Ingredients In two capsules: Vitamin D3 (as cholecalciferol) - 500 IU (125% DV) Calcium (from 80% magnesium oxide, 10% calcium citrate, 10% calcium malate) - 500 mg (50% DV) Magnesium ( from 80% magnesium oxide, 10% magnesium, 10% calcium malate) - 250 mg (63% DV) Zinc (from L-OptiZinc monomethionine) - 7.5 mg (50% DV) Copper (from Copper AAC) - 0.5 mg (25% DV) Manganese (from Manganese AAC) - 2.5 mg (125% DV) Trace Mineral Concentrate - 50 mg
Directions for use: 2 capsules per day, separately, during meals.
Warning: For adults only. Consult your physician if you are pregnant, nursing, taking medications, or have a medical condition. Keep out of the reach of children. The product may change color naturally. After opening, store in a cool, dry place.
Natural dietary supplement “Calcium-magnesium + D3” to maintain vitamin and mineral balance
"Calcium-magnesium + D3" from NOW Foods is a complex of minerals and vitamins necessary for the normal functioning of the body. It contains a wide range of elements that promote the absorption of nutrients, primarily magnesium and calcium. Deficiency of the latter can cause a wide variety of diseases.
Calcium, magnesium and zinc
Have you noticed that after working out at the gym your appetite increases? This is how the body requires nutrients, which it actively used during exercise to replenish the energy balance and maintain the performance of all organs in emergency conditions (and this is how our body perceives physical activity). Food can cover the cost of nutrients only in the case of rare workouts. If you exercise consistently, you cannot do without vitamin-mineral complexes. First of all, you should pay attention to vitamins, calcium, magnesium and zinc, because they are involved in the largest number of biochemical processes. We will talk about the role of the above minerals today.
Maintaining balance is the key to health
Calcium is responsible for the functioning of the muscular system and the musculoskeletal system. Its deficiency leads to brittle bones and muscle weakness. A person suffering from its deficiency is susceptible to various injuries. Even a simple fall can turn into a fracture. This effect is especially pronounced in older people.
It is worth noting that consuming foods rich in calcium does not guarantee its absorption by the body. Therefore, even with proper nutrition, its deficiency can often occur. The solution to the problem is to consume a certain complex of vitamins and minerals. Dietary supplement Cal-Mag Caps 240 capsules contains, in addition to calcium, magnesium, vitamin D3 and a number of other nutrients. This tandem provides the body with the necessary vitamins and microelements. To do this, it is enough to take 2 tablets per day.
The elements included in the preparation “Calcium-magnesium + D3” are also of no small importance for increasing the body’s performance. Magnesium improves stress resistance, helping to cope with negative experiences. In addition, it is directly involved in the transmission of nerve impulses.
Manganese promotes the production of enzymes responsible for the formation of sex hormones. Boron regulates enzymatic processes in the body. In addition, it normalizes the amount of female sex hormones. Copper is responsible for generating energy at the cellular level, and zinc maintains normal acid-base balance.
Magnesium deficiency
Mg is excreted through sweat, so athletes very often face magnesium deficiency. They immediately understand that the level of magnesium from B6 has dropped sharply. Guess how? That's right, magnesium and cramps in the calf muscles or toes are inseparable concepts. This occurs due to decreased energy production in the mitochondria and the development of fatigue.
But such a nuisance as “magnesium deficiency” can also manifest itself through:
- tics;
- abdominal cramps;
- cardiopalmus;
- arrhythmia;
- hypertension;
- dizziness;
- headache;
- anxiety;
- sleep disturbance.
INTERESTING! According to statistics, 60% of adults and 65% of athletes suffer from magnesium B6 deficiency.
Introduction
In contrast to medicinal substances foreign to the human body, pharmacotherapy based on natural micronutrients (vitamins, minerals and trace elements) has characteristic features [1].
The physiological level of vitamins and minerals in the body is not zero, it is maintained in a narrow range of values; there are endogenous regulatory mechanisms for its maintenance - homeostatic mechanisms. These homeostatic processes include:
- mechanisms of distribution, binding to specific carriers in the blood plasma (transferrin for iron, ceruloplasmin for copper);
- storage (eg, red blood cells for folate, bone tissue for calcium; enterohepatic passage for vitamin D and folate);
- maintenance of plasma levels of vitamins and minerals through a feedback mechanism due to changes in intestinal absorption activity, excretion through renal excretion or excretion in bile (for example, for calcium, magnesium and vitamin D [2]).
