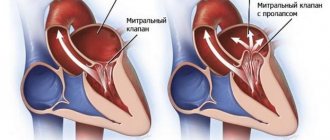
Chronic heart failure (CHF) is a disease characterized by the inability of the heart to pump a certain volume of blood sufficient to provide the body with oxygen. CHF can be caused by many diseases of the cardiovascular system, the most common of which include coronary heart disease, hypertension, endocarditis and rheumatoid heart defects. Weakening of the heart muscle leads to the impossibility of normal pumping of blood, as a result of which the amount of blood released into the vessels gradually decreases.
The development of heart failure occurs gradually; in the early stages, the disease can manifest itself only during physical exertion, then it begins to be felt at rest.
The appearance of characteristic symptoms at rest indicates that the disease has entered a severe stage. The progression of chronic heart failure threatens a significant deterioration of the patient’s condition, a decrease in his working capacity and even disability. The development of chronic liver and kidney failure, blood clots, and strokes may occur.
Conducting timely comprehensive diagnostics and competent treatment ensures a slowdown in the development of CHF and the prevention of dangerous complications of this serious disease.
In order to stabilize the condition, a patient diagnosed with “acute and chronic heart failure” must adhere to the correct lifestyle: normalize his weight, follow a low-salt diet, limit physical and emotional stress.
Chronic heart failure: classification
Chronic heart failure develops gradually, passing through certain stages.
Chronic heart failure - stages with characteristic symptoms:
- the first stage – the patient has no restrictions on physical activity: during normal exercise, weakness (lightheadedness), palpitations, shortness of breath or anginal pain does not occur;
- second stage - physical activity is moderately limited: the patient is in a comfortable state at rest, ordinary physical activity can provoke the appearance of weakness (lightheadedness), palpitations, shortness of breath or anginal pain;
- third stage – physical activity is expressed and limited: the patient’s comfortable state is observed exclusively at rest. When performing physical activity, weakness (lightheadedness), palpitations, shortness of breath or anginal pain appears;
- in the fourth degree of chronic heart failure, performing any exercise is invariably accompanied by discomfort. Chronic heart failure syndrome also appears at rest. Even with minimal loads, discomfort increases.
CHF classification includes various types of disease, subdivided depending on the form (acute and chronic heart failure), localization (left ventricular, right ventricular and mixed heart failure), origin (myocardial, overload or combined chronic heart failure). The tables used by the attending physician provide all the information about the disease, its stages and characteristic symptoms.
Publications in the media
Chronic systolic heart failure is a clinical syndrome that complicates the course of a number of diseases and is characterized by the presence of shortness of breath during exercise (and then at rest), fatigue, peripheral edema and objective signs of impaired cardiac function at rest (for example, auscultatory signs, echocardiographic data) . Statistical data. Chronic systolic heart failure occurs in 0.4–2% of the population. Its prevalence increases with age: in people over 75 years of age it develops in 10% of cases.
Etiology • Heart failure with low cardiac output •• Myocardial damage: ••• IHD (post-infarction cardiosclerosis, chronic myocardial ischemia) ••• Cardiomyopathies ••• Myocarditis ••• Toxic effects (for example, alcohol, doxorubicin) ••• Infiltrative diseases (sarcoidosis, amyloidosis) ••• Endocrine diseases ••• Nutritional disorders (vitamin B1 deficiency) •• Myocardial overload ••• Arterial hypertension ••• Rheumatic heart defects ••• Congenital heart defects (for example, aortic stenosis) •• Arrhythmias ••• Supraventricular and ventricular tachycardias ••• Atrial fibrillation • Heart failure with high cardiac output •• Anemia •• Sepsis •• Arteriovenous fistula.
Risk factors • Refusal of the patient from pharmacotherapy • Prescription of drugs with a negative inotropic effect, and their uncontrolled use • Thyrotoxicosis, pregnancy and other conditions associated with increased metabolic needs • Excess body weight • Presence of chronic pathology of the heart and blood vessels (arterial hypertension, coronary artery disease, defects hearts, etc.).
Pathogenesis • The pumping function of the heart is impaired, which leads to a decrease in cardiac output • As a result of a decrease in cardiac output, hypoperfusion of many organs and tissues occurs •• A decrease in cardiac perfusion leads to activation of the sympathetic nervous system and an increase in heart rate •• A decrease in renal perfusion causes stimulation of the renin-angiotensin systems. The production of renin increases, while excessive production of angiotensin II occurs, leading to vasoconstriction, water retention (edema, thirst, increased blood volume) and a subsequent increase in preload on the heart •• A decrease in the perfusion of peripheral muscles causes the accumulation of under-oxidized metabolic products in them, as well as hypoxia leads to severe fatigue.
