Cardiologists on hypertension believe that since previously conducted meta-analyses included studies that used atenolol and first-generation beta blockers (propranolol, oxprenalol, pindolol, etc.), characterized by relatively low tolerability and a high incidence of lipid and carbohydrate disorders exchange, the results obtained should not be extrapolated to second- and third-generation BABs. The authors of the B. Carlberg meta-analysis did not recommend the use of atenolol as a comparator drug in large multicenter studies. Improvement of the structure of beta blockers has led to the creation of drugs with high cardioselectivity, stable long-term effect, metabolic neutrality and a small number of side effects.
One of the most studied second-generation beta blockers, which has high cardioselectivity, amphophilicity and a long period of action, is bisoprolol.
To reduce the cost of treating patients with hypertension, many countries around the world use generics of original drugs. One of the generics of bisoprolol is BisogammaR (Worwag Pharma, Germany). This is a generic bisoprolol with proven bioequivalence, a highly selective β1-blocker with a β1/β2-blocking ability ratio of 1/75. It does not have internal sympathomimetic activity and membrane stabilizing properties. BisogammaR is characterized by high bioavailability (80–90%). The maximum concentration of the drug in plasma is observed 1–3 hours after administration, the half-life is 10–12 hours, which allows the drug to be administered once a day. BisogammaR binding to blood plasma proteins is about 30%. The dependence of pharmacokinetic parameters on dose is linear, individual and interindividual fluctuations are small. The drug is amphophilic, i.e. it is able to dissolve in both lipids and water. BisogammaR is 50% metabolized in the liver (with the participation of cytochromes CYP 2D6 and CYP 3A4), the other half of the dose is excreted unchanged by the kidneys. The presence of two elimination routes allows the drug to be used for patients with liver and kidney diseases without dose adjustment.
The effectiveness of BisogammaR was assessed in a number of Russian clinics. High antihypertensive effectiveness of the drug was noted. When treated with BisogammaR at a dose of 5–10 mg per day, the target blood pressure level is achieved in 62–89% of patients [2, 3]. Comparison of the therapeutic equivalence of the original bisoprolol and BisogammaR in patients with stage I–II hypertension. demonstrated similar clinical efficacy and tolerability of both drugs [4].
The effectiveness of BisogammaR at a dose of 5 mg/day was studied in 29 menopausal women with hypertension and cardialgia. The duration of the study was 3 months. Therapy with the drug led to a persistent decrease in blood pressure and heart rate, a decrease in the manifestations of menopausal syndrome: the frequency of hot flashes, nervousness, and sweating decreased; headaches decreased [5].
Beta blockers are the only group of antihypertensive drugs among antihypertensive drugs that effectively control heart rate. Treatment with BisogammaR is associated with a decrease in heart rate by an average of 23% [6]. The influence of BisogammaR on the processes of remodeling of resistive vessels and the rheological properties of blood in patients with hypertension was studied in a study by A.M. Shilova [7]. Treatment was carried out for 6 months, BisogammaR was prescribed in a daily dose of 2.5–10.0 mg to patients with stage I–II hypertension. A significant decrease in systolic and diastolic blood pressure was observed by 13.3 and 16.3%, respectively (p < 0.05). The vascular wall stiffness index decreased by 16.1 and 8.1% for the common carotid and femoral arteries, respectively (p < 0.05), the atherogenic index decreased by 43.1% (p < 0.001) due to a decrease in the level of low-density lipoproteins by 34.5% and an increase in the concentration of high-density lipoproteins by 29.7%. An increase in the electrophoretic mobility of erythrocytes and a decrease in platelet aggregation activity by 11.1 and 19.0%, respectively, were detected (p < 0.05). The increase in the ability of erythrocytes to deform is explained by the restoration of the viscosity properties of their membranes due to the normalization of the lipid composition after 6 months of therapy.
