What is Reosorbilact solution?
The infusion contains the following components:
- Sodium lactate, entering the vascular bed, is decomposed into sodium ions, carbon dioxide and water and subsequently forms sodium bicarbonate (soda). It changes the pH to the alkaline side and eliminates the effects of acidosis. The pH changes gradually, and not abruptly, as when using a conventional bicarbonate solution, which is much easier to tolerate by patients.
- Sorbitol is metabolized in the liver into fructose. Next, it is transformed into glucose (used by the body as an urgent energy substrate) and glycogen (deposited in the liver). The active component of the infusion, sorbitol, has an antiplatelet effect. The isotonic solution improves blood supply to organs and tissues at microcirculation levels.
- CaCl2, NaCl, MgCl2 - eliminate the lack of the same ions Ca2+ Cl-, Na+, Mg2+. They are needed for neuromuscular transmission of impulses, contraction of the myocardium, striated skeletal and smooth muscles.
- Potassium chloride is important for heart function. K+ exhibits inotropic (increases the force of myocardial contraction) and bathmotropic (increases the excitability of the heart muscle) effects in the body.
The osmolarity of the solution is 900 mOsm/liter.
The drug has a diuretic effect and increases diuresis, which must be taken into account when prescribing to patients with dehydration. Such patients need to use the medicine in combination with other plasma substitutes.
PHARMACOLOGICAL PROPERTIES:
Plasma replacement solution. Rheosorbilact has a rheological, anti-shock, detoxification effect, and eliminates acidosis. The main pharmacologically active substances of the drug are sorbitol and sodium lactate. When introduced into the vascular bed, sodium, CO2 and H2O are released from sodium lactate, forming sodium bicarbonate, which leads to an increase in the alkaline reserve of the blood. In contrast to the solution of bicarbonate, the correction of metabolic acidosis when using sodium lactate occurs gradually as it is included in the metabolism; in this case, there are no sharp fluctuations in pH. Only 50% of the administered sodium lactate (L-isomer) exhibits pharmacological activity; the second half of the drug (D-isomer) is not metabolized and is excreted in the urine. The effect of sodium lactate appears 20–30 minutes after administration. Sorbitol is quickly included in metabolism, 80–90% of it is utilized in the liver and accumulates in the form of glycogen. In the liver, sorbitol is first converted into fructose, which is further transformed into glucose and then into glycogen. Part of the sorbitol is consumed for emergency energy needs, the rest is deposited in the form of glycogen. Isotonic sorbitol solution has a disaggregant effect and thus improves microcirculation and tissue perfusion.
When is it prescribed?
Reosorbilact droppers are used for the following purposes:
- detoxification;
- normalization of blood flow through arteries and veins;
- increasing capillary blood flow and hemodynamics;
- replenishment of BCC (circulating blood volume) in case of severe blood loss;
- normalization of acid-base balance during acidosis.
This need arises in the following conditions:
- burn, traumatic, hypovolemic (occurs with blood loss or severe dehydration), toxic (more often develops with infectious diseases) and hemolytic (with intravascular destruction of blood cells) shocks;
- sepsis;
- prolonged purulent lesions;
- infectious pathologies;
- chronic viral and toxic hepatitis;
- burn disease;
- thrombosis, endarteritis and thrombophlebitis - prevention and therapy;
- in surgery in the preoperative and postoperative periods;
- with obliterating vascular pathologies (Raynaud's disease).
For the purpose of toxicity, Reosorbilact is used for pneumonia and for skin with pyoderma.
conclusions
1. After infusion of Reosorbilact at a dose of 10–15 ml/kg, a significant decrease in the content of medium-weight molecules and malondialdehyde occurs, which is associated with the effect of hemodilution and increased excretion by the kidneys. 4 hours after infusion of Reo-sorbilact, a decrease in average weight molecules was noted by 14–40% from the initial value in various diseases, malondialdehyde by 36–72%.
2. Rheosorbilact has a pronounced detoxification effect and can be recommended as a basic drug to reduce intoxication in purulent-septic diseases, isolated TBI, pneumonia, in the postoperative period after reconstruction of the ICA.
3. When using Reosorbilact, the parameters of the blood coagulation system quickly normalized, which indicated an improvement in blood rheology.
4. Considering the multifunctionality of Reosorbilact, namely the presence of a hemodynamic effect, a pronounced detoxification effect, improvement of microcirculation and rheology, correcting the water-salt and acid-base balance, it is recommended to use it as a universal solution for various surgical pathologies.
