Velaxin
Use during pregnancy and breastfeeding
Contraindicated for use during pregnancy and lactation (breastfeeding).
Women of childbearing potential should use reliable methods of contraception during treatment and consult a doctor immediately if they become pregnant or plan to become pregnant.
Venlafaxine and the EDV metabolite are excreted in breast milk. The safety of these substances for newborns has not been proven, therefore, if it is necessary to take venlafaxine during lactation, the issue of stopping breastfeeding should be decided. If the mother's treatment was completed shortly before delivery, the newborn may experience withdrawal symptoms.
Use for liver dysfunction
Contraindicated in severe liver dysfunction.
In case of moderate liver failure (prothrombin time from 14 to 18 seconds), the dose should be reduced by 50%.
Use for renal impairment
Contraindicated in severe renal failure (creatinine clearance < 10 ml/min).
In patients with renal failure with CC 10-30 ml/min, the dose should be reduced by 25-50%. Due to the prolongation of T1/2 of venlafaxine and its active metabolite (EDM), such patients should take the entire dose 1 time/day.
Patients on hemodialysis may receive 50% of the usual daily dose of venlafaxine after completion of the hemodialysis session.
Use in children
Contraindicated in children and adolescents under 18 years of age.
Use in elderly patients
In elderly patients, venlafaxine should be used at the lowest effective dose. When increasing the dose, the patient should be under close medical supervision
Elderly patients should be warned about the possibility of dizziness and impaired balance. While taking venlafaxine, especially in conditions of dehydration or decreased blood volume, hyponatremia and/or syndrome of insufficient ADH secretion may occur in elderly patients
special instructions
Venlafaxine should be used with caution after a recent myocardial infarction, with heart failure in the stage of decompensation, with unstable angina, arterial hypertension, tachycardia, tachyarrhythmia, history of seizures, intraocular hypertension, angle-closure glaucoma, history of manic states, predisposition to bleeding from the skin integuments and mucous membranes, initially reduced body weight.
In patients with depressive disorders, the possibility of suicide attempts should be considered before starting any drug therapy. Therefore, to reduce the risk of overdose, venlafaxine should be used at the minimum effective dose when starting treatment, whenever possible, and the patient should be under close medical supervision.
In patients with affective disorders, when treated with antidepressants (including venlafaxine), hypomanic or manic states may occur. As with other antidepressants, venlafaxine should be used with caution in patients with a history of mania. Such patients require medical supervision.
If epileptic seizures occur, treatment should be interrupted.
The risk of tachycardia increases when venlafaxine is used in high doses.
During treatment, regular monitoring of blood pressure is recommended, especially during the period of dose adjustment or increase.
Patients, especially the elderly, should be warned about the possibility of dizziness and impaired balance.
While taking venlafaxine, especially in conditions of dehydration or decreased blood volume (including in elderly patients and patients taking diuretics), hyponatremia and/or syndrome of insufficient ADH secretion may occur.
Mydriasis may occur while taking the drug, and therefore it is recommended to monitor intraocular pressure in patients prone to increased pressure or suffering from angle-closure glaucoma.
As with other drugs that act on the central nervous system, the physician should closely monitor patients for signs of venlafaxine abuse. Careful monitoring and observation is necessary for patients with a history of such symptoms.
While taking venlafaxine, special care should be taken when conducting electroconvulsive therapy, because There is no experience with the use of venlafaxine in these conditions.
During treatment you should avoid drinking alcohol.
Impact on the ability to drive vehicles and operate machinery
Despite the fact that venlafaxine does not affect psychomotor and cognitive functions, it should be borne in mind that any drug therapy with psychoactive drugs can impair thought processes and reduce the ability to perform motor functions. The patient should be warned about this before starting treatment. If such violations occur, the degree and duration of restrictions must be established by a doctor.
Use of velafax in patients with comorbid depression and anxiety
Depressive and anxiety disorders are the two most common groups of mental disorders. Thus, about 19% of the population exhibits signs sufficient to diagnose a depressive episode, and 17% of the general population meets criteria for an anxiety disorder (Kessler RC et al., 1994). A similar pattern is observed among outpatients in both psychiatric (Bradley N. et al., 2007) and general medical institutions (Zing W. et al., 1990). About 2/3 of patients diagnosed with major depression show signs sufficient to diagnose a current anxiety disorder (Zimmerman M. et al., 2000).
The coexistence of symptoms of anxiety and depression has important therapeutic and prognostic significance, since this group of patients is more likely to experience a chronic course of the disease and more severe impairments in social and everyday functioning (Liebowitz MR, 1993, Lyddiard RB, 1991). The presence of anxiety in people with major depression increases the risk of suicide attempts (Placidi GP et al., 2000; Scocco P. et al., 2000, Schaffer A. et al., 2000). Recognizing the coexistence of depression and anxiety is an important factor in determining the optimal treatment. However, until recently, clinical trial designs often excluded patients with comorbid conditions. This has led to the fact that in practice, the choice of drug for therapy in people with comorbid pathology continues to be very difficult, since it is based on data from studies of the spectrum of action of drugs in people with so-called “pure disorders”. It is this fact that makes the study of the effectiveness and safety of antidepressants, especially drugs of the latest generations, in patients with coexisting anxiety and depression undeniable relevance.
In the era of classic antidepressants, only 20–30% of patients with symptoms meeting DSM-IY criteria for major depression sought medical help. This was partly due to the perception among patients that available treatments for depression were “subjectively unpleasant” due to the development of side effects (Angst J., 1990). The need to reduce side effects and increase the effectiveness of therapy has led to the emergence of selective serotonin reuptake inhibitors (SSRIs), which have proven effective against both major depression, dysthymia, and most types of anxiety disorders. However, serotonin reuptake inhibitors turned out to be less effective than tricyclic antidepressants against severe forms of vital depression (Danish University Antidepressant Group, 1990, Anderson IM, 1998), which led to the search for chemical compounds with multiple but specific mechanisms of action. Clinical and experimental experience initiated the creation of the drug venlafaxine (velafax, manufactured by Pliva), which is a mixed norepinephrine and serotonin reuptake inhibitor, devoid of influence on other neurotransmitter systems. According to clinical studies, venlafaxine was not only more effective in relieving symptoms of moderate depression compared to imipramine (Lecrubier Y. et al., 1997), but also in relation to severe depressive symptoms compared to fluoxetine (Clerc GE et al., 1994 ). Velafax has shown its effectiveness in the treatment of depressive disorders of mild and moderate severity, including those with a pronounced anxiety component (Volel B.A., Romanov D.V., 2007). Among the latest generations of antidepressants, venlafaxine has demonstrated the best dose-response relationship, which is obviously due to the fact that in small therapeutic doses (75–125 mg) venlafaxine acts as a serotonin reuptake inhibitor with a simultaneous minimal effect of norepinephrine reuptake, but however, the norepinephrine effect increases when increasing doses to 150–375 mg. However, the side effect profile of venlafaxine is approximately equivalent to that of an SSRI.