If minerals and trace elements are not metabolized in the body, then a defensive response is triggered in relation to xenobiotic drugs - elimination “as early as possible”, their normal physiological level in the blood plasma is “zero”. Effective “machines” for xenobiotic elimination, as a rule, wait for it in two places - the liver and kidneys, and the task of the xenobiotic drug is to avoid them in order to find, firmly bind and block/activate its target of therapeutic action (for example, calcium channels, β- adrenergic receptors, key enzymes of cholesterol synthesis, etc.).
Micronutrients usually act in concert in the body. Intestinal absorption and subsequent metabolism of a given nutrient is highly dependent on the availability of other nutrients. The essential nature of micronutrients implies their interaction at all stages: absorption, distribution, intracellular transport, renal excretion. Deficiency or excess consumption of micronutrients from food, taking medications and dietary supplements containing individual macroelements and vitamins can change the physiological balance of calcium/magnesium/vitamin D, contributing to the development of pathological conditions (nephrourolithiasis, calcification of arteries and soft tissues) [3].
Balance of calcium and magnesium intake, possible consequences of its violation
Although much is known about magnesium, attention to its interaction with calcium and vitamin D has only recently come to light. The impetus for these studies was evidence that from 1977 to 2012, calcium intake in populations eating modern foods* increased by 2–2.5 times compared with magnesium intake. As a result, the ratio of calcium and magnesium intake exceeded 3.0 [4].
Altering the balance of calcium and magnesium intake in combination with taking calcium and vitamin D supplements in the presence of suboptimal magnesium intake may have adverse health consequences [5].
Elevated plasma phosphate and calcium levels correspond to an increased risk of coronary heart disease (CHD), stroke, and mortality. The Atherosclerosis Risk in Communities (ARIC) study, which followed a cohort of 15,700 people over 10 years, confirmed that elevated calcium levels (odds ratio [OR] 1.16, 95% confidence interval [CI] 1.07–1.26; p=0.0005) and phosphate (OR – 1.11, 95% CI – 1.02–1.21; p=0.0219) in blood plasma serve as a risk factor for these diseases [ 6].
Excess calcium from dietary supplements can lead to magnesium deficiency, increasing the risk of arterial calcification [5].
The main element contained in calcified atherosclerotic plaque (AB) is calcium hydroxyapatite, which contains up to 40% calcium, and its chemical structure is identical to calcium hydroxyapatite contained in bones. The degree of coronary artery calcification can be quantitatively reflected using the coronary calcium index (CCI). It has been shown that CCI correlates with the severity of coronary atherosclerosis, the presence of hemodynamically significant stenoses of the coronary arteries and the risk of developing coronary complications [7].
The results of clinical studies demonstrate a relationship between calcification of the coronary arteries and their atherosclerotic lesions, with the area of calcification accounting for approximately 1/5 of the area of coronary arteries [8]. In other words, although the amount of coronary calcium is closely related to the total mass of vulnerable ABs, calcification represents only the tip of the iceberg. The determined volume of calcified ABs is 20% of their total mass.
Most ABs contain calcifications; the overall severity of atherosclerotic arterial lesions (AB volume) correlates with the severity of calcification; the frequency of calcifications increases with age [9].
An increased risk of cardiovascular complications in patients with rheumatic diseases has also been associated with coronary calcification [10], which is associated with increased mortality from both cardiovascular and other causes. Calcification of cardiac tissues and vessel walls is a process that often develops in chronic kidney disease (CKD), which is one of the main causes of the development of cardiovascular diseases (CVD) and increased mortality rates among this category of patients. Its prevalence is highest among patients with severe CKD [11].
One of the most common indications for prescribing calcium-containing drugs is the prevention of osteoporosis of various origins. When analyzing the age and gender characteristics of atherosclerotic vascular lesions, another important aspect attracts attention - the relationship between atherocalcinosis and changes in bone mineral density. No one is surprised by the deterioration of bone tissue with age, and this is explained by the close biological and pathogenetic connections between atherosclerotic calcification and osteogenesis [12]. A significant increase in calcium deposition in the coronary arteries has been proven with a decrease in bone density and an increase in the risk of myocardial infarction.