How and in what doses is prescribed
The medicine is administered into peripheral veins most often by drip, but sometimes by jet, in case of life-threatening incidents.
In case of shock, it is necessary to quickly fill the vessels with fluid and stabilize vital signs. Therefore, 0.6–1 liters of solution is administered in a stream and then dropwise (the dosage is calculated based on 10–15 ml per 1 kg of weight).
In case of heavy bleeding and a sharp drop in blood volume, Reosorbilact is administered intravenously in a stream at the rate of 25 ml/kg (1.5–1.8 l).
They also place IVs and drip the solution to patients:
- For the purpose of detoxification in chronic hepatitis, 6/7 ml/kg (usually 0.4 l).
- Before and after operations, 0.4 liters 1 time per day once or 3-5 days.
- For obliteration (closing of the lumen) of blood vessels, 8–10 ml/kg body weight for 10 days.
REOSORBILACT SR 200ML
Instructions
Trade name of the drug: Rheosorbilact® (Rheosorbilactum)
Active ingredients: Comb.drug (magnii chloridum, natrii lactas, natrii chloridum, kalii chloridum, calcii chloridum, sorbitolum)*
Pharmacotherapeutic group: Saline solutions, Saline solutions.
Release form: 200 ml or 400 ml per bottle, 1 bottle per pack; 200 ml or 400 ml bottles; 250 ml or 500 ml in containers.
Dosage form: Solution for infusion 200 ml, 400 ml (glass bottles)
Compound:
1 ml of solution contains: active substance: sorbitol 60.0 mg, sodium lactate (in terms of 100% substance) 19.0 mg, sodium chloride 6.0 mg, calcium chloride dihydrate (in terms of calcium chloride) 0. 1 mg, potassium chloride 0.3 mg, magnesium chloride hexahydrate (in terms of magnesium chloride) 0.2 mg; excipient: water for injection. theoretical osmolarity – 891 mOsmol/l; pH 6.00-7.60; ionic composition: 1 liter of the drug contains Na+ – 272.20 mmol, K+ – 4.02 mmol, Ca++ – 0.90 mmol, Mg++ – 2.10 mmol, Cl- – 112.69 mmol, Lac- – 169.55 mmol.
Pharmacological properties:
Reosorbilact® has a rheological, anti-shock, detoxification, as well as alkalizing effect and stimulates intestinal motility. The main pharmacologically active substances of the drug are sorbitol and sodium lactate. In the liver, sorbitol is first converted to fructose, which is further converted to glucose and then to glycogen. Part of the sorbitol is used for immediate energy needs, the other part is stored as a reserve in the form of glycogen. An isotonic sorbitol solution has a disaggregating effect and thus improves microcirculation and tissue perfusion. Unlike bicarbonate solution, correction of metabolic acidosis with sodium lactate occurs more slowly as it is included in the metabolism, and there are no sharp pH fluctuations. The effect of sodium lactate appears 20-30 minutes after administration. Sodium chloride has a rehydrating effect. Replenishes the deficiency of sodium and chlorine ions in various pathological conditions. Calcium chloride replenishes the deficiency of calcium ions. Calcium ions are necessary for the transmission of nerve impulses, contraction of skeletal and smooth muscles, myocardial activity, bone tissue formation, and blood clotting. Reduces the permeability of cells and the vascular network, prevents the development of inflammatory reactions, and increases the body's resistance to infections. Potassium chloride restores water and electrolyte balance. It has a negative chrono- and bathmotropic effect, and in high doses – a negative ino-, dromotropic and moderate diuretic effect. Participates in the process of conducting nerve impulses. Increases the content of acetylcholine and causes excitation of the sympathetic part of the autonomic nervous system. Improves skeletal muscle contraction in muscular dystrophy, myasthenia gravis.
Pharmacokinetics:
Sorbitol is quickly included in general metabolism, 80-90% of it is utilized in the liver and accumulates in the form of glycogen, 5% is deposited in brain tissue, cardiac muscle and skeletal muscle, 6-12% is excreted in the urine. When introduced into the vascular bed, sodium, CO2 and H2O are released from sodium lactate, which form sodium bicarbonate, which leads to an increase in the alkaline reserve of the blood. Only half of the administered sodium lactate (isomer L) is considered active, and the second half (isomer D) is not metabolized and is excreted in the urine. Sodium chloride is quickly removed from the vascular bed, only temporarily increasing the volume of circulating blood. Increases diuresis.
