Magnesium is one of the important and irreplaceable elements for the human body. The drug Magnerot normalizes the functioning of the cells and muscles of the heart and participates in the regulation of its contractions.
In stressful situations, large amounts of magnesium are released from the body, resulting in an increased need for additional magnesium intake to combat stress.
In what cases should it be used?
Most often, the medicine is prescribed for chronic heart failure and arrhythmia, which is associated with a lack of salts and magnesium in the human body. The drug repels spastic manifestations and does not allow the development of atherosclerosis.
Indications for use may be greater due to the presence of diseases of the digestive system, when magnesium in food is not absorbed in the stomach, or conditions that require a high content of the active component. These conditions include:
- period of bearing a child;
- chronic alcoholism;
- prolonged physical inactivity;
- prolonged depression.
Instructions for use MAGNEROT® (MAGNEROT)
Magnesium is a macronutrient. Necessary for many energy processes, participates in the metabolism of proteins, fats, carbohydrates and nucleic acids.
Magnesium takes part in the process of neuromuscular excitation, inhibiting neuromuscular transmission. Magnesium is of particular interest as a natural physiological calcium antagonist. Magnesium controls the normal functioning of myocardial cells and is involved in the regulation of myocardial contractile function. In stressful situations, an increased amount of free ionized magnesium is excreted, and therefore the additional amount of magnesium helps to increase resistance to stress.
Magnesium deficiency leads to neuromuscular disorders (motor and sensory hyperexcitability, convulsions, paresthesia), mental changes (depression, confusion and hallucinations), cardiovascular diseases (ventricular extrasystole, tachycardia, increased sensitivity to cardiac glycosides). Magnesium deficiency during pregnancy increases the likelihood of toxicosis and premature birth.
Magnesium is one of the essential minerals needed by all living cells. Magnesium is a cofactor for about 300 enzymes, incl. associated with the transfer of phosphate groups, with all reactions requiring ATP, as well as at all stages of replication and reading of the genetic code. Magnesium is also necessary for cellular metabolism, incl. glycolysis and oxidative phosphorylation. Magnesium is important for membrane stabilization, nerve conduction, calcium channel activity, and ion transport.
Depending on the severity, magnesium deficiency invariably causes secondary electrolyte imbalances (hypocalcemia, loss of intracellular potassium, and sodium and calcium oversaturation), which explains the occurrence of clinical symptoms such as impaired muscle function (neuromuscular disorders, cramps). It has been experimentally established that a lack of magnesium leads to a deficiency of potassium, while a simultaneous lack of magnesium increases the loss of potassium in cells due to a lack of potassium. Potassium replenishment is inhibited in the presence of uncorrected magnesium deficiency.
Salts of orotic acid are involved in the metabolic process. In addition, orotic acid salts are necessary for the fixation of magnesium on ATP in the cell and the manifestation of its action. Orotic acid is a key intermediate in the biosynthetic pathway of pyrimidine metabolism and, accordingly, a component of all living cells. At high metabolic demands, orotic acid is included in the pathway for the synthesis of pyrimidine nucleotides, which are necessary for RNA synthesis, and, accordingly, for RNA-dependent synthesis of proteins and phospholipids. In addition, the production of glycogen and ATP is stimulated. By synthesizing energy-rich phosphates, orotate can improve the energy status of hypoxic cells.
How to take Magnerot
The drug must be taken orally. To enhance the effectiveness of taking it, you need to take the tablet 1 hour before meals. The tablet should be taken with a sufficient amount of purified water. The duration of therapy depends on the patient’s condition and is determined only by a specialist. But there is also a general treatment plan. Initially, you need to take 2 tablets 3 times a day for 7 days. Then reduce to 1 tablet at a time. You can take a maximum of 6 tablets per day. In the absence of contraindications, the drug can be used for a long time.
For night cramps, Magnerot is also prescribed. At night you need to take up to 3 tablets at a time.
The effect of therapy with Magnerot on cardialgia in postmenopausal women
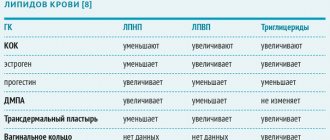
At the age of 50–55 years, when estrogen levels rapidly decrease, in women the incidence of arterial hypertension and cardialgia doubles. It is believed that 90% of cardialgia are caused by three main reasons: ischemic heart disease, vertebrogenic-muscular pathology and psychovegetative disorders. Since stress tests usually do not reveal myocardial ischemia, and coronary angiography - stenotic lesions of the arteries, as a rule, there are no signs of gross musculoskeletal pathology, pain is most often regarded as a manifestation of neurocirculatory dystonia or psychovegetative syndrome [3, 8, 10]. At the same time, it is known that estrogens have a significant effect on vascular tone, stimulating the formation of nitric oxide (NO) by the endothelium and preventing the action of angiotensin II on the vascular wall. This suggested that the occurrence of endothelial dysfunction and vasomotor disorders against the background of estrogen deficiency may be one of the causes of pain in the chest [9, 11, 14]. This concept is supported by the fact that in some cardialgia, endothelial dysfunction is detected with a very high frequency. The causative role of hypoestrogenemia is confirmed by the high effectiveness of hormone replacement therapy.
