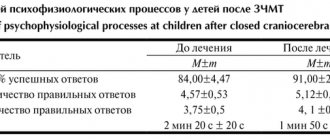
In 1912, a special hereditary pathology was described simultaneously in our country and abroad, which received its name from the authors - Wilson-Konovalov disease. This is a hereditary disease and it is dangerous. Let's find out with an expert whether it can be cured.
ALENA PARETSKAYA
Pathophysiologist, immunologist, member of the St. Petersburg Society of Pathophysiologists VALENTINA KUZMINA Candidate of Medical Sciences, neurologist at SM-Clinic
One of the most characteristic signs of the disease is the pathological accumulation of copper in the area of various organs, tissue damage, especially – liver, nervous system problems, changes in the iris of the eye.
What is Wilson-Konovalov disease
The term Wilson-Konovalov disease refers to a hereditary pathology.
It occurs when parents pass on a defective gene (ATP7B) to their child. The condition is an autosomal recessive pathology, that is, it occurs if each of the parents carries a similar gene in their cells and the child inherits both genes at once - from the mother and from the father. This defective gene gives instructions for the synthesis of a protein that regulates the exchange and transport of copper within the body. When it is defective, copper accumulates in the liver, concentrates in the nerve ganglia, and is deposited in the iris of the eye. The pathology is rare and is sometimes very difficult to recognize, especially if there are no similar patients in the family.
Causes of Wilson-Konovalov disease in adults
The key process in this pathology is the inheritance of a defective gene from parents.
It is located on chromosome 13 and regulates copper metabolism. On average, the body of adults contains approximately 50 - 70 mg of copper and per day it needs no more than 2 mg of the element, which comes from food.
The vast majority of the microelement (95%) is transported in close association with the plasma protein – ceruloplasmin. It is constantly produced by the liver, and only about 5% of copper is transported along with albumin.
Copper is needed to participate in metabolic processes, including oxidative ones. If Wilson's disease develops, its elimination is impaired, the concentration in the plasma increases, and from there it spreads to the tissues. The main accumulation of copper occurs in the brain, in the iris, inside the liver, and also in the kidneys. Excess microelement has a toxic effect.
Introduction
Wilson–Konovalov disease (WKD), or hepatolenticular degeneration, is a monogenic hereditary disease, transmitted in an autosomal recessive manner, which is based on a disorder of copper metabolism, leading to its excessive accumulation in the liver, brain, kidneys and cornea, less commonly in others organs, with reduced excretion of copper with bile [1].
The disease is progressive and is accompanied by a decrease in quality and life expectancy. VWD was first described by K. Wilson in 1912 and was designated as a disease with an unconditional fatal outcome. Over the past 100 years, the pathogenetic mechanisms of the disease have been discovered, and treatment methods have been developed that can extend the life of patients with BVC for decades. BVD is a rare disease. Its prevalence, according to Orphanet, is 1–9 cases per 100 thousand population (on average 1 per 25 thousand), the annual frequency of detection of new cases is from 1 per 30 thousand to 1 per 100 thousand population. According to rough estimates, every 90–100th (1%) person is a carrier of a defective heterozygous gene [2]. Clinical manifestation of the disease usually occurs at an early age. In some cases, the onset of BVK is observed at a later age – after 50 years.