E. Schulz et al. found that patients with severe vessel wall calcification often have low bone density and that significant bone loss in these individuals correlates with more rapid progression of abdominal aortic calcification, while low bone mineral density values correlate with non-calcified AB [13].
The estimated CVD risk associated with total calcium intake may depend on the source of calcium intake. Dietary calcium intake has not been shown to increase the risk of CVD, whereas calcium supplementation has been associated with an increased risk of myocardial infarction. Similarly, dietary calcium intake may reduce the risk of kidney stones, whereas calcium supplementation may increase the risk of nephrolithiasis [14]. One explanation for this apparent paradox may be that acute administration of large loading doses of calcium supplements may transiently increase plasma calcium concentrations [15], which in turn may lead to vascular calcification and other adverse side effects. One potential mechanism underlying the association between calcium intake and CVD risk may be the progression of atherosclerosis. The assessment of coronary artery calcification is a well-established surrogate marker of the severity of atherosclerosis and is a predictor of CVD risk [16].
Excessive calcium in the diet, especially excessive intake of calcium supplements taken to prevent or treat osteoporosis, can have unexpected health consequences. This is evidenced by data from the Multi-Ethnic Study of Atherosclerosis (MESA), carried out by experts from 8 US universities, the results of which were published by several independent groups. At the beginning of the study, all participants (5448 patients aged 45−84 years without clinical signs of CVD) reported their dietary habits to determine how much calcium they consumed in dairy products, greens and grains, what medications and dietary supplements they took . Multislice computed tomography was used to determine coronary artery calcification. After 10 years, it was repeated to assess the risk of developing coronary artery disease.
Based on data published in the Journal of the American Heart Association, the authors concluded that excess calcium intake from dietary supplements increases the risk of hypertension and CVD development by 22% over 10 years [17]. At the same time, patients who followed a healthy diet with a predominance of calcium-rich foods had a 27% lower likelihood of CVD.
The 10-year follow-up results from the MESA study also demonstrate that high CCI increases the risk not only of CVD, but also of cancer, CKD, and chronic obstructive pulmonary disease. Findings from this part of the MESA study were published in the Journal of the American College of Cardiology: Cardiovascular Imaging [18]. In 68% of 710 patients diagnosed with cancer, the ICI was high. After adjustment for other factors, it was found that in persons with CCI >400, the relative risk of developing cancer increased by 53% (OR - 1.53, 95% CI - 1.18-1.99). The incidence of CKD in persons with zero CCI was 3%, with CCI > 400 – 13%.
At the same time, the results of another clinical study performed earlier do not support the assumption of an increased risk of CVD with the use of calcium supplements [19].
Based on a meta-analysis of existing data, another group of researchers concluded that calcium supplements do not increase the risk of CVD compared with placebo when taken by healthy people in daily doses not exceeding 500–2000 mg [20].
The key role of magnesium in maintaining calcium metabolism
One of the possible causes of the development of hypercalcemia and hypercalciuria is magnesium deficiency. However, until now, determining the level of magnesium in blood plasma has not become the norm in real clinical practice, because it is believed that this indicator only indirectly and very approximately reflects its content inside the cell.
About 60% of serum magnesium is in ionized form, the rest is associated with proteins, phosphates, and citrates. Blood plasma and red blood cells contain less than 1% of the total amount of magnesium. The heart accounts for about 20% of all magnesium contained in the human body, which indicates its great importance for normal cardiac activity [21].
Epidemiological studies have linked low magnesium levels to a higher risk of metabolic syndrome, type 2 diabetes, CVD, osteoporosis, chronic obstructive pulmonary disease, and possibly some types of cancer [4].
Magnesium is the second most abundant intracellular cation and plays a key role in bone mineralization, influencing the synthesis of active vitamin D metabolites.
According to modern understanding, any effect of magnesium or calcium depends on the calcium/magnesium ratio. As nutritionist Carolyn Dean puts it, “magnesium is key to the proper assimilation and utilization of calcium, as well as vitamin D. If we consume too much calcium without enough magnesium, the excess calcium is misused and can actually become toxic, causing these conditions. , such as nephrolithiasis, some forms of arthritis, osteoporosis and arterial calcification. The effectiveness and benefits of calcium on bone health and osteoporosis prevention are significantly impaired in the absence of adequate levels of magnesium in the body" [25].
An effective tool for correcting imbalances can be adding magnesium to the diet [26, 27]. Higher magnesium intake is associated with a lower risk of increased CCI [28], and supplemental magnesium intake improves endothelial function in patients with coronary artery disease [29].
