When does Mifepristone begin to act and what does a woman feel at this time?
The time it takes for the first medication abortion pill to take effect may vary. Sometimes its effect begins to appear after 3-4 hours, and sometimes after 12 hours. The temporal variation in the effect is due to metabolic characteristics, which are individual for each woman.
- As a rule, no negative changes in well-being are felt on the first day of a medical abortion after. Sometimes you may experience a nagging pain in the lower abdomen and mild nausea.
- Patients who have experienced toxicosis begin to feel its weakening. Nausea, vomiting, pain in the mammary glands disappear, and the general condition improves. This is due to the cessation of the development of pregnancy, which had a negative effect on the body.
Often, when carrying out a medical abortion, bloody discharge is observed after taking the first pill, which, as a rule, is not accompanied by any subjective complaints. This is understandable, since the medicine only causes the termination of pregnancy and the death of the embryo, which remains in the uterine cavity. The uterus does not contract.
Therefore, very often after using the first tablets there is nothing. In this case, there is no need to worry - after taking Misoprostol, discharge will appear and the fertilized egg will come out.
A few words about natural stimulation of labor
It is possible that you can speed up the approach of labor without the help of medications. This work is only possible when:
- pregnancy is full term;
- the doctor approved the method.
Here are some tips on how to speed up the birth of your baby if the due date has already approached:
- when the cervix is ripe, but labor is not noticeable, try massaging the nipples; sometimes it helps, and the process starts in the next three days;
- walking up and down the stairs often provokes the onset of labor; Walking is also suitable - the main thing is to maintain a vertical body position so that the baby drops lower and causes the cervix to dilate;
Walking brings many mothers closer to the onset of labor. - sex without a condom - not just once, but many times; the uterus will become toned, and the sperm contains prostaglandins, which will soften the cervix;
- talk to the baby, explain to the baby how loved and expected he is, tell him that the whole family is preparing for his birth; this kind of meditation will calm the woman, relieve anxiety, stress - and ultimately childbirth will come;
- some practice cleaning floors while standing on all fours;
- introduce more foods with a laxative effect into your diet: prunes, cucumbers, cabbage, vegetable oil; active intestinal peristalsis will cause the uterus to “move” - the tone of the organ will increase; just don’t overdo it so as not to provoke intestinal upset.
Be careful with traditional medicine - some recommend drinking primrose oil, castor oil and other remedies; you risk causing allergies or acute diarrhea, which is especially dangerous on the eve of childbirth .
Misoprostol – why take it and what sensations it causes
2 days after taking Mifepristone, the patient is given another hormonal drug, Misoprostol, which causes uterine contractions. Its task is to separate the fertilized egg from the uterine wall and remove it. If this is not done, an incomplete abortion will occur. The dead embryo will remain inside the uterus, leading to bleeding and a purulent process.
Misoprostol is taken in a dosage of 400 mcg. Its effect begins quite quickly - the woman begins to experience spotting, which intensifies to the intensity of menstrual bleeding. Sometimes the volume of blood can be greater than during menstruation - it all depends on the individual characteristics of each woman and the duration of pregnancy.
If bleeding has not started 4 hours after taking the first two tablets, the woman is given another 400 mcg of the drug for medical abortion. In this case, the total dose is 400 mcg
Against the background of bleeding, the fertilized egg is released, looking like a round red formation. After this, all unpleasant sensations subside. This condition resembles a miscarriage, so a medical abortion, even the first one, does not cause as serious consequences as a surgical termination.
The release of the fertilized egg may be accompanied by cramping pain in the lower abdomen, radiating to the sacrum, coccyx, groin area, and lower back. Severe pain is usually observed during a medical abortion during the first pregnancy in a nulliparous woman.
Causes of pain during medical abortion:
- Late interruption period, approaching the limit of 7 weeks.
- Individual characteristics of a woman’s reproductive system – congenital anomalies (bicornuate, saddle-shaped uterus, presence of intrauterine septa), displacement of the uterus.
- Inflammatory processes of the genital area.
- Recent uterine manipulation (surgery, curettage).
- Low pain threshold
In this case, you can take painkillers prescribed by your gynecologist.
