Pancreatitis is inflammation of the pancreas.
The pancreas is the second largest gland in the digestive system (after the liver). It plays an extremely important role in the digestion process.
The pancreas produces pancreatic juice, which contains more than 30 different enzymes. It contains components necessary for the breakdown of fats, proteins, and carbohydrates. Up to 800 grams are produced daily. pancreatic juice, which flows through the pancreatic duct into the duodenum. To prevent the juice from corroding the tissue of the pancreas itself, enzymes are initially produced in an inactive form. To transform them into an active form and start the digestive process itself, it is necessary to interact with bile, which normally should occur in the duodenum. If bile enters the pancreatic duct or if the outflow of pancreatic secretions is obstructed, premature activation of enzymes occurs, which leads to the process of self-destruction of the pancreas. The gland begins to digest itself - tissue necrosis begins, pancreatitis occurs.
Forms of pancreatitis
Acute – characterized by acute girdling pain in the upper abdomen. Pain often appears after eating fatty foods or alcohol. Unpleasant sensations can be either barely noticeable or unbearable, radiating to the scapula or sternum. Nausea, vomiting, and stool disturbances are observed. Due to the obstructed flow of bile, the skin takes on a yellowish color.
Chronic - the main localization of pain is on the upper part of the abdominal wall with irradiation to the back, chest (left side), lower abdomen. Unpleasant sensations occur after eating heavy fatty foods, alcoholic drinks, and constant stress.
The development of chronic pancreatitis is characterized by nausea, loss of appetite, bloating, bowel dysfunction, and sometimes vomiting.
The chronic form of the pathology differs from the acute form by periods of remission and exacerbation. As the disease progresses, periods of exacerbation become more frequent; intestinal disorders, disturbances in normal digestion, and weight loss are possible.
Chronic pancreatitis often causes complications (stomach bleeding, cancer, cysts and abscesses, liver damage, diabetes mellitus, enterocolitis). That is why you need to take the disease seriously and, at the slightest suspicion of the development of inflammation, consult a doctor.
Etiology
The etiological factors of pancreatitis are very diverse - metabolic, mechanical, infectious, vascular. Often the disease occurs as a result of the interaction of several factors. The etiology of AP is determined only in 75% of patients.
Chronic pancreatitis is classified according to etiology and risk factors according to the TIGAR-O classification (Table 1).
Table 1. Etiological classification of chronic pancreatitis (TIGAR-O)
| Toxic-metabolic |
| Alcohol; Tobacco, smoking; Hypercalcemia (hyperparathyroidism); Hyperlipidemia; Chronic renal failure; Drugs and toxins. |
| Idiopathic |
| Early start; Late start; Tropical calcific pancreatitis, fibrocalcular pancreatic diabetes. |
| Genetic |
Autosomal dominant
|
| Autoimmune |
| Autoimmune pancreatitis type 1 (IgG4 positive); Autoimmune pancreatitis type 2 (negative IgG4). |
| Recurrent (reversible) and acute |
| Ponecrotic (acute); Reversible sharp:
Ischemic (postoperative, hypotensive); Infectious (viral); Chronic alcoholism; Poradiative; Diabetes. |
| Obstructive |
Benign pancreatic duct stricture:
Malignant stricture; Periampullary carcinoma; Pancreatic adenocarcinoma. |
Table 2. Rare causes of pancreatitis
| Nosology | Characteristics | Diagnostics |
| Metabolic pancreatitis | Hypertriglyceridemia and hypercalcemia | OP or HP |
| Drug-induced pancreatitis | Azathioprine, 6-mercaptopurine, sulfonamides, estrogens, tetracycline, valproic acid, antiretroviral drugs | OP or HP |
| Autoimmune pancreatitis | Focal or diffuse enlargement of the pancreas, hypotensive pancreatic shunt, expansion of the papillary part due to lymphoplasmocytes p. | HP |
| Hereditary pancreatitis | Usually occurs at a young age, gene mutations are detected | Acute recurrent pancreatitis |
| Pancreatitis after the procedure | Endoscopic retrograde cholangiopancreatography was recently performed | Most often OP |
| Pancreatitis with sedimentation of bile (sediment) | Bile deposits and small stones (microlithiasis) | Most often OP |
| Pancreatitis Paraduodeninio groove ( groove ) | Fibrous formations between the head of the pancreas and the thickened wall of the duodenum, leading to duodenal stenosis, cystic changes in the pancreaticoduodenal groove or duodenal wall, pancreatic and bile duct stenosis | Exclusively HP |
| Duodenal diverticulum | Periampullary diverticulum, wind deformation | OP>HP |
| Traumatic pancreatitis | Direct trauma to the pancreas, intrapancreatic hematoma, rupture of the pancreas with fluid around it | OP or HP |
| Infectious pancreatitis | Various infectious factors: viruses, bacteria, fungi. | Most often in OP |
| Ischemic pancreatitis | Pancreatitis due to circulatory disorders, arterial hypotension, cardiogenic shock | OP or HP |
Reasons for the development of pancreatitis
The disease develops due to damage to pancreatic tissue. This happens for the following reasons:
- alcohol and tobacco abuse
- abdominal trauma, surgery
- uncontrolled and long-term use of medications: antibiotics, hormonal drugs, corticosteroids, some diuretics
- intoxication with food products, chemicals
- genetic predisposition
- improper diet with a predominance of spicy and fatty foods and long breaks between meals
Symptoms of pancreatitis
Manifestations of pathology vary depending on the form - acute or chronic pancreatitis. In acute pancreatitis the following are observed:
- The pain is intense, constant, the nature of the pain is described by patients as cutting, dull.