Etiology and pathogenesis
The cause of BVD is mutations in the ATP7B gene, which encodes a P-type copper-transporting ATPase [3]. The gene is located on chromosome 13 in region 13q14.3. More than 700 different ATP7B mutations are known [4]. ATPase 7A and ATPase 7B are enzymes that transport copper in the body. ATPase 7A is found in enterocytes and the choroid plexus of the brain; it is involved in the absorption of copper in the intestine and its penetration into the brain. ATPase 7B is present in hepatocytes and brain capillaries [5], it transports copper ions from cells and is involved in the formation of functionally active ceruloplasmin from apoceruloplasmin, which is then released into the blood [6]. ATPase 7B ensures the removal of copper from the body. Deficiency of this enzyme disrupts the removal of copper from the brain into the blood, from the blood into bile and then from the body with feces, which leads to the accumulation of copper in the liver, spleen, kidneys, brain, cornea, lens of the eye and other organs. Copper accumulation in the liver causes hepatocyte necrosis, inflammation, fibrosis, bile duct proliferation, and cirrhosis; in the brain – necrosis of neurons with the formation of cavities (cysts) [7]. The destruction of hepatocytes entails a significant release of copper into the blood, which can lead to an increase in its concentration in the blood plasma, copper-induced hemolysis, and fulminant liver failure [8].
Classification
In Russia, the priority is the classification proposed by N.V. Konovalov [9], according to which there are 5 forms of VCD, of which the main ones are abdominal and cerebral. The abdominal form can manifest itself with an independent, multivariable spectrum of symptoms of liver damage. Variants of the cerebral form are rigid-arrhythmic-hyperkinetic, tremulous-rigid, tremulous and extrapyramidal-cortical.
Clinical picture
The course of BVC can be divided into two stages: latent and the stage of clinical manifestations. During the latent stage, there are no clinical symptoms; signs of the disease and copper accumulation in the body are revealed only during laboratory examination. In some patients, BVD manifests itself with hemolytic anemia, leukopenia and thrombocytopenia, and nephropathy of the tubular nephritis type [9, 10]. With effective treatment, the stage of negative copper balance is additionally distinguished. In curable cases, regression of clinical and laboratory manifestations of the disease is observed [11, 12].
In children with a defective ATPase 7B gene, copper initially begins to accumulate in the liver immediately after birth. That is why in children, BVD usually manifests itself as one of the variants of liver damage (abdominal form), which clinically manifests itself over the age of 4–5 years, although practically from birth they have a moderately elevated level of transaminases [13]. Then, after the liver is “saturated” with copper, which in some cases occurs asymptomatically, it is redistributed systemically, accumulating primarily in the central nervous system, which leads to the development of neuropsychiatric symptoms, which most often develop after 20–30 years [14]. In the cornea, copper accumulation occurs after the liver is “saturated” with it and almost simultaneously with the appearance of neuropsychic changes. Some patients develop copper “sunflower” cataracts [15].
In patients with BVC, any liver damage can occur, and “hepatic” manifestations may precede the development of neurological symptoms. The severity of liver damage can vary from asymptomatic to fulminate liver failure and decompensated cirrhosis [16, 17].
VCD is characterized by a variety of neurological, behavioral and psychiatric symptoms of varying severity - from insignificant to rapidly increasing and leading to complete disability in a short time. Neurological manifestations of BVD are usually detected between the ages of 10 and 35 years, but there are cases of manifestation at a later age. The clinical picture includes dystonia, ataxia, tremor, early parkinsonism with hypokinesia. The most common symptoms are dysarthria, salivation, impaired fine motor skills and walking, and tremor [18].
Behavioral and mental disorders are not only typical for VCD, but in some cases may precede “hepatic” and neurological symptoms. Children's performance at school decreases, mental retardation, personality changes, labile mood, inappropriate behavior, and manic-depressive manifestations are noted. Initial symptoms are often misdiagnosed as behavioral problems associated with puberty. Full-blown psychoses with psychoproductive symptoms are not typical for BVD [18, 19].
It is known that in 15% of patients, the initial symptom of BVC may be Coombs-negative hemolytic anemia. Episodes of hemolysis can be both acute and chronic and can be recurrent. Severe hemolysis is usually associated with severe liver damage. Massive breakdown of hepatocytes leads to the release of large amounts of stored copper, which enhances hemolysis [20].
Various renal dysfunctions are associated with VVC. As a result of the toxic effect of copper, dysfunction of the proximal and/or distal tubules develops. The glomerular filtration rate decreases. Distal tubular acidosis is a factor predisposing to the development of nephrolithiasis [21].
