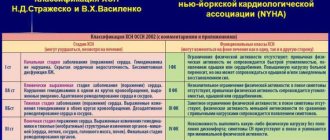
How are respiratory failure classified by severity?
The main criteria on which the classification is based are the measurement of blood gas balance, primarily the partial pressure of oxygen
(PaO2), carbon dioxide in arterial blood, as well as blood oxygen saturation (SaO2).
When determining the severity, it is important to identify the form in which the disease occurs.
DN shapes depending on the nature of the flow
There are two forms of DN - acute and chronic.
Differences between the chronic form and the acute form:
- chronic form of
DN - develops gradually, may not have symptoms for a long time. Usually appears after an untreated acute form; - acute
DN - develops quickly, in some cases symptoms appear within a few minutes. In most cases, the pathology is accompanied by hemodynamic disturbances (indicators of blood movement through the vessels).
The disease in a chronic form without exacerbations requires regular monitoring of the patient by a doctor.
Acute respiratory failure is more dangerous than chronic respiratory failure and requires immediate treatment.
Classification according to severity includes 3 types of chronic and 4 types of acute forms of pathology.
Severity of chronic DN
As DN develops, the symptoms become more complex and the patient’s condition worsens.
Diagnosing the disease at the initial stage simplifies and speeds up the treatment process.
| Degrees of DN | Types | Symptoms |
| I | Asymptomatic (hidden) |
|
| II | Compensated |
|
| III | Decompensated |
|
Symptoms in chronic deficiency are not as intense as in the acute form.
How is acute respiratory failure classified?
There are 4 degrees of severity of acute DN:
I degree
. It is characterized by shortness of breath (may appear on inhalation or exhalation), increased heart rate.
- PaO2 - from 60 to 79 mm Hg;
- SaO2 - 91-94%.
II degree
. The skin is marbled, bluish. Convulsions are possible, consciousness becomes darkened. When breathing, even at rest, additional muscles are activated.
- PaO2 - 41-59 mm Hg;
- SaO2 - from 75 to 90%.
III degree
. Shortness of breath: sharp shortness of breath is replaced by attacks of respiratory arrest, a decrease in the number of breaths per minute. Even at rest, the lips retain a rich bluish tint.
- PaO2 - from 31 to 40 mm Hg;
- SaO2 - from 62 to 74%.
IV degree
. State of hypoxic coma: breathing is rare, accompanied by convulsions. Possible respiratory arrest. Cyanosis of the skin of the whole body, blood pressure at a critically low level.
- PaO2 - up to 30 mm Hg;
- SaO2 - below 60%.
IV degree corresponds to a terminal condition and requires emergency assistance.
In the body of a healthy person, PaO2 is above 80 mm Hg, the level of SaO2 is above 95%.
If the indicators are outside the normal range, this indicates a high risk of developing respiratory failure.
What to do if you have ARF
First aid for respiratory failure should be provided after calling an ambulance. There is no talk of waiting for a local therapist in case of ARF.
The algorithm of actions is as follows:
- Call an ambulance.
- You can seat the person near the table so that he can put his hands on the table and raise his shoulders higher - closer to his chin. This will allow the auxiliary respiratory muscles to have more range of motion.
- Try to calm the victim.
- Free him from his outerwear, unfasten all the buttons and the belt of his trousers so that nothing interferes with his breathing.
- Provide fresh air flow from windows and vents.
- Constantly reassure the patient and be with him.
- If a person has asthma, help him take 1-2 breaths from his inhaler.
- If such symptoms occur after eating fish or canned food, give him “Activated carbon” or other sorbents.
If ARF develops as a result of a foreign body entering the throat, an urgent need to perform the Heimlich maneuver: stand behind the victim, clasp him with both hands. Clench one hand into a fist and place the palm of your other hand under it. Now, with a pushing movement directed upward, bending our elbows, we press on the abdominal area “under the stomach” until the victim’s airways are completely cleared.
If the development of ARF was preceded by a cold or a barking cough, it is recommended to inhale with a 0.05% naphthysine solution through a nebulizer before the ambulance arrives: 3-4 drops per 5 ml of saline solution.
When signs of ARF are present in a person who has been in a car accident, then it is possible to remove him from the car or shift him only after fixing his cervical spine with a Shants-type collar.
How are the severity of pathology in children determined?
DN in a child usually occurs in an acute form. The main differences between pathology in adults and children are different levels of blood gas parameters.
| Severity | Indicators (in mmHg) | Symptoms |
| I | — Ra oxygen drops to 60-80 |
|
| II |
|
|
| III |
|
|
| IV (hypoxic coma) |
|
|
If signs of DN 3 and 4 severity are detected, the child requires emergency hospitalization and intensive care. Treatment of children with mild DN (stages 1 and 2) is possible at home.
Development mechanism
The pathology is based on three pathogenetic aspects.
- Obstructive changes. Simply put, it is the closure of the respiratory structures in one way or another. For example, against the background of a spasm, when narrowing occurs due to tension in the walls of the bronchial tree.