The effectiveness of BisogammaR in patients with CHF and stable angina of functional classes II–III was assessed in a study by A.M. Shilova et al. [6]. The drug was prescribed at a dose of 5–7.5 mg/day for 4 weeks. A decrease in heart rate and an improvement in the parameters of diastolic relaxation of the LV were established: an increase in the rate of early and late myocardial relaxation (by 18.8 and 43.1%, respectively), a decrease in the time of deceleration of diastolic blood flow. A decrease in heart rate and restoration of LV diastolic filling parameters led to a significant (59.1%) reduction in the frequency of ischemic episodes according to Holter ECG monitoring. An increase in exercise tolerance was noted: the distance in the 6-minute walk test increased by 73.6% (from 252.3 ± 28 to 438.1 ± 33.1 m; p < 0.001). The positive effect of BisogammaR is due to a decrease in myocardial oxygen demand due to a decrease in heart rate, prolongation of diastole, and improved perfusion. Treatment with bisoprolol was accompanied by normalization of the “myocardial oxygen demand/oxygen delivery” ratio, which led to a decrease in the area of hibernating myocardium.
BisogammaR has an antiarrhythmic effect by reducing the activity of the sympathetic nervous system, increasing the threshold for ventricular fibrillation, and blocking catecholamine-induced permeability of cardiomyocyte membranes to calcium. The drug reduces the pacemaker function of the sinus node and the speed of impulse transmission through the conduction system of the heart (mainly in the antegrade direction, to a lesser extent in the retrograde direction through the AV node). Due to the high antiarrhythmic effect, treatment with bisoprolol is associated with a significant – 44% – reduction in the risk of death [8].
In average therapeutic doses (2.5–10.0 mg), BisogammaR practically does not cause dysmetabolic effects such as hyperlipidemia, hyperglycemia or hypokalemia.
Experts of the European Society of Cardiology on the diagnosis and treatment of hypertension (2009) believe that beta blockers should not be prescribed to patients with metabolic syndrome due to their negative effect on carbohydrate metabolism. For a long time it was believed that beta blockers increase the risk of hypoglycemia, mask its manifestations, and slow down the recovery of glucose levels after hypoglycemia. A meta-analysis of 22 large randomized trials, including 143,153 patients, showed an increase in the number of new cases of diabetes mellitus when treated with beta blockers. It is known that beta blockers have different prodiabetogenic potential. Bisoprolol has virtually no effect on blood glucose levels in patients with diabetes, so its use does not require dose adjustment of glucose-lowering drugs.
A study was conducted on the safety of administering BisogammaR for 3 months to patients with impaired glucose tolerance [9]. The drug was prescribed at a daily dose of 2.5–10.0 mg in combination with metformin at a daily dose of 500–1000 mg. During therapy, normalization of blood glycemia and lipid levels was noted. After 3 months of therapy, the atherogenic index decreased by 35.3% (p < 0.001), fasting glucose level - by 9.8%, insulin resistance index - by 37.2%, and glycosylated hemoglobin level - by 17.8%. No negative effect of BisogammaR on glycemic parameters was detected. Similar results were obtained in the study [10].
The high selectivity of BisogammaR allows one to avoid the negative effects of this drug on lung function and peripheral circulation. A comparative study was conducted of the effect of BisogammaR and atenolol on indicators of respiratory function in patients with hypertension and concomitant chronic obstructive pulmonary disease [9]. Therapy with BisogammaR at the maximum therapeutic dose (20 mg/day) did not affect airway resistance. A single dose of atenolol 100 mg significantly increased airway resistance (by 12%).
Thus, BisogammaR is a highly selective β1-blocker with a long half-life, which is highly effective in patients with hypertension and coronary artery disease. In therapeutic doses, the drug has virtually no affinity for β2-adrenergic receptors, which determines its safety and metabolic neutrality.