CLASSIFICATIONS Classification of the XII All-Union Congress of Therapists in 1935 ( N.D. Strazhesko, V.Kh. Vasilenko). • Stage I (initial) - latent heart failure, manifested only during physical activity (shortness of breath, tachycardia, fatigue). • Stage II (severe) - prolonged circulatory failure, hemodynamic disturbances (stagnation in the systemic and pulmonary circulation), dysfunction of organs and metabolism are also expressed at rest •• Period A - the beginning of a long stage, characterized by mild hemodynamic disturbances, dysfunction hearts or only parts of them •• Period B - the end of a long stage, characterized by profound hemodynamic disturbances, the entire cardiovascular system is involved in the process. • Stage III (final, dystrophic) - severe hemodynamic disorders, persistent changes in metabolism and functions of all organs, irreversible changes in the structure of tissues and organs.
New York Heart Association classification (1964) • Class I - ordinary physical activity does not cause significant fatigue, shortness of breath or palpitations • Class II - mild limitation of physical activity: satisfactory health at rest, but ordinary physical activity causes fatigue, palpitations, shortness of breath or pain • Class III - severe limitation of physical activity: satisfactory health at rest, but less than usual load leads to the appearance of symptoms • Class IV - inability to perform any physical activity without deteriorating well-being: symptoms of heart failure are present even at rest and intensify with any physical activity .
The classification of the Society of Heart Failure Specialists (OSSN, 2002) was adopted at the All-Russian Congress of Cardiologists in October 2002. The convenience of this classification is that it not only reflects the state of the process, but also its dynamics. The diagnosis must reflect both the stage of chronic heart failure and its functional class. It is necessary to take into account that the correspondence between the stage and the functional class is not entirely clear - the functional class is set in the presence of slightly less pronounced manifestations than is necessary to assign the corresponding stage of heart failure.
• Stages of chronic heart failure (may worsen despite treatment) •• Stage I - the initial stage of heart disease (damage). Hemodynamics are not impaired. Latent heart failure Asymptomatic left ventricular dysfunction •• Stage IIA - clinically pronounced stage of heart disease (damage). Hemodynamic disturbances in one of the blood circulation circles, expressed moderately. Adaptive remodeling of the heart and blood vessels •• Stage IIB - severe stage of heart disease (damage). Pronounced changes in hemodynamics in both circles of blood circulation. Maladaptive remodeling of the heart and blood vessels •• Stage III - the final stage of cardiac damage. Pronounced changes in hemodynamics and severe (irreversible) structural changes in target organs (heart, lungs, blood vessels, brain, kidneys). The final stage of organ remodeling.
• Functional classes of chronic heart failure (can change during treatment in either direction) •• FC I - there are no restrictions on physical activity: habitual physical activity is not accompanied by rapid fatigue, shortness of breath or palpitations. The patient can tolerate increased workload, but it may be accompanied by shortness of breath and/or delayed recovery •• FC II - slight limitation of physical activity: there are no symptoms at rest, habitual physical activity is accompanied by fatigue, shortness of breath or palpitations •• FC III - noticeable limitation of physical activity: at rest there are no symptoms, physical activity of lesser intensity compared to usual exercise is accompanied by the appearance of symptoms •• FC IV - inability to perform any physical activity without discomfort; Symptoms of heart failure are present at rest and worsen with minimal physical activity.
Clinical manifestations • Complaints - shortness of breath, attacks of suffocation, weakness, fatigue • • Shortness of breath in the initial stage of heart failure occurs during physical activity, and in case of severe heart failure - at rest. It appears as a result of increased pressure in the pulmonary capillaries and veins. This reduces the extensibility of the lungs and increases the work of the respiratory muscles. •• Severe heart failure is characterized by orthopnea - a forced sitting position taken by the patient to facilitate breathing with severe shortness of breath. The deterioration of health in the supine position is due to the deposition of fluid in the pulmonary capillaries, leading to an increase in hydrostatic pressure. In addition, in the lying position, the diaphragm rises, which makes breathing somewhat difficult. • Chronic heart failure is characterized by paroxysmal nocturnal shortness of breath (cardiac asthma), caused by the occurrence of interstitial pulmonary edema. At night, during sleep, an attack of severe shortness of breath develops, accompanied by coughing and the appearance of wheezing in the lungs. As heart failure progresses, alveolar pulmonary edema may occur •• Rapid fatigue in patients with heart failure appears due to insufficient oxygen supply to skeletal muscles •• Patients with chronic heart failure may experience nausea, loss of appetite, abdominal pain, abdominal enlargement (ascites) due to blood stagnation in the liver and portal vein system •• From the side of the heart, pathological III and IV heart sounds can be heard. Moist rales are detected in the lungs. Hydrothorax is characteristic, often right-sided, resulting from an increase in pleural capillary pressure and extravasation of fluid into the pleural cavity.