The belief in the professional community that magnesium absorption is reduced in the presence of calcium contradicts modern ideas about the mechanisms of calcium and magnesium entry into the body [30].
The processes of calcium absorption in the gastrointestinal tract and its reabsorption in the renal tubules are mediated by two representatives of the TRP (transient receptor potential channels) superfamily** - ion channels TRPV5 and TRPV6 (Fig. 1).
The release of calcium from enterocytes is ensured by the sodium-calcium exchanger, which is a transmembrane protein of the cytoplasmic membrane that transports calcium ions out of the cell in exchange for sodium ions that enter the cell (antiport mechanism). The exchanger uses the energy stored in the electrochemical sodium gradient, passing 3 Na+ ions into the cell along the concentration gradient and removing one Ca2+ ion from the cell against the concentration gradient.
In the nephron epithelium, Ca2+-ATPase (PMCA1b), integrated into the basement membrane of kidney epithelial cells, is responsible for the reabsorption of calcium and its return to the systemic circulation.
Paracellular transport of calcium ions depends on the activity of claudin proteins 16 and 19, located in the area of intercellular contacts. The name "claudin" comes from the Latin word claudere ("to close"), which corresponds to the barrier role of these proteins. Claudins (represented by 24 proteins in humans) are the most important component of tight intercellular junctions - a paracellular barrier that controls the transport of water and ions between epithelial cells.
Claudins have four transmembrane domains, two extracellular and one intracellular loop, located in the cytoplasm at the N- and C-termini.
In turn, the expression of key participants in transepithelial calcium transport—TRPV5 and PMCA1b—is under the control of vitamin D (Fig. 2). Since all vitamin D-dependent reactions are directly dependent on the presence of magnesium, the consequence of the interaction between magnesium and vitamin D is normocalcemia.
Intracellular transport of magnesium in enterocytes of the digestive tract and kidney epithelial cells is carried out using channels of the TRPM subfamily – TRPM6 and TRPM7 (Fig. 3). The activity of these channels is controlled by epidermal growth factor (EGF), which is formed from the Pro-EGF precursor localized on the basolateral membrane of the epithelium. Transcellular magnesium transfer at the level of the basement membrane is regulated by the work of Na+/K+-ATPase.
Magnesium is a cofactor in 700–800 enzyme systems in the human body, including all vitamin D-dependent processes/reactions. The activity of the 3 main vitamin D-converting enzymes and vitamin D-binding proteins is dependent on the presence of magnesium. These include 25-hydroxylase in the liver and 1- and 24-hydroxylase in the kidneys [4]. Thus, magnesium serves as a cofactor for the biosynthesis, transport and activation of vitamin D. In turn, 1,25(OH)2D stimulates the absorption of magnesium in the intestine [2].
Magnesium deficiency manifests itself at the level of parathyroid hormone and calcitonin secretion; additional magnesium intake significantly reduces resistance to vitamin D treatment [33]. Magnesium reduces parathyroid hormone levels and works synergistically with vitamin D and calcium, stimulating the specific activity of calcitonin [31]. Calcitonin, in turn, promotes bone tissue mineralization, reducing plasma and tissue calcium levels, and prevents the development of osteoporosis, calcium nephrolithiasis and some forms of arthritis [32].
Calcium-containing preparations
Currently, pharmacological agents containing calcium are divided into several groups [34]:
- First generation drugs are drugs containing exclusively calcium compounds.
- Second-generation drugs contain a combination of calcium and vitamin D and are characterized by higher therapeutic efficacy compared to first-generation drugs.
- Third generation drugs are modern combination products that combine the most bioavailable compounds of calcium, magnesium and vitamin D, promoting balanced absorption of calcium. They are characterized by a prolonged therapeutic effect and a reduced risk of side effects associated with excess calcium in tissues.
One of these third-generation drugs is Osteocare® produced by Vitabiotics (UK). In tablet form, Osteocare is a registered drug; in liquid form, it is a dietary supplement and, importantly, the only liquid form of calcium. In addition to calcium and vitamin D (100 IU), the drug contains magnesium and zinc (see table).
Treatment with the drug is indicated for the prevention and correction of mineral and vitamin D deficiency, the prevention of calcium deficiency during periods of life characterized by an increased need for it (menopause, old age, pregnancy and lactation), as well as the prevention of systemic osteoporosis and caries. The drug has undergone a number of studies with successful results, which have proven its positive effect on bone mineral density and calcium balance; a significant decrease in bone resorption and a decrease in pain during therapy was noted [41].