The high efficacy and safety of venlafaxine have led to the fact that this drug is used as a standard or reference drug in many comparative studies. At the same time, in Russia, drugs whose active ingredient is venlafaxine (including the drug velafax, produced by the Pliva company) appeared only a few years ago, which gives research into their therapeutic characteristics undoubted interest and relevance.
STUDY PROCEDURE
A 12-week open-label post-marketing study aimed to investigate the effectiveness of velafax on depressive and anxiety symptoms, clinical global impression, and tolerability and safety in patients experiencing a “depressive episode” (F32), “recurrent depressive disorder” (F33) or “mixed anxiety and depressive disorder” (F41.2) according to ICD-10 criteria. In this case, a necessary condition for inclusion in the group of subjects was the severity of depressive symptoms corresponding to 20 points or more on the Hamilton Depression Scale (HAM-D21), and the level of anxiety in accordance with the Hamilton Anxiety Scale (HAM-A) had to be ≥ 20 points. Only those patients whose clinical severity score according to the CGI-S was ≥ 4 were included in the study.
The study design involved 4 visits (inclusion visit, third, sixth and 12th weeks of therapy). During the visits, the severity of depression was assessed using the 21 Item Hamilton Depression Rating Scale (HAM-D21) and the Montgomery Asberg Depression Rating Scale (MADRS), the severity of anxiety was assessed using the Hamilton Anxiety Rating Scale (HAM-A), as well as the determination of general clinical impressions using Clinical Global Impression Severity of Illness (CGI-S) and Improvement (CGI-I). Tolerability of the study drugs was assessed at the 3rd and 4th visits. The study did not include persons with established hypersensitivity to the study drug, alcohol abusers, moderate and severe forms of renal and liver failure, and uncompensated forms of diabetes mellitus. Exclusion criteria also included opioid use, pregnancy and lactation, the presence of comorbid psychotic diseases, the patient's current risk of suicide, and age under 18 years.
The optimal dose was selected individually in accordance with clinical data. The starting dose of velafax ranged from 75 to 150 mg per day, divided into two doses. Dosage increases of 37.5–75 mg were allowed every two to three days until response to therapy was achieved. The maximum daily dose was 375 mg. The study design allowed, if necessary, the use of benzodiazepine anxiolytics during the first three weeks of taking velafax, followed by a gradual reduction in dosage by the fourth week of use, as well as the use of benzodiazepines, imidazopyrine anxiolytics and hypnotics for sleep disorders throughout the study period.
Before the start of the study, written informed consent to participate in the study was obtained from patients.
Statistical processing of the obtained data was carried out using the Statistika 6.0 program (StatSoft, USA).
MATERIALS
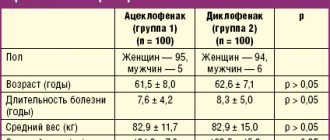
In a study conducted in the department of geriatric psychiatry of the St. Petersburg Psychoneurological Research Institute named after. V.M. Bekhterev, 30 patients were included (11 inpatient and 19 outpatient): 10 men and 20 women aged from 21 to 72 years. The average age of the patients was 54.1 ± 6.32 years. The condition of 6 patients included in the study group met the criteria for a depressive episode (F32), 25 patients suffered from recurrent depressive disorder (F33) ICD-10. The level of depressive symptoms at the time of inclusion in the study in patients was 25.54 ± 3.85 HAM-D21 points, 30.10 ± 6.70 MADRS points, which corresponds to a severe depressive episode. Our sample did not include persons with an established diagnosis of “mixed anxiety and depressive disorder,” however, the severity of anxiety measured by HAM-A was 21.06 ± 3.28 points, which is sufficient for diagnosing an anxiety state. The average severity of the disease was 4.32 ± 0.77 points on the CGI-S.
11 (33%) patients had confirmed concomitant somatic pathology, while out of 10 patients suffering from coronary heart disease and hypertension, 8 were constantly taking β-blockers, calcium channel blockers or antihypertensive drugs. Two patients included in the study had gastrointestinal pathology, but the patients' condition did not require concomitant therapy.
The initial dose of velafax in 12 patients was 75 mg, in 18 patients – 150 mg, the dosage was determined by the severity of depressive symptoms. The effective dose was maintained until the end of observation (12 weeks of therapy). The average dose of the drug at the end of the study was 256.9 ± 81.0 mg per day.
RESULTS
Of the 30 patients included in the study, 27 patients (90.0%) completely completed the 12-week course of taking Velafax. Two patients (10.0%) dropped out of the study during the first three weeks of taking the drug for the following reasons: 1 patient (3.2%) due to severe nausea with a good therapeutic response, 1 patient refused to continue participation due to an increase in blood pressure numbers and fears of developing decompensation of hypertension with increasing dosages. One (3.2%) patient was withdrawn from the study in the sixth week of taking velafax due to the ineffectiveness of high-dose therapy.
During the study, there were no reasons for adjusting the doses of drugs for the treatment of concomitant somatic pathologies; no signs of drug interactions or complications of the course of existing somatic diseases were identified. In 2 patients with gastrointestinal pathology (chronic gastritis), no adverse events were observed. Among the side effects noted during the period of taking velafax, 2 (6.4%) young male patients with a good therapeutic effect experienced moderate sexual dysfunction, which, however, did not lead to refusal to take therapy. Tolerability of the drug assessed at the third and fourth visits was defined as “good”, “very good” or “excellent” in all patients.
Five patients, upon inclusion in the study, were taking benzodiazepine tranquilizers or hypnotics due to severe sleep disorders, the need for which disappeared as their condition stabilized (end of the 3rd week of taking velafax).