The tactics of labor management during full-term pregnancy and premature rupture of amniotic fluid (PROM) are still controversial. The most common opinion is that it is necessary to induce labor several hours after the rupture of amniotic fluid in order to prevent a long anhydrous interval [6, 14]. However, this approach is not always optimal, especially in the absence of biological readiness of the pregnant woman’s body for childbirth, as it often leads to labor anomalies, fetal hypoxia and, as a consequence, to an increase in the frequency of surgical delivery and obstetric injuries [7, 10]. In this regard, active expectant tactics for managing pregnancy and childbirth at full term against the background of PIOV, which allows labor to develop without the use of uterotonic drugs or to achieve optimal biological readiness for childbirth before induction of labor, is very relevant [1, 3, 10]. However, despite the presence of effective antibacterial drugs used to prevent purulent-septic complications in PIOV, an anhydrous period of more than 3 days, according to a number of authors, is not optimal [3, 10]. Based on this, there is a need to improve active expectant management of pregnancy and childbirth during PIOV using modern methods of preparing the soft birth canal for childbirth.
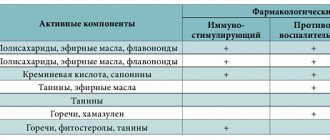
A number of authors suggest using prostaglandins of the E2 group in the form of intravaginal suppositories for PIOV. However, this method did not give positive results for the pathology under discussion. The use of kelp for PIOV is not recommended by many researchers, as the development of an ascending infection is accelerated. In recent years, antigestagen drugs have been actively studied and put into practice [2, 11]. In 1980, the first antigestagen, mifepristone (Ru 486), was developed and licensed in the laboratory of the Russel Uclaf company. Mifepristone has a high affinity for progesterone receptors, which determines the receptor mechanism of its action. Mifepristone binds to progesterone receptors, which leads to their conformational rearrangement, and further transcriptional effects become impossible. Thus, mifepristone blocks the effects of progesterone through competitive inhibition of its receptors [5]. When 100-800 mg of mifepristone is taken orally, the drug is rapidly absorbed from the gastrointestinal tract, and after 0.7-1.5 hours its concentration in the blood plasma averages 2.5 mg/l. In blood plasma, 98% of mifepristone is in a protein-bound state. After 12-72 hours, the concentration of mifepristone is reduced by half [9]. When mifepristone is prescribed to prepare for childbirth, pronounced signs of collagenolysis occur in the cervix. According to P. Stenlund et al. [12], after using mifepristone at a dose of 200 mg once a day, spontaneous labor began within the first 48 hours after taking the drug in 79.2% of patients (compared to 16.7% of pregnant women in the control group receiving placebo). It was noted that during vaginal delivery, women in labor who received mifepristone required lower doses of oxytocin than in the control group [8]. The use of antigestagens does not have a negative effect on the development of lactation and menstrual functions of women after childbirth and the condition of newborns [4, 8, 14].
Studies by D. Wing [13] show that the time interval from the start of treatment to the onset of labor averages 36.8±11.6 hours when using mifepristone and 44.5±14.7 hours after taking placebo. Vaginal delivery occurred in 87.5% of women receiving mifepristone and in 70.8% of women receiving placebo [13]. Currently, mifepristone is used to prepare the cervix for labor and induce labor at a dose of 200 or 400 mg [2, 4, 12, 13]. In the absence of biological readiness of the body for childbirth, pregnant women with PIOV have a need for more intensive preparation of the soft birth canal for it. However, the administration of 400 mg of mifepristone once in preparation for childbirth leads to a slight decrease in the average assessment of the newborn’s condition on the Apgar scale at 1 minute, but the difference with the control group is not significant. No differences were noted at the 5th and 10th minutes [12]. The use of this drug in a dosage of 200 mg once in pregnant women with PIOV, according to D. Wing and C. Guberman [14], did not give positive results compared to labor induction with oxytocin. Thus, there is a need to develop and implement new regimens for the use of antigestagens for PIOV.
The purpose of the study was to evaluate the effectiveness of using a drug from the antigestagen group - mifepristone - during full-term pregnancy and PIOV in the absence of the body’s biological readiness for childbirth.
Material and research methods
The main group consisted of 63 pregnant women with a gestational age of 37-40 weeks, in whom PIOV occurred against the background of an “immature” or “ripening” cervix. In these patients, active expectant management with mifepristone was used. The control group included 67 patients of the same period with PIOV in the absence of biological readiness for childbirth. In this group, standard tactics were used - labor induction 2-3 hours after the rupture of amniotic fluid.