Symptoms of damage to other organs and systems are not typical for BVC, but in some cases arrhythmias and cardiomyopathies [22], pancreatitis and exocrine pancreatic insufficiency [23], cholelithiasis, copper-induced rhabdomyolysis, osteoporosis and osteomalacia, arthritis and arthralgia, amenorrhea, spontaneous abortion [11, 24].
Diagnostics
The diagnosis of VCD should always be considered in cases where a young patient has a combination of signs of liver and nervous system damage, hemolytic anemia, Kayser-Fleischer rings are detected on the iris, and there is a corresponding family history [11, 25]. It should be remembered that at the early stage of BVC and with inactive cirrhosis of the liver, liver tests may be normal or minimally changed, and signs of central nervous system damage and the Kayser-Fleischer ring are absent in 50% of such patients [14]. In the literature, there are descriptions of the combination of VCD with other liver diseases, for example, with chronic hepatitis C [26].
In patients with the abdominal form of BVC, hyperproteinemia, hypergammaglobulinemia, elevated IgG levels may be observed, and various autoantibodies are detected, which can be misleading about the presence of autoimmune hepatitis. It is characteristic that against the background of copper-eliminating therapy, complete normalization of IgG and autoantibody levels is observed. Obviously, in all patients with autoimmune hepatitis who do not respond to immunosuppressive therapy, BVD should be excluded [8, 27].
The most well-known clinical symptom of VWD are Kayser–Fleischer rings on the iris [11, 25, 28]. The main laboratory tests used to diagnose the disease are indicators of copper metabolism [29].
Ceruloplasmin, a protein synthesized in the liver, is an acute phase reagent of BVD. A decrease in ceruloplasmin levels is not the main diagnostic criterion for the disease. Its subnormal values have low prognostic significance, but a CPN concentration of less than 200 mg/l is considered a necessary criterion for considering the diagnosis of BVC.
A normal or elevated serum copper level with a reduced ceruloplasmin value indicates an increase in the content of copper not bound to this protein in the blood, which is used as a diagnostic test for BVD. Most untreated patients have copper levels greater than 50 mcg/dL (normal range is 5–12 mcg/dL). This indicator can be sharply increased in conditions of liver failure of any etiology.
Daily urinary copper excretion of more than 100 mcg (normal ≤40–50 mcg/day) in patients with symptoms of BVC is regarded as a positive diagnostic test.
The quantitative content of copper in liver tissue is the most informative diagnostic test. Its value above 250 μg/g dry weight of the organ (the norm is 15–55 μg/g) is the best confirmation of the presence of BVD. However, this test is rarely used in clinical practice.
To identify characteristic structural changes in the central nervous system, it is advisable to use magnetic resonance or computed tomography of the brain [30]. Comprehensive DNA diagnostics in patient families, including a search for the most common mutations, may be useful [31].
Treatment
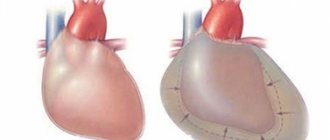
The main treatment for BVD is the use of copper-eliminating drugs (chelation therapy) and adherence to a strict diet with a reduced amount of copper in the diet. Currently, the following complexing drugs are used for BVC: D-penicillamine, trientine, tetrathiomolybdate and dimercaprol (Unithiol) [11, 32, 33]. As liver failure progresses, liver transplantation is recommended [11].
Of the tablet medications currently used in Russia for the treatment of BVD, D-penicillamine preparations (in particular, Cuprenil) are registered. The mechanism of action of D-penicillamine is associated with the formation of chelate complexes with copper and their elimination in the urine, the induction of metallothionein synthesis and the transfer of intracellular copper to a non-toxic state, an increase in the intracellular level of glutathione, a decrease in inflammation and a decrease in the activity of fibrogenesis. The therapeutic dose of the drug is 1–1.5 g/day (up to 4.0 g/day) 30 minutes before meals in 3–4 doses, the maintenance dose is 0.75–1.0 g/day also in 3–4 reception. Self-cessation of D-penicillamine by patients while their condition improves can lead to the development of fulminant hepatitis.