However, quite often one has to deal with a negative attitude towards the use of hormone replacement therapy (HRT), both from patients and from doctors. In addition, their use is often hampered by the presence of contraindications. This makes it urgent to search for other approaches to the treatment of cardialgia. One way may be to use the drug Magnerot, which has a mild antispasmodic effect and a beneficial effect on the psycho-vegetative status.
The purpose of the study was to study the effect of the drug Magnerot on the dynamics of cardialgia, psycho-vegetative status and endothelial dysfunction in postmenopausal women.
We examined 32 women (average age 53.3 ± 1.2 years), the duration of postmenopause was 4.0 ± 1.0 years. All patients had climacteric syndrome, in most cases of moderate severity (Cooperman index was 28.4 ± 2.3 points).
Chest pain was assessed using a visual analogue scale and a questionnaire, which took into account: the nature of the pain, localization, conditions of occurrence and relief. All women underwent: treadmill test, information load test, cold test, and hyperventilation test.
The photoplethysmogram of the fingers was recorded on an Ultra PVD device (AMP, USA) both at rest and during information-stress, cold, and hyperventilation tests. The results were assessed by changes in the amplitude of the photoplethysmogram (APPG).
To study the vasomotor function of the endothelium, we used Doppler scanning of the brachial artery using an Acuson Sequoia-512 device (Japan) with high-resolution ultrasound at rest and during reactive hyperemia after 3-minute clamping of the brachial vessels with a cuff. An increase in the diameter of the artery by 10% or more was considered normal during the test with reactive hyperemia.
The severity of autonomic dysfunction was assessed using a standardized questionnaire [2].
Anxiety and depressive disorders were assessed using the standardized Beck scales for depression and the Spielberger–Hanin scales for anxiety.
To assess the antithrombogenic function of the endothelium, we conducted a platelet aggregation study using the GV Born method in the O'Brien modification, induced by ristomycin at a concentration of 0.5 mg/ml, before and after the cuff test. The difference in platelet aggregation indicators (D%) was calculated using the formula: X, D% = (X (PM) - X (ref.) x 100%, where X (PM) is the platelet aggregation indicator after the cuff test; X (ref.) — initial indicator of platelet aggregation.The results of platelet hemostasis were compared with the data of the control group (12 postmenopausal women, whose average age was 55.4 ± 1.4 years, without cardialgia, with normal vasomotor function of the endothelium).
All women received the drug Magnerot according to the following regimen: 1 week - 2 tablets. 3 times a day, then - 1 tablet. 3 times a day. Treatment was carried out for 3 months. Health status was monitored monthly; instrumental examinations were carried out initially and after 3 months of Magnerot therapy.
The results were processed by the method of variation statistics with data presented in the form of an average value and its standard deviation (M ± m). The significance of the differences was assessed using the Student's test.
The results of the study revealed that in 5 (15.6%) women the pain was localized behind the sternum, had a compressive nature and lasted up to 10 minutes. In 27 (84.4%) women, chest pain was of a pressing, aching nature; the patients experienced a feeling of discomfort and complained of stabbing pain to the left of the sternum, lasting from 10 to 30 minutes. According to the visual analogue scale, chest pain was of moderate intensity (38.1 ± 5.64%, according to VAS).
Pain was provoked mainly (78%) by psycho-emotional factors and did not have a clear connection with physical activity.
6 (18.8%) women had severe weather dependence of cardialgia. All women had no positive effect from taking nitrates. In most patients, pain was accompanied by a feeling of lack of air (28.2%); palpitations (15.6%); sweating (21.9%); decreased mood and fatigue (15.6%); numbness and chilliness of the limbs (18.7%).
When performing a stress test (treadmill test), all women achieved a submaximal heart rate, at which no diagnostically significant ST segment depression was detected.
ST segment depression was not detected during information load, cold and hyperventilation tests.
In the ultrasound reaction of the brachial artery to compression of the shoulder with a cuff, 9 (28.1%) patients had a normal reaction (increase in its diameter by 15.5 ± 1.6%), 23 (71.9%) had a pathological reaction: 11 (34.4%) insufficient expansion (Dd < 10%); 7 (21.9%) had no response to the cuff test (Dd = 0%); in 5 (15.6%) patients there was narrowing of the artery (angiospasm).
When comparing the nature of the pain syndrome in the chest and the reaction of the brachial artery to the cuff test, compressive pain was noted in all 5 (15.6%) women with vasospasm (narrowing of the artery), while in case of inadequate expansion (less than 10%), the pain was predominantly of a pressing nature . Women with normal brachial artery response experienced chest discomfort, aching and stabbing pain.
All patients initially had a decrease in the amplitude of the photoplethysmogram of the fingers by 5.8 ± 0.7 mm (in the control group - 8.1 ± 0.5 mm), indicating a decrease in pulse blood flow in the subcutaneous arterioles.
A study of mental status revealed an increase in the levels of reactive (48.9 ± 2.4) and personal anxiety (53.5 ± 2.2); all patients had depression: mild in 11 (34.4%), moderate in 19 (59.3%) and severe in 2 (6.3%). All women had signs of autonomic dysfunction (average score - 39.8 ± 2.9).
