- Causes of hypothermia
- Temperature control processes
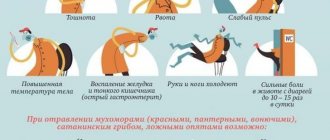
- Symptoms and stages of hypothermia
- Diagnosis of hypothermia
- First aid
Temperature is an important indicator of health status. Critical hypothermia of the body with a temperature drop below 35°C is called hypothermia. Typical symptoms include tremors, confusion, changes in breathing and heart rate, and blue lips, fingers, and toes.
Symptoms of hypothermia
The main cause of hypothermia is heat loss in the cold through the skin and breathing.
A protective program is activated - a thermoregulation mechanism. The body saves important organs by sacrificing the skin, fingers and toes, nose - without this a person can survive. Hypothermia is divided into three stages:
Lightweight
The temperature drops to the first critical level of 35-34 °C. Trembling appears - the release of heat through muscle activity. The blood vessels narrow and the skin turns pale. It is easy to get frostbite at this stage. Metabolism slows down, so a person feels lethargic, apathetic, and critical thinking suffers. Symptoms of mild hypothermia include memory problems; the person does not remember where or where they are going. If hypothermia begins in nature, at this moment it is easy to lose your bearings. Hunger and fatigue worsen symptoms.
Moderate
Body temperature drops to 30 °C. Weak pulse—the heart slows down to conserve heat and protect the brain. The skin becomes cold, bloodless - a characteristic marble shade. Limbs bend with difficulty. Metabolism and chemical reactions in the nervous system are disrupted. Consciousness disorders progress - severe drowsiness, speech disturbances, and sometimes hallucinations begin.
Heavy
Low temperature, up to 27 °C and below. The person loses consciousness, limbs become numb, severe frostbite. The pulse practically disappears - you can feel it on the carotid artery. Breathing problems begin - rare and intermittent. At this stage, the pupils do not react to light, and the heart may stop.
The first satellite of hypothermia is frostbite of the extremities. A spasm of capillaries occurs, and the tissues do not receive enough oxygen and nutrition. The process occurs at different stages of supercooling. The negative consequences are enhanced by:
- hunger and overwork;
- immobile or uncomfortable position;
- tight shoes;
- wet clothes;
- weakened immune system;
- vascular disease;
- mechanical damage;
- blood loss;
- alcohol intoxication.
Temperature control processes
The ability to maintain a constant body temperature of about 37°C is called thermoregulation. The control center is located in the hypothalamus. The so-called target temperature value is also set here. Each part of the body is equipped with a temperature “sensor” (receptor) that signals temperature fluctuations.
From the point of view of creating comfortable temperature conditions, vital organs occupy a dominant place, and the skin and limbs - according to the residual principle. In conditions of moderate hypothermia, to reduce heat loss over a large area, heat is spent primarily on internal organs. Skin temperature indicators may differ from internal ones; fluctuations range up to 9 °C.
The temperature range perceived by the body as pleasant does not require large expenditures for thermoregulation and can be maintained at a constant level only due to blood circulation in the skin. This state is called the temperature of indifference. It is 28-30 °C, provided that the calculated values are taken for a person without clothes at rest and with average air humidity. For a clothed person, this parameter drops to 22 °C.
Body temperature is an individual parameter. In children, it is always slightly increased due to activity and intense metabolism. In older people, the temperature may be lower than normal - 34-35 degrees Celsius, which is due to the speed of chemical reactions.
There are peripheral and central temperatures. Peripheral (superficial) – skin temperature. Measured on the forehead and armpits. Central - records the temperature of internal organs and large vessels, kept at 36.1-38.2 degrees Celsius. Areas for measurement: rectum, mouth, esophagus, nasopharynx, bladder.
First aid for hypothermia
If the victim shows signs of hypothermia, the goal of first aid is to stop heat loss. During all stages of hypothermia or frostbite, hot baths or showers are prohibited. The patient should not be brought into a hot room, rubbed with snow or given alcohol.
Rescue blanket
A rescue blanket is used to protect the victim from overheating or overheating..