Analysis of the data obtained during the study allows us to state a reduction in symptoms of depression and anxiety in patients included in the study. The results of statistical processing of data from the psychometric scales HAM-D21, HAM-A, MADRS are presented in Fig. 1 (parameters with significant differences are presented, p < 0.0001).
As follows from the data presented in Fig. 1, the level of anxiety and depression in patients included in the study, measured using the HAM-D21, HAM-A, MADRS scales, decreased, while significant differences in the severity of symptoms were observed between the first and second, second and third, third and fourth visits. all of the above scales. At the same time, by the 12th week of taking velafax, the average level of depression at the end of the study in our sample, the average score on HAM-D21 was 5.7 ± 3.45, on MADRS – 6.89 ± 4.80, which corresponds absence of depressive symptoms. It should be noted that the dynamics of Hamilton Depression Scale scores in our sample varied among patients of different age subgroups. Thus, in patients under 50 years of age, a rapid reduction in depressive symptoms was observed: 10 out of 12 patients (83%) in this age category could be classified as responders by the 3rd week of admission, since the level of depressive symptoms in accordance with HAMD decreased by more than 50 %. By the 12th week of taking Velafax, 93% of patients under 50 years of age achieved remission. At the same time, in patients over 50 years of age, a slower decrease in the severity of symptoms was noted; by the 6th week of treatment, only 65% of patients in this age subgroup could be classified as responders, but by the end of the study, 83% of patients over 50 had reached remission years.
Of particular interest is the dynamics of parameters identified as the so-called. “key factor” and “anxiety/somatization factor”, as well as a reflection of one’s own depressive and actual anxiety components of the depressive state. The dynamics of the parameters that make up the key factor are presented in Fig. 2.
As follows from the data presented in Fig. 2, the values of the parameters “depressive mood”, “feeling of guilt”, “impaired performance”, “lethargy” differed significantly between the inclusion visit and the 6th week of admission (second visit), significantly decreased between the 3rd and 6th, 6 1st and 12th weeks of therapy (first, second and third visits, respectively). The value of the “suicidal thoughts” variable significantly decreased between the inclusion visit and the 3rd week of taking velafax (first visit) and subsequently did not have any significant differences.
The dynamics of the parameters of the “anxiety/somatization” factor are presented in Fig. 3.
As follows from the data presented in Fig. 3, the level of mental and somatic anxiety, the severity of gastrointestinal and somatic symptoms differed significantly between the inclusion visit and the 3rd week of admission (first visit), 3rd and 6th, 6th and 12th weeks of administration of velafax (first , second and third visit respectively). Significant differences in the values of the parameter “hypochondria” and “attitude to the disease” were found between the third and sixth, sixth and twelfth weeks of taking Velafax.
In our sample of patients, a gradual decrease in the severity of the disease was observed, as evidenced by significant differences in the CGI-S scale indicators between the start of treatment and the third week of taking velafax, the third and sixth, sixth and twelfth weeks of taking velafax, while simultaneously changing the parameters of general improvement with the most pronounced significant changes in CGI-I scores between the 3rd and 6th weeks of admission (first and second visit, respectively).
THE DISCUSSION OF THE RESULTS
Treatment of patients with symptoms of depression and anxiety in the clinical picture continues to present significant difficulties, despite the significant arsenal of drugs currently available to the practitioner. Often in clinical practice, the effectiveness of antidepressants in relation to anxiety and depressive symptoms is lower than demonstrated by clinical studies, due to the fact that simple extrapolation of data obtained from studying the effectiveness and safety of drugs in patients with “pure conditions” introduces certain difficulties in the issues of choosing the optimal drug for the treatment of patients with comorbid depression and anxiety. That is why studies of the effectiveness and safety of antidepressant drugs, especially the latest generation of drugs, in this category of patients do not lose their relevance.
The purpose of our study was to study the therapeutic activity and tolerability of velafax in patients whose condition fell within the framework of a depressive episode or recurrent depressive disorder ICD-10. Our sample consisted of individuals whose severity of depressive symptoms at the time of inclusion in the study, assessed using the 21 Item Hamilton Depression Rating Scale (HAM-D21) and Montgomery Asberg Depression Rating Scale (MADRS), met the criteria for a major depressive episode. At the same time, the severity of anxiety, assessed by the Hamilton Anxiety Rating Scale (HAM-A), was sufficient to diagnose an anxiety state, which allows us to classify the patients included in our sample as individuals with comorbid depression and anxiety.
Our data allows us to state the fact that velafax is sufficiently effective not only in relation to depressive symptoms themselves, but also anxiety coexisting with depression, as evidenced by changes in the parameters of psychometric scales assessing the severity of anxiety. Noteworthy is the synchronicity and harmony of the decrease in the level of depressive and anxiety symptoms when taking Velafax in patients in our sample. The dynamics of the indicators of the psychometric scales we used indicate the presence of a significant difference in the level of severity of anxiety and depression already by the third week of taking velafax compared to the beginning of the study, which indicates the rapidity of the onset of the therapeutic effect.
It is worth noting some features of the effect of velafax on psychopathological symptoms in different age groups. Thus, the number of responders among young patients by the third week of taking the drug was more than 80%, which is consistent with the data available in the literature on the high rate of onset of the effect of velafax (Volel B.A., Romanov D.V., 2007). At the same time, in patients over 50 years of age, the therapeutic effect occurred more slowly; only by the 6th week of treatment the number of responders was about 65%. At the same time, by the time the study was completed, the average level of severity of depressive symptoms and anxiety in our sample corresponded to the state of remission in both age subgroups. This kind of dynamics of the onset of a therapeutic effect is not unexpected, since it is characteristic of elderly patients, especially when using selective serotonin reuptake inhibitors and tianeptine, and to a lesser extent amitriptyline (Andrusenko M.P., 2003).
At the same time, it should be emphasized that the significant degree of severity of psychopathological symptoms led to relatively high average effective dosages of the drug; more than 50% of patients received maximum or submaximal doses of velafax, while in all patients who completely completed the study, tolerability was characterized as “good”, “very good” and “excellent”. The low percentage of patients who dropped out of the study indicates the high effectiveness and good tolerability of velafax.
Thus, the results of our study showed the high therapeutic efficacy of velafax against severe depression and anxiety, which, along with a favorable tolerability profile and a high level of safety, may serve as a basis for the use of velafax in patients with comorbid anxiety and depressive disorders.