Active expectant management included a comprehensive examination: clinical blood test 2 times a day, general urine test 1 time a day, bacterial culture from the cervical canal every 12 hours, thermometry every 3 hours, cardiotocography, ultrasound, Doppler. The pregnant woman was transferred to a separate ward. Vaginal examination was carried out once a day. Preparation for childbirth was carried out with antispasmodics and antioxidants.
Mifepristone was prescribed after PIOV, 0.2 g 2 times. The first time is immediately after the rupture of amniotic fluid. The second time - after 6 hours in the absence of regular labor (patent application for invention No. 2009121368/14 dated 06/04/2009).
If irregular uterine contractions occurred, therapy was supplemented with β-mimetics and calcium antagonists, and medicated sleep and rest were provided at night. If the water-free interval was more than 12 hours, antibacterial therapy was prescribed: amoxiclav 1.2 g intravenous bolus, 2 times a day. When optimal biological readiness of the body for childbirth was achieved, labor induction was carried out. In the absence of labor and a water-free interval of 72 hours, labor induction was planned.
Clinical characteristics of the study groups were as follows. The main group included 47 (74.6±5.5%) primiparous and 16 (25.4±5.5%) multiparous. In the control group there were 49 (73.13±5.4%) primiparous and 18 (26.87±5.4%) multiparous. In the main group, the average age of primiparous women was 27.2±6.4 years, multiparous women - 33.5±6.2 years. The average age of primiparous women in the control group was 26±5.4 years, multiparous women—35.4±6.8 years.
There were 3 older primigravidas in the main group (4.7±2.7%), and 2 (2.9±2.1%) in the control group. In the main group, infertility was detected in 9 (14.29±4.4%) patients, in the control group - in 11 (16.42±4.5%). During pregnancy, 17 (26.9±5.6%) patients in the main group and 21 (31.34±5.7%) in the control group were diagnosed with various types of genital tract infections that required antibacterial therapy. In the main group, PIOV occurred against the background of a “ripening” cervix in 44 (69.84±5.8%) patients, in 19 (30.16±5.8%) - against the background of an “immature” cervix. In the control group, PIOV occurred on the cervix in 49 (73.1±5.4%) pregnant women, in 18 (26.9±5.4%) - against the background of “immature”.
Research results and discussion
According to the analysis of the dynamics of the birth act, in the main group the anhydrous interval in primiparous women averaged 14 hours 20 minutes, in multiparous women - 11 hours 50 minutes. In the control group, the anhydrous period averaged 12 hours 35 minutes for primiparous women and 11 hours 55 minutes for multiparous women. Thus, as shown in Fig. 1,
Figure 1. Duration of the anhydrous interval with different labor management tactics. The duration of the anhydrous interval is slightly longer in primiparas of the main group, and almost the same in multiparous ones.
The latent period (the time interval between the discharge of amniotic fluid and the onset of labor) in the main group averaged 8 hours 25 minutes and 5 hours 15 minutes in the control group. The average duration of labor in primiparas of the main group was 7 hours 50 minutes, in multiparous women - 6 hours 35 minutes. The average duration of labor in primiparas in the control group was 8 hours 50 minutes, in multiparous women - 7 hours 15 minutes (Fig. 2).
Figure 2. Duration of labor with different management tactics. Thus, with active expectant management, the duration of labor increases, but not statistically significant.
Anomalies of labor in the main group were noted in 6 (9.5±3.7%) women in labor. Of these, 5 (7.9±3.4%) had weak labor and 1 (1.6±1.6%) had rapid labor. Anomalies of labor were detected in 21 (31.34±5.7%) parturients in the control group. Of these, 12 (17.9±4.7%) had weak labor, 4 (5.9±2.9%) had discoordinated labor, and 5 (7.5±3.2%) had rapid labor. childbirth. Thus, the use of mifepristone with active expectant management tactics statistically significantly reduces the incidence of labor anomalies (Table 1).
In the main group, 4 (6.3±3.1%) patients delivered through the abdominal route. The reason for one operation was fetal hypoxia. Intraoperatively, a double entanglement of the umbilical cord around the fetal neck was detected. The indication for the remaining three operations was weakness of labor, which was not amenable to drug correction. In the control group, 15 (22.4±5.1%) women gave birth using cesarean section. Indications for operative delivery were the lack of effect from induction of labor in 8 (11.9±3.9%) cases, weakness of labor combined with fetal hypoxia in 3 (4.5±2.55) cases, weakness of labor not responding to drug correction, in 2 (2.9±2.1%) women in labor, fetal hypoxia in 2 (2.9±2.1%) cases. Two births (2.9±2.1%) in the control group were completed by applying exit forceps due to fetal hypoxia.