82.00 UAH.
Blizzard rescue blanket
The Blizzard rescue thermal blanket is the No. 1 first aid product for hypothermia.
Rescue blanket.. 2,065.00 UAH.
Rewarming and complications
With sharp peripheral vasodilation, arrhythmia and cardiac arrest may develop in several ways: 1. “Acidic” blood from the peripheral vascular bed due to active metabolic processes reaches the “core” of the body, which leads to the development of acidosis. As a result of acidosis, the content of catecholamines in the blood increases, which potentiates increased cardiac activity, increased heart rate, and increased blood pressure. Increased acidosis reduces the sensitivity of receptors to adrenergic substances, and arrhythmia may occur. 2. Due to myocardial damage, hypovolemia, after peripheral vasodilation, blood pressure decreases, which leads to the development of shock. 3. Cold blood from the peripheral parts of the bloodstream reaches the “core,” which leads to increased hypothermia, i.e., a further decrease in the temperature of the “core.”
First aid for hypothermia
Conditions are created so that the body can warm up - they pull the victim out of the water or snow, leave the cold room or open area.
- Warm the patient.
- Remove wet clothes, paying special attention to shoes.
- Cover with a warm blanket, put on a heating pad, warm with your body or organize another heat source.
- If possible, organize a warm bath or shower. Raise the water temperature gradually, at first barely warm. So that a sharp increase in blood circulation does not destroy the blood vessels. The water is gradually brought to 40 °C. You need to take a bath until your body temperature rises to the stage of mild hypothermia - 34 ° C
- In case of severe hypothermia, first aid is not enough. You need to call a doctor or take the victim to the hospital.
1.What is hypothermia and its causes
Hypothermia, or hypothermia
, occurs when the body becomes cold and loses heat faster than it can produce it.
Normal human body temperature is 36.6 °C. This is if you measure it in the usual way - under the armpit. The method of measuring rectal body temperature is considered more accurate. Normally, rectal temperature ranges from 36.4°C to 37.6°C. For most people, the average is 37 °C.
Sometimes a healthy adult's normal body temperature is slightly lower - 36°C. If the person is not sick and feels well, then, as a rule, there is no need to see a doctor in this case. There's nothing wrong.
Causes of hypothermia
Hypothermia occurs when you are exposed to cold air, water, wind or rain. Typically, hypothermia is caused by prolonged and forced exposure to cold water or outdoors in winter.
When the air temperature is 10 °C or slightly higher in damp and windy weather, hypothermia may already occur. Staying in water that has a temperature of -16-21°C can also cause hypothermia. For mild hypothermia, treating hypothermia at home may be enough to return your body temperature to normal.
A must read! Help with treatment and hospitalization!
First aid for frostbite
- It is necessary to remove the patient from the cold, gradually warm the frostbitten area, and rub it with your hand until it turns red. This is done carefully, increasing the pressure gradually so as not to damage the vessels. Afterwards, give the patient a warm, not hot drink.
- When sensitivity returns to the limbs, the victim feels pain in the affected area, it is necessary to prepare an anesthetic in advance.
- Next, the limb is wrapped in a warm cloth and secured in a sling to reduce swelling. If severe frostbite occurs, the patient is taken to the hospital. Before this, the patient is carefully insulated.
- Do not place frostbitten hands on a radiator or other hot surfaces, rub them with snow, or grease them with grease.
Diagnostics
Although the pathophysiological and clinical manifestations of hypothermia occur one by one, they are usually divided into three stages: mild, moderate and important (see Table 2). As has already been noted, the clinical course of mild hypothermia may appear gradually, especially in older patients. Once a diagnosis has been made, the patient’s condition may be underestimated, since standard medical thermometers cannot measure temperatures below 34.4°C. Therefore, it is important to use special rectal thermometers, adapted for recording low temperatures, or rectal thermistor sensors. During the course of research, tympanic thermometry and sechomichur sensors were also often used, their accuracy has not yet been established. If the exact method of measuring the internal body temperature is not counterproductive, it is important to immediately stop all obvious methods, as long as the patient is warmed up, a temperature difference between different sections of the body appears. la.