During treatment with Magnerot, the well-being of all patients improved significantly. First of all, it should be noted that there was a significant improvement in the mental status of women within the first month. By the end of the 3rd month, the indicator of reactive anxiety decreased from 48.9 ± 2.4 to 35.5 ± 2.2; personal anxiety - from 48.9 ± 2.4 to 43.7 ± 0.8; depression - from 10.5 ± 1.4 to 5.1 ± 0.2 (p < 0.01).
The manifestations of menopausal syndrome decreased: the Cooperman index by the end of the 3rd month decreased to 16 ± 2.1 points.
The severity of autonomic dysfunction (initial average score - 28.7 ± 2.9) decreased within the first month of Magnerot therapy, and by the end of the 3rd month of treatment these changes reached a significant level (average score - 19.4 ± 1.9; p < 0.01).
Subjective improvement in condition at the end of the first month was also manifested in the form of a decrease in the severity of pain in the chest (decrease in the VAS score to 22.7 ± 3.0), and by the end of the 3rd month of therapy with Magnerot, complete elimination of pain in the chest was noted.
After 3 months of therapy with Magnerot, all women with a previously impaired response of the brachial artery to the cuff test experienced an increase in its diameter by more than 10% (table), which indicates restoration of the vasomotor function of the endothelium. A tendency towards a decrease in ristomycin-induced platelet aggregation in response to the cuff test can also be considered as evidence of restoration of the functional state of the endothelium: before occlusion - 7.4 ± 1.0%; after occlusion - 7.2 ± 1.1% (D% = - 2.7).
The reaction of microvessels to tests that provoke their spasm has significantly improved. The PPG amplitude increased significantly during the cold test (9.4 ± 0.8 mm; p < 0.01). The PPG amplitude increased compared to the initial one and during the information load (6.7 ± 0.8 mm) and hyperventilation (6.85 ± 0.7 mm) tests, but this difference did not reach a statistically significant level.
Thus, we can conclude that with the onset of postmenopause in women, the frequency of chest pain increases significantly, the interpretation of which is often difficult. The cause of cardialgia can be dysfunction of the autonomic nervous system [2], spasm of the coronary arteries [4] or microcirculation disorders [8].
In recent years, much attention has been paid in the literature to endothelial dysfunction as a possible cause of chest pain in postmenopausal women [11, 14]. At the same time, the connection between chest pain and endothelial dysfunction has not been sufficiently studied.
In all women with cardialgia of a compressive and pressing nature, we detected a decrease in the amplitude of the photoplethysmogram of the fingers, reflecting the pulse blood flow in the subcutaneous arterioles. When conducting cold and hyperventilation tests that provoke vasospasm, an additional, significantly more pronounced decrease in PPG amplitude was noted than in the control group. These changes can be considered as evidence of increased vascular tone and their hyperreactivity to constricting stimuli. When performing a test with reactive hyperemia (cuff test), a violation of the vascular reaction was also determined, manifested in insufficient expansion of the brachial artery, and in 5 women even its narrowing. This vascular reaction is generally considered to be a manifestation of endothelial dysfunction. The impairment of endothelial function in these patients is also indicated by an increase in ristomycin-induced platelet aggregation in response to clamping of the arm vessels with a cuff. The relationship between platelet hemostasis indicators and disturbances in the vasomotor response to the cuff test was noted by us earlier in other studies [7, 9].
All women were noted to have anxiety, depression, and autonomic dysfunction.
While taking the drug Magnerot, within 1 month the severity of pain, according to VAS, decreased from 38.1 to 22.7%, and by the end of the 3rd month the pain completely stopped.
Along with the regression of pain, there was a decrease in the severity of anxiety and depression, autonomic dysfunction and a significant improvement in well-being.
Clinical improvement was accompanied by restoration of endothelium-dependent vasodilation: after 3 months, the increase in arterial diameter was at least 12%. The amplitude of the photoplethysmogram of the fingers also increased, and its response to vasoconstrictor stimuli became the same as in the control group.
Against the background of restoration of the vasomotor function of the endothelium, a decrease in ristomycin-induced platelet aggregation in response to the cuff test was observed, which also indicated normalization of endothelial function.
The results obtained indicate a beneficial complex effect of the drug Magnerot both on psychovegetative disorders and on the functional state of the vasomotor function of the endothelium, which helps eliminate cardialgia. Our data fully coincide with the positive results of other studies [6, 13, 15].
Thus, in postmenopausal women with cardialgia, in the absence of indications for hormone replacement therapy (or the presence of contraindications), the appointment of Magnerot can be considered as pathogenetic therapy.
The use of this drug in women is of particular interest, since magnesium therapy can also significantly reduce the manifestations of premenstrual syndrome and primary dysmenorrhea, and the participation of magnesium in the formation and maintenance of bone mass may be important for the prevention of postmenopausal osteoporosis [1, 5, 6].
In the future, given the urgency of improving treatment methods for functional disorders in peri- and postmenopause, we consider it appropriate to conduct a larger randomized controlled trial.