Bibliography
1. Andrusenko M.P. Features of the development of the therapeutic effect of antidepressants in late age // Psychiatry. 2003; 1:46–51. 2. Volel B.A., Romanov D.V. Experience of using venlafaxine (velafax) in patients in outpatient and clinical practice // Therapy of mental disorders. 2007; 2:48–52. 3. Anderson IM SSRIs versus tricyclic antidepressants in depressed inpatients: a meta-analysis of efficacy and tolerability // Depress Anxiety. 1998; 7: 11–18. 4. Angst J. Natural History and epidemiology of depression. In: Gobb J., Goeting N., eds. Current approaches, Southampton: Duphar Medical Relations, 1990; 1–11. 5. Bradley N., Rush J., Trivedi M., Wisniewski S., Balasubramani GK, Spencer D., Petersen T., Klinkman M., Warden D., Nicholas L., Fava M. Major Depression Symptoms in Primary Care and Psychiatric Care Settings: A Cross-Sectional Analysis // Ann Fam Med. 2007; 5: (2: 126–134. 6. Clerc GE, Ruimy P., Verdeau-Pailles. And on behalf of the Venlafaxine French Inpatient Study Group. A double-blind comparison of venlafaxine and fluoxetine in patients hospitalized for major depression and melancholia // Int. Clin. Psychopharmacol. 1994; 9: 139–143. 7. Danish University Antidepressant Group. Paroxetine: a selective serotonin reuptake inhibitor showing better tolerance, but weaker antidepressant effect than clomipramine in controlled multicenter study // J. Affective Disorders 1990; 18: 289–299 8. Kessler, RC, Blazer, DG, McGonagle, KA The prevalence and distribution of major depression in a national community sample: the National Comorbidity Survey // American Journal of Psychiatry. 1994; 151; 979–986. 9. Lecrubier Y, Bourin M., Moon C. Efficacy of venlafaxine in depressive illness in general practice // Acta Psychiatr. Scand. 1997; 95: 485–493. 10. Liebowitz MR Depression with anxiety and atypical depression // J. Clin. Psychiatry. 1993; 54: Suppl. 2: 10–14. 11. Lyddiard RB Co-exiting depression and anxiety: special diagnostic and treatment issues // J. Clin. Psychiatry. 1991; 52: Suppl. 6:48–54. 12. Placidi GP, Oquendo MA, Malone KM Anxiety in major depression: relationship to suicide attempts // Am. J. Psychiatry. 2000; 157:1614–1622. 13. Scocco P., Marietta P., Tonietto M. The role of psychopathology and suicidal intention in predicting suicide risk: a longitudinal study // Psychopathol. 2000; 33: 143–150. 14. Schaffer A., Levitt AJ, Bagby RM, Suicidal ideation in major depression: sex differences and impact of comorbid anxiety // Can. J. Psychiatry. 2000; 45:822–828. 15. Zimmerman M., McDermut W., Mattia JI Frequency of anxiety disorders in psychiatric outpatients with major depressive disorder (Brief report) // Am. J. Psychiatry. 2000; 157:1337–1340. 16. Zing WW, Magruder-Habib K., Velez R. The comorbidity of anxiety and depression in general medical outpatients: a longitudinal study // J. Clin. Psychiatry. 1990; 51: Suppl. 6:77–80.
Venlafaxine
Use during pregnancy and breastfeeding
Venlafaxine should not be prescribed to pregnant and breastfeeding women, because
The safety of the drug during pregnancy and lactation in women has not been sufficiently established, due to the fact that there are no adequately controlled clinical studies on a sufficiently large sample of such patients. This concerns the health of both the mother and, to a greater extent, the fetus/child. Women of childbearing age should be warned about this before starting treatment and should immediately consult a doctor if they become pregnant or plan to become pregnant during treatment with the drug. Venlafaxine and its metabolite (EFV) are excreted into breast milk. If it is necessary to take the drug during lactation, breastfeeding must be stopped.
In practice, there are cases of prescribing venlafaxine to mothers during pregnancy and shortly before childbirth, when in a particular situation the expected benefit to the mother outweighs the potential risk to the fetus. In these cases, newborns often experienced complications that required: increased hospitalization, maintenance of breathing and tube feeding. These complications can develop immediately after childbirth and are also typical when taking other antidepressants from the SNRI group or SSRIs (not containing venlafaxine). In such cases, the following clinical symptoms in newborns have been reported: respiratory disorders, cyanosis, apnea, convulsions, temperature instability, feeding difficulties, vomiting, hypoglycemia, muscle hypertension or hypotonia, hyperreflexia, tremor, trembling, irritability, lethargy, constant crying, drowsiness or insomnia. Such disturbances may indicate the serotonergic effects of the drug Venlafaxine.
If venlafaxine was used during pregnancy and maternal treatment was completed shortly before delivery, the newborn may experience withdrawal symptoms. In such a newborn, the presence of serotonin syndrome or neuroleptic malignant syndrome should be excluded. Epidemiological evidence suggests that use of SSRIs during pregnancy, especially late in pregnancy, may increase the risk of persistent neonatal pulmonary hypertension.
special instructions
Suicide and suicidal behavior
Depression is associated with an increased risk of suicidal ideation, self-harm, and suicide (suicidal behavior). This risk persists until significant remission occurs. Since improvement may not be observed during the first few weeks of therapy or even longer, patients should be closely monitored until such improvement occurs. Based on accumulated clinical experience, the risk of suicide may increase in the early stages of recovery.
Patients with a history of suicide attempts or high levels of suicidal ideation prior to treatment are at greater risk for suicidal ideation or suicide attempts and should be closely monitored. A meta-analysis of placebo-controlled clinical trials of antidepressants in adult patients with mental disorders found that antidepressants were at increased risk of suicidal behavior compared with placebo in patients under 25 years of age. Drug treatment of these patients, and in particular those at high risk of suicide, should be accompanied by careful monitoring, especially early in therapy and during dose adjustment. Patients (and caregivers of such patients) should be warned to monitor for any signs of clinical worsening, suicidal behavior or ideation, or unusual changes in behavior, and to seek immediate medical attention if these symptoms occur.
In a small number of patients taking antidepressants, incl. venlafaxine, aggression may occur during initiation of treatment, dose changes, or discontinuation of treatment.
