Definition
Hiccups are periodically occurring involuntary myoclonic contractions of the diaphragm with possible involvement of the intercostal muscles (usually unilateral). The contraction results in a sudden inhalation followed by closure of the glottis, which is accompanied by a characteristic sound.
Duration
Short-term – up to 48 hours; long-term – from 48 hours to 1 month; intractable – more than 1 month.
Prevalence
Prolonged, difficult-to-control hiccups are quite common in patients with advanced cancer.
Anatomy and pathophysiology
The physiological mechanism of hiccups remains unclear. The hiccup reflex arc includes:
- afferent pathways: phrenic and vagus nerve pathways, sympathetic nervous system;
- diffuse “hiccup center”: midbrain, brain stem, proximal cervical spinal cord (C3 – C5);
- central neurotransmitters: dopaminergic and gamma-aminobutyric acid (GABA);
- efferent pathways: diaphragmatic, vagus and intercostal nerve pathways, conducting signals that cause contraction of the diaphragm.
general characteristics
A sudden attack of hiccups may be preceded by overeating, fast food with poor chewing of hard and dry foods, swallowing air, and drinking highly carbonated and alcoholic drinks.
In young children and sometimes in adults, hiccups are triggered by hypothermia. Some patients begin to hiccup after taking muscle relaxants, barbiturates, benzodiazepines and other medications. Often the symptom appears for no reason and goes away on its own within a few minutes. At the time of an attack, a person experiences jerky muscle contractions in the epigastric region, accompanied by protrusion of the anterior abdominal wall and a strangled sound. Due to the closure of the glottis, breath holding occurs for a short period of time. A special feature of hiccups is the impossibility of conscious control. With intense hiccups, moderate pain is sometimes noted behind the sternum, in the lower parts of the chest. An attack of hiccups is characterized by rhythmic muscle contractions at approximately equal intervals.
Prolonged, especially pathological hiccups often have a debilitating effect and may be accompanied by irritability, emotional instability, increasing asthenia, vegetative manifestations - sweating of the palms, paleness or redness of the skin, a decrease in the temperature of the skin of the distal extremities. For episodes that repeat several times a day or several days a week, last more than an hour and are combined with other disorders (heartburn, pain, shortness of breath, etc.), you should seek medical help.
General information
Hiccups are a respiratory dysfunction caused by forced, myoclonic contraction of the intercostal muscles and diaphragm.
The contraction of these muscles occurs synchronously. Most often, contractions occur only on the left side of the diaphragm, but the entire diaphragm can be involved. Almost simultaneously with the contractions, a sudden short and intense inhalation occurs with the glottis closed, which creates the characteristic “hic” sound. Wikipedia indicates that these disorders are an involuntary physiological reaction and occur due to irritation of the phrenic nerve. This condition occurs more often in men. The most common acute hiccups are episodic, do not last long (a few seconds or minutes) and their attacks are harmless. Most often this is due to excessive filling of the stomach, which is why hiccups occur after eating or during eating. It quickly stops with any actions on the part of the person or goes away on its own.
In cases where hiccups occur frequently and in prolonged episodes, they are considered pathological. Persistent (>48 hours) causes fatigue, irritability, discomfort, insomnia and depression . If you have prolonged hiccups (more than two days) or even longer hiccups (more than 1 month), you should consult a doctor. Long-term symptoms may indicate serious illnesses and therefore require serious attention. Persistent and intractable hiccups are rare and difficult to treat.
Some causes of this pathology can be identified and eliminated with treatment. Thus, respiratory disorders due to ischemic stroke disappear with thrombolytic therapy, and hiccups due to meningitis disappear with antibacterial treatment. In this article we will look at how you can stop hiccups in adults and what methods will help stop them. Options for drug treatment that can relieve long-term hiccups will be considered, as well as surgical treatment as an option to permanently remove it if drug treatment is ineffective.