- High body temperature, high or low blood pressure - the patient’s well-being quickly deteriorates due to the rapid development of the inflammatory process.
- Pale or yellowish complexion.
- Nausea and vomiting - dry mouth and a white coating appear, attacks of vomiting do not bring relief. The most correct step at this moment is to fast; any food intake can only worsen the situation.
- Diarrhea or constipation - stool in acute pancreatitis is most often foamy, often with a foul odor, with particles of undigested food. On the contrary, there are constipation, bloating, and hardening of the abdominal muscles, which may be the very first signal of an acute attack of pancreatitis.
- Bloating – the stomach and intestines do not contract during an attack.
- Shortness of breath - appears due to loss of electrolytes during vomiting.
Chronic pancreatitis is characterized by the following symptoms:
- Abdominal pain - may be girdling or have a clear localization radiating to the back. Appears after eating.
- Intoxication of the body - general weakness, loss of appetite, tachycardia, increased body temperature, and decreased blood pressure appear.
- Endocrine disorders - ketoacidosis, diabetes mellitus, tendency to hypoglycemia. Bright red spots may also appear in the abdomen, back, and chest, which do not disappear with pressure.
With a long course of the disease, the patient gradually develops anemia, weight loss, dry skin, brittle hair and nails, symptoms of vitamin deficiency, and increased fatigue.
Publications in the media
Regarding the treatment of this disease, you can contact the Department of X-ray surgical methods of diagnosis and treatment of the Clinic of Faculty Surgery named after. N.N. Burdenko
Acute pancreatitis is an inflammatory-necrotic lesion of the pancreas caused by enzymatic autolysis caused by various reasons. Etiology • Diseases of the biliary tract (cholelithiasis, choledocholithiasis, stenosis of the papilla of Vater) • Alcohol excess and rich fatty foods • Surgical interventions on the pancreas and adjacent organs, abdominal trauma with damage to the pancreas • Acute circulatory disorders in the gland (vessel ligation, thrombosis, embolism) • Severe allergic reactions • Diseases of the stomach and duodenum (peptic ulcer, parapapillary diverticulum, duodenostasis) • Endoscopic retrograde cholangiopancreatography • Viral infections (mumps) • Drugs (azathioprine, estrogens, thiazides, furosemide, sulfonamides, GC and valproic acid) • Hypercalcemia, hyperparathyroiditis, uremia • Kidney transplantation.
Pathogenesis • Enzymatic autolysis of gland tissue with the development of a demarcation inflammatory reaction and the formation of microthrombi • The progressive course of the disease is characterized by pancreatogenic toxemia, hemodynamic disturbances, inhibition of the activity of parenchymal organs and post-necrotic complications. Pathomorphology. Autolysis, interstitial edema, hemorrhages, cellular and fat necrosis are noted in the pancreas.