Indications for use:
To improve capillary blood flow for the purpose of prevention and treatment of traumatic, surgical, hemolytic, toxic and burn shock, with acute blood loss, burn disease, infectious diseases that are accompanied by intoxication, with exacerbation of chronic hepatitis, sepsis, for preoperative preparation and in the postoperative period, for improving arterial and venous circulation to prevent thrombosis, thrombophlebitis, endarteritis, Raynaud's disease.
Mode of application:
Reosorbilact® is administered intravenously to adults by drip at a rate of 40-60 drops/min. If necessary, a jet injection of the drug is allowed after the test by drip injection at a speed of 30 drops/min. After administering 15 drops, use of the drug should be stopped, and after 3 minutes, if there is no reaction, Reosorbilact® should be administered in a stream. In case of traumatic, burn, postoperative and hemolytic shocks for adults, administer 600-1000 ml (10-15 ml/kg of patient’s body weight) once and repeatedly 600-1000 ml (10-15 ml/kg of patient’s body weight) first in a stream, then drip. For chronic hepatitis, adults administer 400 ml (6-7 ml/kg body weight) by drip. For acute blood loss, adults administer 1500-1800 ml (up to 25 ml/kg body weight). In this case, Reosorbilact® infusions are recommended to be carried out at the prehospital stage in a specialized ambulance. In the postoperative period and after various surgical interventions - at a dosage of 400 ml (6-7 ml/kg body weight) dropwise for 3-5 days. For thrombus-obliterating diseases of the blood vessels - at the rate of 8-10 ml/kg body weight by drip, repeated every other day, up to 10 infusions per course of treatment.
Side effects:
From the immune system: anaphylactoid reactions, angioedema, hyperthermia. From the cardiovascular system: increased or decreased blood pressure, tachycardia, shortness of breath, acrocyanosis. Neurological disorders: tremor, headache, dizziness, general weakness. Changes in the skin and subcutaneous tissue: skin rashes, urticaria, itching sensation. Gastrointestinal disorders: nausea, vomiting. General disorders: changes at the injection site, including pain and burning.
Contraindications:
Individual hypersensitivity to the components of the drug. Reosorbilact® should not be used in case of alkalosis, as well as in cases where the infusion of large volumes of fluid is contraindicated (cerebral hemorrhage, thromboembolism, cardiovascular decompensation, stage III arterial hypertension, decompensated heart defects, end-stage renal failure), dehydration, oliguria.
Drug interactions:
Do not use as a carrier solvent for other medications. Incompatibility. Reosorbilact® must not be mixed with phosphate- and carbonate-containing solutions.
Special instructions:
The drug is used under the control of the acid-base status and blood electrolytes, the functional state of the liver and blood pressure. Administer with caution to patients with calculous cholecystitis. The drug contains sorbitol, therefore patients with rare hereditary fructose intolerance should not use this drug. Use during pregnancy or breastfeeding. There are no data on contraindications during pregnancy or breastfeeding. Children. There are insufficient data on experience with administration to children. The ability to influence the reaction rate when driving vehicles or other mechanisms. Since the drug is used in a hospital setting, there are no data on such effects. The drug should not be used after the expiration date and should be stored out of the reach of children.
Overdose:
Phenomena of alkalosis occur, which quickly disappear on their own if the drug is immediately stopped, sometimes collapse, dehydration (due to increased diuresis). If the rate of administration is exceeded, tachycardia, increased blood pressure, shortness of breath, headache, chest pain, and abdominal pain may develop. These symptoms quickly disappear after stopping or significantly reducing the rate of administration of the solution.
Storage conditions: Store at a temperature not exceeding 25°C. Do not freeze.
Shelf life: 2 years.
Dispensing conditions: By prescription.
Manufacturer: Yuria-Pharm, LLC, Ukraine
Frequently asked questions from pharmacy visitors
How to instill the drug?
The medicine is administered intravenously in a stream or drip, depending on the pathology. The volume of fluid is determined individually and depends on the severity of the condition.
Why are they dripping?
The solution is administered as a plasma substitute for detoxification, improving the rheological properties of blood, and as an antishock agent.
What is rheosorbilact?
A solution for intravenous administration, which is used as a plasma substitute with a wide range of effects.
At what age is it prescribed?
There are no age restrictions, the main thing is to choose the right dosage for the child.
Material and methods
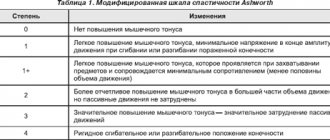
We examined 50 patients with purulent-septic diseases, isolated traumatic brain injuries (TBI), pneumonia, and operations for reconstruction of the internal carotid artery (ICA) (Table 1).