Classification
The main criteria used in systematizing the variants of hiccups are its connection with pathological conditions, development mechanisms, and duration. In most cases, hiccups are physiological in nature and are not associated with any diseases. Diaphragmatic myoclonus is called pathological, occurring against the background of various diseases and presented in such forms as:
- Central hiccups
. It is caused mainly by disturbances in the brain regulation of diaphragmatic contractions. It is observed in cases of inflammation, tumors and injuries of the brain and spinal cord. It is possible to develop hiccups with functional disorders of the central nervous system. - Peripheral hiccups
. Associated with damage to various parts of the phrenic and vagus nerves. Characteristic of volumetric processes in the mediastinum, diseases of the chest and abdominal cavity adjacent to the diaphragm. - Referred hiccups
. It is provoked by pathological conditions in organs located outside the zone of innervation of the vagus and phrenic nerve. It can be observed against the background of enteritis, colitis, helminthic infestations and diseases of the female reproductive system. - Toxic hiccups
. It becomes a consequence of poisoning of the nervous system with endo- and exotoxins. It is detected in case of poisoning with mushroom poisons, alcohol and medications (anaesthetics, drugs), uremia, diabetic coma, terminal conditions.
Physiological hiccups are usually short-lived. With pathological contractions of the diaphragm, there are episodes of transient hiccups (from several minutes to several hours), persistent hiccups lasting more than 2 days, and long-term hiccups (from a month or more). Although usually prolonged hiccups indicate the presence of pathological conditions, in rare cases it can be observed in a healthy person.
Pathogenesis
The mechanism for the occurrence of hiccups involves a “reflex arc”, consisting of afferent sections, central and efferent sections. Trauma, irritation, inflammation or pathological stimulation can occur at any part of the arch, causing persistent or intractable hiccups. The afferent pathway (branches of the phrenic, vagus nerves and thoracic sympathetic trunk) carries impulses to the hiccup center, where the signal is processed. It is located in the medulla oblongata next to the respiratory center, hypothalamus and reticular formation and in the upper part of the spinal cord (segment C3-C5). The efferent link includes motor fibers of the phrenic nerve, which innervates the diaphragm and the respiratory muscles of the chest (intercostal and scalene). The diaphragm is innervated by two phrenic nerves originating from segments CIII-CIV (neck area).
For any pathology of the abdominal or thoracic cavity, when the phrenic or vagus nerve is stimulated, the “hiccup center” is activated. The hiccup center, which controls the respiratory muscles, especially the diaphragm, is independently activated in brain diseases. In both cases, repeated myoclonic contractions of the diaphragm and respiratory muscles occur. Sometimes hiccups develop when the vagus nerve is stimulated (for example, due to bloating of the stomach and intestines).
The hiccup mechanism can be triggered by the vagus nerve when it is exposed to general irritating factors and local ones (when it is compressed along the path). The vagus nerve passes from the thoracic cavity into the abdominal cavity through an opening in the diaphragm, innervating the organs of the thoracic and abdominal cavity. Therefore, inhaled exhaust fumes and chemical gases, cigarette smoke, alcohol, spicy foods or cold drinks that irritate the gastric mucosa provoke an attack. Irritation of the vagus nerve occurs when a person eats hastily, overeats, and is in an uncomfortable position.
Causes of hiccups
Hiccups in physiological conditions
Most often, hiccups are associated with improper eating habits: fast eating, insufficient chewing of food, dry eating, smoking on an empty stomach. Hiccups are also provoked by overeating and drinking highly carbonated drinks, which leads to stretching of the stomach and irritation of the vagal receptors. With a forced position of the body, fear, or the passage of large pieces of solid food into the esophageal opening of the diaphragm, the vagus nerve can be pinched. In such cases, hiccups are protective in nature and are aimed at restoring normal innervation.
In childhood, and less often in adulthood, hiccups become a consequence of autonomic dysfunction caused by general hypothermia. During pregnancy, the increase in episodes of hiccups is potentiated by a complex of changes occurring in the woman’s body. The leading cause is an enlarged uterus, which is accompanied by an increase in intra-abdominal pressure and a displacement of internal organs towards the diaphragm. An additional factor is the increased emotionality of the pregnant woman.
