According to the ICD 10th revision, the following liver disorders are distinguished:
- By 70. Alcohol disease
- To 70.0. Alcoholic fatty infiltration
- To 70.1. Alcoholic hepatitis, toxic
- By 70.9. Alcohol disease, unspecified
Liver diseases
combines various disorders of the structure of the parenchyma and the functional state of the hepatocyte caused by the systematic consumption of alcoholic beverages.
Alcoholic liver diseases
are classified as toxic.
Related information: coding for alcoholism, therapeutic plasmapheresis, withdrawal from binge drinking
Highlight:
- adaptive alcoholic hepatopathy , which is the initial stage of the disease, is established on the basis of histomorphological and electron microscopic examination of biopsy specimens (hypertrophy of the smooth endoplasmic reticulum, sharply enlarged mitochondria, hepatocytes with frosted glassy cytosol, Mallory bodies - specific hyaline);
- Alcoholic fatty liver disease (fatty hepatosis)
is the most common form of alcohol-related disease.
General information
Fatty liver disease is also known as fatty liver, fatty liver, or hepatic steatosis (mistakenly known as liver stenosis). It is considered an independent syndrome or disease that is caused by fatty degeneration of liver cells. In the 60s of the last century, it was isolated as an independent disease after the introduction of puncture biopsy of liver tissue into practice.
The pathology is characterized by the deposition of fatty droplets in the extra- and (or) intracellular space of the liver. A morphologically important criterion for hepatosis is the content of triglycerides in the hepatic system above 10% of dry weight.
With non-alcoholic steatohepatitis, there is the same increase in liver enzymes and identification of specific morphological changes in liver biopsies, as with alcoholic hepatitis , with the only difference that patients with NASH do not abuse alcohol-containing drinks in volumes that can cause such damage to hepatocytes. ICD-10 code for fatty liver disease: K70.0 Alcoholic fatty liver [fatty liver]
Alcoholic liver fibrosis
Alcoholic fibrosis is the appearance of pericellular and venular fibrosis against the background of long-term alcohol consumption. This form of the disease precedes cirrhosis, sometimes without clinical, histological signs of acute or chronic alcoholic hepatitis. An important point in the development of fibrosis is the ability of ethanol to activate lipid peroxidation and fibrogenesis: the reticular-mesenchymal system, lipocytes - cells, ito, which exhibit the ability to produce collagen. Perivenular fibrosis is characterized by increased tissue proliferation around the central veins of the hepatic lobule. Some of the strands from the centrilobular zone spread into the parenchyma along the sinusoids and hepatocytes, which creates pericellular fibrosis.
The clinical and functional manifestations of fibrosis and fatty hepatosis are identical. A distinctive feature of the first is the increase in the blood of the amino acids proline and hydroxyproline, which are a large component of collagen.
Perivenular fibrosis can be stopped by abstinence from alcohol, treatment as for fatty liver
. Chronic centrilobular sclerosis transforms into cirrhosis even with complete abstinence, however, treatment and abstinence from alcohol delay the development of the cirrhosis stage.
Pathogenesis
Fat is deposited in the cytoplasm of liver cells only when the rate of triglyceride formation in the liver exceeds the rate of their utilization. The latter process involves lipolysis of triglycerides, their incorporation into pre-B lipoproteins, oxidation of fatty acids and secretion into the bloodstream.
Regular changes in the form of fatty infiltration in the liver are observed with:
- decompensated form of diabetes mellitus ;
- chronic alcohol intoxication;
- protein deficiency (including nutritional origin);
- obesity;
- poisoning by toxic compounds;
- lack of lipotropic substances in exocrine pancreatic insufficiency.
The most common disorder of fat metabolism with characteristic fat deposition in the hepatic system is ketosis . The pathology is characterized by increased deposition of ketone bodies due to altered metabolism , which leads to their accumulation in organs and tissues in the decompensated form of diabetes mellitus. Quite often, along with fatty degeneration, gallbladder dyskinesia , sometimes in combination with cholelithiasis .
Reasons why fat may be deposited in liver cells:
- decreased production of lipoproteins of various densities in the hepatic system;
- excessive intake of free fatty acids into the hepatic system;
- functional liver failure caused by liver pathology;
- excessive formation and absorption of free fatty acids in the liver;
- slowing down beta-oxidation of free fatty acids in the mitochondrial system of hepatocytes.
Histological features
Brown liver atrophy is characterized by a decrease in the size of hepatocytes, however, their number is much greater than with its normal structure. The general structure of the hepatic system remains unchanged. Liver cells are reduced in volume mainly in the central lobules located near the central vein. The radial arrangement of the hepatic beams is disturbed, they are thinned. The cells themselves have an irregular oval and round shape. The nuclei are stained darker and reduced in size. In the cytoplasm there are many small grains of a yellowish-brown color, which gives the organ a brownish-brown color.
Classification
It is customary to distinguish two nosologically independent forms of fatty hepatosis:
- non-alcoholic steatohepatitis (toxic liver dystrophy);
- alcoholic fatty liver disease.
The non-alcoholic, toxic form is diagnosed in 7-8% of patients undergoing liver biopsy. The alcoholic form is detected 10 times more often.
Morphological forms according to the type of fat deposition in the hepatocyte lobule:
- focal disseminated variant (practically asymptomatic);
- zonal, pronounced disseminated variant (fat deposits accumulate in different areas of hepatocytes);
- diffuse variant (microvesicular, diffuse liver steatosis).
According to genesis there are:
- Primary hepatosis. The pathology is caused by various endogenous dysmetabolic disorders such as diabetes mellitus , obesity , and dyslipidemia .
- Secondary hepatosis. Develops under the influence of external influences that worsen metabolism.
The secondary form is registered with malabsorption syndrome , taking certain medications, after surgery on the digestive tract (gastroplasty for obesity, ileo-jejunal anastomosis, intestinal resection). Pathology can be observed during prolonged stay on parenteral nutrition, as well as in persons practicing fasting.