Clinical studies conducted to date have not revealed tolerance or dependence to venlafaxine. Despite this, as with other drugs that act on the central nervous system, the physician should closely monitor patients for signs of drug abuse, as well as patients with a history of such symptoms.
Special patient groups
Venlafaxine is not approved for use in children.
In patients with a history of aggression, venlafaxine should be used with caution.
In patients with affective disorders, bipolar disorder when treated with antidepressants, incl. venlafaxine, hypomanic and manic states may occur. Like other antidepressants, venlafaxine should be used with caution in patients with a history of mania. Such patients require medical supervision.
Convulsive disorders may occur during therapy with venlafaxine. As with all antidepressants, venlafaxine should be used with caution in patients with a history of seizure disorders and such patients should be closely monitored. Treatment should be discontinued if seizures develop.
Akathisia
The use of venlafaxine has been associated with the development of akathisia, which is characterized by an unpleasant feeling of internal motor restlessness for the patient and manifested in the patient’s inability to sit quietly in one position for a long time or remain motionless for a long time. This condition may occur at the beginning of treatment and during the first weeks of treatment. In patients who develop such symptoms, increasing the dose is not recommended.
Bipolar disorder
Before starting treatment, it is necessary to identify those patients who are at risk for bipolar disorder. Such a check should include a detailed examination of the medical history, incl. family, to identify cases of suicide, bipolar disorder. It should be noted that venlafaxine is not recommended for use in the treatment of bipolar depression.
Use in patients with concomitant diseases
Clinical experience with the use of venlafaxine in patients with concomitant diseases is limited.
It should be used with caution in patients with diseases in which the effect of venlafaxine on hemodynamic parameters and/or metabolism may be significant.
Patients should be warned to immediately consult a doctor if a rash, urticaria or other allergic reactions occur.
Some patients while taking venlafaxine experienced a dose-dependent increase in blood pressure and/or an increase in heart rate, so regular monitoring of blood pressure and ECG is recommended, especially during the period of adjusting or increasing the dosage of venlafaxine. In post-marketing experience with venlafaxine (overdose), fatal cardiac arrhythmias have been reported. Before prescribing venlafaxine to patients at high risk of developing serious cardiac arrhythmias, the ratio of the likely benefit to the possible risk of use should be assessed.
Patients, especially the elderly, should be warned about the possibility of dizziness and impaired balance in order to prevent injury.
While taking venlafaxine, especially in conditions of dehydration or decreased blood volume (including in elderly patients and patients taking diuretics), hyponatremia and/or syndrome of insufficient secretion of antidiuretic hormone may occur.
Venlafaxine has not been studied in patients with recent myocardial infarction and decompensated heart failure. The drug should be prescribed to such patients with caution.
Taking SSRIs or venlafaxine in patients with diabetes may cause changes in plasma glucose levels. Dosage adjustments of insulin and/or antidiabetic medications may be required.
During treatment, it is recommended to refrain from drinking any alcohol-containing drinks.
The safety and effectiveness of venlafaxine in combination with weight loss medications (including phentermine) have not been established. The simultaneous use of venlafaxine and drugs that reduce body weight is not recommended.
Women of childbearing potential should use appropriate contraception while taking venlafaxine.
Explanations of special symptoms and conditions that may occur during treatment with the drug
Dry mouth occurs in 10% of patients receiving venlafaxine. This may increase your risk of developing tooth decay. Patients should practice good oral hygiene.
The use of venlafaxine may cause the development of akathisia, characterized by subjective discomfort or restlessness and the need to move frequently, often accompanied by an inability to sit or stand still. This mostly occurs during the first few weeks of treatment. Increasing the dose in patients who develop these symptoms may cause undesirable effects.
In placebo-controlled clinical trials, a clinically significant increase in serum cholesterol was reported in 5.3% of patients. Cholesterol level control is necessary during long-term treatment.
Withdrawal syndrome
When stopping treatment, withdrawal symptoms are common, especially if it is stopped abruptly. The risk of withdrawal syndrome may depend on several factors, including the duration of treatment, the size of therapeutic doses and the rate of dose reduction. These symptoms are very rarely reported in patients who accidentally missed taking the drug.
Withdrawal symptoms usually occur within the first few days after stopping treatment. These symptoms usually go away within 2 weeks, although in some people they may last 2-3 months or more. It is recommended to gradually reduce the dose of venlafaxine when stopping the drug - over several weeks or months, depending on the severity of the clinical symptoms of the disease.
Serotonin syndrome
Taking venlafaxine, like other serotonergic drugs, can cause serotonin syndrome, a potentially life-threatening condition, especially when used concomitantly with other drugs that can affect the serotonergic neurotransmitter systems such as MAO inhibitors.
Symptoms of serotonin syndrome may include mental status changes (agitation, hallucinations, coma), autonomic instability (tachycardia, blood pressure lability, hyperthermia), neuromuscular disorders (hyperreflexia, incoordination), and/or gastrointestinal symptoms (nausea, vomiting). , diarrhea).
Impact on the ability to drive vehicles and operate machinery
During the treatment period, care should be taken when performing potentially hazardous types of work that require increased concentration and speed of psychomotor reaction (including driving a car and operating machinery).
Material and methods
We examined 32 patients, 15 women and 17 men, aged from 18 to 57 years (average age 31.75 years) with endogenous depression, who were undergoing inpatient treatment in the clinical departments of the department for the study of endogenous mental disorders and affective states of the Federal State Budgetary Institution "Research Center for Mental Health" » RAS.
The design of the study was open naturalistic. The average duration of the disease from its first manifestation was 7.9 years, the average number of depressive episodes suffered before inclusion in the study was 3.3. The duration of the current depressive episode before starting Velaxin was on average 4.5 months.
According to nosological affiliation, the patients were distributed as follows: 22 (68.6%) patients were diagnosed with endogenous affective diseases - manic-depressive psychosis (MDP), cyclothymia; in 5 (15.6%) depression developed in the dynamics of low-progressive schizophrenia, and in 5 (15.6%) postpsychotic depression was noted in the context of paroxysmal schizophrenia. According to ICD-10, the depressive state of patients was diagnosed according to the following categories: F31.3—F31.4; F32.0—F32.2; F33.0—F33.2; F21; F20.4. Typologically, depressive states were defined as melancholy (3 patients, 9.4%), anxious (11 cases; 34.4%) and apatho-adynamic (18 patients; 56.2%). Thus, in accordance with the two-level psychopathological model of depression [24], its first 2 types were defined as typical, representing positive affectivity (sad and anxious depression), apatho-adynamic depression as atypical and related to negative affectivity.