Hiccups due to brain damage
The causes of hiccups in patients with brain pathology are usually irritation of structures that directly or indirectly stimulate diaphragmatic contractions. Most often, attacks of hiccups are observed in pathological formations and processes in the posterior cranial fossa. However, the occurrence of symptoms is also possible with other localization of damage. Identification of frequently recurrent and persistent hiccups may indicate the development of diseases such as:
- Cerebrovascular disorders
. Attacks of hiccups are characteristic of various types of stroke, especially hemorrhages in the ventricles of the brain. The addition of incessant hiccups is an unfavorable prognostic sign and is often a sign of deep destruction of brain tissue with damage to subcortical structures. - Inflammatory processes
. Hiccups develop as part of viral encephalitis with rubella, herpes simplex, polio, and other inflammations caused by neutrotropic viruses (tick-borne, Japanese mosquito, encephalitis lethargica, etc.). Irritation of areas of the brain that provoke hiccups is observed in meningococcal, tuberculous, fungal and other meningitis. - Cerebral space-occupying neoplasms
. Pathological efferentation, which potentiates hiccups, occurs with cysts and other space-occupying processes that compress the brain tissue. The symptom is more typical of brain stem tumors. In primary and metastatic malignant neoplasia, the situation is aggravated by irritation of neurons during tumor growth. - Brain injuries
. The causes of hiccups in patients who have suffered a traumatic brain injury are swelling of brain tissue and irritation of stem neurostructures due to intracranial hypertension. An additional factor is functional disorders of neuronal metabolism, provoked by traumatic injuries and causing pathological impulses. - Epileptic disease
. It is extremely rare that hiccups become a manifestation of simple motor paroxysm in focal epilepsy. Diaphragmatic myoclonus in such patients is the result of pathological activity of the epileptogenic focus. Often such hiccups are combined with other types of paroxysms, precede a full-blown seizure in the form of an aura, and serve as a manifestation of hyperkinesis. - Functional disorders
. Hiccups can be caused by dysfunction of the reticular formation, disruption of the secretion of individual mediators or their interaction with neuronal receptors. Such conditions are typical for patients with neuroses, somatoform dysfunction of the autonomic nervous system, and Birke syndrome. Hiccups sometimes develop during a panic attack in children.
Hiccups in spinal pathology
Since the reflex arc, which causes myoclonic contractions of the diaphragm, is closed in the cervical segments of the spinal cord, hiccups are associated with damage to the spinal tissue. Inflammation, trauma and space-occupying processes are sometimes accompanied by increased activity of motor neurons, from the processes of which the phrenic nerve is formed. In the presence of persistent hiccups, the following are excluded:
- Spinal column injuries
. Damage to the gray and white matter of the spinal cord, provoking uncontrolled contraction of the muscle fibers of the diaphragm, is observed with spinal bruises and compression fractures in the cervical region. In cases of spinal cord injuries, the appearance of continuous hiccups is considered an unfavorable sign. - Spinal neoplasms
. Pathological hiccups occur with ependymomas and other intramedullary tumors, in which segmental symptoms develop with irritation of spinal motor neurons in the area of the space-occupying process. The situation is aggravated by metabolic and destructive disorders in the damaged area. - Myelitis
. Hiccups, combined with shortness of breath, disturbances in urination and pain sensitivity, spastic paralysis of the limbs, are detected in infectious myelopathy and spinal epidural abscess with damage to the upper cervical region. The causative agents of inflammation that causes spinal injury are often HIV, syphilis, and coccal flora.
Hiccups with peripheral neuritis and neuropathies
The reflex development of pathological hiccups is observed with lesions of the spinal nerve roots, nerve plexuses and nerves connecting the diaphragm with the upper segments of the cervical cord. As an independent symptom, hiccups are rarely observed in patients. Often this manifestation is combined with other focal neurological symptoms within such pathological conditions as:
- Radicular syndrome
. With osteochondrosis, spondylosis, and intervertebral hernias, violent contractions of the diaphragm occur due to compression of the spinal roots at the level of the II-VII cervical segments, from which the phrenic nerve is formed. In addition to hiccups, patients complain of decreased sensitivity, pain in the back of the head, neck and above the collarbone, impaired tilting and turning of the head, and shoulder elevation. With tumors that compress the root, wasting of the muscles of the neck, scapula, and shoulder girdle is often detected. - Inflammation of the cervical plexus
. The combination of hiccups with severe pain, impaired sensitivity in the ears, back of the head, neck and upper chest, difficulty speaking, turning and tilting the head is characteristic of cervical plexitis. This pathological condition can be observed with sore throat, influenza, tuberculosis and other infectious diseases. A provoking factor is also compression of the plexus by enlarged lymph nodes with lymphadenitis, lymphogranulomatosis and the development of tumors in the cervical region.