Hydropic liver dystrophy
The pathology is also known as hydrocele . Characterized by the appearance of vacuoles that contain cytoplasmic fluid. Gradually, as the fluid becomes overfilled, the cell structures decompose. The hydropic form can only be diagnosed by microscopic examination, because Externally, the liver organ appears without any special visual changes.
Fatty infiltration of the liver and pancreas
Let's figure out what it is. Fatty infiltration is characterized by the deposition of fat and the subsequent displacement of normal cell structures, which negatively affects the functioning of the organ. In addition to the liver, the pancreas can also be affected, fatty infiltration of which indicates severe metabolic disorders in the body. In this case, a diagnosis is made - steatohepatitis .
There are alcoholic and non-alcoholic steatohepatitis. Classification according to ICD 10 - K76.0 Pathology is divided according to the degree of damage and the degree of activity of the fatty process. At the initial stage, steatohepatitis of minimal activity is formed. In the absence of proper treatment, elimination of the causative factor and changes in lifestyle, the disease becomes severe.
What is pancreatic steatosis? Fatty damage to the pancreas is called steatosis.
Introduction
Since steatohepatitis was first described in the early 1980s as a “poorly understood and hitherto unnamed liver disease” [1], the understanding of non-alcoholic fatty liver disease (NAFLD) has evolved significantly and gradually gained acceptance among hepatologists. NAFLD is a chronic stress-induced liver disease associated with abdominal obesity and metabolic syndrome, which develops in patients who do not drink alcohol in doses of more than 40 g of pure ethanol for men and 20 g for women per day or in the absence of other possible causes of the pathology. liver, including secondary ones (taking certain medications, storage diseases, etc.) [2]. The medical community is paying more and more attention to this problem from the perspective of both fundamental and clinical medicine. The number of publications devoted to NAFLD is growing exponentially.
The purpose of the review is to highlight a number of epidemiological and pathophysiological aspects, as well as issues of management and treatment of patients with NAFLD.
Epidemiological, clinical and pathophysiological aspects of non-alcoholic fatty liver disease
The prevalence of NAFLD ranges from 6.3 to 33% with a median of 20% in the general population; in the USA it reaches 46%, in the Asian part of Europe - 27.4% [3]. About 10-20% of patients with NAFLD have signs of lymphoid-macrophage infiltration (necroinflammatory activity), from 1.5 to 6.5% of the general population have non-alcoholic steatohepatitis (NASH) according to a study of biopsy material, and 15% have signs of progressive liver fibrosis and/or cirrhosis [4-7]. The detection rate of NAFLD in patients with type 2 diabetes mellitus reaches 55.5% [8], which defines this pathology as the leading risk factor for the development of NAFLD.
There is a negative upward trend in the prevalence of NAFLD among children; the highest rate (up to 11.8%) was found in the Spanish population. Established risk factors include obesity and type 2 diabetes, as well as a family history of NAFLD and maternal gestational diabetes. It is expected that the epidemiological situation in this population will only worsen [9].
Researchers from the USA using the A.A. model. Markov predicted a more than twofold increase in the incidence of NAFLD and its progressive forms by 2030. Mortality from liver diseases will increase by 178%, which is estimated at 78,300 deaths in 2030. Thus, in the period from 2015 to 2030, according to forecasts, 800 thousand deaths associated with liver diseases will be recorded [10].
Over the past 10 years, the prevalence of NAFLD as a reason for liver transplantation has increased by 170%. In comparison, the incidence of hepatitis C virus and alcoholic liver disease as reasons for transplantation increased by only 14 and 45%, respectively. Researchers from European and Asian countries also note an emerging trend towards an increase in the proportion of NAFLD among the causes of overall mortality, the development of cirrhosis, hepatocellular carcinoma and associated death [11, 12].
NAFLD is the second leading etiology of liver disease in recipients of hepatocellular carcinoma. Less information is available on NAFLD as an indication for liver transplantation in the European registry. Since 1968, 145 transplant centers in 26 European countries have performed 93,634 transplants (France 16,366, Spain 15,714, UK 13,684 and Italy 11,697). In recent decades, alcoholic liver disease has been the leading reason for liver transplantation (20%), followed by viral hepatitis C and B (14 and 5%), while cryptogenic cirrhosis accounts for only 4% [13].
The lifetime cost of treatment for all patients with NAFLD in the United States in 2021 was $222.6 billion, and the cost of managing patients with NASH was $95.4 billion. From these data, it can be concluded that treatment and Management of patients with various stages of NAFLD is associated with a high economic burden, and in the absence of treatment, the total direct costs of the disease for these patients will continue to rise, and these costs will be even greater when social costs are taken into account [8].
The modern concept of NAFLD covers a spectrum of liver damage, including the following forms: fatty liver disease (FHL), non-alcoholic (metabolic) steatohepatitis (NASH), fibrosis and cirrhosis (as an outcome of progressive NASH) (Fig. 1) . When conducting a cytological examination of biopsy material, it is not always possible to assess the condition of the liver as a whole, so scientists have formed the opinion that there is an intermediate form of NAFLD, which is characterized by the presence of fatty deposits and an inflammatory reaction without necrosis of hepatocytes, which does not allow us to speak unambiguously about the rate of progression of the disease.
Rice. 1. Forms of non-alcoholic fatty liver disease in the structure of causes of liver transplantation.
HCC is hepatocellular carcinoma, NASH is non-alcoholic steatohepatitis.
A generally accepted strategy is to establish a diagnosis of NAFLD with clarification of risk factors for the disease and the activity of the process (steatosis, steatohepatitis, intermediate form). Undoubtedly, the clinical and biochemical activity of the disease is a reflection of the severity of NAFLD and the risk of developing liver cirrhosis. However, the priority prognostic factor is liver fibrosis, which determines the further survival of patients and the development of complications. It has been proven that, in contrast to mortality associated with complications, including fibrosis and NASH, overall mortality in patients with NAFLD was associated only with fibrosis, but not with NASH [14]. According to an assessment of more than 17 thousand patients, the presence of liver fibrosis in a patient, as well as progression of the disease to stages III-IV (according to elastometry results), increase overall mortality and mortality associated with liver disease by more than 2 times [15]. It can be said that, by analogy with assessing the degree of inflammation and the stage of chronic gastritis or the glomerular filtration rate in chronic kidney disease, when establishing a diagnosis of NAFLD, it is necessary to determine the degree of inflammation (NASH) and the staging of liver fibrosis.