According to the total scores on the Hamilton Depression Scale (HAM-D) before treatment: mild depressive disorders were registered in only 2 (6.25%) people, moderate in 13 (40.6%), severe depression in 17 (53.15%), i.e., the vast majority of patients had moderate to severe depression.
The study used venlafaxine, marketed as Velaxin 75 mg tablets (Hungary). The drug was prescribed orally, starting from 37.5-75 mg per day. Subsequently, based on the condition of the patients, over the next few days the daily dose was increased, reaching the maximum for a given patient, but not more than 300 mg. On average, the highest mean dose of Velaxin used was 182.1–198.2 mg per day. The drug was taken twice, morning and evening. According to the study protocol, the course of Velaxin therapy was 56 days (8 weeks).
To assess the severity of depressive symptoms and determine the therapeutic effect, in addition to the clinical observation method, the HAM-D-24 scale, containing 24 signs, was used. The severity of depressive symptoms was assessed before the start of the course of treatment (day 0), then on days 1, 3, 5 of therapy and then at the end of each of the 8 weeks of course treatment. The effectiveness of the antidepressant effect of velaxin was assessed by the degree of reduction in HAM-D scores in % relative to the score before treatment in the following gradations: reduction in scores up to 20% - as “insignificant”, by 21-50% - as “moderate”, by 51- 80% - as “good” and 81-100% - as a “significant” effect (including “practical recovery”). A decrease in the total HAM-D score to 6 or less meant complete “entry” into remission. Maintaining the HAM-D depression severity score at the same level or increasing the total score was regarded as no effect or “worsening” of the condition. To assess the spectrum of antidepressant action of Velaxin, the degree of reduction in the average total score of individual signs identified in the HAM-D was determined, conditionally characterizing melancholic or sad (items 1-3, 22-24), apatho-adynamic (items 7 and and anxious (items 9 and 10) manifestations in the structure of the depressive state.
The severity of depressive symptoms was assessed before the start of the course of treatment (day 0), then on days 1, 3, 5 of therapy and then at the end of each of the 8 weeks of course treatment. The effectiveness of the antidepressant effect of velaxin was assessed by the degree of reduction in HAM-D scores in % relative to the score before treatment in the following gradations: reduction in scores up to 20% - as “insignificant”, by 21-50% - as “moderate”, by 51- 80% - as “good” and 81-100% - as a “significant” effect (including “practical recovery”). A decrease in the total HAM-D score to 6 or less meant complete “entry” into remission. Maintaining the HAM-D depression severity score at the same level or increasing the total score was regarded as no effect or “worsening” of the condition. To assess the spectrum of antidepressant action of Velaxin, the degree of reduction in the average total score of individual signs identified in the HAM-D was determined, conditionally characterizing melancholic or sad (items 1-3, 22-24), apatho-adynamic (items 7 and and anxious (items 9 and 10) manifestations in the structure of the depressive state.
In addition, at the above periods, the severity of the depressive state and the degree of its improvement over time were assessed using the CGI Clinical Global Impression scale and its subscales CGI-S and CGI-I. To record side effects, the UKU interview scale was used, which consists of 4 subscales that allow us to distinguish mental, neurological, autonomic and so-called other side effects.
results
During the prescribed 56-day course of treatment with Velaxin, 31 (96.9%) people were recognized as responders, of which a “minor” effect of treatment was observed in 1 (3.1%) patient, a “moderate” effect in 3 (9.4 %), “good” - in 2 (6.25%), and 25 (78.1%) patients showed a “significant” therapeutic effect. Thus, a decrease in the intensity of depressive disorders by 50% or more during treatment with Velaxin was found in the vast majority of cases - in 27 (84.4%) patients, as shown in Fig. 1.
Rice. 1. The degree of severity of the therapeutic effect of Velaxin for endogenous depression. The x-axis is the degree of reduction according to HAM-D,%; The y-axis is % of patients.
In general, the effectiveness of Velaxin, assessed on the 56th day of therapy, was quite high: the average total score of depression severity according to HAM-D was reduced by 85.9%. By the end of the 1st week of treatment with Velaxin, a positive therapeutic response to the drug was observed: the reduction in depression was at the level of a “minor” effect, but was approaching a 20% reduction in disorders, bordering on a “moderate” improvement. A clear “moderate” improvement (reduction in HAM-D score by 33.2%) was observed by the 14th day of treatment; between the 21st and 28th days of treatment, the therapeutic effect reached the “good” range with a decrease in HAM-D scores by 50% or more, and by the 6th week the effect of Velaxin treatment was already approaching the “significant” border (up to 76.7% reduction in the severity of depressive symptoms). In the subsequent 7-8 weeks of therapy, an undeniable “significant” improvement in the patients’ condition was detected (reduction of disorders by more than 80%), up to “recovery” (Fig. 2). In 20 out of 31 patients (64.5% of cases) who completed the course of treatment with Velaxin, depression was completely reduced and “entry” into remission was observed (their total HAM-D score became 6 or lower).
Rice. 2. The spectrum of therapeutic action of velaxin for endogenous depression (HAM-D score). Here and in Figs 3, 4 and 5 (in the last one - the right axis): on the ordinate - the average score as a percentage of the score before the start of therapy, on the x-axis - the day of therapy.
The severity of the condition, assessed by the CGI-S subscale, on average decreased during treatment with Velaxin from 4.7 to 1.6 points at the end of the study (from “significantly expressed” to less than “mildly expressed”, i.e., to the virtual absence of distress ). Moreover, a noticeable decrease in the severity of symptoms was noted in the period between the 7th and 21st days of treatment, when the intensity of the manifestations of depression consistently decreased on average to “moderately” and “weakly” expressed. From the 5th week of therapy, the severity of depressive disorders became “very weak”, and at the 7-8th week of course therapy there was a practical “exit” from depression with the “absence” of depressive symptoms (their average level of severity was 1.6 points). During the 56-day course of therapy, assessment of the degree of improvement in the depressive state on the CGI-I subscale showed a “deterioration” of the mental state (5th assessment level) in only 1 (3.1%) person, remained “unchanged” (4th assessment level) also in 1 (3.1%) patient, “minor improvement” (3rd level) - also in 1 (3.1%), “pronounced” improvement (2nd level) was observed in 4 (12 .6%), the remaining 25 (78.1%) patients showed a “significant” improvement (grade 1).