Literature
- Belakovsky M. S. Calcium and human need for it // Nutrition issues. - 1999. - No. 6. - P. 4–8.
- Autonomic disorders. Clinic, diagnosis, treatment / Ed. A. M. Veina. - M., Medical Information Agency, 1998. - P. 53–57.
- Neurology for general practitioners. Ed. A. M. Veina. - M.: Eydoe Media, 2002.
- Gogin E. E., Gruzdev A. K., Lazarev I. A. et al. Variants of unstable angina in the light of modern ideas about the mechanisms of endothelial damage // Therapeutic Archive. - 1999. - No. 4. — 21–28.
- Zlatopolska E. Pathophysiology of calcium, magnesium and phosphorus metabolism. - M. Medicine, 1987. - 217–278.
- Zoltan PA et al. Premenstrual syndrome // Journal of Hungarian gynecologists. - 2003 No. 66. - P. 217–221.
- Ezhovskaya I. G., Vinogradova I. V. The effect of dipyridamole on platelet aggregation caused by von Willebrand factor in patients with intermittent claudication. Thrombosis, hemorrhage, DIC syndrome. Treatment problems. - M., 2000. - 69–70.
- Karpov R. S., Pavlyukova E. N., Taranov S. V. et al. Syndrome X: clinical, functional and morphological study // Cardiology. - 1999. - No. 8. - P. 19–26.
- Kirichenko A. A., Panchuk L. N., Novichkova Yu. N., Vinogradova I. V., Zubkova L. V. Comprehensive assessment of the vasomotor function of the endothelium and ristomycin-induced platelet aggregation in women with chest pain suffering from arterial hypertension, postmenopause // Regional blood circulation and microcirculation. - 2003. - No. 3(7). — P. 44-49.
- Rudakova T.P. Features of coronary heart disease in women. New St. Petersburg Medical Gazette. - 2000. - No. 1. — P. 47–50.
- Sergienko V. B., Sayutina E. V., Samoilenko L. E. et al. The role of endothelial dysfunction in the development of myocardial ischemia in patients with coronary heart disease with unchanged and slightly changed coronary arteries // Cardiology. - 1999. - No. 1 - P. 25_30.
- Born G., Schwartz C. (Ed.) Vascular Endothelium. Stuttgart. —1997.
- De Souza MC et al. A synergistic effect of a daily supplement for 1 month of magnesium for relief of anxiety-related premenstrual symptoms: a randomized, double blind, crossover study. - J Womens Health 2000, 9: 131–139.
- Quyyumi AA, Cannon ROIII, Panza JA et al. Endothelial dysfunction in patients with chest pain and normal coronary arteries. Circulation 1992; 86:1864–1871.
- Walker A. et al. Magnesium supplementation alleviates premenstrual symptoms of fluid retention. - J Womens Health 1998, 7,1157–1165.
A. A. Kirichenko , Doctor of Medical Sciences, Professor O. N. Flegentova Yu. N. Novichkova , Candidate of Medical Sciences, Associate Professor I. V. Vinogradova , Candidate of Medical Sciences A. A. Ryazantsev , Candidate of Medical Sciences K. V. Yurchenko RMAPO, Central Design Bureau No. 1 of JSC Russian Railways, Moscow
Side effects
The medicine in tablet form is well absorbed by the body, but if you neglect the established treatment regimen and regularly exceed the dose, then unwanted reactions may occur. They may manifest as stomach upsets. In this case, you need to reduce the dose and expect relief.
In practice, there are cases when urticaria, skin itching and rash appeared after taking it. If such manifestations occur, you need to contact a specialist who will adjust the treatment regimen.
Overdose
If the dose is exceeded, magnesium intoxication may occur. With normal kidney function, such a problem is almost impossible. Excess of the substance can lead to the following conditions:
- gag reflex, diarrhea, pain in the abdomen;
- paralysis of the respiratory muscles;
- violation of the patency of the stomach and bile ducts.
To cope with such conditions, you need to consume as much potassium as possible. It is also necessary to take in as much water as possible.
Overdose of the drug Magnerot, symptoms and treatment
The manifestations of the described adverse reactions may increase. With full renal function, magnesium intoxication rarely occurs. With magnesium intoxication, symptoms from the central nervous system (nausea, vomiting, bladder obstruction, constipation, paralysis of the respiratory system) and cardiac symptoms (deterioration of atrioventricular conduction and excitation from the ventricles), as well as a curare-like effect on neuromuscular conduction are noted. Magnesium intoxication is treated with intravenous calcium (100–200 mg Ca2+). Additionally, hemodialysis, peritoneal dialysis and artificial respiration may be needed.
special instructions
The drug can be stored for 5 years from the date of manufacture. Should be kept in a dry place at room temperature away from children.
The medicine should not be used in parallel with sodium fluoride and iron salts. The combination of Magnerot with tranquilizers and sedatives enhances their effect on the body.
The medication can be purchased at a pharmacy. No doctor's prescription required. On average, the medicine costs 380-500 rubles.
The drug and its analogues do not in any way affect the ability to drive a vehicle or operate other mechanisms that require increased attention.