Table 2. Stages and clinical manifestations of hypothermia
| Stage of hypothermia | Body temperature | Clinical manifestations |
| Easy | 32.2°–35°C | Pochatkova phase of awakening for sublanny cooling:
About an hour later, after the second appeared:
|
| Average importance | 28–32.2°C | Arrhythmia anterior Bradycardia Reduced level of CV Bradypia Widened zone Reduced vomit reflex Extinction of groves Hyporeflexia Hypotension Appearance of J-wave on ECG (div. Figure 1) |
| Vazhka | <28°C | Apnea Coma Decreased or absent activity on electroencephalography Sites do not respond to light Oliguria Swelling of the leg Scholastic arrhythmias/asystole |
Prevention of hypothermia
Protective measures are divided into two stages:
Passive cold protection
- Passive protection is properly fitted clothing that contains three separate layers:
- Basic - removes moisture from the skin. The best option is thermal underwear.
- Thermal insulation - retains heat.
- Protective – prevents moisture from penetrating inside. In modern jackets it is a waterproof membrane.
- Clothing must be clean; dirt prevents moisture from evaporating.
Active heat replenishment.
Food will help replenish heat reserves in the body; it is better to choose high-calorie portions and have a hearty lunch before going out. A thermos with warm drink will keep you from freezing. You don't feel thirsty in the cold, so it's easier to become dehydrated than in the heat, and a lack of water in the body increases the symptoms of hypothermia.
An external heat source is the easiest way to stay warm. When walking around the city, you need to pause and go indoors. A suitable option is thermochemical and electric heating pads.
Laboratory changes
Possible development of nitric deficiency as a result of rhabdomyolysis or acute tubular necrosis. During resuscitation visits, the level of electrolytes may change rapidly, so they should be regularly monitored. Zokrem, rhubarb often contains potassium as a result of changes in the acid-water balance, which occurs as the body warms up. In patients with hypothermia, coagulopathy is due to impaired activity of temperature-dependent enzymes in the coagulation cascade, although the results of coagulation tests are often normal, and a blood sample is taken before testing. heats up to 37°C.
As a matter of fact, coagulopathy is limited and does not require intervention. The results of these studies recommend the use of uncorrected values instead of blood gases to make clinical decisions. Although the rate of leukocytosis unreliably reflects the evidence of infection, patients with advanced rhiziquity - newborns, elderly people or those with evidence of immunodeficiency - a trace empirically Prescribe antibiotics while microbiological tests are running.
Likuvannya
Once the level of glucose in the blood is determined, glycogen reserves have been depleted in most patients, and hypothermia can mask the clinical manifestations of hypoglycemia. All patients should be given thiamine as a precaution, as fragments of this vitamin may cause only minimal side effects, and it is impossible to obtain a history of alcohol abuse. Wet clothes must be taken off and the sick person covered with carpets for thermal insulation. Avoid excessive looseness and insertion of a nasogastric tube, which may result in fibrillation of the sac. Aggressive rehydration with heated ingredients will help combat dehydration caused by extreme diuresis in the cold.
Glucocorticoids should not be empirically prescribed to all patients, but only to those with a complex medical history due to the obvious deficiency of epithelial cells and to those whose body temperature does not normalize, without regard to stagnation of the thyroid gland. playful visits.
It is extremely important to tighten the cardiovascular system in patients with hypothermia. In the absence of Doppler ultrasonography, it is important to assess the pulse rate; the American Heart Association (AHA) recommends palpating the pulse for at least 30–45 minutes before cardiac and pulmonary resuscitation. seconds In patients with hypothermia, the ECG can show silent changes - from tachycardia to bradycardia, from atrial fibrillation with an increased sac rhythm to sac fibrillation and asystole. There is also an increase in the PR, QRS and QT intervals, J-waves (Fig. 1), changes that are associated with acute coronary insufficiency.
Rice. 1.
EKG with J-tails.