It was found that in the spectrum of antidepressant action of Velaxin, all 3 components of its psychotropic activity, in accordance with the final results of treatment, are presented to almost the same extent with a slight advantage in terms of anti-depressive action (see Fig. 2). Thus, the degree of reduction in the average total score of disorders on items 1-3 and 22-24 of HAM-D (reflecting the actual thymoleptic effect of the drug) was 88.2%, on items 7 and 8 (stimulating effect) - 83.7%, and on points 9 and 10 (anti-anxiety effect) - 85.1%. However, the implementation of all 3 components of the action of Velaxin over time was different and had its own characteristics. Thus, thymoleptic and especially anxiolytic effects were detected most quickly during treatment. They developed almost in parallel, reaching a level of reduction in the severity of disorders according to HAM-D by 32.8 and 37.1%, respectively, by the 14th day of therapy (“moderate” effect). At the same time, the stimulating effect of Velaxin was somewhat “lagged” compared to the anti-anxiety and anti-sadness effects, reaching similar values (“moderate” effect - reduction of disorders by 36.9%) only by the 21st day of the study.
Subsequently, in the period from the 21st to the 28th days of treatment, the thymoleptic and anti-anxiety components of the action in the spectrum of antidepressant activity of Velaxin leveled off and increased in rate of development to the range of a clear “good” effect (score reduction by 60.2 and 59. 2%). But already from the 5th week of treatment, the thymoleptic effect itself began to surpass the anxiolytic one in terms of the depth of reduction of disorders according to the corresponding HAM-D items: the thymoleptic effect appeared at the “significant” level already at the 6th week, and the anti-anxiety effect only after the 7th week course therapy. The formation of the stimulating effect was “lagged” in the degree of manifestation compared to the other two components of the action of Velaxin at 1 week, and its “significant” severity was determined only at the 8th week of treatment. And only at this stage of treatment, as already mentioned, the depth of the stimulating effect of Velaxin approximately coincided with the severity of the thymoleptic and anxiolytic effects.
In accordance with established data on the peculiarities of the implementation of individual components of antidepressant action in the spectrum of psychotropic activity of velaxin, its therapeutic effectiveness was analyzed depending on the syndromic type of depression, i.e., on the dominant affect that determines the picture of the depressive state (Fig. 3). It was found that with leading anxious affect, the reduction in the average total score on HAM-D was 85.5% by the 56th day of treatment; with a predominance of apatho-adynamic affect, the effectiveness of Velaxin was similar - the average total score on HAM-D decreased by 85.9%. The highest effectiveness of Velaxin was observed in the treatment of patients with a leading sad affect in the picture of depression - the reduction in the average total score on HAM-D was 91.1%. But with a relatively similar degree of reduction in depressive symptoms, differences were also noted in the dynamics of the implementation of the antidepressant effect of the drug. Thus, with leading anxious and melancholy affects, i.e. in patients with positive affectivity and the most typical manifestations of depression, the reduction of depressive symptoms proceeded at an equal pace, reaching 21.1% (with anxious depression) and 22.5% (with melancholy depression) already by the 7th day of therapy. Subsequently, the decrease in the average total score on HAM-D occurred more intensively and reached more than 50% reduction in depressive symptoms by the 28th day of treatment. When treating patients with negative affectivity (atypical apatho-adynamic depression) with Velaxin, improvement occurred more slowly. A reduction in the average total HAM-D score by 20% or more (“moderate” effect) occurred only in the 2-3rd week of therapy; and only by the 4th week a “good” effect of Velaxin was recorded (reduction of disorders by 61.3%). By the 7-8th week of treatment, the improvement in the condition was already “significant” (more than 80% reduction in disorders), it coincided in severity with the therapeutic effect of Velaxin for anxious depression and was somewhat “lag behind” the effect for melancholy depression.
Rice. 3. Dynamics of the effectiveness of Velaxin for different types of endogenous depression (HAM-D score).
Analysis of the effectiveness of Velaxin depending on the nosological affiliation of depression also revealed some features (Fig. 4): the lowest rate of decrease in the average total score on HAM-D by the end of the course of treatment was in patients with low-progressive schizophrenia, it was equal to 82.3%. These same patients also had the slowest rate of reduction in depressive disorders - by the 7th day it was only 15.2%, and a reduction of 50% or more (the limit of a “good” effect) was achieved only by the 28th day; A “significant” effect was detected in patients with low-progressive schizophrenia only after the 7th week of treatment with Velaxin. In patients with affective illness (MDP, cyclothymia), the reduction in the average total score on HAM-D at the end of course therapy was close in value (86.6%), and the rate of reduction in depressive symptoms was similar: by the 7th day this figure reached 18 .2%, and by the 4th week of therapy it was already 59.4% (“good” effect). The best treatment result was achieved in patients with postpsychotic depression and paroxysmal schizophrenia - 90.4% reduction in disorders on the 56th day of treatment. Despite the fact that by the end of the 1st week of the study, the rate of reduction in depressive symptoms reached gradations of “insignificant” improvement (19.2%), subsequently the reduction in depressive symptoms occurred more intensively than with MDP, demonstrating a “good” effect already at 14 days. 1st day of treatment (symptom reduction rate -53.9%), and by the 28th day it was already 76.5%, i.e. it was almost on the border of “significant”. However, it should be noted that in these patients the initial severity of depressive disorders was significantly lower, at the level of “moderate” severity, than in other, more “severe” depressions (23 points on HAM-D versus 31.3 points for affective illness and 31.6 for low-progressive schizophrenia).
Rice. 4. Antidepressant effect of Velaxin in different nosological groups of patients (HAM-D score).
All of the indicated patterns of development of the therapeutic effect of Velaxin indicate the absence of a direct dependence on the size of its daily dose. As can be seen from Fig. 5, the therapeutic effect began to appear and increase from the 3-4th week of treatment (reduction of depressive symptoms by 50% or more according to HAM-D), with an increase in the average daily dose to the maximum (182.1-198.2 mg per day) . But subsequently, despite stabilization and even a slight decrease in the achieved maximum average daily dose of Velaxin (up to 190.3 mg per day), the response to therapy continued to increase at a faster pace, to the level of “significant” improvement,
Rice. 5. The relationship between the therapeutic effect (HAM-D score) and the daily dose of Velaxin. On the left ordinate is the average daily dose of the drug (mg).