Patients with NAFLD have a higher prevalence of cardiovascular diseases than patients without NAFLD, regardless of body mass index (BMI) and traditional risk factors for the development of cardiovascular pathology [16]. The mortality rate from cardiovascular diseases in the group of patients with NAFLD prevails over the mortality rate from liver diseases and is 36% compared to 6.8%. To date, it has been established that the outcomes of progressive non-alcoholic steatosis and steatohepatitis are fibrosis, liver cirrhosis, and hepatocellular carcinoma. With long-term observation, progression of fibrosis is detected in 50% of patients with NAFLD, and often this process occurs without clinical manifestations. Population-based studies suggest that NASH results in 60–80% of cryptogenic liver cirrhosis. NAFLD is the leading cause of liver transplantation worldwide. Liver fibrosis is recognized as a leading factor determining patient prognosis and the risk of death associated with both major cardiovascular events and progression of NAFLD [15, 17].
A more complete understanding of the pathogenesis of NAFLD and research data on the relationship of NAFLD and its forms with diseases of the heart, blood vessels, kidneys, and pancreas leads us to the conclusion that this disease should be considered as a component of the metabolic continuum, the inducer of which is obesity and associated systemic inflammation and fibrosis [18, 19]. In this regard, in 2021, a new concept for understanding NAFLD was announced as fatty liver associated with metabolic dysfunction or metabolic-associated fatty liver disease (MAFLD) [20]. Criteria for the diagnosis of MAFLD are based on the presence of steatosis in addition to one of the following three criteria, namely: overweight/obesity, presence of type 2 diabetes mellitus, or evidence of metabolic dysregulation, that is, at least two criteria for metabolic syndrome at normal body weight patient (Fig. 2) .
Rice. 2. Principles of diagnosing metabolic-associated fatty liver disease.
HDL - high density lipoproteins; HbA1c - glycated hemoglobin; BP - blood pressure.
It is known that obesity is a widespread and growing problem in all countries of the world. The prevalence of obesity is increasing in both developed and developing countries, affecting more people in older age groups. NAFLD is associated with obesity and overweight [21]. The prevalence of hepatic steatosis in morbidly obese individuals receiving bariatric care increases to 90%. BMI is an independent predictor of the development of fatty liver infiltration, and its increase to 30 kg/m2 and above is accompanied by the development of hepatic steatosis in 95–100% and NASH in 20–47% [22]. However, studies have demonstrated that almost 25% of patients with NAFLD do not have metabolic disorders and are classified as having normal body weight. In the absence of obesity, this fact suggested a favorable course of NAFLD without progression, but thanks to the National Health and Nutrition Examination Survey III, it was demonstrated that the mortality of patients with “metabolically normal” NAFLD is the same as in the cohort without this pathology. A study of 430 patients with biopsy-proven NAFLD found that 55% of patients without obesity and NASH had fibrosis stage ≥F2, despite less metabolic changes than in patients who were obese and NAFLD. And according to the results of a 10-year follow-up of patients with NAFLD and high stages of fibrosis, no differences were found in long-term prognosis for patients with and without obesity [23, 24]. There is a shift from assessing obesity based on BMI (BMI-based approach) to assessing obesity based on the presence or absence of obesity-related diseases or conditions (complication-based approach), as announced at the XXIII Annual Scientific Congress of the American Endocrine Association. In the new algorithm for diagnosing obesity, NAFLD is also included in the list of painful conditions-complications [25].
The expert group proposes a set of criteria to define cirrhosis associated with MAFLD and a conceptual framework for considering other causes of fatty liver disease. The authors suggest that achieving consensus on MAFLD criteria will help to unify terminology (eg, for ICD coding), increase the legitimacy of clinical practice and clinical trials, improve clinical care, and improve research efforts. Experts proposed to distinguish phenotypes based on the coexistence of metabolic disorders and other lesions of the liver tissue, alcoholic liver diseases, autoimmune diseases, since the pathogenesis of fatty liver disease is heterogeneous, and the morphological reflection of pathological processes is similar. This aspect dictates the need, first of all, to take into account clinical factors, and the identification of phenotypes will allow the development of individual patient management strategies. However, given the knowledge of liver fibrosis as a factor determining mortality in patients with NAFLD, researchers emphasize the need to evaluate it regardless of the leading factor initiating fibrogenesis [26, 27].
Therapeutic goals
Despite its high prevalence and contribution to the decline in the health-saving potential of the population, there are currently no approved treatments for NAFLD [28]. Among all aspects of the study of this pathology, progress in the therapeutic field has been the slowest, although there has been steady progress in understanding the disease epidemiology, pathophysiology, and identification of therapeutic targets.
Because no medications or surgeries are currently approved for the treatment of NAFLD, lifestyle interventions (diet, physical activity, and dietary modification) remain the cornerstone of the management approach. It has been noted that physical aerobic activity reduces the chances of developing NASH by reducing the risk of developing type 2 diabetes mellitus, hypertension and metabolic syndrome [29, 30]. Exercise reduces liver fat content regardless of the amount of weight loss [31], but weight loss of more than 7–10% has been shown to reduce the stage of fibrosis [32].
In terms of nutrition, the main goal is to reduce the total calorie content of the daily diet, include foods with antioxidant activity (rich in vitamins C, E and D), limit simple sugars and sweetened drinks in favor of fructose and saturated fats in favor of polyunsaturated fats. The listed requirements are fully met by the Mediterranean type of nutrition [33].
An important and, according to researchers, underappreciated topic is the influence of the circadian clock on the development and progression of NAFLD. A. Mukherji et al. suggest that the circadian clock regulates physiological functions and plays a key role in maintaining metabolic homeostasis. Genetic and genomic studies have established that many genes are directly controlled by the circadian clock mechanism, influencing both anabolism and catabolism. Many hepatocyte functions, including nutrient uptake, processing, assimilation, and detoxification, are subject to diurnal fluctuations according to nutrient availability and energy expenditure. Researchers have focused on the mechanisms linking circadian dysregulation to the development and progression of NAFLD and diseases of other organ systems. Thus, adjusting the rhythm of life in accordance with the circadian clock mechanism can be considered as a potential therapeutic target for hepatic steatosis and NASH [34].