Clinical and morphological classification • Edematous form of pancreatitis • Fatty pancreatic necrosis • Hemorrhagic pancreatic necrosis. Clinical picture • Constant severe girdling pain and pain in the epigastric region, accompanied by nausea and vomiting • The abdomen on palpation is painful, tense and moderately swollen • Positive symptoms of Shchetkin-Blumberg, Voskresensky, Mayo-Robson, Razdolsky. The severity of symptoms depends on the form of the disease, the degree of intoxication and complications • The skin and mucous membranes are often pale, sometimes cyanotic or icteric. Mondor's syndrome, Gray Turner's symptom, and Cullen's symptom appear. The body temperature with edematous pancreatitis is normal. • With pancreatic necrosis, pain is most pronounced in the epigastric region. With the progressive course of pancreatic necrosis, on the 7th–10th day of the disease, abdominal pain decreases due to the death of sensory nerve endings in the pancreas. Also characteristic is a serious condition, vomiting, increased body temperature (37.7–38.3 °C), cyanosis of the skin, tachycardia, arterial hypotension, oliguria, and symptoms of peritonitis. Symptoms of Grunwald and Davis are characteristic. Often, symptoms of intoxication prevail over local manifestations of the disease • With parapancreatic phlegmon and abscess of the pancreas, deterioration of the condition is noted: increased body temperature, chills, inflammatory infiltrate in the upper floor of the abdominal cavity, leukocytosis with a shift in the leukocyte formula to the left • Severe inflammation and necrosis of the pancreas can cause bleeding into the retroperitoneal space, which can lead to hypovolemia (arterial hypotension, tachycardia) and accumulation of blood in soft tissues. Laboratory tests • CBC - leukocytosis (10–20109/l) with a shift of the leukocyte formula to the left • Biochemical blood test •• Increased content of α-amylase - 95% of cases (decreases with pancreatic necrosis) •• Increased ratio of amylase to creatinine clearance (higher 5%), which is normally 1–4% •• Increase in Ht to 50–55% •• Moderate increase in ALT and/or AST with concomitant alcoholic hepatitis or choledocholithiasis •• Moderate increase in ALP concentration with concomitant alcoholic hepatitis or choledocholithiasis •• Hyperbilirubinemia - in 15–25% of patients •• Increased levels of serum lipase •• Hyperglycemia in severe cases •• Hypocalcemia on the first day of the disease.
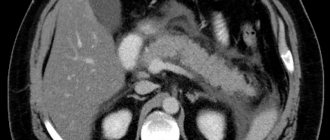
Special studies • Plain radiography of the abdominal organs - signs of dynamic intestinal obstruction, accumulation of gas in the area of the lesser omentum (abscess inside or near the pancreas); displacement of the abdominal organs (exudation and swelling of the lesser omentum and organs adjacent to the pancreas); blurred shadows of the iliopsoas muscles with retroperitoneal necrosis of the pancreas • X-ray contrast study with a barium suspension is used to diagnose pathology of the upper gastrointestinal tract: an increase in the radius of the horseshoe of the duodenum due to edema of the pancreas is possible; with relaxation duodenography, a pillow symptom can be detected • X-ray examination of the chest organs - pleural effusion (rare) • Ultrasound of the pancreas - decreased echogenicity, edema, thickening in the anteroposterior direction, virtual absence of tissue between the pancreas and the splenic vein • CT scan of the pancreas (high resolution) • Selective celiacography: with edematous pancreatitis - increased vascular pattern; with pancreatic necrosis - narrowing of the lumen of the celiac trunk, deterioration of the blood supply to the gland with areas of vascular bed exclusion • Radioisotope study with pancreatic necrosis - lack of fixation of the isotope in the pancreas, decreased excretory function of the liver • Endoscopic retrograde cholangiopancreatography • Laparoscopy - foci of fat necrosis, hemorrhage and edema of the gastrocolic ligaments, exudate in the abdominal cavity (serous or hemorrhagic), assess the condition of the gallbladder.
Differential diagnosis • Penetrating or perforating gastric and/or duodenal ulcer • Acute cholecystitis • Choledocholithiasis • Mesenteric vascular obstruction and/or infarction • Perforation of internal organs • Obstructive intestinal obstruction • Aortic aneurysm • Pancreatic cancer • Acute appendicitis • Ectopic pregnancy • Posterior MI • Hematoma of the muscles of the anterior abdominal wall • Blunt trauma or penetrating injury to the spleen.