• Clinical manifestations of heart failure significantly depend on its stage •• Stage I - signs (fatigue, shortness of breath and palpitations) appear during normal physical activity, there are no manifestations of heart failure at rest •• Stage IIA - there are unexpressed hemodynamic disturbances. Clinical manifestations depend on which parts of the heart are predominantly affected (right or left) ••• Left ventricular failure is characterized by stagnation in the pulmonary circulation, manifested by typical inspiratory shortness of breath with moderate physical exertion, attacks of paroxysmal nocturnal shortness of breath, and rapid fatigue. Swelling and enlargement of the liver are uncharacteristic. ••• Right ventricular failure is characterized by the formation of congestion in the systemic circulation. Patients are concerned about pain and heaviness in the right hypochondrium, decreased diuresis. The liver is characterized by enlargement (the surface is smooth, the edge is rounded, palpation is painful). A distinctive feature of stage IIA heart failure is considered to be complete compensation of the condition during treatment, i.e. reversibility of manifestations of heart failure as a result of adequate treatment •• Stage IIB - there are profound hemodynamic disturbances, the entire circulatory system is involved in the process. Shortness of breath occurs with the slightest physical exertion. Patients are concerned about a feeling of heaviness in the right hypochondrium, general weakness, and sleep disturbances. Orthopnea, edema, ascites are characteristic (a consequence of increased pressure in the hepatic veins and peritoneal veins - transudation occurs, and fluid accumulates in the abdominal cavity), hydrothorax, hydropericardium •• Stage III - the final dystrophic stage with profound irreversible metabolic disorders. As a rule, the condition of patients at this stage is severe. Shortness of breath is pronounced even at rest. Characterized by massive edema, accumulation of fluid in the cavities (ascites, hydrothorax, hydropericardium, edema of the genital organs). At this stage, cachexia occurs.
Instrumental data • ECG : you can identify signs of blockade of the left or right branch of the His bundle, ventricular or atrial hypertrophy, pathological Q waves (as a sign of a previous MI), arrhythmias. A normal ECG casts doubt on the diagnosis of chronic heart failure. • EchoCG allows you to clarify the etiology of chronic heart failure and assess the functions of the heart, the degree of their impairment (in particular, determine the ejection fraction of the left ventricle). Typical manifestations of heart failure are expansion of the cavity of the left ventricle (as it progresses, expansion of other chambers of the heart), an increase in the end-systolic and end-diastolic dimensions of the left ventricle, and a decrease in its ejection fraction. • X-ray examination •• It is possible to detect venous hypertension in the form of redistribution of blood flow in favor of the upper parts of the lungs and an increase in the diameter of blood vessels •• With congestion in the lungs, signs of interstitial edema are detected (Kerley lines in the costophrenic sinuses) or signs of pulmonary edema •• Hydrothorax is detected ( most often right-sided) •• Cardiomegaly is diagnosed when the transverse size of the heart increases by more than 15.5 cm in men and more than 14.5 cm in women (or when the cardiothoracic index is more than 50%). • Catheterization of the cardiac cavities reveals an increase in pulmonary capillary wedge pressure of more than 18 mm Hg. Diagnostic criteria - Framingham criteria for the diagnosis of chronic heart failure, divided into major and minor • Major criteria: paroxysmal nocturnal dyspnea (cardiac asthma) or orthopnea, distention of the jugular veins, wheezing in the lungs, cardiomegaly, pulmonary edema, pathological III heart sound, increased central venous pressure ( more than 160 mm water column), blood flow time more than 25 s, positive “hepatojugular reflux” • Minor criteria: swelling in the legs, night cough, shortness of breath on exertion, liver enlargement, hydrothorax, tachycardia more than 120 per minute, decrease in vital capacity by 1 /3 of the maximum • To confirm the diagnosis of chronic heart failure, either 1 major or 2 minor criteria are required. The symptoms detected must be related to heart disease.