The mechanism of action of trientine (triethylenetetramine dihydrochloride) is the formation of chelate complexes with copper and their elimination in the urine, as well as a decrease in copper absorption in the intestine. The dose of trientine is 1–2 g/day in 3 divided doses on an empty stomach.
The point of application of zinc preparations (oxide, sulfate, acetate) differs from that of D-penicillamine and trientine. Zinc binds copper in the intestines, as a result of which the latter is not absorbed and is excreted from the body in feces. Zinc therapy may promote a negative copper balance and reduce its accumulation in the body [32–34]. The mechanism of action of zinc preparations in BVD is due to the induction of the synthesis of metallothionein (a copper-binding protein rich in cysteine - an endogenous metal chelator) in the epithelial cells of the small intestine, as well as in hepatocytes, and the transfer of copper to a non-toxic state. The dose is 150 mg/day in 3 divided doses. The criteria for the effectiveness of treatment are: improvement in general condition, reduction in the severity of visceral and neurological symptoms (weakening of hyperkinesis and extrapyramidal symptoms, decrease in muscle tone, improvement in coordination of movements, articulation, handwriting, reduction in heaviness in the right hypochondrium), reduction in the level of free copper in the blood, normalization of other laboratory parameters [11, 32, 33].
Clinical observation
Patient B., 51 years old, was admitted to the Department of Chronic Liver Diseases of the State Budgetary Healthcare Institution of the Moscow Scientific Research Center of the Department of Health with symptoms of lethargy and confusion. On examination - swelling of the legs, enlargement of the abdomen, unsteadiness of gait, loose stool.
From the anamnesis: the patient was born in Moscow, has higher education, is a military man, married, has two daughters. Heredity is not burdened. He became acutely ill about 30 years ago (at the age of 21), when, after participating in the liquidation of the consequences of the Chernobyl accident, he noted the appearance of severe weakness, skin hyperpigmentation, edema, ascites, and the development of neurological symptoms in the form of aphasia and adynamia. During the examination, varicose veins of the esophagus were discovered, which made it possible to formulate a diagnosis of liver cirrhosis. After identifying a reduced level of ceruloplasmin and Kayser-Fleischer rings, the patient was diagnosed with Wilson-Konovalov disease, abdominal form, stage of liver cirrhosis. Cuprenil therapy was started with a positive effect (regression of neurological symptoms, ascites).
Subsequently, the patient felt quite satisfactory and led an active lifestyle. Since 2007 (15 years after the manifestation of the disease), I began to “forget” to take Cuprenil (breaks in taking up to several days). I didn’t go to the doctors, which I explained by my heavy workload.
Since the end of February 2021, the patient began to notice the appearance of swelling of the legs, drowsiness and general weakness, attacks of impaired consciousness such as hepatic encephalopathy, and a psychotic episode developed (he did not remember the events that happened, did not recognize his wife, and was aggressive). He was sent for inpatient treatment to the State Budgetary Healthcare Institution MKSC DZM for treatment correction.
On admission the condition was of moderate severity. Asthenic build, normal nutrition, weight – 73 kg, height – 182 cm, body mass index – 22.0 kg/m2. Consciousness preserved, inhibited. Number connection test – more than 120 seconds. The speech is chanted.