In connection with such theories, it is interesting to develop “time-restricted feeding” (TRF) - a circadian synchronized dietary approach in which access to food is limited for a certain period of time (8-16 hours) [35]. A study of patients with NAFLD showed that TRF significantly reduced body weight and triglyceride levels after 12 weeks compared with those in the control group [36]. Mice exposed to a TRF regimen show a reduction in the severity of hyperinsulinemia, liver fat content, and inflammation despite consuming a high-fat diet compared to controls [37].
In terms of pharmacological aspects of treatment, more than 1000 molecules are in development with potential to reduce steatosis, NASH and fibrosis. The most promising are molecules affecting lipid and glucose metabolism, insulin sensitizers and antioxidants.
Thiazolidinediones, also known as glitazones, are the group of drugs with the strongest evidence base tested for the treatment of NAFLD [38]. However, side effects such as congestive heart failure and osteoporosis do not allow the use of these drugs to their full potential.
Liraglutide is an incretin mimetic that acts as a glucagon-like peptide-1 receptor agonist and is used primarily for the treatment of type 2 diabetes mellitus and obesity, thus having the potential to act as a metabolic regulator in NAFLD. In an animal model, liraglutide therapy was associated with a reduction in hepatic steatosis in mice fed a high-fat/high-fructose diet [39]. The addition of liraglutide or semaglutide to metformin in patients with type 2 diabetes for 26 weeks resulted in weight loss and improvement in hepatic steatosis and visceral adipose tissue. The findings support the use of liraglutide or semaglutide as adjunctive therapy in patients with NAFLD and type 2 diabetes mellitus not optimally controlled with metformin. Further studies are needed to evaluate the effectiveness of longer treatment and to determine whether liraglutide or semaglutide improves histological parameters, including liver fibrosis [40].
Among the drugs that can influence metabolic processes, modulators of nuclear transcription factors, in particular the farnesoid X receptor, are undoubtedly promising. The farnesoid X receptor (FXR) is a nuclear receptor expressed in the liver, intestine, and kidney. FXR acts as a sensor for elevated bile acid levels and initiates homeostatic responses to control bile acid levels and also modulates other metabolic processes such as gluconeogenesis and lipogenesis. Obeticholic acid (OCA), an FXR stimulator, in a phase IIb study (FLINT) showed that 45% of patients with NASH treated with OCA 25 mg/day for 72 weeks had improved liver histology. compared with 21% of NASH patients receiving placebo during the same period [41]. In the phase III study (REGENERATE), after 72 weeks of therapy with OCA at a dose of 25 mg, there was a decrease in liver fibrosis (at one or more stages) in the absence of worsening of NASH (p = 0.0002) and a dose-dependent decrease in the activity of alanine aminotransferase, aspartate aminotransferase and γ-glutamyl transpeptidase , which led to the conclusion of consistent effectiveness with an overall adverse event profile similar to that observed in previous studies [42].
Peroxisome proliferator-activated receptors (PPARs) are a group of nuclear receptors that are expressed in the liver, adipose tissue, heart, skeletal muscle, and kidney and transcriptionally regulate numerous metabolic processes, including β-oxidation, lipid transport, and gluconeogenesis [43]. They are classified into three isotypes, designated PPARα, PPARβ (also known as PPARδ), and PPARγ, which differ in tissue distribution; however, they target the same DNA segment. Activation of PPARα increases the expression of lipoprotein lipase (LPL), thereby increasing the clearance of plasma triglycerides. In vitro and in vivo studies show that PPARα suppresses the secretion of interleukins (IL-1, IL-6) and tumor necrosis factor (TNF), as well as intercellular adhesion molecule 1 (ICAM1) and vascular cell adhesion molecule 1 (VCAM1) [44 ]. The double-blind, randomized, phase II b clinical trial GOLDEN (Europe and USA) compared elafibranor, a PPAR alpha/delta (α/δ) agonist, at doses of 80 mg and 120 mg daily with placebo in 276 patients with histologically proven NASH in for 52 weeks. However, an interim analysis yielded negative results [45]. Lanifibranor, as an agonist of all three isotypes, is currently the most promising among this group of drugs. The NATIVE phase II clinical trial demonstrated positive dynamics of NASH with the use of lanifibranor 1200 mg/day without an increase in fibrosis and, conversely, a reduction in fibrosis by at least one stage from the initial one without worsening NASH [46].
A promising and interesting molecule appears to be resmetir (MGL-3196), a thyroid hormone mimetic that is approximately 28 times more selective for thyroid hormone receptor β (THR-β) over α (THR-α) than triiodothyronine [47]. In NASH, this selectivity for THR-β is thought to provide metabolic benefits of thyroid hormone that are mediated by the liver, while avoiding the undesirable effects of excess thyroid hormone in the heart and bones that are primarily mediated through THR-α. A multicenter, randomized, double-blind, placebo-controlled, phase II clinical trial examining resmetirom treatment (NCT03900429) demonstrates significant reductions in liver fat in patients with NAFLD after 12 and 36 weeks of treatment. Side effects of treatment in patients in the study groups were mild or moderate, with the exception of a high incidence of transient mild diarrhea and nausea in those receiving resmetir [48].
Of particular interest is the study of the galectin-3 inhibitor belapectin. An increase in galectin-3 content is associated with the development of NASH and fibrosis of any etiology, which has been proven in experimental mouse models. A randomized phase II b trial of the safety and efficacy of GR-MD-02 (belapectin) in patients with NASH, cirrhosis, and portal hypertension is underway. However, preliminary results demonstrate that belapectin infusion administered twice weekly for a year is safe but is not associated with a significant reduction in steatosis or fibrosis compared with placebo [49].