Differential diagnosis • Nephrotic syndrome - a history of edema, proteinuria, renal pathology • Liver cirrhosis • Occlusive lesions of the veins with subsequent development of peripheral edema. Treatment • It is necessary to first evaluate the possibility of influencing the cause of the deficiency. In some cases, effective etiological intervention (for example, surgical correction of heart disease, myocardial revascularization in ischemic heart disease) can significantly reduce the severity of manifestations of chronic heart failure • In the treatment of chronic heart failure, non-drug and drug therapy methods are distinguished. It should be noted that both types of treatment should complement each other.
Non-drug treatment • Limiting the consumption of table salt to 5–6 g/day, liquid (up to 1–1.5 l/day) • Optimizing physical activity •• Moderate physical activity is possible and even necessary (walking for at least 20–30 minutes 3 –5 r/week) •• Complete physical rest should be observed if the condition worsens (at rest the heart rate decreases and the work of the heart decreases).
Drug therapy . The ultimate goal of treatment of chronic heart failure is to improve the quality of life and increase its duration.
• Diuretics. When prescribing them, it is necessary to take into account that the occurrence of edema in heart failure is associated with several reasons (constriction of the renal vessels, increased secretion of aldosterone, increased venous pressure. Treatment with diuretics alone is considered insufficient. In chronic heart failure, loop (furosemide) or thiazide (for example, hydrochlorothiazide) diuretics. If the diuretic response is insufficient, loop diuretics and thiazides are combined •• Thiazide diuretics. Hydrochlorothiazide is usually used in a dose of 25 to 100 mg/day. It should be remembered that if the renal GFR is less than 30 ml/min, it is not advisable to use thiazides •• Loop diuretics begin to act faster, their diuretic effect is more pronounced, but less durable than that of thiazide diuretics. Furosemide is used at a dose of 20–200 mg/day IV, depending on the manifestations of edema and diuresis. It can be prescribed orally at a dose of 40– 100 mg/day.
• ACE inhibitors cause hemodynamic unloading of the myocardium due to vasodilation, increased diuresis, and decreased filling pressure of the left and right ventricles. Indications for prescribing ACE inhibitors are clinical signs of heart failure, a decrease in left ventricular ejection fraction of less than 40%. When prescribing ACE inhibitors, certain conditions must be observed according to the recommendations of the European Society of Cardiology (2001) •• It is necessary to stop taking diuretics 24 hours before taking ACE inhibitors •• Blood pressure should be monitored before and after taking ACE inhibitors •• Treatment begins with small doses with gradual their increase •• It is necessary to monitor renal function (diuresis, relative density of urine) and the concentration of blood electrolytes (potassium, sodium ions) while increasing the dose every 3–5 days, then every 3 and 6 months •• Avoid co-administration of potassium-sparing diuretics (their can be prescribed only for hypokalemia) •• Concomitant use of NSAIDs should be avoided.
• The first positive data have been obtained on the beneficial effect of angiotensin II receptor blockers (in particular, losartan) on the course of chronic heart failure as an alternative to ACE inhibitors in cases of intolerance or contraindications to their use.
• Cardiac glycosides have a positive inotropic (increase and shorten systole), negative chronotropic (decreasing heart rate), negative dromotropic (slowing AV conduction) effect. The optimal maintenance dose of digoxin is considered to be 0.25–0.375 mg/day (in elderly patients 0.125–0.25 mg/day); The therapeutic concentration of digoxin in blood serum is 0.5–1.5 mg/l. Indications for the use of cardiac glycosides are tachysystolic atrial fibrillation and sinus tachycardia.
• b-blockers •• The mechanism of beneficial action of β-blockers in chronic heart failure is due to the following factors ••• Direct protection of the myocardium from the adverse effects of catecholamines ••• Protection against catecholamine-induced hypokalemia ••• Improvement of blood flow in the coronary arteries due to a decrease in heart rate and improvement diastolic relaxation of the myocardium ••• Reducing the effect of vasoconstrictor systems (for example, due to decreased renin secretion) ••• Potentiation of the vasodilating kallikrein-kinin system ••• Increasing the contribution of the left atrium to the filling of the left ventricle due to improved relaxation of the latter •• Currently from b -adrenergic blockers for the treatment of chronic heart failure, carvedilol is recommended for use - a b1- and a1-blocker with vasodilating properties. The initial dose of carvedilol is 3.125 mg 2 times / day, followed by an increase in the dose to 6.25 mg, 12.5 mg or 25 mg 2 times / day in the absence of side effects in the form of arterial hypotension, bradycardia, decreased left ventricular ejection fraction (according to EchoCG) and other negative manifestations of the action of b-blockers. Metoprolol is also recommended, starting with a dose of 12.5 mg 2 times / day, bisoprolol 1.25 mg 1 time / day under the control of ventricular ejection fractions with a gradual increase in dose after 1-2 weeks.