A total of 8 (12.7±4.2%) cases of fetal hypoxia were identified in the main group. There were no cases of children being born in a state of asphyxia. The diagnosis of fetal hypoxia in the control group was recorded in 21 (31.3±5.7%) births. In 7 (10.45±3.7%) cases, children were born in a state of asphyxia, with one (1.49±1.48%) of them in a state of severe asphyxia (2 points on the Apgar scale).
Labor induction in the main group was performed in 13 (20.6±5.1%) cases. The cause of labor induction was the presence of a “mature” cervix. In the remaining cases (46 women, 73.0%), labor developed spontaneously. In the control group, labor began spontaneously within 3 hours after PIOV in only 3 (4.5±2.5%) women. In 65 (97.1±2.1%) examined patients, labor was induced. Thus, the use of mifepristone during active expectant management significantly reduced (p<0.01) the need for induction of labor.
Perineotomy was performed in the main group in 14 (22.2±5.1%) cases, in the control group - in 27 (40.3±5.2%). This difference is statistically significant and, according to our observations, is associated with a high incidence of labor weakness and fetal hypoxia in the control group.
Drug pain relief during labor was performed in 21 (33.3±5.9%) women in labor in the main group, and in 23 (36.5±6.1%) in the control group. Long-term epidural anesthesia (LPA) in the main group was performed in 9 (13.4±4.1%) women, in the control group - in 14 (22±5.2%).
In the postpartum period, 4 (6.3±3.1%) cases of uterine subinvolution were noted in the main group. In 2 (3.2±2.2%) cases, infiltrate was detected in the area of the perineal sutures, in 1 (1.6±1.6%) - endometritis (Table 2).
Postpartum women received conservative therapy with a positive outcome. Thus, 7 (10.45±3.7%) women had complications in the postpartum period in the main group.
In the postpartum period, 7 (10.45±3.7%) cases of uterine subinvolution were noted in the control group. In 2 (2.9±2.1%) postpartum women, infiltrates were detected in the area of the perineal sutures. In total, the number of complications in the postpartum period in the control group was 9 (13.4±4.2%). It is obvious that active expectant management of pregnancy and childbirth during PIOV does not affect the course of the postpartum period.
conclusions
1. The use of mifepristone during active expectant management of urgent labor after PIOV in the absence of the body’s biological readiness for childbirth can reduce the incidence of labor anomalies, operative delivery, fetal hypoxia and asphyxia of the newborn.
2. The use of antigestagens during PIOV promotes the spontaneous development of labor and helps reduce the frequency of labor induction.
3. When choosing active expectant tactics for PIOV with the use of mifepristone, there is no significant increase in the anhydrous interval, as well as the incidence of purulent-septic complications during childbirth and the postpartum period.
4. These data give reason to believe that the use of antigestagens in PIOV will be further developed.
Can an abortion fail?
This situation occurs extremely rarely - only in 1.6% of cases. Moreover, the earlier the interruption was carried out, the higher the likelihood that it will be successful.
It is almost impossible to determine by external signs whether a medical abortion has occurred, therefore, after the termination is completed, an ultrasound diagnosis is required to make sure that the fertilized egg has been completely released.
Unfortunately, it is impossible to create a pregnancy that is not terminated after taking the pills. Mifepristone and Misoprostol have a negative effect on the fetus and can lead to the development of severe congenital anomalies. Therefore, the pregnancy will have to be terminated in any case.
Can taking abortion pills cause any complications?
Since the drugs used during pharmacological abortion are hormonal, they can cause a disruption in the production of hormones. In this case, periods after a medical abortion may come very late. The first menstruation may be scanty or too short. As a rule, after a few months the menstrual cycle returns to normal.
MAKE AN APPOINTMENT
[contact-form-7 id=”296″ title=”Untitled”]
Abortion and contraception clinic in St. Petersburg - department of the medical gynecological association "Diana"
Make an appointment, tests or ultrasound via the contact form or by calling +8 (812) 62-962-77. We work seven days a week from 09:00 to 21:00.
We are located in the Krasnogvardeisky district, next to the Novocherkasskaya, Ploshchad Alexander Nevsky and Ladozhskaya metro stations.
The cost of a medical abortion in our clinic is 3,300 rubles. The price includes all pills, an examination by a gynecologist and an ultrasound to determine the timing of pregnancy.