TREATMENT Diet. Fasting is prescribed for up to 7 days; after reducing the severity of pain, you should eat small meals with a high carbohydrate content, limiting fats and proteins (to reduce the secretion of pancreatic enzymes). Expansion of the diet in accordance with the patient's condition. Management tactics • For edematous form of pancreatitis •• Nasogastric tube and gastric drainage - for vomiting, nausea •• IV solutions of glucose, Ringer-Locke (1.5–2 l), rheopolyglucin (lowers blood viscosity, prevents the aggregation of formed blood elements, leading to improved microcirculation and reduced swelling of the pancreas), hemodesis (binds toxins and quickly removes them in the urine) •• Lytic mixture: trimeperidine, atropine, diphenhydramine, procaine •• Protease inhibitors: aprotinin •• Moderate forced diuresis •• To relieve spasm of the sphincter of Oddi and blood vessels - papaverine hydrochloride, atropine, platyphylline, drotaverine, aminophylline •• Antihistamines (promethazine, chloropyramine, diphenhydramine) - to reduce vascular permeability, analgesic and sedative effects •• Perinephric procaine blockade and splanchnic nerve blockade for relief inflammatory process and pain reaction, reducing the external secretion of the pancreas, normalizing the tone of the sphincter of Oddi, improving the outflow of bile and pancreatic juice. These manipulations can be replaced by the administration of 0.5% procaine solution intravenously •• On 3–5 days, patients are discharged, as a rule, in satisfactory condition.
• For pancreatic necrosis (treatment of fatty and hemorrhagic pancreatic necrosis is carried out in the intensive care unit) •• For rapid restoration of blood volume and normalization of water and electrolyte metabolism - intravenous administration of solutions of glucose, Ringer-Locke, sodium bicarbonate, as well as rheopolyglucin, hemodez, and then plasma, albumin with simultaneous stimulation of diuresis •• Lytic mixture, protease inhibitors, cytostatics •• Cytostatics (for example, fluorouracil) have an anti-inflammatory, desensitizing effect and (most importantly!) inhibit the synthesis of proteolytic enzymes •• Protease inhibitors (aprotinin) suppress the activity of trypsin, kallikrein, plasmin, forming inactive complexes with them. They are administered IV every 3–4 hours in loading doses (for example, aprotinin up to 80–320 thousand units/day) •• To force diuresis - IV mannitol 15% solution 1–2 g/kg or furosemide 40 mg •• For an infectious process (for example, in the lungs, bile ducts or urinary tract) - broad-spectrum antibiotics. Data on the effectiveness of antibiotics for the prevention of purulent complications in the pancreas are contradictory. In case of an infectious lesion of the pancreas, antibiotic therapy is necessary •• To reduce the external secretion of the pancreas, cold applied to the epigastric region, aspiration of gastric contents, intragastric hypothermia are indicated •• UV laser irradiation of blood (15 min each, 2-10 sessions) relieves pain and inflammation , improves the rheological properties of blood and microcirculation •• Extracorporeal detoxification methods (plasmapheresis, lymphosorption) are aimed at removing pancreatic enzymes, kallikrein, toxins, and cellular decay products from the body •• Close-focus radiation therapy has an anti-inflammatory effect. 3–5 sessions are performed •• In case of progression of signs of peritonitis, surgical drainage of the cavity of the lesser omentum and abdominal cavity is indicated.
Surgical treatment is carried out in case of • Ineffectiveness of conservative therapy - drainage of the omental bursa and abdominal cavity, necrectomy • Inability to exclude acute surgical disease of the abdominal organs • Symptoms of diffuse peritonitis • Combination of acute pancreatitis with destructive cholecystitis • Pancreatitis caused by an impacted gallstone - endoscopic retrograde cholangiopancreatography , sphincterotomy and stone removal • Severe blunt trauma or penetrating injury to the abdomen.
Complications • Toxic •• Pancreatic shock •• Delirium •• Hepatic-renal and cardiovascular failure • Post-necrotic •• Pancreatic abscess •• Phlegmon of the retroperitoneal tissue •• Peritonitis •• Erosive bleeding •• Cysts and pancreatic fistulas. Prognosis • Signs detected upon admission •• Age over 55 years •• Leukocyte count in peripheral blood more than 16109/l •• Fasting blood glucose concentration above 11 mmol/l •• LDH activity in the blood above 350 IU/l •• AST content more than 25 IU/l • Signs detected 48 hours after admission •• Drop in Ht by more than 10% •• Increase in blood urea nitrogen content to 1.8 mmol/l •• Serum calcium concentration below 2 mmol /l •• paO2 below 60 mm Hg •• Base deficiency more than 4 mEq/l •• Loss of fluids into the third space - more than 6 l • If less than 3 of the above signs are present, mortality is 1%, 3–4 - 16% , 7 - 90%, more than 7 - 99% • 85–90% of cases of edematous form of acute pancreatitis resolve spontaneously, mortality 3–5%.