Overdose
An overdose of the drug is accompanied by the following symptoms:
- severe bradycardia ;
- ventricular extrasystole;
- AV block;
- arrhythmia;
- pronounced decrease in blood pressure;
- HNS;
- cyanosis (blueness) of the fingers or palms;
- difficulty breathing;
- dizzy;
- bronchospasm;
- syncope;
- convulsions.
Treatment involves performing a gastric lavage procedure, taking adsorbent medications and prescribing symptomatic therapy:
- of atropine or epinephrine into a vein for AV block (in some patients, a temporary pacemaker is installed to solve the problem);
- injection of lidocaine for ventricular extrasystole (class IA drugs should not be used);
- moving the patient to the Trendelenburg position when blood pressure decreases ;
- intravenous administration of plasma-substituting solutions (if there are no signs of incipient pulmonary edema ; if this does not give the expected effect, the patient should be administered epinephrine , dobutamine or dopamine in blood pressure );
- prescribing cardiac glycosides , diuretics , as well as glucagon for heart failure ;
- intravenous diazepam for seizures;
- inhaled administration of β-agonists for bronchospasm.
Introduction
One of the most common forms of heart rhythm disturbances is paroxysmal supraventricular tachycardia (SVT).
In the general population, its occurrence reaches 20%, and among patients with hypertension (HTN) and coronary heart disease (CHD) it is much more. Due to the severity of clinical manifestations, paroxysmal SVT occupies a leading place among all cardiac arrhythmias in terms of the frequency of requests for emergency medical care. Frequent and prolonged paroxysms of SVT induce arrhythmogenic myocardial dilatation and systolic chronic heart failure (CHF) [1], contribute to the formation of more complex cardiac arrhythmias [2], and correlate with the risk of developing atrial fibrillation, ischemic stroke and cardiovascular death [3]. For drug therapy of paroxysmal SVT, β-blockers (BABs) are most often used [4]. The rationale for their use is the blockade of the sympathoadrenal system, which is often in a state of pathological hyperactivation [5]. However, in a significant proportion of patients, the use of beta blockers may be limited by their side effects: increased tone of the bronchi and peripheral arteries, decreased physical and mental performance, and erectile dysfunction.
Therapy with certain beta blockers can sometimes be accompanied by a worsening of an existing arrhythmia. Negative chrono-, dromo- and inotropic effects limit the use of beta blockers for bradycardia, atrioventricular block, arterial hypotension, and severe left ventricular (LV) systolic dysfunction [6]. These circumstances justify the choice of drugs that selectively eliminate arrhythmia and do not worsen the functional state of the body.
Assuming a possible multidirectional effect of beta blockers, monitoring the effectiveness of drug therapy should be carried out using sensitive diagnostic methods that determine not only antiarrhythmic and organoprotective effects, but also the functional state of the body as a whole, its ability to regulate and adapt. For an objective quantitative assessment of the regulatory-adaptive status (RAS), a cardiorespiratory synchrony test (CRS) is used, which reflects the interaction of the two most important functions of autonomic support - cardiac and respiratory. The test is based on the close functional connection between the central mechanisms of rhythmogenesis of the heart and respiration, the possibility of voluntary control of the breathing rhythm, and the participation of multi-level afferent and efferent structures of the central nervous system [7].
There is no information in the literature on monitoring the effect of beta blockers on the ASD of patients with paroxysmal SVT. It is possible that their intragroup heterogeneity, mediating different clinical and hemodynamic effects, also has different effects on ASD. Therefore, the selection of optimal beta blockers that effectively suppress SVT paroxysms and have a positive effect on both target organs and the RAS seems relevant.
Purpose of the study
— compare the effectiveness of bisoprolol and sotalol in patients with paroxysmal SVT secondary to hypertension and/or coronary artery disease, taking into account their effect on the RAS.
Interaction
Inadmissible combinations with Bisoprolol:
- Floctafenine;
- Sultopride.
Not recommended combinations:
- with calcium antagonists;
- with antihypertensive drugs , which are characterized by a central mechanism of action;
- with MAO inhibitors (except for MAO-B inhibitors).