Magnerot tablets 500 mg, 50 pcs.
Manufacturer
Peak-Pharma Lek, Russia
Compound
For 1 tablet:
Active ingredient: magnesium orotate dihydrate - 500 mg;
Excipients: colloidal silicon dioxide, croscarmellose sodium, microcrystalline cellulose, corn starch, povidone K30, lactose monohydrate, sodium cyclamate, talc, magnesium stearate.
pharmachologic effect
Pharmacotherapeutic group: magnesium drug
ATC code: A12CC09
Pharmacological properties
Pharmacodynamics
Magnesium preparation. An essential macronutrient, magnesium carries out more than 300 enzymatic reactions, regulates cellular permeability and neuromuscular excitability. Necessary for many energy processes, participates in the metabolism of proteins, fats, carbohydrates and nucleic acids. Magnesium has a curare-like effect on the terminals of cholinergic neurons, with a decrease in the release of acetylcholine; magnesium and calcium interact in the body partially synergistically; however, when competitively inhibiting calcium, magnesium can also affect its binding sites as a "physiological calcium antagonist".
Pharmacokinetics
Approximately 35-40% of the dose taken is absorbed. Hypomagnesemia stimulates the absorption of magnesium ions. The presence of orotic acid salts improves the absorption of magnesium.
Magnesium is excreted by the kidneys; excretion decreases with magnesium deficiency and increases with its excess.
Indications
Established magnesium deficiency, isolated or associated with other deficiency conditions, accompanied by symptoms such as increased irritability, minor sleep disturbances, gastrointestinal cramps, increased fatigue, muscle pain and spasms, and a tingling sensation in the muscles.
If after a month of treatment there is no improvement in these symptoms, continuing treatment is not advisable.
Use during pregnancy and breastfeeding
The drug Magnerot® can be used during pregnancy only on the recommendation of a doctor.
Magnesium passes into breast milk. The use of the drug should be avoided during breastfeeding.
The use of the drug during pregnancy and lactation is possible if the potential benefit to the mother outweighs the potential risk to the fetus and child.
Contraindications
Hypersensitivity to the components of the drug, urolithiasis, renal dysfunction, predisposition to the formation of calcium-magnesium-ammonium phosphate stones, myasthenia gravis, atrioventricular block, liver cirrhosis with ascites, children under 18 years of age, lactose intolerance, lactase or glucose deficiency galactose malabsorption (due to the presence of lactose in the composition).
Side effects
The incidence of adverse reactions cannot be determined based on the available data.
Gastrointestinal disorders: unstable stool and diarrhea, which resolve on their own when the dose of the drug is reduced.
From the immune system: allergic reactions.
If any of the side effects listed in the instructions get worse, or you notice any other side effects not listed in the instructions, tell your doctor.
Interaction
When taking magnesium-containing drugs simultaneously with iron, sodium fluoride and tetracyclines, absorption of the latter may decrease. In addition, aminoquinolines, quinidine, and penicillamine should not be administered simultaneously with magnesium preparations. Therefore, these drugs should be taken at intervals of 2-3 hours. Oral contraceptives, diuretics, muscle relaxants, glucocorticosteroids, insulin reduce the effect of the drug.
Magnesium should be used with caution if you are taking medications that contain magnesium, such as antacids or laxatives, or potassium-sparing diuretics or medications that contain calcium. When used simultaneously with drugs containing aluminum, the absorption of aluminum in the body may be increased.
Magnesium should be used with caution when used concomitantly with digitalis preparations as concurrent use may interfere with the absorption of digitalis preparations.
Some antibiotics (aminoglycosides), cisplatins and cyclosporine A may lead to increased excretion of magnesium.
Some diuretics (thiazides and furosemide), cetuximab and erlotinib, proton pump inhibitors (omeprazole and pantoprazole), foscarnet, pentamidine, rapamycin and amphotericin B may cause magnesium deficiency and thus reduce the effect of Magnerot®.
How to take, course of administration and dosage
The tablets are taken orally before meals with a small amount of water.
2 tablets 3 times a day for 7 days, then 1 tablet 2-3 times a day daily. The duration of treatment is 4 weeks. Treatment should be stopped immediately after normalization of magnesium concentration in the blood.
Overdose
With normal kidney function, oral magnesium does not cause toxic reactions. Magnesium poisoning can develop in kidney failure. Toxic effects mainly depend on serum magnesium concentration.
Symptoms: decreased blood pressure, nausea, vomiting, depression, slowed reflexes, respiratory depression, coma, cardiac arrest, anuric syndrome.
Treatment: rehydration, forced diuresis; in case of renal failure, hemodialysis or peritoneal dialysis is necessary.
Description
White or almost white round flat tablets with bevels on both sides and a score on one side.
Special instructions
The drug contains lactose monohydrate, therefore its use is not recommended for patients with hereditary galactosemia, glucose-galactose malabsorption syndrome or lactase deficiency.
Impact on the ability to drive vehicles and machinery
The drug does not affect the ability to drive vehicles or operate machinery.
Release form
pills
Storage conditions
At a temperature not higher than 25 °C.
Keep out of the reach of children.