This heterogeneity of the patients we studied is explained by the fact that we were interested in the detoxifying effect of Reosorbilact in various toxic conditions caused by infection, injury, hypoxia and hypercapnia. These patients were in the surgical intensive care units No. 1 and the second clinic of the Tashkent Medical Academy from April to June 2013. In all patients, the detoxifying function of the drug Reosorbilact was assessed, as well as its effect on the coagulation system.
To judge the severity of intoxication in all patients, we used a rapid method for determining the concentration of average mass molecules (MWM) in the blood and urine, which, according to the vast majority of authors, have a universal toxic effect as a result of their pronounced membranotropic effect (Gabrielyan N.I. et al., 1985; Galaktionov S.G. et al., 1984; Ogai V.Ch., 1987).
The normal levels of MSM in the blood are: with a spectrum of 254 nm - 0.16-0.18 nmol, with a spectrum of 286 nm - 0.126-0.136 nmol.
MSM levels in urine are normal: with a spectrum of 254 nm - 0.5-0.9 nmol, with a spectrum of 286 nm - 0.26-0.43 nmol.
For the same purpose, we studied malondialdehyde (MDA) in the blood, which is formed during lipid peroxidation (LPO). Malondialdehyde is a secondary product of LPO. It has been established that under conditions of hypoxia and in some pathological conditions accompanied by tissue hypoxia, accumulation of lipid peroxidation products, in particular MDA, occurs (Osinskaya L.F., 1980; Morozov A.V. et al., 1986).
The calculation was carried out according to the method of L.I. Andreeva et al. (1988). The normal level of MDA in the blood is 2–3 nmol/ml.
The normal level of MDA in urine is 6–9 nmol/ml.
The essence of infusion preparation was to improve peripheral hemocirculation and remove toxins from tissue depots. This can be considered as a process of mobilization of toxins.
Having set the goal to achieve the most effective mobilization of toxins from tissue depots into the central bloodstream, we studied the level of MSM and MDA in venous blood and urine. For higher reliability, studies were carried out at different spectrophotometer wavelengths of 254 and 286 nm.
The amount of the drug administered intravenously is 400 ml 2 times a day at an injection rate of 40–60 drops per minute.
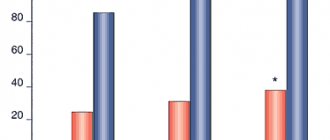
In the tables below. Figures 2–5 show the dynamics of MSM and MDA in the blood and urine before an intravenous infusion of 400 ml of Reosorbilact and 20, 120 and 240 minutes after its completion.
From the table 3 it is easy to notice that after intravenous infusion of Reosorbilact at a dose of 10–15 ml/kg body weight to patients with purulent-septic diseases, an increase in the concentration of MSM and MDA in the blood plasma was observed after 20 minutes from the end of the infusion, then the concentration of MSM and MDA decreased in blood plasma by an average of 22% from the initial level. In patients with pneumonia, isolated TBI, chronic cerebrovascular insufficiency (Tables 2, 4, 5), a gradual decrease in the concentration of toxins was noted by the 20th minute. In all study groups, 4 hours after the infusion of Reosorbilact, the concentration of MSM and MDA in the blood plasma decreased by an average of 65–70%.
This phenomenon can be explained based on the pharmacodynamic properties of Reosorbilact. By increasing plasma volume and reducing blood viscosity, Reosorbilact causes activation of microhemocirculation, erosion of aggregates of blood cells, restoration of exchange between blood and interstitium in all tissues of the body, which naturally leads to the leaching of MSM and MDA from the microhemocirculation into the central bloodstream.
In a parallel study of MSM and MDA in the urine after infusion of Reosorbilact, after 6 hours the concentration of MSM and MDA reached a maximum, which indicates an improvement in the rheological properties of blood caused by the infusion of Reosorbilact and an increase in glomerular filtration. This is confirmed by an increase in the concentration of MSM and MDA in the urine (Table 6–9).
Note!
The description of the drug Reosorbilact on this page is a simplified author’s version of the apteka911 website, created on the basis of the instructions for use.
Before purchasing or using the drug, you should consult your doctor and read the manufacturer's original instructions (attached to each package of the drug). Information about the drug is provided for informational purposes only and should not be used as a guide to self-medication. Only a doctor can decide to prescribe the drug, as well as determine the dose and methods of its use.