The drug is prescribed with caution with:
- antiarrhythmic drugs class I and III;
- calcium antagonists , which belong to the group of dihydropyridine derivatives ;
- anticholinesterase drugs;
- Local β-blockers;
- insulin preparations and oral antidiabetic agents ;
- cardiac glycosides (digitalis preparations);
- anesthetics;
- non-steroidal anti-inflammatory drugs;
- ergotamine derivatives;
- β-sympathomimetics;
- sympathomimetics, which are characterized by the ability to activate α- and β-adrenergic receptors ;
- antihypertensive drugs that increase the risk of hypotension (for example, tricyclic antidepressants , phenothiazines or barbiturates );
- Baclofen;
- Amifostin;
- parasympathomimetics.
Allowed combinations:
- mefloquine;
- corticosteroid drugs.
special instructions
The drug should be prescribed with caution:
- patients diagnosed with psoriasis , as well as patients whose family history contains indications of this disease;
- with diabetes mellitus in the stage of decompensation;
- patients who are predisposed to allergic reactions ;
- patients whose work requires a high speed of psychomotor reactions or potentially threatens health and/or life (as a rule, the reaction speed may decrease in the initial stages of treatment, when changing the drug, as well as when Bisoprolol interacts with alcohol).
For patients diagnosed with pheochromocytoma , the drug is prescribed only after completing a course of treatment with α-blockers .
Sudden withdrawal of the drug is unacceptable; the course of its use is completed gradually, gradually reducing the prescribed dose (it is considered optimal to reduce it by halving the dose daily).
Material and methods
The study involved 60 patients with paroxysmal SVT secondary to stage II–III hypertension and/or coronary artery disease. After randomization (by random sampling), the first group of patients (n=30) was prescribed bisoprolol, the second group (n=30) was prescribed sotalol. The initial dose of bisoprolol was 2.5 mg/day in 1 dose, sotalol - 80 mg/day in 2 doses. Taking into account hemodynamic parameters and individual tolerance, drug doses were titrated at intervals of 2–4 weeks. up to 10 and 320 mg/day, respectively (Table 1).
As part of combination therapy, all patients received lisinopril, and, if indicated, atorvastatin 15.6±5.1 mg/day, n=14, and 14.2±4.6 mg/day, n=15, and acetylsalicylic acid 92 .3±18.8 mg/day, n=15, and 94.8±15.8 mg/day, n=18, or rivaroxaban 20 mg/day, n=3 and n=2, respectively. Treatment adherence was assessed during monthly physician visits.
Inclusion criteria for the study: patient age 30–70 years, presence of paroxysmal SVT against the background of stage II–III hypertension and/or coronary artery disease with preserved LV systolic function (LV ejection fraction (EF) ≥50%), non-use of test drugs within the previous 10 years days, familiarization with the study protocol and written consent to participate in it.
Exclusion criteria: dependence on alcohol and drugs, acute vascular events (cerebral and coronary) during the last year, stage III arterial hypertension, angina pectoris functional class 3-4 (FC), heart rhythm and conduction disorders, CHF FC 3-4 according to the New York Heart Association classification, LV systolic dysfunction, history of cardiac and neurosurgical interventions, respiratory, renal and liver failure, exacerbation of autoimmune diseases, malignant neoplasms, endocrine disorders in the stage of decompensation.
The study was approved by the ethics committee of the State Budgetary Educational Institution of Higher Education "Kuban State Medical University" of the Ministry of Health of the Russian Federation (protocol No. 34 of February 27, 2015).