Best before date
5 years
Active substance
Magnesium orotate
Dosage form
pills
Barcode and weight
Barcode: 4030674000194, 4630016120230 Weight: 0.051 kg
Is it possible to take Magnerot during pregnancy?
From an objective point of view, the drug can be prescribed to women during pregnancy. But even a slight excess of the dosage can cause serious consequences, including miscarriage. Therefore, Magnerot can be taken only as prescribed by a doctor, if the expected benefit significantly outweighs the possible danger to the baby.
Reviews from pregnant women indicate that if the treatment regimen is followed, the drug is well tolerated by the body.
Some experts prescribe the drug for severe swelling, increased blood pressure, and tremors in the arms and legs. For edema, magnesium can be given to pregnant women at 4-8 months. The medicine also improves uterine blood flow, which has a positive effect on the condition of the pregnant woman.
The use of magnesium preparations for cardiovascular diseases in children
Magnesium, which is involved in ensuring the most important biochemical and physiological processes in the body, as well as influencing energy, plastic, and electrolyte metabolism, is currently considered one of the most important intracellular microelements. Being a universal regulatory factor, magnesium has a normalizing effect on the functional state of almost all organs and systems (Table 1).
Under physiological conditions, magnesium enters the body with food and water. Magnesium is absorbed throughout the entire intestine, but the bulk of it is absorbed in the duodenum. It is known that the body absorbs only up to 35% of magnesium from food. Magnesium absorption may be increased in the presence of vitamin B6 and certain organic acids (lactic, orotic and aspartic).
The absorption of magnesium in the gastrointestinal tract decreases when there is a large amount of protein and fat in the diet, since magnesium forms insoluble or sparingly soluble compounds with them. Magnesium absorption decreases with excess calcium and phosphates.
The total magnesium content in the adult human body is about 25 g. The percentage of magnesium in various organs and tissues is shown in the figure. In the blood, 60–75% of magnesium is in ionized form.
Magnesium balance is regulated by the kidneys. They can reabsorb up to 99% of the magnesium filtered through the glomerular membrane. Up to 100 mg of magnesium is excreted in the urine per day. Magnesium losses in urine increase under the influence of catecholamines and corticosteroid hormones, which explains the mechanism of deficiency of this microelement during stress. With a reduced intake of magnesium from food, its excretion by the kidneys decreases, and with excess, it increases.
According to the Institute of Nutrition of the Russian Academy of Medical Sciences, the magnesium requirement of an adult is 300–400 mg per day. At the same time, at a young age, in people engaged in physical labor, athletes, pregnant and lactating women, the need for magnesium may increase by an additional 150 mg per day. The recommended average daily intake of magnesium is as follows [3]:
- children under 12 months - 55–70 mg;
- from 1 to 3 years - 150 mg;
- from 4 to 6 years - 200 mg;
- from 7 to 10 years - 250 mg;
- from 11 to 17 years - 300 mg;
- men - 350 mg;
- women - 300 mg;
- pregnant and lactating women - 450 mg.
The magnesium content in food (mg per 100 g of product) is as follows (4):
- buckwheat groats - 200;
- rolled oatmeal - 129;
- oatmeal - 119;
- wheat cereal - 88;
- rice cereal - 48;
- wheat grain bread - 74;
- rye bread - 47;
- whole milk powder - 119;
- skimmed milk powder - 160;
- condensed milk - 34;
- buckwheat groats - 200;
- cheese - 50;
- fish products - 116;
- watermelon - 224;
- peas - 90;
- spinach - 83;
- Brussels sprouts - 42;
- salad - 40;
- carrots - 38;
- raisins - 42;
- hazelnuts - 191.
The prevalence of magnesium deficiency in the population ranges from 16 to 42% [5].
The main causes of magnesium deficiency in the body:
- reduction in consumption (dietary restrictions, heat treatment of foods, excess carbohydrates and fats in the diet);
- increased need (stress, physical overexertion, physical inactivity, periods of growth, pregnancy and lactation, condition after viral and bacterial diseases);
- impaired absorption of magnesium in the intestine associated with diseases of the gastrointestinal tract;
- increased excretion by the kidneys in diseases of the urinary system;
- endocrine pathology (hyperthyroidism, hyperparathyroidism, hyperaldosteronism, diabetes);
- drug therapy (glucocorticosteroids, cytostatics, aminoglycosides).
Magnesium deficiency has no pathognomonic clinical signs. However, the polysymptom nature of this condition makes it possible, based on the clinical picture, to suspect magnesium deficiency in the patient with a high degree of probability.
Clinical manifestations of magnesium deficiency in the body
Cardiovascular: vasospasm, arterial hypertension, myocardial dystrophy, tachycardia, arrhythmias, increased QT interval, tendency to thrombosis, development of atherosclerosis, pathological course of pregnancy (toxicosis and gestosis).
| Drawing. Distribution of magnesium in the body |
Neurological: chronic fatigue syndrome, autonomic dysfunction, decreased attention, depression, fear, anxiety, dizziness, migraine, sleep disorders, paresthesia, tetany.