Choreoathetoid movements in the hands. The skin and sclera are subicteric. Multiple spider veins on the skin. Peripheral lymph nodes are not enlarged. Severe swelling of the legs and feet. The muscular system is without any peculiarities. Auscultation reveals vesicular breathing, no wheezing, respiratory rate is 14 per minute. Heart sounds are muffled, the rhythm is correct, heart rate is 80 per minute, blood pressure is 120/80 mm Hg. The oral mucosa is pink and clean. The tongue is moist and clean. The abdomen is increased in size due to flatulence and ascites. The liver protrudes 2 cm from under the right edge of the costal arch, dense, painless. The spleen could not be palpated due to the enlarged abdomen. Diuresis is negative.
Examination by an ophthalmologist: no Kayser-Fleischner rings were found.
Clinical blood test: signs of anemia (hemoglobin level - 11.6 g/l, red blood cell count - 3.7 × 1012/l), prothrombin - 85.5%.
In the biochemical blood test: slight cytolysis (AST and ALT less than 1.5 normal values), severe hypoalbuminemia (25.4 g/l). The level of ceruloplasmin in the blood serum was reduced to 11.6 mg/dl, the copper level was reduced to 22.4 μg/dl (normal is up to 150 μg/l). Daily urinary copper excretion is 172.4 mcg/l and 310.8 mcg/day (normal is less than 40–50 mcg/day).
Ultrasound examination revealed signs of portal hypertension. During esophagogastroduodenoscopy, grade 2 varicose veins of the esophagus were detected (according to Soehendra).
Treatment with Cuprenil was resumed at a daily dose of 1500 mg (6 tablets) under the control of daily urinary copper excretion in combination with Zincteral (zinc sulfate) 620 mg per day. Therapy was also carried out with albumin, diuretics - spironolactone in combination with furosemide (under control of weight and diuresis), L-aspartate-L-ornithine (intravenous 20 ml/day, later - in the form of granulate 6 g/day), proton enzyme inhibitors pumps.
As a result of the treatment, the patient’s well-being improved: attacks of impaired consciousness did not recur, lethargy became less pronounced (number connection test - 48 seconds), edema syndrome regressed (swelling of the legs was stopped, ascites decreased significantly), according to laboratory examination, cholestasis symptoms were relieved, normalization albumin indicators. The patient was discharged in satisfactory condition. A special feature of this case is the effective use of L-aspartate-L-ornithine, which, in combination with chelation therapy, affects the symptoms of encephalopathy.
Thus, the above clinical observation illustrates one of the clinical variants of BVD, characterized by a latent course (up to 20 years), decompensation of liver cirrhosis and the appearance of severe neurological symptoms against the background of decreased adherence to treatment.
Symptoms of Wilson-Konovalov disease in adults
Possible manifestations are very diverse.
Most often, the liver is affected (about 40 - 50% of cases), and in other cases, neurological damage and mental problems may occur. When the nervous system and vision are damaged, a typical symptom appears - the manifestation of the Kayser-Fleischer ring (occurs due to the deposition of copper in the iris with its specific brown coloration). In the abdominal form of the disease, symptoms usually appear closer to 40 years of age. Among the key features:
- cirrhosis of the liver;
- chronic or fulminant (fulminant) hepatitis.
In childhood, the rigid-arrhythmohyperkinetic variant of the disease occurs more often.
It begins with rigidity (compaction, poor compliance) of muscles, disturbances in facial expressions, speech disorders, problems with performing movements requiring fine motor skills, and a slight decrease in intelligence. The disease is progressive, with periods of exacerbation and remission. The variant of shaking Wilson's disease usually occurs in the age range from 10 years to 30 - 35 years. Symptoms such as trembling, slow movements, speech inhibition, epilepsy attacks, and mental problems may occur.
The rarest form of the disease is extrapyramidal-cortical disorders. It is similar to all forms, in addition there will be convulsive attacks, severe intellectual problems, and movement disorders.
Read also
Huntington's chorea
There are many neurodegenerative diseases that exhibit symptoms similar to Parkinson's disease.