• Spironolactone. It has been established that the administration of the aldosterone antagonist spironolactone at a dose of 25 mg 1–2 times a day (in the absence of contraindications) helps to increase the life expectancy of patients with heart failure. • Peripheral vasodilators are prescribed for chronic heart failure if there are contraindications or if ACE inhibitors are poorly tolerated. Of the peripheral vasodilators, hydralazine is used at a dose of up to 300 mg/day, isosorbide dinitrate at a dose of up to 160 mg/day.
• Other cardiotonic drugs . β-Adrenergic agonists (dobutamine), phosphodiesterase inhibitors are usually prescribed for 1–2 weeks in the final stage of heart failure or in case of a sharp deterioration in the patient’s condition.
• Anticoagulants. Patients with chronic heart failure are at high risk of thromboembolic complications. Both pulmonary embolism due to venous thrombosis and thromboembolism of vessels in the systemic circulation caused by intracardiac thrombi or atrial fibrillation are possible. The administration of indirect anticoagulants to patients with chronic heart failure is recommended in the presence of atrial fibrillation and a history of thrombosis.
• Antiarrhythmic drugs. If there are indications for the prescription of antiarrhythmic drugs (atrial fibrillation, ventricular tachycardia), it is recommended to use amiodarone at a dose of 100–200 mg/day. This drug has minimal negative inotropic effects, whereas most other drugs in this class reduce left ventricular ejection fraction. In addition, antiarrhythmic drugs themselves can provoke arrhythmias (proarrhythmic effect). Surgery
• The choice of the optimal method of surgical treatment depends on the cause leading to heart failure. Thus, in case of ischemic heart disease, in many cases, myocardial revascularization is feasible; in case of idiopathic subaortic hypertrophic stenosis, septal myectomy; in case of valvular defects, prosthetics or reconstructive interventions on the valves; in case of bradyarrhythmias, pacemaker implantation, etc.
• In case of heart failure refractory to adequate therapy, the main surgical treatment is heart transplantation. • Methods of mechanical circulatory support (implantation of assisters, artificial ventricles and biomechanical pumps), previously proposed as temporary options before transplantation, have now acquired the status of independent interventions, the results of which are comparable to the results of transplantation. • To prevent the progression of cardiac dilatation, devices are implanted in the form of a mesh that prevents excessive expansion of the heart. • In case of cor pulmonale that is tolerant to treatment, transplantation of the heart-lung complex seems to be a more appropriate intervention.
Forecast. Overall, the 3-year survival rate of patients with chronic systolic heart failure is 50%. The mortality rate from chronic systolic heart failure is 19% per year.
• Factors, the presence of which correlates with a poor prognosis in patients with heart failure •• Decrease in left ventricular ejection fraction of less than 25% •• Inability to climb one floor and move at a normal pace for more than 3 minutes •• Decrease in the content of sodium ions in blood plasma less than 133 mEq /l •• Decrease in the concentration of potassium ions in the blood plasma less than 3 meq/l •• Increase in the content of norepinephrine in the blood •• Frequent ventricular extrasystole during daily ECG monitoring.
• The risk of sudden cardiac death in patients with heart failure is 5 times higher than in the general population. Most patients with chronic heart failure die suddenly, mainly from ventricular fibrillation. Prophylactic administration of antiarrhythmic drugs does not prevent this complication.
ICD-10 • I50 Heart failure
Chronic heart failure: pathogenesis
The main causes of chronic heart failure: damage to the heart muscle or impairment of its ability to pump the required amount of blood through the vessels, which can occur in patients suffering from the following pathologies:
- arterial hypertension – high blood pressure;
- IHD (coronary heart disease);
- heart defects.
The development of CHF in women is most often caused by arterial hypertension. In men, chronic heart failure usually occurs as a consequence of coronary heart disease.
In addition, chronic heart failure can develop due to the presence of the following diseases and dependencies:
- diabetes mellitus;
- arrhythmias (heart rhythm disturbances);
- cardiomyopathies;
- myocarditis;
- alcoholism and smoking.
CHF: symptoms
The clinical picture of CHF is quite diverse and depends on the severity and duration of its course. The disease develops slowly over several years. Lack of treatment threatens serious deterioration of the patient's condition.