Or an overlap with a foreign object, an intense inflammatory process as part of pneumonia or an asthmatic attack. There are many options.
- The second mechanism is restriction. Translated from Latin - restriction. As the name suggests, the pathological process is associated with changes in the structure of the lungs and bronchi. They become insufficiently elastic to allow normal breathing.
This is possible, for example, with pneumothorax.
Or as part of sclerosis, when lung tissues and structures are replaced by scar tissue. They become rough and are unable to collapse and restore their shape.
How to determine the severity of respiratory failure
To definitively diagnose the disease and its stage, it is enough to determine the level of blood gases.
Early diagnosis of DN includes examination of external respiration, identification of obstructive and restrictive disorders.
An examination for suspected DN necessarily includes spirometry and peak flowmetry, and arterial blood is taken for analysis.
The algorithm for determining respiratory failure consists of the following diagnostic criteria:
- oxygen tension (Pa) - lower than 45-50;
- carbon dioxide tension is higher than 50-60 (indicators in mmHg).
There is a low likelihood that a patient will undergo a blood gas test without good reason. Most often, diagnosis is carried out only when the pathology has manifested itself in the form of obvious
signs.
Diagnostics
You should start looking for the causes and treatment of shortness of breath immediately after you begin to notice such changes. The following methods are used to diagnose respiratory failure:
- Collection of anamnesis of the disease. The doctor carefully studies the patient’s medical history, his complaints, and learns his lifestyle.
- External examination of the patient. By studying the skin, chest muscles, and heart rhythm, the doctor can confirm or refute his guesses.
- Blood gas analysis is a reliable test. If there are deviations, a disease of the chest organs can be assumed.
The doctor makes the final diagnosis after a comprehensive diagnosis. It must be confirmed by laboratory tests.
How to recognize respiratory failure
Common clinical symptoms of DN include:
- rapid breathing, periodically changing to slow breathing;
- no breathing sounds are heard;
- pulse is unstable;
- retracted area between the ribs;
- the breathing process is difficult, it requires the use of additional muscles;
- the upper and lower limbs, the tip of the nose and the nasolabial triangle acquire a bluish tint;
- the patient has a pre-fainting state, loss of consciousness is possible;
- there is an increase in cardiac output (the volume of blood that is ejected by heart contractions per minute);
- the appearance of respiratory distress syndrome.
If at least a few symptoms of DN appear, the patient should undergo an examination, find out the reasons for the development of the pathology, and adhere to the doctor’s recommendations.
4.Treatment
The main directions are the restoration of airway patency, respiratory movements, cardiac activity, vascular tone, blood volume and composition. As a rule, the patient is intubated and connected to a ventilator (artificial lung ventilation), or an oxygen mask, nasal catheter, etc. is used. Bronchodilators, antispasmodics, analgesics or anesthetics, respiratory stimulants, blood substitutes and other compounds according to indications are administered symptomatically.
Measures are taken for drainage, removal of foreign bodies and accumulated substances, detoxification, desensitization, etc.
The prognosis is always serious - too much depends on the reasons that caused ARF, on accompanying circumstances and complications, on individual factors, but most importantly, on the timeliness and adequacy of the provision of pre-medical and medical care.
Sign up for a consultation
Causes
Development factors fit into the three pathogenetic moments mentioned above: obstruction, restriction and hemodynamic disorders. It is worth specifying the culprits of respiratory failure in patients:
- Bronchial asthma. A chronic disease for which spasms and asthma attacks are typical.
- Pneumonia. In other words, it is pneumonia of an infectious nature. Most often bacterial form.
- Severe types of tracheitis.
- Tumors.
- Congenital or acquired disorders of the structure of the chest and respiratory organs. Genetic or other abnormalities. Possible injury.
- Heart disorders. Ischemic disease, failure in the sub- or decompensation phase. Previous myocardial infarction and many other abnormalities. The full list can be found in the ICD classifier.
- Bronchitis. Inflammation of the anatomical structures of the same name.
- COPD Chronic obstructive pulmonary disease. Severe pathology.
- Thrombosis. Blockage of blood vessels with blood clots.
- Thromboembolism. The same thing, only there is also inflammation of the wall of the artery and vein.
- Vascular damage. Vasculitis. Autoimmune disorders.
- Poisoning. Intoxications that block cellular gas exchange. For example, cyanide compounds.
And this is only part of the reasons. Respiratory failure syndrome develops as a result of narrowing of the bronchi, changes in their structure (scarring), disturbances in the functioning of blood vessels and blood circulation.
Consequences
Complications concern the heart, central nervous system, lungs and bronchi themselves. Without treatment, a person is guaranteed to die. It is the matter of time.
In addition, the following problems are possible:
- Heart failure.
- Ischemic disease.
- Dementia.
- Decreased memory and concentration.
- General cognitive deficit.
- Pulmonary hypertension.
- Stroke.
- Heart attack.
- Left ventricular hypertrophy.
Pulmonary insufficiency is a severe and dangerous pathological process, which is accompanied by respiratory and cardiac disorders. The goal of treatment is to eliminate the primary disease and prevent complications.