Hiccups due to diaphragm pathology
The immediate cause of hiccups is the contraction of the diaphragmatic fibers; accordingly, this symptom can be detected with inflammatory, traumatic and other damage to the muscular septum separating the thoracic and abdominal cavities. The prerequisites for triggering an attack of reflex hiccups depend on the characteristics of the pathological process:
- Diaphragmatic paralysis
. The leading factor in the development of the symptom is vagal afferentation, caused by irritation of receptors against the background of displacement of the stomach and other abdominal organs, and kinking of the esophagus. In addition to periodic episodes of hiccups, patients with diaphragm relaxation complain of breathing problems, chest pain and weakness after eating, and sometimes dyspepsia. - Traumatic injuries
. Often, intractable hiccups further aggravate the symptoms of closed and open injuries to the diaphragm, exacerbating existing breathing disorders. Hiccups usually develop as a result of intense irritation of the receptors of the sensory fibers of the phrenic nerve when the integrity of the muscular septum is violated. - Diaphragmatic hernia
. Most often, hiccupping attacks are caused by compression of the vaginal nerve at its transition from the thoracic to the abdominal cavity. In the presence of a hiatal hernia, the vagus can be compressed by the cardia and the fundus of the stomach, which prolapse into the mediastinum. Hiccups are often combined with chest pain or girdle pain after eating, dysphagia, and heartburn.
Hiccups in diseases of the esophagus
The symptom of frequent or prolonged hiccups is observed with esophageal pathology, in which the vagus nerve is compressed. The direct cause of hiccups is pathological afferentation, aimed at implementing the protective reflex and restoring normal nerve conduction. Hiccups in combination with pathognomonic symptoms can manifest themselves in:
- Increase in organ volume
. The development of prolonged attacks of intractable hiccups in patients suffering from dilatation of the esophagus due to achalasia cardia, its benign tumors or cancer is due to the anatomical proximity of the organ to the vagus nerve. In addition to pathological hiccups, dysphagia and chest pain are usually observed. - Gastroesophageal reflux disease
. Constant reflux of gastric contents onto the esophageal mucosa leads to the appearance of erosions of the esophagus, aggravated by inflammatory processes. Increased afferentation along the sensory fibers of the vagus against the background of irritation of the nerve endings in the membranes of the esophagus stimulates the hiccup reflex. - Ruptures of the esophageal mucosa
. A sudden, intractable attack of hiccups is sometimes provoked by injuries to the mucous membrane in the cardioesophageal zone in Mallory-Weiss syndrome, triggering a corresponding reflex arc through the fibers of the vagus nerve. In this case, hiccups are combined with bloody vomiting and sharp chest pain.
Hiccups in diseases of the abdominal organs
In some patients, hiccups are one of the manifestations of the pathology of the digestive tract, which is associated with the peculiarities of the passage of the phrenic-abdominal branches of the phrenic nerves and their anastomosis with the sympathetic plexus of the diaphragm. An additional role is played by possible irritation of the vagus during abdominal pathological processes. An attack of hiccups can be complicated by both chronic gastrointestinal diseases (atrophic gastritis, pancreatitis) and acute pathology (intestinal obstruction due to strangulation of inguinal, umbilical and femoral hernias).
Episodes of hiccups are possible due to pathological processes in the right hypochondrium: subphrenic abscesses, attacks of cholecystitis, biliary colic. A feature of such conditions, in addition to signs of organ damage, is the identification of a phrenicus symptom, indicating irritation (irritation) of the phrenic nerve. Sometimes hiccups occur with abdominal injuries and during abdominal operations, which is associated primarily with vagal effects. Enteritis, colitis, giardiasis and helminthiasis are characterized by the so-called reflected hiccups.
Hiccups in thoracic pathology
The cause of the symptom in people suffering from cardiac, bronchopulmonary and mediastinal diseases is usually irritation of the vagus nerve passing in the mediastinum near the esophagus. When the pathological focus is localized in the diaphragm, stimulation of diaphragmatic receptors that trigger hiccups is possible. The combination of attacks of hiccups with pain radiating to the shoulder girdle and neck is characteristic of mediastinal teratomas that compress the vagus.
Hiccups that occur with dry diaphragmatic pleurisy often complicate the diagnostic search. Its combination with flatulence, abdominal tension, pain in the hypochondrium and abdominal cavity is often mistakenly interpreted as an additional sign of an acute abdomen. A similar situation is observed with leading abdominal syndrome in patients with pulmonary embolism and severe dyspeptic symptoms during pulmonary infarction. In sporadic cases, hiccups accompanied by dull pain in the chest and signs of heart failure occur in postcardiotomy syndrome.