Most often, chronic heart failure is manifested by the following symptoms:
- shortness of breath during physical exertion, when the patient moves to a supine position, and later at rest;
- dizziness, fatigue and weakness;
- nausea and lack of appetite;
- swelling of the lower extremities;
- development of ascites (accumulation of fluid in the abdominal cavity);
- weight gain due to swelling;
- fast or irregular heartbeat;
- dry cough with pinkish sputum;
- decreased intelligence and attention.
Classification of the disease
In ICD 10, chronic heart failure is coded 150, divided into systolic and diastolic forms. This is not the only division of pathology; there are other bases for classification. One of the most common divisions is by stages :
- Stage I - primary changes, decreased functionality of the left ventricle of the heart. At this moment, there are still no serious disturbances in blood flow, so symptoms of chronic heart failure do not appear.
- Stage II A - blood moves along the bed more slowly and can form areas of stagnation in the pulmonary fields or lower segment of the body.
- II B - hemodynamics suffer, affecting both circles of blood circulation at once. This stage is already characterized by noticeable changes in blood vessels and the heart muscle itself. The doctor can identify signs of the disease by recording extraneous whistling in the lungs and swelling of the lower extremities.
- Stage III - swelling spreads throughout the body. Now they appear not only in the legs, but also become noticeable in the hips and lumbar area. Fluid can accumulate in the peritoneum and spread throughout the body. At this stage, irreversible changes affect vital organs: the brain, heart, bronchopulmonary system, kidneys and liver.
There is a well-known classification by functional units or classes, which is determined by the general well-being of a sick person in response to physical activity. There are 4 stages of chronic heart failure. At the first stage, activity does not cause major changes. Shortness of breath may occur during intense activities, although in many situations there is no shortness of breath.
The second functional class can be determined by normal well-being during the period of rest and increased heartbeat under light loads. When moving to stage 3, the patient experiences significant limitations in physical activity. And at the 4th stage, loads are practically inaccessible, as they cause acute discomfort. Another popular gradation is the division by zones of heart damage. Thus, experts distinguish between left-, right- and two-ventricular heart failure.
Chronic heart failure: risk group
The following risk factors, or at least one of them, can provoke the development of CHF. When several factors are combined, the likelihood of chronic heart failure increases significantly.
The risk group for the development of CHF includes patients suffering from the following diseases:
- cardiac ischemia;
- history of myocardial infarction;
- high blood pressure;
- heart rhythm disturbance;
- diabetes;
- Congenital heart defect;
- frequent viral diseases;
- chronic renal failure;
- alcohol addiction.
Pregnancy with chronic heart failure: disease progression
The body of a pregnant woman has to overcome quite serious loads, including on the heart. Due to intrauterine growth and fetal development, the heart muscle must cope with the circulation of increased blood volume.
In women suffering from certain cardiovascular diseases, this heart function is often impaired, which leads to the development of CHF. The degrees of heart failure manifest themselves in different ways, but if even the slightest discomfort occurs, pregnant women should immediately inform their doctor.
Prevention and prognosis
To prevent heart failure, you need proper nutrition, sufficient physical activity, and giving up bad habits. All diseases of the cardiovascular system must be promptly identified and treated.
The prognosis in the absence of treatment for CHF is unfavorable, since most heart diseases lead to its wear and tear and the development of severe complications. When carrying out drug and/or cardiac surgery, the prognosis is favorable, because the progression of the insufficiency slows down or a radical cure for the underlying disease occurs.
Diagnosis of chronic heart failure
When diagnosing CHF, doctors at the Yusupov Hospital take into account medical history, characteristic symptoms and the results of a physical examination, instrumental and laboratory tests.