Conclusion
A review of the literature indicates a possible association of coronary artery calcification and an increased risk of CVD with the intake of an additional source of calcium in the form of dietary supplements. One of the effective tools for maintaining normal calcium metabolism in the body is maintaining a calcium/magnesium balance, which can be achieved by combining medications containing calcium, magnesium and vitamin D. Magnesium is involved in the activation and functioning of vitamin D, having a normalizing effect on calcium homeostasis in the body. body. Adequate intake of calcium and magnesium is one of the important conditions for the safe prevention of osteoporosis and other age-associated diseases. When choosing a drug, you should remember not only the need for a balanced combination of vitamin D and calcium salt in the drug with a high percentage of it, but also the additional presence of a magnesium compound in such a drug.
Zinc deficiency
Lack of zinc in the hair first affects the dermis and its derivatives. You can diagnose yourself with hypozincosis if you suffer from:
- hair loss;
- fragility of nails;
- skin rashes;
- peeling of the skin;
- prolonged wound healing.
The following signs indicate that it’s time to look on the Internet for an answer to the question: “Zinc deficiency – what to do?”
- disturbance of the sense of taste and smell;
- decreased visual acuity;
- passivity, depression;
- loss of appetite;
- low immunity;
- poor memory, poor concentration.
Who needs vitamins, calcium, magnesium, zinc?
Supplements based on magnesium, calcium and zinc sulfate must be taken when:
- active training;
- frequent stress;
- abuse of alcohol, coffee or carbonated drinks;
- smoking;
- drinking chlorinated water;
- vegetarianism (the best sources of magnesium with B6 are meat dishes);
- complete rejection of dairy products;
- strict diets (by limiting yourself in calories, you limit yourself in vitamins, calcium, magnesium);
- osteoporosis;
- presence of diabetes mellitus or liver disease;
- chemotherapy;
- the appearance of the first symptoms of calcium, magnesium or zinc deficiency;
- taking hormonal medications, in particular oral contraceptives;
- problems with menstruation (especially when it comes to amenorrhea);
- menopause;
- over 40 years of age (magnesium sulfate is absorbed more slowly, and Ca is generally washed out in mature and elderly people);
- significant loss of water (for example, in the summer, when a lot of magnesium and B6 are lost through sweat, with constant use of diuretics, during vomiting);
- pregnancy;
- breastfeeding.
Vitamin D3
Vitamin D3 or cholecalciferol is one of the most important metabolites belonging to the vitamin D family. It is synthesized from 7-dihydrocholesterol in the skin under the influence of ultraviolet rays.
A certain amount of vitamin D itself, which differs from cholecalciferol by replacing several atoms in the molecule, enters the body with food. But these differences do not in any way affect the functional properties of the compound. Therefore, we can assume that there are two ways of getting vitamin D: formation in the skin and absorption from food.
The further pathway of vitamin D3 is conversion to 25-hydroxycholecalciferol in the liver, where the new compound can be stored for use in cases of vitamin D deficiency. Or the subsequent conversion of 25-hydroxycholecalciferol in the kidneys to 1,25-dihydroxycholecalciferol, the most active metabolite of vitamin D3. The synthesis process in kidney cells is controlled by parathyroid hormone (parathyroid hormone) and controlled by calcium ions. The presence of parathyroid hormone triggers the reaction of converting one substance into another. With calcium it’s exactly the opposite: the higher the calcium concentration in the blood plasma, the less 1,25-dihydroxycholecalciferol is formed.
The complex multi-level mechanism for controlling the absorption, synthesis and breakdown of vitamin D3 metabolites is explained by its enormous biological significance:
- regulation of mineral metabolism at the level of the intestines, kidneys and bone tissue to increase the absorption of calcium and phosphates;
- increased calcium deposition in bone tissue and dentin of teeth, accelerated bone formation and fracture healing;
- decreased excretion of calcium and phosphate by the kidneys;
- participation in the formation of important enzymes (ATPase and alkaline phosphatase).
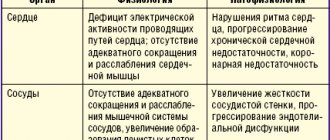
Signs of an imbalance of elements in the body