If most arrhythmias resolve spontaneously as the patient warms up, fibrillation of the sac will require defibrillation. If the initial rounds were unsuccessful, defibrillation tests and internal stagnation of medications began until the patient’s temperature exceeded 30°C, then continue to chew the rounds to maintain vitality. Reality. If the patient is already fertile, and suffular fibrillation will continue, then the remaining recommendations are to stop amiodarone.
Patient care
In patients with hypothermia, it is necessary to consider several clinical parameters at the same stage of hypothermia (see Fig. 2). Passive play
can be considered as a single method of treatment for patients with mild hypothermia and is aimed at creating a new warm, dry environment and adequate thermal insulation. Passive heating may be successful in those with intact thermoregulatory mechanisms, normal endocrine function, and adequate energy reserves for endogenous heat production. A small part of this method is that the internal body temperature increases significantly.
Rice. 2.
Algorithm for the treatment of patients with hypothermia.
Active external ignition
It is ensured simply by the flow of thermal action on the skin and effective body while maintaining circulation, with the help of which the peripheral blood can be heated to circulate to the internal organs. Hot water splashes and heaters applied before the passage of main vessels can cause the cold skin to swell from the sounding vessels. Systems that rely on hot air blowing effectively ensure the beginning of heat transfer through additional convection. An exciting new technology is based on frozen axillary arteriovenous anastomoses, when the heat of the venous blood from the axillary sections turns to the internal organs. These anastomoses are opened when the hands or feet are soaked in warm (45°C) water or the forearm is placed in a special device with warm air, which locally creates a vacuum to –40 mm Hg. Art. There is still a lack of clinically significant methods.
The main effect of active external heating lies in the resulting decrease in internal body temperature when the cold peripheral blood reaches the heart. In the past, this has led to many unjustified fatal episodes, some doctors came to the rescue when the patient’s condition deteriorated, and began resuscitation. This complexity can be minimized, stagnation and minimal invasive methods for fermentation of the internal core of the body before the beginning of active external fermentation.
In addition, “digestive acidosis” may occur if lactic acid accumulates on the periphery and returns to the central bloodstream. Peripheral vasodilation, due to active external pollution, can cause stagnation of blood in the venous bed and “hot shock”. Due to this deformation, the patient’s position in front of the cuticle may become painful for a short time.
Methods of active stimulation of the internal core of the body
They are susceptible to invasiveness and potential complications. There are no results from consistent research, so the choice of method depends on the capabilities of the doctor. It is easy to ferment steamed meats with fermenting acid at 40°C, because the heat loss through evaporation changes during cooking, and the internal body temperature increases by 1.0–2.5°C. Internal preparations (usually 5% glucose and fertilizing agents) are then heated to 40–45°C. These two methods have a minimal range of side effects, which is likely to occur in all patients, although they require only passive heating.
The most effective method of active internal fermentation is extracorporeal blood fermentation using an additional unit of blood circulation, arteriovenous and venovenous fermentation, or hemodialysis. With the help of these methods, the internal body temperature of the skin is 3–5 min. increases by 1–2°C. A retrospective study by Walpoth et al. (1997) found that among 32 patients with severe hypothermia who were treated with an additional blood circulation machine, the rate of dispensary care during the same period was 47%. Unfortunately, not all medical institutions have access to this method of treatment.
Active warming of the body's internal core can be completed by washing a small amount of empty body with warm water. Irrigation of the colon, large intestine and sechoic mixture will provide a greater temperature rise (1.0–1.5°C), leaving the area for heat exchange enclosed. Peritoneal dialysis with fisrosine, Ringer's solution or dialysate, heated to 40–45°C, with a fluidity of 6–10 l/year. Combined with the supply of heated acid, the temperature will increase by 1–3°C. Please note that all of these methods work completely and can become stagnant in case of moderate or even high stage hypothermia, if extracorporeal blood fermentation is not possible.