Laboratory tests include the following tests:
- General blood test - as a rule, there are no changes. Sometimes the presence of moderate anemia is determined;
- ESR (erythrocyte sedimentation rate) - an increase in ESR is observed with rheumatic heart disease or infective endocarditis, which resulted in the development of heart failure;
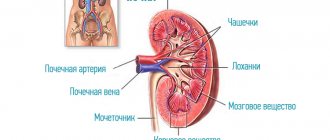
- general urinalysis - performed to diagnose kidney complications and exclude the renal origin of edema. The most common possible manifestation of CHF is an increase in protein levels in the urine;
- study of total protein and protein fractions - in CHF their indicators decrease, which is associated with redistribution into the edematous fluid;
- blood glucose level – important in order to exclude such a risk factor for CHF as diabetes mellitus;
- indicators of cholesterol, low and high density lipoproteins - a clear relationship has been proven between high cholesterol levels and atherosclerosis, hypertension, coronary heart disease; Elevated levels of lipoproteins and cholesterol in CHF may indicate a more severe course of the disease;
- the level of sodium and potassium in the blood - edema that occurs in patients with CHF is the cause of a significant decrease in the level of these microelements. Monitoring blood composition is especially important when taking diuretic drugs, as well as in cases where the patient has chronic heart and kidney failure;
- study of the level of brain natriuretic propeptide, a protein whose formation in the heart muscle is associated with its excessive stretching and overload. Its circulation in the blood is quite long, so laboratory testing can easily determine its level. With increasing cardiac overload, the secretion of propeptide is activated. Therefore, its indicators are important for determining the severity of CHF.
Additionally, instrumental studies are prescribed, the scope of which is determined by the attending physician:
- plain chest x-ray - to assess the position and size of the heart, exclude or confirm concomitant changes in the lungs (if the patient is suspected of chronic pulmonary heart failure);
- electrocardiography (ECG) - to determine heart rhythm disturbances and the consequences of a previous myocardial infarction;
- echocardiography - to differentiate systolic and diastolic heart failure, assess the activity of all parts of the heart, its size, the thickness of the heart muscle and its valves;
- stress tests – allow you to study the reaction of the heart muscle to increased physical activity;
- coronary angiocardiography - the essence of this x-ray study is the introduction of a special contrast agent through a catheter directly into the vessels of the heart, thanks to which it is possible to diagnose coronary heart disease;
- transesophageal echocardiography - ultrasound examination of the heart with placement of a sensor in the esophagus. Can be used if conventional cardiography does not provide a sufficiently clear image, and also helps to identify blood clots in the right atrium in patients with atrial fibrillation;
- stress echocardiography - ultrasound examination of the heart at rest and after exercise or after the use of medications with an effect similar to exercise. The study allows you to assess the reserve capabilities of the heart and identify areas of viable heart muscle;
- spiral computed tomography - during the procedure, X-rays are taken at different depths, which, in combination with MRI, provides an accurate image of the heart;
- endomyocardial biopsy - during the diagnostic procedure, tissues of the muscle and inner lining of the heart are taken for histological examination, which makes it possible to clarify the cause of the disease in complex cases.
In addition, patients at the Yusupov Hospital are given consultations with therapists and cardiac surgeons.
How is heart failure diagnosed?
Diagnosis begins with a comprehensive assessment of a person's medical history, paying particular attention to symptoms (onset, duration, manifestation). This helps classify the severity of the symptom. The heart and lungs are examined. If a heart attack or rhythm disorder is suspected, a 12-lead resting ECG is performed. In addition, echocardiography and complete blood count. The need for catheterization is determined individually.
In diagnosis, you need to start with analyzing complaints and identifying symptoms. Patients complain of shortness of breath, fatigue, and palpitations.
The doctor asks the patient:
- How does he sleep?
- Has the number of pillows changed over the past week?
- Did the person begin to sleep sitting instead of lying down?
The second stage of diagnosis is a physical examination, including:
- Skin examination;
- Assessment of the severity of fat and muscle mass;
- Checking for edema;
- Pulse palpation;
- Palpation of the liver;
- Auscultation of the lungs;
- Auscultation of the heart (1st sound, systolic murmur at the 1st point of auscultation, analysis of the 2nd tone, “gallop rhythm”);
- Weighing (a 1% decrease in body weight over 30 days indicates the onset of cachexia).
If heart failure is suspected, the electrolyte and gas composition of the blood, acid-base balance, urea, creatinine, cardio-specific enzymes, and indicators of protein-carbohydrate metabolism are determined.
Based on specific changes, an ECG helps to identify hypertrophy and insufficiency of blood supply (ischemia) of the myocardium, as well as arrhythmias. Based on electrocardiography, various stress tests using an exercise bike (veloergometry) and a treadmill (treadmill test) are widely used. Such tests with a gradually increasing level of load make it possible to judge the reserve capabilities of heart function.
Using ultrasound echocardiography, it is possible to determine the cause of heart failure, as well as evaluate the pumping function of the myocardium. Using cardiac MRI, coronary heart disease, congenital or acquired heart defects, arterial hypertension and other diseases are successfully diagnosed. X-ray of the lungs and chest organs in heart failure determines congestive processes in the pulmonary circulation, cardiomegaly.