Visceral (except cardiovascular): bronchospasm, laryngospasm, hyperkinetic diarrhea, spastic constipation, pylorospasm, nausea, vomiting, biliary dyskinesia and cholelithiasis, diffuse abdominal pain, formation of kidney stones.
Muscular: skeletal muscle cramps, increased uterine contractility (miscarriages, premature birth).
To assess magnesium content in the body, various methods are used:
- determination of intracellular magnesium content in erythrocytes and mononuclear cells;
- study of magnesium levels in hair;
- determination of magnesium excretion in urine (stress test);
- assessment of magnesium concentration in blood plasma (norm - 0.8–1.1 mmol/l).
The most common method is to measure plasma magnesium concentrations, but its clinical value is limited. Since Mg++ is an intracellular ion, its concentration in serum is not very informative for assessing its total amount in the body and diagnosing deficiency. Only the presence of hypomagnesemia indicates Mg++ deficiency. In case of hidden (intracellular) deficiency, this indicator remains within the normal range [5].
Having many clinical effects, magnesium is widely used as a medicine for various diseases, and especially for pathologies of the cardiovascular system.
In pediatric practice, for diseases of the cardiovascular system, it is considered advisable to prescribe drugs such as Magnerot, Magne B6, asparkam (Panangin), magnesium citrate (Natural Kalm), as well as medicinal mineral water enriched with magnesium (Donat Magnesium). The latter contains magnesium in an active ionized form (more than 1000 mg/l).
We studied the effectiveness of therapy with magnesium preparations in 35 children and adolescents with cardiorheumatic diseases.
As a source of magnesium, medicinal mineral water Donat Magnesium was prescribed at the rate of 3 ml/kg body weight (single dose) 15–20 minutes before meals, 3 times a day. Course duration: 3 weeks.
After a course of treatment with mineral water, there was a significant (p < 0.05) decrease in the frequency of clinical manifestations of neurovegetative disorders in the majority of the examined patients. At the same time, the most significant dynamics were such clinical manifestations as cardialgia, tachycardia, increased blood pressure (BP), headaches, dizziness, weakness, fatigue, anxiety and irritability, and impaired sleep quality.
The use of magnesium therapy was accompanied by a hypotensive effect in almost all patients. However, complete normalization of blood pressure occurred in 62.5% of cases. In 33.3% of patients (7 people), only a tendency to a decrease in blood pressure was observed. These were children with arterial hypertension during adolescence.
The results of the study showed that magnesium has a clear hypotensive effect with an increase in blood pressure caused by the prevailing sympathicotonic influences in children with autonomic dysfunction. The data obtained are consistent with the authors' opinion about the depressant effect of magnesium on the activity and release of catecholamines, and the partial blockade of adrenaline-sensitive receptors. The influence of magnesium on the central mechanisms of blood pressure regulation cannot be ruled out [9].
The emerging positive dynamics of blood pressure in arterial hypertension indicated the advisability of increasing the duration of the course of magnesium therapy to 4–5 weeks. If it is necessary to prescribe antihypertensive drugs, magnesium preparations should be recommended as a component of combination therapy for arterial hypertension in adolescents.
The positive dynamics of the ECG serves as convincing evidence of the presence of cardiotrophic, antiarrhythmic, vegetotropic effects of magnesium therapy.
A number of medications containing magnesium have been used and continue to be introduced in pediatric cardiology practice. The latter differ in magnesium content, its combinations with various biologically active substances and the mechanisms of their complex effects. Such medicines include the following.
Magnerot is a magnesium salt of orotic acid. One tablet contains 500 mg magnesium orotate (32.8 mg magnesium). Orotic acid stimulates the synthesis of adenosine triphosphate (ATP). Since 90% of intracellular magnesium is bound to ATP, a relative increase in the intracellular ATP store through orotic acid improves the fixation of magnesium in cells. The treatment regimen in different age groups is presented in Table 2.
| Table 2 Recommended doses of the drug Magnerot depending on age [6] |
Magne B6 . Available in tablets or oral solution. One tablet contains 48 mg of magnesium and 5 mg of pyridoxine. One ampoule of solution (10 ml) contains a total of 100 mg of magnesium and 10 mg of pyridoxine. For children weighing more than 10 kg (after one year), it is recommended 5–10 mg per kg of body weight (for magnesium) per day, in two or three doses; children over 12 years old - 3 tablets per day, in three doses.
Asparkam (panangin). One tablet contains 36.2 mg of potassium ion and 11.8 mg of magnesium ion.
Magnesium citrate (natural calm) is an aqueous solution of magnesium carbonate and citric acid. In the body, magnesium citrate normalizes the acid-base balance in conditions of acidosis in various pathological conditions, and especially hypoxia. The above makes its use justified for cardiovascular pathology in children. In addition, citrates are ideal conductors of various biologically active substances into cells; they help neutralize toxins. Due to the interaction of magnesium and citrate, their clinical effects in the body are enhanced.