During the course of Velaxin therapy, 45 adverse events of various types were registered in 21 (65.6%) patients; in 5 they were single, and in 16 they were combined. The most common were mental and autonomic adverse events noted on the UKU scale; they occurred in 40% of patients. One patient withdrew from the study early (after 2 weeks of treatment) due to the development of acute affective-delusional psychosis, requiring a change in therapy. Neurological and other side effects occurred in only 8.9 and 11.1% of patients. The most common individual side effects observed were “excitement/anxiety” (in 15.5% of patients), decreased sleep duration and nausea (in 11.1%), tachycardia and hyperhidrosis (in 6.6%), sedation and constipation (in 4.4%). All other side effects occurred in isolated cases. The incidence of side effects during a course of treatment with Velaxin was highest in the 2nd week of treatment, when the average daily dose of the drug was insignificant (157.7 mg per day). The most common adverse events during this period were psychiatric and autonomic adverse events. But subsequently, despite increasing the average daily dose, the incidence of side effects gradually decreased. The exception was “other” side effects, the frequency of which practically remained at the same level until the end of treatment. These were mainly sexual dysfunctions, which developed according to an increase in the daily dose of Velaxin.
It should be noted that, in general, all adverse events were mild or approaching moderate severity in the first 2 weeks of treatment, and then their average severity as assessed by UKU decreased to a “mild” level, despite a gradual increase in the average daily doses of Velaxin. At the same time, mental side effects were initially the most severe: the average UKU severity score at 1–2 weeks of treatment was 1.9–2.0. However, during the further course of treatment, the severity of adverse mental symptoms decreased from the 3rd week. The severity of some other adverse events increased slightly compared to the initial one: if on the 2nd week of treatment their severity on average corresponded to the UKU “mild” degree (1 point), then later they reached 1.5 points, and at the same time their degree severity increased according to an increase in the average dose of Velaxin.
Velaxin®
Depression increases the risk of suicidal thoughts and suicide attempts. This risk persists until stable remission occurs. Therefore, patients should be under constant medical supervision and should be given only small quantities of the drug capsules to reduce the risk of possible abuse and/or overdose. Velaxin® should not be used in the treatment of children and adolescents under 18 years of age. An increase in the likelihood of suicidal behavior (suicide attempt and suicidal ideation), as well as hostility, was observed more often in clinical trials among children and adolescents receiving antidepressants compared with groups receiving placebo.
Aggressive behavior has been reported while taking venlafaxine (especially at the beginning of treatment and after discontinuation of the drug).
The use of venlafaxine may cause psychomotor restlessness, which clinically resembles akathisia, characterized by restlessness with a need to move, often combined with an inability to sit or stand still. This is most often observed during the first few weeks of treatment. If these symptoms occur, increasing the dose may have an adverse effect and the advisability of continuing to take the drug should be considered.
Like all antidepressants, venlafaxine should be prescribed with caution to patients with a history of mania and/or hypomania, as the drug may cause an increase in their symptoms. In these cases, medical supervision is necessary.
Caution should be exercised when treating patients with a history of seizures. If convulsive seizures occur or their frequency increases, treatment with venlafaxine should be interrupted.
Like selective serotonin reuptake inhibitors, venlafaxine should be used with caution when used concomitantly with antipsychotic drugs, as symptoms resembling neuroleptic malignant syndrome may develop.
Patients should be warned to seek immediate medical attention if rash, hives, or other allergic reactions occur.
Some patients experienced a dose-dependent increase in blood pressure while taking venlafaxine, and therefore regular monitoring of blood pressure is recommended, especially at the beginning of treatment or when increasing the dose.
Isolated cases of orthostatic hypotension have been described while taking venlafaxine. Patients, especially the elderly, should be warned about the possibility of dizziness and impaired balance.
Venlafaxine may cause an increase in heart rate, especially at high doses. Particular caution should be exercised when prescribing the drug to patients with conditions that may be aggravated by an increase in heart rate.
There are insufficient studies of the use of venlafaxine in patients who have recently suffered a myocardial infarction or suffering from decompensated heart failure, so this drug should be used with caution in these patients.
Like other serotonin reuptake inhibitors, venlafaxine may increase the risk of bleeding into the skin and mucous membranes, so caution is required when treating patients predisposed to bleeding.
Hyponatremia and/or syndrome of insufficient antidiuretic hormone secretion (SIADH) may occur while taking venlafaxine, especially in conditions of dehydration or decreased blood volume (including in elderly patients and patients taking diuretics).
Cases of mydriasis have been reported while taking venlafaxine, so patients with a predisposition to increased intraocular pressure or those at risk of angle-closure glaucoma require careful medical monitoring.
In case of renal and liver failure, special caution is required. In some cases, a dose reduction is required (see section "Method of administration and dosage").
The safety and effectiveness of using venlafaxine with weight-loss drugs, including phentermine, have not been established, so their simultaneous use (as well as the use of venlafaxine as monotherapy for weight loss) is not recommended. Clinically significant increases in serum cholesterol levels have been observed in some patients receiving venlafaxine for at least 4 months. Therefore, when taking the drug for a long time, it is advisable to monitor serum cholesterol levels.
After stopping the drug, especially abruptly, withdrawal symptoms often occur (see section “Side effects”). The risk of withdrawal symptoms may depend on several factors, including course length and dose, and the rate of dose reduction.
Withdrawal symptoms such as: dizziness, sensory disturbances (including paresthesia and electrical sensations), sleep disturbances (including insomnia and unusual dreams), agitation or anxiety, nausea and/or vomiting, tremor, sweating, headache, diarrhea, rapid and increased heart rate, and emotional instability are usually mild to moderate in severity, but may be severe in some patients. They are usually observed in the first days after discontinuation of the drug, although there have been isolated reports of such symptoms in patients who accidentally missed a dose. Usually these phenomena resolve on their own within 2 weeks; however, in some patients they may be longer lasting (2-3 months or more). Therefore, before discontinuing venlafaxine, it is recommended to gradually reduce its dose over several weeks or months, depending on the patient's condition (see sections "Dosage and Administration").