Therefore, the doctor requires special attention when interviewing the patient, as well as when… Read more
Parkinsonism
Parkinsonism is a well-known neurological syndrome that manifests itself in the form of a violation of voluntary movements. This syndrome is characterized by muscle stiffness, tremors of the limbs, and slowness of movements.…
More details
Parkinsonism, Parkinson's disease
What is Parkinson's disease? Parkinson's disease is a chronic progressive brain disease primarily associated with the degeneration of dopaminergic neurons in the substantia nigra with the accumulation of...
More details
Tiki
Tics in children: causes, symptoms, treatment methods. A tic is a sudden, jerky, repetitive movement that involves individual muscle groups or parts of the body. It could also be…
More details
Tourette's syndrome
Tourette's syndrome is a pathology of the nervous system, which is characterized by sudden and repeated movements and sounds called tics. Tourette's syndrome occurs more often in men than...
More details
Diagnostics
If eye symptoms are present, the doctor will first examine the eyes with a slit lamp to confirm the presence of a Kayser-Fleischer ring.
The appointment of biochemical tests of blood and urine is indicated, which will show an increased copper content in the urine and a reduced concentration of ceruloplasmin in the blood plasma.
A CT or MRI will show atrophic processes in the brain and cerebellum, damage to the basal ganglia.
Additionally, a consultation with a geneticist and a series of genetic tests are carried out to identify defective genes.
Symptoms
The age of manifestation of the disease varies: symptoms may begin to appear in a child of 3–5 years, or the disease may not make itself felt for decades. However, most often Wilson-Konovalov disease develops by the age of forty, in rare cases - after fifty years. The clinical picture of the disease depends on gender and age, for example, in children (average age - 10 years) liver damage often predominates.
Signs and symptoms of the disease include:
- liver manifestations (hepatomegaly, acute hepatitis, chronic hepatitis, cirrhosis, fulminant liver failure) usually precede neurological and psychiatric symptoms;
- change in color of the skin, mucous membranes and sclera of the eyes to yellow;
- swelling of the legs and abdomen (ascites);
- pain in the upper right abdomen;
- bruising of the skin, coagulopathy;
- increased fatigue;
- loss of appetite and weight;
- nausea and vomiting;
- neurological symptoms (tremor, impaired coordination and gait, dysphagia, dysarthria, chorea, spasticity, dystonic postures, muscle rigidity);
- mental disorders (emotional instability, phobias, anxiety, depression, compulsive behavior, aggression, personality and behavior changes) vary widely from patient to patient, appear simultaneously with neurological symptoms or develop within about 3 years after their onset;
- Kayser-Fleischer rings at the border of the cornea of the eyes (in almost all patients with neurological symptoms and mental disorders);
- amenorrhea;
- delayed puberty;
- miscarriages, infertility;
- arthralgia, bone pain;
- damage to bones and joints (osteoporosis, osteophytes);
- cardiomyopathy;
- hemolytic anemia;
- hematuria;
- nephrotic syndrome;
- renal tubular acidosis;
- stones in the kidneys;
- hepatocellular carcinoma (rare).
Modern methods of treatment
The main method of treatment for this disease is the prescription of thiol drugs, especially unithiol or D-penicillamine, cuprenil.
The drugs are taken for a long time, the doctor selects the most optimal dose to avoid side effects. Additionally, the doctor may use drugs from the group of antipsychotics; for muscle stiffness, levodopa or carbidopa.
In severe cases, liver transplantation and immunosuppressive therapy are indicated. It is possible to use biohemoperfusion with an isolate of living cellular elements of the spleen and liver.
Additionally, it is necessary to follow a diet excluding foods containing large amounts of copper.
Prevention of Wilson-Konovalov disease in adults at home
“To prevent pathology,” says neurologist Valentina Kuzmina, “it is necessary to adhere to diet No. 5, and also limit copper intake to 1 g per day - exclude nuts, dried fruits, chocolate, crayfish, cookies, whole wheat. It is also recommended to take drugs from the vitamin B6 group, unithiol, trientine.