A logical and justified approach to selecting therapy for NAFLD by combining 2 or 3 drugs that affect different parts of the pathogenetic chain of the natural course of the disease, especially since trials of drugs as monotherapy for the treatment of NASH and fibrosis showed a response rate of less than 32% compared with placebo. The largest number of studies use an overlapping combination sequence, where both study drugs are administered simultaneously for the duration of the study. Currently, most combination therapy studies are conducted using antidiabetic drugs, obeticholic acid and drugs that affect lipid metabolism (statins) [50].
Causes of fatty liver
Fatty deposits in the parenchymal cells of the liver appear as a result of the toxic effects of endogenous and exogenous factors. Other pathological conditions of the body, including starvation, can also lead to fat accumulation.
Causes of fatty liver and fatty hepatosis:
- diseases of the biliary tract and digestive system;
- formed intestinal bypass anastomosis;
- diabetes mellitus type 2;
- Wilson-Konovalov disease;
- obesity;
- long-term use of parenteral nutrition;
- malabsorption and maldigestion syndrome ;
- taking certain medications (estrogens, corticosteroids);
- chronic abuse of alcoholic beverages;
- celiac enteropathy;
- systemic diseases;
- viral, bacterial diseases.
The Invisible Disease: Fatty Liver Disease
We were looking for one thing and found it... fatty liver disease. This figurative expression generally reflects the peculiarity of this disease: in the initial phases of its development, a person is often not bothered by anything. It is discovered accidentally - for example, during an examination for another disease.
We talk about what this disease is and why it should be given due attention with the gastroenterologist at the Expert Kursk Clinic, Natalya Vitalievna Soshnikova.
— Natalya Vitalievna, what is non-alcoholic fatty liver disease?
This concept combines a spectrum of clinical and structural changes in the liver, which are represented by steatosis, non-alcoholic steatohepatitis, fibrosis and cirrhosis, and develop in patients who do not drink alcohol in quantities toxic to the liver.
Hepatitis C is often called the “gentle killer.” Why was he called that? Quote from the material “Shield and sword against hepatitis C. How to protect yourself and your loved ones?”
— Is non-alcoholic fatty liver disease somehow coded according to ICD-10?
Yes, its code is K76.0 (fatty liver degeneration).
— Hepatosis, steatosis and fatty liver disease – are they the same diagnosis or are they different diseases?
Strictly formally not quite so. Classification steatosis (hepatosis) is the first phase of fatty liver disease. In addition to steatosis, there is a phase of steatohepatitis and cirrhosis.
FOR TODAY'S ONE, OK
OF THE STUDYED DEVELOPMENT MECHANISM
NO FATTY LIVER DISEASE
— Is fatty liver disease an independent disease or can this condition be a consequence of some other disease?
More likely the second, but with clarification. The main cause of the development of this disease is the so-called metabolic syndrome - a complex of metabolic and hormonal disorders, which includes obesity, high blood pressure, pathology of lipid metabolism and insulin resistance. To date, there is no single, well-studied mechanism for the development of fatty liver disease.
— What is the danger of this disease? What happens to the liver during fatty disease?
The fact is that this pathology goes through certain stages. First, fat begins to accumulate in the liver cells (steatosis). Later, their functions change, and an inflammatory process develops (steatohepatitis). In the last, 3rd stage, connective tissue grows in the liver (fibrosis, turning into cirrhosis).
- For what reasons does this disease occur?
The main role is played by insulin resistance and changes in the profile of hormones that regulate fat metabolism (for example, leptin). This leads to disruption of fatty acid metabolism, penetration of triglycerides into liver cells and their accumulation.
— Who is at risk?
These are people with obesity, type 2 diabetes mellitus, arterial hypertension, coronary heart disease, and hypothyroidism.
“One of the signs of liver disease is suddenly appearing bruises on the patient’s body.” Quote from the material “MRI of the liver: pros and cons”
— What are the symptoms of fatty liver disease?
Most often, there may be no signs, i.e. it is discovered accidentally when the patient is being examined for another reason.
However, some people may still have nonspecific complaints. This is, for example, increased fatigue; aching pain or discomfort in the right hypochondrium, without a clear connection with food intake; sometimes - a feeling of bitterness, dry mouth.
DANGERS OF FATTY LIVER DISEASE
IS THAT ITS INITIAL PHASES
OFTEN THEY DO NOT MAKE THEM KNOW ABOUT THEM
In the third phase, when it comes to liver cirrhosis, the manifestations will be more obvious. This is an increase in the volume of the abdomen due to the accumulation of fluid in the abdominal cavity, hemoptysis and some other symptoms. This is the danger of fatty liver disease, that its initial phases often do not make themselves felt.
— How is the diagnosis established? Is there a “gold standard” of testing for suspected non-alcoholic fatty liver disease?
The most often performed is a detailed biochemical blood test, lipid profile (total cholesterol, high and low density lipoproteins, triglycerides), and liver ultrasound.
How safe is contrast? There is nothing to be afraid of, the contrast agent is hypoallergenic. Quote from the material “Why do we need contrast in MRI?”
If the picture of the disease is “blurred”, there are suspicions of other pathologies, an MRI of the liver with contrast can be performed (in the absence of contraindications), elastometry, and a liver tissue biopsy.
— What specialty does a doctor treat fatty liver disease?
Gastroenterologist. However, when caring for such a patient, we also need doctors of related specialties - a cardiologist and an endocrinologist. With their participation, an adequate treatment plan is developed.
If there is no gastroenterologist, the patient can be treated by a therapist, but again with the assistance of the above specialists.
— Can fatty hepatosis be cured?
By maintaining a correct, healthy lifestyle and receiving adequate treatment, fatty liver disease can be stabilized in the first phase of the disease. This prevents the disease from moving into deeper phases and improves the prognosis.
— Natalya Vitalievna, tell us about the prevention of non-alcoholic fatty liver disease. What recommendations should be followed so that this disease does not take you by surprise?
For obesity, it is necessary to reduce body weight by at least 10%. An important condition: the rate of weight loss should not exceed 500-1000 g per week. A faster pace can worsen steatosis and lead to steatohepatitis.