At the beginning of the study and after 6 months. drug therapy was carried out:
quantitative assessment of ASD using the SDS test with determination of the ASD index (the RAS index is the ratio of the synchronization range (DS) to the duration of development of SDS at the minimum border of SDS×100) [8]. ASD index score: 100 or more – high, 99–50 – good, 49–25 – satisfactory, 24–10 – low, 9 or less – unsatisfactory [9];
ECG in V- and M-modes;
treadmill test using the SHILLER CARDIOVIT CS 200 device (Switzerland) to determine exercise tolerance and identify hidden coronary insufficiency;
six-minute walk test (SMW);
daily monitoring (CM) of blood pressure (BP) in order to determine the daily blood pressure profile, as well as adequate monitoring of the effectiveness of pharmacological therapy;
SM ECG to identify paroxysms of SVT and monitor the effectiveness of therapy;
assessment of quality of life (QOL) using the questionnaire “Quality of life of a patient with arrhythmia” [10].
Statistical processing was carried out using variation statistics methods using the STATISTICA package (version 6.0). Differences were considered statistically significant at p<0.05. Data from only those patients who fully complied with the study protocol were analyzed.
Synonyms and analogues of Bisoprolol
Level 4 ATC code matches:
Biol
Metocard
Metozok
Nebilet
Nebilong
Betaxolol
Bisogamma
Aritel
Cordinorm
Vasocardin
Corvitol
Bidop
Nebivolol
Biprol
Bisoprol
Concor Cor
Lokren
Concor
Niperten
Betaloc ZOK
Structural analogues of Bisoprolol (synonyms) are the drugs Biprol , Bisogamma , Niperten , Bisoprolol-Prana , Bisoprolol-Lugal , Bisoprolol-Ratiopharm , Bisoprolol-Teva , Concor , Concor Cor , Bisomore , Bioscard , Corbis , Bidop , Aritel Cor , Bisomore .
Analogues of the drug according to the mechanism of action are Atenolol , Betacard , Betalok , Binelol , Cordanum , Lidalok , Lokren , Metozok , Metoprolol , Metocor , Nebivator , Nebilong , Nebilet , OD-Neb , Egilok , Estekor .
Which is better - Bisoprolol or Concor?
Concor is the brand name under which the original bisoprolol is produced. The manufacturer of the drug is the German pharmaceutical company Merck KGaA. However, the patent for this medicine has long expired, so there are currently a large number of more affordable generic bisoprolol on the market.
It is believed that all of them are not inferior in quality to the original drug, however, there is not enough official data to confirm this today.
During pregnancy
Bisoprolol is not recommended for the treatment of pregnant and lactating women. However, in situations where the benefits to the mother potentially outweigh the likely risks to the developing fetus, the drug may still be prescribed.
In exceptional cases, when the medicine is used during pregnancy , it should be discontinued no later than 72 hours before the expected date of birth. Otherwise, there is a high probability of developing hypoglycemia , arterial hypotension , bradycardia , and respiratory depression .
When withdrawal is not possible, constant monitoring of the baby's condition is necessary during the first 72 hours after birth.
If it is necessary to prescribe Bisoprolol to a nursing woman, it is necessary to resolve the issue of stopping lactation .
Reviews of Bisoprolol
Most often, the topic of drug withdrawal is discussed on relevant forums. Reviews about Bisoprolol left by patients and doctors are mainly related to withdrawal syndrome , which occurs against the background of an abrupt cessation of treatment with this drug.
Particular manifestations of it are increased heart rate and attacks of arterial hypertension . Some patients note that during treatment with the drug their vision decreased .
However, since Bisoprolol is prescribed for a long period of time (for some patients even for life), visual impairment and medication intake may be unrelated phenomena.
Taking Bisoprolol may be accompanied by side effects. Some patients practically do not notice them in themselves, while in others, if you believe the reviews, they are quite pronounced.
In connection with all of the above, neither treatment nor discontinuation of the use of this drug should be an independent decision of the patient. In each specific case, the treatment regimen and dosage regimen are determined solely by the doctor who is caring for the patient.
conclusions
Regimens using bisoprolol or sotalol as part of combination pharmacological therapy had an equally positive effect on target organs, comparable increased exercise tolerance, and had antiarrhythmic and hypotensive effects.