One teaspoon of the drug solution contains 205 mg of elemental magnesium. For children under 10 years old, it is recommended to take 1/4 teaspoon 1–2 times a day; for children over 10 years old, up to 1/2–1 teaspoon (in the absence of diarrhea).
cardiomagnyl as an antiplatelet agent - a compound of acetylsalicylic acid and magnesium hydroxide (in a tablet - 75 and 15.2 mg, respectively), where the latter plays a protective role, as a non-absorbable fast-acting antacid, has a cytoprotective effect and prevents possible damage to the mucous membrane stomach with acetylsalicylic acid [10, 11].
Cardiomagnyl can be used:
- in adolescents with arterial hypertension who have excess body weight, hyperlipidemia, a tendency to hypercoagulation with a family history of cardiovascular diseases [12];
- in children with subacute and chronic coronaritis, the causes of which were Kawasaki disease, infective endocarditis; as well as for systemic vasculitis, when long-term maintenance antiplatelet therapy is required (at a rate of 1–2 mg/kg).
Thus, a generalization of literature data and analysis of the results of our studies allows us to recommend therapy with magnesium preparations in children and adolescents with diseases of the cardiovascular system in the following conditions:
- vegetative dystonia in sympathicotonic and mixed variants;
- arterial hypertension of adolescence;
- myocardial dystrophy (infectious-toxic cardiopathy);
- heart rhythm disturbances (extrasystole, sinus tachycardia, acquired secondary QT interval prolongation syndrome);
- prevention of arrhythmias in patients undergoing heart surgery [6];
- latent magnesium deficiency;
- taking medications that promote accelerated excretion of magnesium.
Literature
- The use of medicinal mineral water “Donat Mg” for somatic pathology in children: A guide for pediatricians / ed. prof. N.A.Korovina. M., 2004.
- Tereshenko N.P. The role of magnesium in maintaining acid-base balance // Abstracts of the report of the IV Russian Congress of Pediatricians, October 2005.
- Tutelyan V. A., Spirichev V. B., Sukhanov B. P., Kudasheva V. A. Micronutrients in the diet of a healthy and sick person: A reference guide to vitamins and minerals. M., 2002. pp. 174–175.
- Skalny A.V. Microelements for your health. M., 2003. pp. 81–85.
- Gorodetsky V.V., Talibov O.B. Magnesium preparations in medical practice. Small encyclopedia of magnesium. M., 2004.
- Altura BM Basic biochemistry and physiology of magnesium. A brief review. Magnesium and Frace Elements 1991; 10: 167–171.
- Kroll MN Elin RJ Relationships between magnesium and protein concentrations in serum // Clin. Chem. 1995; 31: 244–246.
- Shkolnikova M.A. Metabolism of magnesium and the therapeutic value of its preparations. - M., 2002. 28 p.
- Davies AO, Mares A., Pool JL, Taylor AA Mitral valve prolapse with symptoms of beta-adrenergic hypersensitivity. Beta 2-adrenergic receptor supercoupling with desensitization on isoproterenol exposure // Amer. J. Med. - 1987; 82 (2): 193–201.
- Ostroumova O. D. Acetylsalicylic acid is the number one drug for the treatment of cardiovascular diseases: main indications for use, clinical benefits, effective doses and ways to increase tolerability // Breast Cancer. 2004. T. 11. No. 5. P. 275–281.
- Barkagan Z. S., Kotovshchikova E. F. Comparative analysis of the main and side effects of various forms of acetylsalicylic acid. 2004, 13 (3).
- Leontyeva I.V. Lectures on pediatric cardiology. M., 2005. pp. 17–30.
N. A. Korovina , Doctor of Medical Sciences, Professor T. M. Tvorogova , Candidate of Medical Sciences, Associate Professor L. P. Gavryushova , Candidate of Medical Sciences, Associate Professor RMAPO, Moscow
Which is better: Magnesium B6 or Magnerot
A direct analogue of Magnerot is Magnesium B6. Both drugs have a similar effect on the body, but their structure is different.
The Magnerot medication contains exclusively magnesium compounds, while Magna B6 contains pyridoxine. The action of the drugs is aimed at replenishing the lack of magnesium in the body. Magne B6 cannot be classified as a cheap analogue.
If you have heart disease, high blood pressure, migraines, or excessive sweating, it is better to take Magnerot, since this medicine is aimed specifically at treating problems with the heart and blood vessels.
Cheaper but effective analogues include: Magnelis B6, Vitrum mag. The latter drug replenishes not only the lack of magnesium in the body, but also calcium.
Special instructions for the use of the drug Magnerot
Magnerot can be used for a long time in conditions associated with magnesium deficiency. It should be taken into account that magnesium deficiency in the body can be caused by diseases of the gastrointestinal tract, consumption of foods with reduced magnesium content, chronic alcoholism (due to decreased resorption of magnesium in the renal tubules and increased excretion of magnesium from the body), taking certain medications ( oral contraceptives, diuretics, muscle relaxants, glucocorticoids, insulin), conditions that require increased magnesium intake (physical inactivity, stress, sports, pregnancy). With simultaneous treatment with iron preparations, tetracycline, sodium fluoride, the interval between taking magnesium preparations and these drugs should be 2-3 hours. The use of the drug during pregnancy and breastfeeding is possible, since during this period the need for magnesium increases significantly. If its content in the body is not balanced, it can lead to serious complications for both mother and child.