It is recommended to adhere to the Mediterranean type of diet (lots of vegetables and fruits, plant fiber, fish), fatty meat, fast food, carbonated drinks, canned food are limited).
You should move enough. The minimum load is walking at an average pace for 20 minutes a day, at least 5 times a week. Swimming and cycling are useful. In other words, you need to lead a healthy lifestyle.
Other materials on topics:
Is it possible to cleanse the liver?
What to do if gallstones are found?
How to protect yourself from Botkin's disease?
For reference:
Soshnikova Natalya Vitalievna
In 2003 she graduated from the Faculty of Medicine of Kursk State Medical University.
From 2003 to 2004 she studied at an internship in the specialty “Therapy”.
In 2005, she underwent professional retraining in the specialty “Gastroenterology”.
Currently working as a gastroenterologist at Clinic Expert Kursk. Receives at the address: st. Karl Liebknecht, no. 7.
He is an active member of the Russian Gastroenterological Association (RGA) and the Russian Society for the Study of the Liver (ROSPI).
Symptoms of hepatosis
The clinical symptoms of steatosis vary depending on the etiology of the disease.
In chronic alcohol intoxication with damage to the hepatic system, patients complain of shortness of breath during physical activity and anorexia. Most often, fatty liver disease is practically asymptomatic. It is extremely rare for patients to complain of discomfort and heaviness in the upper quadrant of the abdomen on the right. The pain increases with walking and movement.
There is no pain on palpation of the liver, except in cases where fat in the liver accumulates rapidly in the decompensated form of diabetes mellitus and alcoholism.
The complexity of this pathology lies in the fact that, despite significant morphological changes, most patients do not have specific symptoms of fatty liver hepatosis.
65-70% of patients are women, and most of them are overweight. Many patients have non-insulin-dependent diabetes mellitus. The vast majority of patients do not have signs of fatty liver disease, as characteristic manifestations of pathology of the hepatic system.
Tests and diagnostics
Palpation indicates an increase in liver size, but much depends on the concomitant pathology.
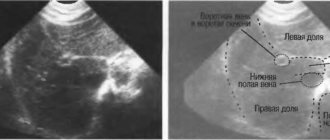
Sonographic signs
Often, after undergoing an ultrasound, the patient does not understand what the echographic signs of fatty hepatosis mean. In fact, the echogenicity of the liver tissue in fatty hepatosis may not be changed or may be increased. Signs of hepatosis of the liver on ultrasound are difficult to differentiate from fibrosis and cirrhosis of the liver . Therefore, to obtain more detailed information, it is recommended to undergo magnetic resonance or computed tomography. Thanks to these research methods, it is possible to accurately identify fatty deposits in the hepatic system.
Ultrasound examination reveals areas with increased echogenicity, and computed tomography identifies areas with a low absorption coefficient. However, the final diagnosis is made after a targeted liver biopsy, which is carried out under the control of computed tomography. Over time, lesions may change or completely disappear during therapy, which makes it possible to evaluate the dynamics.
Thus, the presence of fatty deposits can be accurately confirmed after a histological examination of the biopsy specimen. The materials obtained from the biopsy are stained with eosin and hematoxylan. Sections of hepatocytes reveal a nucleus displaced to the periphery and “empty” vacuoles.
In fatty hepatosis caused by long-term alcohol intoxication, together with large-droplet obesity of hepatocytes, the following is observed:
- deposits of hyaline Mallory bodies in hepatocytes;
- pericellular fibrosis , known as "creeping collagenization" near centrally located veins;
- swelling of hepatocytes;
- neutrophilic infiltration of intra- and interlobular sections of the liver.
In patients with fatty hepatosis, a natural increase in GGTP (g-glutamyl transpeptidase) is recorded, which may also indicate consumption of alcoholic beverages. The levels of albumin, bilirubin and prothrombin remain within normal values, but the alkaline phosphatase and the activity of serum transaminases increase.
In obesity, an increase in ALT and AST is detected, hypertriglyceridemia , dyslipidemia and other manifestations of metabolic syndrome .
If it is impossible to identify the true cause that led to the deposition of fatty bodies in the liver, they speak of an idiopathic or cryptogenic form of hepatosis.
Alcoholic hepatitis and liver cirrhosis
Alcoholic hepatitis, according to the International Classification of Diseases of the Liver Organ, is divided into acute and chronic. The disease is one of the main variants, along with alcoholic fibrosis, which transforms into cirrhosis
.
Acute alcoholic hepatitis - episodes of acute toxic necrosis (acute liver failure of alcoholics) are extremely difficult and often pose a threat to the patient’s life. This form of hepatitis develops in 30% of patients who abuse alcohol for at least 3-5 years, and malnutrition, parental alcoholism, decreased activity of acetal and alcohol dehydrogenase, and decreased HLA B40 antigen play a role.
The relationship between the lack of histocompatibility antigen HLA B40 and the development of chronic active hepatitis with subsequent transition to cirrhosis
.
This form of hepatitis (acute necrosis) can develop against the background of fatty liver
, acute hepatitis, fibrosis or cirrhosis.
In cirrhosis,
the development of acute hepatitis (necrosis) very often leads to decay (parenchymal) and shunt (portocaval) hepatic encephalopathy, which most often ends in death.
Histologically, perivenular damage to hepatocytes, balloon degeneration, their necrosis, alcoholic hyaline (Mallory bodies), leukocyte infiltration, pericellular fibrosis, etc. are observed. Necrosis of hepatocytes in the center of the hepatic hexagonal lobules.
Acute hepatitis often develops in young and middle-aged people after binge drinking with previous long-term alcohol consumption. An acute onset of pain and dyspeptic syndromes is typical, but in some patients the disease can develop gradually.
The most common icteric variant: severe weakness, lack of appetite, nausea, vomiting, jaundice, diarrhea, and sudden loss of body weight. The pain is localized in the right hypochondrium, epigastric region. There may be a fever.