Sotalol, in comparison with bisoprolol, reduces RAS less and improves quality of life more significantly.
Taking into account the less pronounced negative effect of sotalol on the RAS in patients suffering from a paroxysmal form of SVT against the background of stage II–III hypertension and/or coronary artery disease, its use may be preferable to bisoprolol.
Bisoprolol price, where to buy
The price of Bisoprolol depends on which pharmaceutical company produced the drug.
The drug can be bought for 80-310 rubles in Russian pharmacies. Bisoprolol-Prana 5 mg costs about 80-100 rubles. The price of Bisoprolol-Ratiopharm 5 mg in Russia is unknown; at the moment it is not available in pharmacies. Price Bisoprolol-Teva 10 mg No. 30 - 207 rub.
The price of Bisoprolol-Astrapharm in Ukraine starts from 13 UAH.
The price of drug analogues on the Russian pharmaceutical market is from 32 rubles.
- Online pharmacies in RussiaRussia
- Online pharmacies in UkraineUkraine
- Online pharmacies in KazakhstanKazakhstan
ZdravCity
- Bisoprolol tab.
p/o 10mg 30pcs ALKALOID AD Skopje 150 RUR order - Bisoprolol tablets p.p.o. 2.5 mg 30 pcs. Ozone LLC/Ozone Pharm LLC
85 rub. order
- Bisoprolol-Teva tablets p.p.o. 10 mg 30 pcs. Teva LLC
220 rub. order
- Bisoprolol-Teva tablets p.p.o. 10 mg 50 pcs. Teva LLC
290 rub. order
- Bisoprolol tablets p.p.o. 5 mg 50 pcs. R-Pharm Novoselki LLC
175 rub. order
Pharmacy Dialogue
- Bisoprolol (5 mg tablet No. 50)Biocom
134 RUR order
- Bisoprolol Canon (tab.p.pl.vol. 2.5 mg No. 30) Kanonpharma Production CJSC
79 RUR order
- Bisoprolol (tab.p.pl/vol. 5 mg No. 30) Uniquem Laboratories
108 RUR order
- Bisoprolol Welfarm (tab.p.pl.vol. 10 mg No. 50) Welfarm LLC
RUB 291 order
- Bisoprolol-Teva (tab.p.pl/vol. 10 mg No. 30) Teva LLC
RUB 199 order
show more
Pharmacy24
- Bisoprolol-Teva 10 mg N50 tablets Merkle GmbH, Nimechchina
64 UAH. order - Bisoprolol KPKA 10 mg N30 tablets KRKA, d.d., Novo Mesto, Slovenia/TAD Pharma GmbH, Nimeččina
22 UAH order
- Bisoprolol-KV 10 mg N30 tablets PAT "Kiev Vitamin Plant", Kiev, Ukraine
22 UAH order
- Bisoprolol-Teva 10 mg No. 30 tablets Merkle GmbH, Nimechchina
39 UAH order
- Bisoprolol KPKA 5 mg No. 30 tablets KRKA, d.d., Novo Mesto, Slovenia/TAD Pharma GmbH, Nimeččina
20 UAH order
PaniPharmacy
- Bisoprolol tablets Bisoprolol-KV tablets 5 mg N30 Ukraine, Kiev Vitamin Plant PJSC
13 UAH order
- BISOPROLOL tablets Bisoprolol Sandoz film-coated tablets 5 mg No. 30 Germany, Salutas Pharma
28 UAH order
- BISOPROLOL tablets Bisoprolol tablets 5 mg No. 20 Ukraine, Astrapharm LLC
13 UAH order
- BISOPROLOL tablets Bisoprolol tablets 5 mg No. 50 Germany, Merckle
59 UAH order
- BISOPROLOL tablets Bisoprolol Sandoz film-coated tablets 10 mg No. 90 Germany, Salutas Pharma
76 UAH order
show more