Chronic heart failure: treatment, drugs
CHF is a disease in which patients need to constantly take medications. For chronic heart failure, drugs are used that help slow the progression of the process and improve the patient's condition. In some patients with CHF, treatment requires surgical intervention.
Medicines for chronic deficiency are primary, auxiliary and additional.
The main drugs include ACE inhibitors (angiotensin-converting enzyme), angiotensin receptor antagonists, beta-blockers, aldosterone receptor antagonists, diuretics, ethyl esters of polyunsaturated fatty acids, cardiac glycosides. Cardiac glycoside for the treatment of chronic heart failure is used most often in patients with atrial fibrillation.
Auxiliary drugs for chronic heart failure are used in special clinical situations with complications of CHF. These include nitrates, calcium antagonists, antiarrhythmic drugs, antiplatelet agents, and non-glycoside inotropic stimulants.
Additional medications for chronic insufficiency: statins, indirect anticoagulants.
For patients diagnosed with chronic heart failure, clinical recommendations from doctors relate not only to taking medications, but also to revising their lifestyle in general:
- it is necessary to stop smoking and drinking alcohol;
- bring your weight back to normal;
- follow a salt-free diet. Nutrition for CHF should be balanced, contain a sufficient amount of proteins and vitamins;
- walk more in the fresh air.
How is heart failure treated?
For chronic heart failure, medications (such as ACE inhibitors, beta blockers and diuretics) are used. Medicines are used to prevent complications and improve quality of life. ACE inhibitors and beta blockers can prolong life, but they must be taken regularly to achieve a beneficial effect.
In addition, rhythm therapy (to treat cardiac arrhythmias) and implantation of a three-chamber pacemaker are used. The latter ensures timely activation of the atria and both ventricles. A defibrillator is also often implanted as part of a pacemaker to counteract dangerous heart rhythm disturbances in the setting of severe heart failure. This treatment is also known as resynchronization therapy. An important part of successful treatment is physical therapy.
In the treatment of heart failure, a properly organized diet plays an important role. Dishes should be easily digestible. The diet should include fresh fruits and vegetables as a source of vitamins and microelements. The amount of table salt is limited to 1-2 g per day, and liquid intake to 500-600 ml.
Pharmacotherapy, which includes the following groups of drugs, can improve the quality of life and prolong it:
- cardiac glycosides – enhance the contractile and pumping function of the myocardium, stimulate diuresis, and increase the level of exercise tolerance;
- ACE inhibitors (angiotensin-converting enzyme) and vasodilators - reduce vascular tone, expand the lumen of blood vessels, thereby reducing vascular resistance and increasing cardiac output;
- nitrates - dilate the coronary arteries, increase cardiac output and improve blood filling of the ventricles;
- diuretics – remove excess fluid from the body, thereby reducing swelling;
- β-blockers - increase cardiac output, improve the filling of the heart chambers with blood, reduce the heart rate;
- anticoagulants - reduce the risk of blood clots in blood vessels and, accordingly, thromboembolic complications;
- agents that improve metabolic processes in the heart muscle (potassium supplements, vitamins).
If cardiac asthma or pulmonary edema (acute left ventricular failure) develops, the patient requires emergency hospitalization.
Prescribed drugs that increase cardiac output, diuretics, nitrates. Oxygen therapy is mandatory. Removal of fluid from body cavities (abdominal, pleural, pericardial) is carried out by puncture.
Chronic heart failure: recommendations for prevention
Prevention of chronic heart failure is based on the basic principles that every person should adhere to, especially after 40-45 years:
- engage in physical activity regularly;
- control blood pressure;
- lead a lifestyle that prevents the development of coronary artery disease;
- normalize metabolism (reduce excess weight, control cholesterol levels, limit salt intake);
- give up frequent consumption of coffee, alcoholic beverages, quit smoking.
Thanks to the clear and consistent implementation of the above recommendations, it is possible to significantly slow down the pathological process and improve the patient’s quality of life.
Diagnosis and treatment of CHF in Moscow is offered by the Yusupov Hospital Therapy Clinic, a leading multidisciplinary center equipped with the latest equipment. The use of innovative techniques and the vast experience of the clinic’s team of specialists - therapists, cardiologists, diagnosticians - allows us to achieve impressive results in the treatment of chronic heart failure. Each patient at the Yusupov Hospital is provided with professional nursing care. In case of chronic heart failure, not only drug treatment is necessary, but also a review of the diet, which our qualified nutritionists help to cope with, who develop a special nutrition plan for each patient with CHF.