Examination reveals jaundice, hepatomegaly, and fever. The area where the organ is located is painful on palpation and smooth. In some patients, the spleen enlarges, palmar roofing material (erythema), skin spider veins, hand tremors (asterixis), which is a sign of hepatic encephalopathy, mental disorders (lethargy, agitation, hallucinations), ascites resistant to diuretics. Concomitant infections are noted: pneumonia, pyelonephritis, active tuberculosis. The cholestatic variant with skin itching, light-colored feces, and dark urine are rare. The blood is characterized by severe hyperbilirubinemia, hypercholesterolemia, increased activity of alkaline phosphatase, gammaglutamyl transpeptidase, and a slight increase in AST and ALT.
There are fulminant (fulminant) acute alcoholic hepatitis, which is severe, often with an unfavorable prognosis, and a latent variant with an asymptomatic course. Leukocytosis with a shift to the left and a sharp increase in ESR are always observed.
Prognostically unfavorable symptoms are hepatic encephalopathy, hepatorenal syndrome, prolongation of prothrombin time by more than 50%, relapses of acute hepatitis at the stage of established cirrhosis. The prognosis is most favorable for the latent form of acute hepatitis.
Recovery is possible with complete abstinence from alcohol, but this does not always guarantee the absence of subsequent cirrhosis
.
Chronic hepatitis is divided into persistent and active mild, moderate, severe, most often representing stages of progression of acute hepatitis.
Chronic persistent hepatitis is histomorphologically manifested by pericellular and subsinusoidal fibrosis, Mallory bodies, balloon degeneration of hepatocytes. A similar picture without progression of fibrosis can persist for 5-10 years, even with moderate alcohol consumption.
Chronic persistent hepatitis is accompanied by moderate abdominal pain, bloating, anorexia, unstable stools, belching, and heartburn. The liver organ is slightly enlarged and compacted. Diffuse compaction, increase confirmed by ultrasound data. The activity of gammaglutamyl transpeptidase, serum transaminases, and sometimes the thymol test increases moderately.
Chronic active hepatitis has the above-described histomorphological picture of alcoholic hepatitis with the presence of more or less pronounced active fibrosis, sclerosing hyaline necrosis. Abstinence from alcohol for 3-6 months. leads to an improvement in the morphological picture of the type of chronic non-alcoholic hepatitis. Chronic active hepatitis in the presence of autoimmune destruction of the parenchyma is characterized by progression of the process with the transition to cirrhosis
.
Clinical manifestations are more striking than with persistent hepatitis. Jaundice and splenomegaly are more often observed (when transitioning to cirrhosis, the organ can sharply shrink). Bilirubin, gammaglutamyl transpeptidase, immunoglobulin A, moderate thymol test, and blood transaminase activity increase significantly.
There are no direct morphological markers of the alcoholic etiology of diseases of the liver organ, but there are changes that are quite characteristic of the effects of ethanol. This is alcoholic hyaline (Mallory bodies), characteristic ultrastructural changes in hepatocytes, stellate reticuloepitheliocytes. Hyalin is a protein substance synthesized by hepatocytes. In light-optical examination, it has the appearance of eosinophilic masses of various shapes (ribbon-like, reticular, globular, irregular), which are usually localized near the nucleus of the cytoplasm of hepatocytes. After the death of the hepatocyte, it can be located extracellularly. With Mallory's tricolor stain, hyaline accumulations are colored pink.
In electron microscopic examination of biopsies taken from patients with chronic alcoholism, alcoholic hyaline is detected as fibrillar or granular material. Hyaline fibrils are shorter and thicker than normal tonofilaments. The formation of Mallory bodies in hepatocytes has been described in a number of diseases of non-alcoholic etiology: diabetes mellitus, Indian childhood cirrhosis, Wilson-Konovalov disease, primary biliary cirrhosis, liver cancer, after intestinal anastomosis for obesity.
Characteristic ultrastructural changes in hepatocytes and stellate reticuloendotheliocytes reflect the toxic effects of ethanol on the body.
Changes in hepatocytes are represented by hyperplasia, vacuolization of elements of the smooth cytoplasmic reticulum, and the formation of giant mitochondria with an irregular shape. Changes in stellate reticuloepitheliocytes indicate the failure of their phagocytic function: their cytolemma does not form outgrowths, single lysosomes with electron-light content.
Constantly occurring morphological markers of the effects of ethanol on the liver are:
- fatty degeneration of hepatocytes;
- foci of liquefaction necrosis affecting the central parts of the lobules;
- inflammatory infiltrate containing, along with lymphocytes and macrophages, a large number of neutrophilic leukocytes;
- restructuring of the liver organ with the formation of false lobules of a predominantly monolobular type separated by narrow fibrous septa.
An important diagnostic value for chronic hepatitis (alcoholic, like any other etiology) is an ultrasound of the abdominal organs (liver, spleen and other organs), as well as to identify ascites and the size of the portal vein. Doppler ultrasound should be performed to exclude or establish the severity of portal hypertension. Traditionally, radionuclide hepatosplenoscintigraphy continues to be used for diagnostic purposes.
Treatment of hepatosis
Systematization of the treatment of fatty hepatosis, given such a wide variety of causes that cause it, is considered difficult. First of all, treatment of fatty liver hepatosis should be aimed at eliminating the cause that causes the deposition of fatty droplets in the hepatic system. Therapy involves restoring the functioning of the biliary system. For this purpose, drug treatment is prescribed, drugs that negatively affect the functional state of the liver are discontinued. Activities should be aimed at improving the functional state of the liver. The consumption of alcoholic beverages and certain medications is completely excluded.
How to cure? After eliminating the causative factor, symptomatic, course treatment is prescribed.
After complete recovery, the patient should be observed by the attending physician for a year:
- Ultrasound control is carried out once every 6 months;
- Once every 3 months, biochemical analysis for ALT, AST;
- Once every 2 months, an examination is carried out by the attending physician.
Prevention of NAFLD
The main recommendation for preventing this disease is to lead a healthy lifestyle. Maintaining a normal weight and proper nutrition comes first. It is important to eliminate as many risk factors as possible: monitor your body weight, do not overeat, get rid of bad habits.
Prevention measures also include maintaining an active lifestyle, moderate physical activity and proper drinking regimen.