Hiccups in gynecological diseases
Reflected hiccups are sometimes observed in pathologies of the uterus and appendages (endometritis, adnexitis, benign and malignant tumors). The mechanism of its occurrence remains unclear, although the role of complex regulatory interactions involving sympathetic and parasympathetic fibers of the visceral nervous system cannot be ruled out. In addition, autonomic dysfunction causes the development of hiccups during algodismenorrhea. Patients also experience functional disorders of many systems: dyspepsia, fainting, palpitations, etc.
Hiccups during intoxication
The appearance of agonal hiccups is an ominous sign of an unfavorable course of serious diseases and terminal conditions. Typically, the development of a symptom indicates gross metabolic disorders in the brain tissue, dysfunction of the nuclei of the medulla oblongata and subcortical structures. Hiccups of central origin are observed in severe metabolic disorders caused by functional failure of various organs and systems - hepatic, uremic and diabetic coma. Intoxication hiccups are possible with burn disease and cancer cachexia.
The most common causes of exogenous intoxications that occur with hiccups are poisoning with various substances: alcohol, drugs with muscle relaxant, sedative and anesthetic effects, and some hormonal agents. The probable cause of the symptom is considered to be brain dysfunction with an imbalance of excitatory and inhibitory influences, changes in neuronal metabolism, and the formation of foci of pathological activity.
Treatment
Non-drug
It is recommended for use before the use of medications; it is prescribed purely individually. The most common types of non-drug therapy are the following.
Changing the diet : reduce the single volume of food taken with an increase in the frequency of intake.
Use of mint infusion : helps relax the sphincters, should be freshly prepared, not used together with prokinetics that increase the tone of the muscles of the stomach and intestines and the lower esophageal sphincter.
Nasopharyngeal stimulation techniques:
- rinse your nose with cold water;
- suck cold water through a straw, swallow or suck small pieces of ice;
- swallow 1 teaspoon of dry granulated sugar;
- quickly drink two glasses of water;
- gargle with water;
- suck on lemon slices;
- swallow pieces of dry bread;
- inhale saline solution through a nebulizer;
- stretch your neck;
- massage the soft palate for 1 minute;
- stretch out your tongue with your fingers;
- press hard on your tongue.
Preventing irritation of the diaphragm : bend forward, pressing your knees to your stomach.
Stimulation of the C5 dermatome (interrupts stimulation of the hiccup neural arch):
- patting or scratching the back of the neck;
- placing a cold, safe metal object behind the collar (for example, a key);
- cold compress on the face.
Breathing manipulations:
- holding your breath;
- causing sneezing or coughing;
- frequent deep breathing (hyperventilation);
- breathing into a paper bag (hypoventilation);
- “Valsalva maneuver” (forced exhalation with the nose and mouth closed). Should not be carried out if you have a cold, because... the infection can penetrate into the middle ear cavity, and in patients with heart disease (increases blood pressure). Use caution in patients with pulmonary emphysema, primary/secondary tumor lesions of the lungs, so as not to provoke pulmonary hemorrhage.
Medication
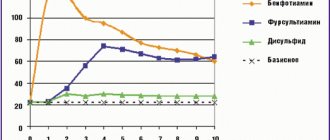
Treatment for hiccups is determined by the cause of its occurrence. In palliative care, hiccups are most often caused by several causes; as a rule, an integrated symptomatic approach is used for treatment (see Diagram 1, Appendix 1).
Table 1 shows the medications and dosages used in the treatment of hiccups. The route of administration of drugs is oral (inside), unless otherwise indicated.
Survey
A diagnostic search aimed at clarifying the causes of hiccups is carried out when it is combined with other symptoms, occurs frequently, and attacks last more than 60 minutes. The examination plan is drawn up taking into account the medical history and accompanying symptoms. Most often, primary diagnosis is carried out by a gastroenterologist, who, according to indications, involves other specialists in examining the patient. Depending on the suspected cause of the symptom, the following are used for express diagnostic purposes:
- Endoscopic studies
. Gastroscopy is the most informative method that allows you to quickly objectify pathological changes in the esophagus and stomach. If space-occupying formations, erosions and ulcers are detected during endoscopy, a biopsy is performed for histological analysis of the material. - X-ray methods
. X-ray of the abdominal cavity, X-ray examination of the chest are carried out to detect gastrointestinal pathology, relaxation of the diaphragm, pleurisy, mediastinal tumors and other possible causes of hiccups. Next, RCP and other X-ray contrast techniques are used. - Ultrasound research .