Active heating of the internal midsection of the body through a closed thoracic irrigation system occurs in installed large-diameter thoracostomy drainages along the mid-axillary and mid-clavicular lines for Safely serving and viticanning heated fizz. Direct thoracic irrigation is used for direct irrigation of the mediastinum after thoracotomy, ensuring an increase in core body temperature by 8°C. A retrospective study by Brunette et al. (2000) it was found that among 22 patients who underwent thoracotomy with special assistance, the survival rate was 71%. Following a left-sided thoracotomy, fragments of irrigation of the cooled myocardium with warm water can cause fibrillation of the sac.
Forecast
The lowest temperature recorded in patients with hypothermia who lived was 14.2°C in children and 13.7°C in adults. These facts are confirmed by the statement: “The patient cannot be considered dead until he is identified and reconciled with him.” Resuscitation approaches are not allowed to continue, meaning that the patient appears dead, until after reaching a body temperature of more than 30–32°C there is no sign of vitality. The death of a patient can be established at the scene of its discovery, if it is possible to exclude obvious lethal traumatic injuries, it is clear that during life, resuscitation is possible, or if evacuation may become and a threat to the warriors. Patients with mild hypothermia can be returned home after warming up, while in important cases they can be hospitalized for dynamic monitoring and continued restraint after stabilization. I will.
Material and methods
In a multicenter retrospective study conducted by the all-Russian public organization “Federation of Anesthesiologists and Resuscitators” (FAR), data was collected from the analysis of resuscitation cards of patients admitted to the ICU in 2021. The study involved 6 ICUs of various hospitals in the Russian Federation (Arkhangelsk, Krasnodar, Moscow , Novodvinsk, Chita, Yakutsk). The study included both surgical and medical patients.
The criterion for inclusion in the study was the presence of hypothermia (a decrease in body temperature below 35 °C) upon admission to the ICU. Respondents completed individual patient registration forms and sent them to the study coordinator for processing. The cards included the following information about patients: gender, age, diagnosis, surgical intervention performed before admission to the ICU, length of stay in the ICU, mortality, methods of temperature measurement, use of special treatment methods (ventilator, inotropic, vasopressor support, warming), and also hemodynamic parameters and laboratory examination data: temperature, blood pressure (BP), heart rate (HR), pH, levels of lactate, hemoglobin, leukocytes, platelets, international normalized ratio (INR) on admission, 6 and 24 hours after admission to the ICU.
Statistical analysis.
For statistical analysis, the application package Microsoft Excel for Office 365 (Microsoft corporation, USA), MedCalc 12.3.0 (MedCalc Software, Belgium) was used.
When analyzing the results, the normality of data distribution was assessed using the Shapiro-Wilk test. Data are presented as arithmetic mean and standard deviation or median Me (25th–75th percentiles) depending on the distribution. Statistical processing of data was carried out using parametric and non-parametric tests: t
-test and the Mann-Whitney test.
χ
test was used to analyze qualitative features. Repeated measures data based on distribution were assessed using ANOVA for repeated measures, followed by a test of contrasts or using the Friedman test.
To identify data correlations, Spearman correlation analysis was used to calculate the correlation coefficient rho
.
For all tests, a p
<0.05 was considered statistically significant.
Preventive visits
Hypothermia is a serious condition that can potentially be treated with additional lightening and other preparations. The Centers for Disease Control and Prevention (CDC, USA) recommend keeping special winter survival kits in the premises, including carpets, first aid kits, water and food to avoid messing around. Other aspects - sealing stitches on windows, thermal insulation of doors - are important for older people. If a person has had an accident on a transport vehicle, to save heat, you should move all the traffic from the trunk to the passenger compartment.
If a person is out in the fresh air, he wears a large ball of clothing, and the largest inner ball is made of linen, seam or polypropylene fabric, splinters and materials collected It’s better to warm up, nizh bavovna. A spherical jacket can absorb plenty of wind, thereby minimizing the loss of heat through convection. Wearing a hat or thick scarf on your head prevents heat loss through ventilation. As soon as mild stage hypothermia begins to manifest, it is necessary to turn to the premises to prevent the progression of hypothermia.
Prepared by Bogdan Boris