If you notice symptoms of liver hepatosis, you should immediately consult a doctor. Qualified specialists see patients at the CELT clinic; you can contact a gastroenterologist or hepatologist. Experienced doctors will prescribe all the necessary tests, conduct a full examination and select the most effective method of treatment. If you start therapy in the early stages, visible improvement will occur within a short time.
Treatment of fatty liver hepatosis with drugs
Hepatoprotectors that protect liver cells from the damaging effects of negative factors:
- Phosphogliv;
- Rezalut Pro;
- Essentiale Forte N;
- Essliver Forte;
- Heptral;
- Heptor.
Treatment of liver steatosis with herbal preparations:
- Allohol;
- Silimar;
- Gepabene;
- Legalon.
Ursodeoxycholic acid preparations to normalize the functioning of the biliary system;
- Urdoxa;
- Ursofalk;
- Ursosan.
Steatohepatitis is not a death sentence; fatty liver responds well to drug therapy in combination with changes in the patient’s lifestyle.
Treatment of fatty liver hepatosis with folk remedies
Fatty hepatosis can be treated with folk remedies only at the initial stage of the disease; in advanced cases, traditional medicine acts as an addition to the main drug treatment regimen.
You should not self-medicate with folk remedies; all methods of therapy must be discussed with your doctor, this will help avoid complications and allow you not to waste precious time.
Traditional methods are aimed at removing toxins and waste, restoring hepatocytes, improving metabolism in the liver system, losing weight and reducing the percentage of fat. Most medicines contain herbal ingredients.
For the treatment of fatty liver with folk remedies, the following are used:
- dog-rose fruit;
- St. John's wort;
- immortelle flowers;
- bran;
- milk thistle seeds;
- Pine nuts;
- turmeric.
Fatty infiltration of the liver and pancreas responds well to treatment at the initial stage of the disease, so you should not delay treatment, including traditional methods.
Hepatosis in pregnant women
Damage to the liver system in pregnant women is most often observed in the second and third trimesters. Pathological changes are formed against the background of increased load on the organs and multiple changes, some of which are associated with hormonal imbalance.
Cholestatic hepatosis in pregnant women is a dysfunctional liver disorder in which metabolic processes in hepatocytes are disrupted. The cholestatic variant develops due to malfunction of hepatocytes, which disrupts the bile acid . Due to their accumulation in the ducts, bile blood clots form. Blockage of the ducts leads to the penetration of bile components into the bloodstream.
Pregnant women complain of severe itching , especially in the palms of the hands. The forum for expectant mothers is inundated with questions about the prognosis of pathology and the risk of negative effects on the health of the fetus. Timely diagnosis and well-chosen treatment make the prognosis favorable.
Acute fatty hepatosis in pregnant women is extremely rare and is characterized by a very severe course. Maternal and perinatal mortality rates are excessively high. The acute version of hepatosis is difficult to diagnose due to the blurred clinical picture and the masking of the pathology as other liver diseases.
Symptoms and stages
NAFLD is often asymptomatic at first. The main stages of the disease are listed below6,7.
- Steatosis. Symptoms are almost completely absent. Steatosis is often discovered by chance when the patient seeks help for other reasons. However, fatigue, changes in appetite, and heaviness or discomfort in the right hypochondrium may occur6,7.
- Steatohepatitis. It can also be almost asymptomatic or accompanied by fatigue, weakness and discomfort or pain in the right side of the abdomen, not associated with meals7.
- Fibrosis. This is a condition in which connective tissue takes the place of hepatocytes.
- Cirrhosis. Serious impairment of liver function, which may result in liver failure. Spider veins may appear, the skin and mucous membranes turn yellow, the skin becomes dry, and itching occurs. There may be other symptoms: ascites (accumulation of fluid in the abdominal cavity), varicose veins of the esophagus and stomach and, as a result, bleeding6,7.
Diet for fatty hepatosis
Diet 5th table
- Efficacy: therapeutic effect after 14 days
- Duration: from 3 months or more
- Cost of products: 1200 - 1350 rubles per week
Diet 8 table
- Efficiency: weight loss to the required level
- Time frame: long-term, until the expected effect is achieved
- Cost of products: 1120 - 1230 rubles per week
Diet for fatty liver hepatosis
- Efficacy: therapeutic effect after 3-6 months
- Terms: 3-6 months
- Cost of products: 1500-1600 rubles. in Week
Therapeutic nutrition is based on minimizing simple carbohydrates and animal fats in the diet. The diet is aimed at reducing insulin resistance and weight correction. Reducing body weight by even 10% significantly accelerates lipid and carbohydrate metabolism. Main directions in nutrition:
- Daily calorie content is 2800-3200 kcal. Calorie intake should increase due to fruits and vegetables.
- The daily amount of protein is 100-130 g. Animal proteins should account for 80 g, and the rest should be plant proteins.
- Half of the diet should be carbohydrates. The share of simple carbohydrates is no more than 25%.
- The proportion of fat is 0.8-0.9 g per 1 kg of weight. Vegetable fats should make up 60% of the diet.
Consequences of fatty liver
Long-term steatosis can be complicated by fibrosis with the risk of further degeneration into cirrhosis. It is important to understand that fatty hepatosis (fatty liver) is a completely reversible process - just reconsider your diet and lifestyle.
Prolonged exposure to several negative factors at once, as well as the complete lack of adequate therapy, provokes the transition of hepatosis to a severe form. The rate of development of fibrosis increases significantly if the patient has obesity , diabetes mellitus , viral hepatitis , as well as abuse of alcohol-containing beverages.
Fibrosis is also considered a reversible process, which is characterized by the growth of scar, connective tissue in place of damaged cells of the liver system - hepatocytes. Fibrosis is a protective mechanism by which the body tries to restrict healthy tissue from being damaged. Fibrosis responds well to treatment, but most often due to the lack of adequate therapy, liver cirrhosis .
Cirrhosis is an irreversible process of replacing liver tissue with coarse scar tissue. Characterized by a significant decrease in the number of functioning cells. At the initial stage, it is possible not only to stop the pathological process, but even to partially restore damaged structures. However, in severe cases, cirrhosis is fatal. The only possible way to save life is to transplant a donor liver.