Sonography of the abdominal cavity is performed to assess the echostructure of the main parenchymal organs and identify free fluid; according to indications, it is supplemented by ultrasound of the gallbladder and liver. If pleurisy or mediastinal tumors are suspected, ultrasound of the pleural cavity and mediastinum is indicated. - Tomography
. If radiography and sonography are insufficiently informative, CT, MSCT and MRI of the abdominal or thoracic cavities and individual organs are performed. MRI of the head and spine are highly accurate in diagnosing cerebral and spinal pathologies. In difficult cases, an MRI of the whole body is performed. - Electrofunctional Research
. After excluding abdominal and thoracic causes of hiccups, electroencephalography is recommended. The method identifies foci of pathological activity in the brain. To clarify the level of damage to the nervous system, electroneurography and electromyography are also performed. - General blood analysis
. With high leukocytosis, a shift of the leukocyte formula to the left, and an increased ESR, further diagnostic search is aimed at identifying inflammatory and neoplastic processes. The analysis is often supplemented with the study of enzymes (ALT, AST) and determination of the level of C-reactive protein.
Upon receipt of preliminary information about a possible disease that provoked hiccups, further examination is carried out according to the appropriate protocol and may include a wide range of laboratory and instrumental methods. Differential diagnosis is carried out between various pathological processes in which hiccups may develop.
If you have hiccups, it is recommended to drink water in small sips.
Tests and diagnostics
For diagnosis, it is important to collect an anamnesis, as a result of which illnesses suffered, the presence of head injuries, surgical interventions on the brain and spinal cord, and manipulations are revealed. Triggers that provoke hiccups, medication use, and the patient’s attitude toward smoking and alcohol are identified.
- a full examination and examination by specialists (otolaryngologist and neurologist);
- Clinical and biochemical blood test (electrolytes, C reactive protein, urea, creatinine, amylase, liver tests);
- MRI of the brain;
- CT scan of the chest;
- electroencephalography;
- esophageal manometry;
- esophagogastroduodenoscopy;
- bronchoscopy;
- spirography;
- Lumbar puncture.
Symptomatic therapy
Episodes of physiological hiccups go away on their own within 2-10 minutes. Sometimes, to relieve them faster, it is enough to be distracted, take a deep breath 2-3 times, hold your breath for a while, or drink a couple of sips of water. If the attack continues despite distracting and reflexive methods being taken, taking into account the patient’s condition, it is recommended to contact a local or family doctor, who will prescribe further examination, or call an ambulance if the patient’s condition rapidly worsens.
Before hospitalization and examination to stop hiccups, a medical professional can stimulate some reflexogenic zones in the face and exit points of the phrenic nerve, insert a catheter intranasally to a depth of 12 cm. Sometimes an intravenous infusion of calcium preparations has a relief effect. With a probable central and especially psychogenic genesis of hiccups, sedative herbal preparations, tranquilizers and antipsychotic drugs are used.
Attention (this is important)!
Intractable hiccups that last more than an hour can be a sign of intoxication or severe brain pathology. In such cases, delay in hospitalization significantly worsens the prognosis of the underlying disease, leading to the need for more complex drug regimens and emergency invasive interventions. An urgent call to an ambulance is necessary for hiccups combined with vomiting, disturbances in sensitivity, motor activity and consciousness. Repeated bouts of hiccups are also a reason for a thorough examination.
Diet
There is no special diet for central hiccups, since it is impossible to influence this process with therapeutic nutrition. For food-related hiccups, it is important to monitor the amount of food you eat and the speed at which you eat it, as both of these factors can trigger hiccups. For diseases of the gastrointestinal tract, therapeutic nutrition should be used in accordance with the underlying disease. The general principles are fractional meals, exclusion of fatty, spicy, fried foods, foods that cause bloating (legumes, baked goods, kvass, an abundance of simple carbohydrates).
List of sources
- Ivashkin V.T., Trukhmanov A.S. Evolution of ideas about the role of disorders of the motor function of the esophagus in the pathogenesis of gastroesophageal reflux disease. Russian Journal of Gastroenterology, Hepatology, Coloproctology 2010; 20(2):13-9
- Cherkasov M.A., Mokhanna M.I., Ibragimov Z.A., Rabadanov R.Sh., Kovalenko A.N., Aliev A.G. Persistent hiccups after epidural anesthesia for revision hip replacement // International Journal of Applied and Fundamental Research. – 2021. – No. 9. – P. 86-90.
- Shtulman D.R., Levin O.S. Neurology: A Practitioner's Handbook. 6th ed. 2008, 1024 p.