ICD-10 • K85 Acute pancreatitis • K90.3 Pancreatic steatorrhea
First aid for an attack of pancreatitis
To reduce pain, you can use a heating pad filled with cold water. It needs to be applied to the abdominal area, namely to the epigastric region (the area under the xiphoid process, corresponding to the projection of the stomach onto the anterior abdominal wall). This allows you to reduce the intensity of pain, slightly reduce swelling and inflammation.
The patient must comply with the hospital regime. This will reduce blood flow to the organ, and therefore reduce inflammation.
Eating is prohibited. The digestion process can cause more severe pain, nausea and vomiting. And the diet will reduce the production of enzymes that increase the inflammatory response and pain. You need to fast for 3 days. You can drink clean water without gases.
It is imperative to call a doctor for an examination, even if the patient is not exactly sure that this is an attack of acute pancreatitis. As we already know, this pathology can subside and then rapidly recur. At this time, you can take a painkiller to reduce discomfort.
Complications after taking medications
Medicines for pancreatitis, like any medicine, can lead to complications. Antibiotics - for digestive upset, non-steroidal anti-inflammatory drugs - for complications in the gastrointestinal tract and cardiovascular system. Enzyme preparations can cause allergies and lead to iron deficiency. Antisecretory drugs, although they are considered drugs with a minimum of side effects, can cause withdrawal syndrome: the appearance of heartburn and sometimes pain in the sternum after stopping their use. Even vitamins, if taken immoderately and without prior testing, can become not just a useless, but also a dangerous supplement.
Diagnosis of the disease at the private medical clinic “Medunion”
Diagnosing this disease is not difficult, since the first signs speak for themselves. However, in order to prescribe adequate treatment, it is necessary to determine the form of the disease. To do this, the doctor performs laparoscopy - a method that allows you to examine the abdominal cavity from the inside using a special instrument.
If acute pancreatitis is suspected, laboratory tests are performed:
- General blood analysis
- Blood chemistry
- Analysis of urine
- Stool analysis
- Ultrasound, MRI or radiography of the abdominal organs
- Computed tomography according to indications
In the chronic form, the same studies are carried out, but it is better to take tests during the period of exacerbation of the disease.
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Ultrasound of the abdominal organs (liver, gall bladder, pancreas, spleen) | 3 800 |
| Pancreatocholangiography | 4 500 |
| MSCT of the abdominal cavity and retroperitoneal space of the abdomen | 6 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Treatment of acute pancreatitis
If acute pancreatitis is detected, the patient should be hospitalized immediately. Treatment should take place in a hospital setting, as this condition is very dangerous.
To relieve pain, antispasmodics are taken; in difficult cases, the contents of the stomach are pumped out to relieve the load on the gland.
In case of exacerbation of pancreatitis, patients require hospitalization with daily monitoring of blood parameters, water balance, leukocyte count, and enzyme levels in the blood serum during the first week. In the first 1–3 days, fasting and taking alkaline solutions every 2 hours are recommended.
During an exacerbation of chronic pancreatitis, the patient is shown therapy similar to the acute process. The patient must follow a diet throughout his life and take drugs from the group of antispasmodics and drugs that normalize the secretory function of the organ.
The most important thing in the chronic form of the disease is to maintain a diet that involves excluding fatty and fried foods from the diet. At the slightest violation of the regimen, the patient may experience discomfort and nausea. For intense pain, the doctor prescribes antispasmodics. Antisecretory therapy can be used for a short course.
Summary
Advantages of complex minimally invasive surgical technology for the treatment of acute destructive pancreatitis:
- Prevention of the development of pancreatic necrosis and purulent complications in destructive pancreatitis (abortive course of acute pancreatitis).
- Reduced mortality caused by bleeding, purulent-septic complications, and general surgical trauma.
- Reducing the number of complications associated with intraoperative bleeding.
- Reducing the amount of secondary intrasecretory insufficiency.
- Reducing patient disability.
- Good cosmetic effect (no laparotomy or lumbotomy scars, including those from wounds healed by secondary intention, no need for subsequent plastic surgery of skin wounds and hernias).
Author: Ph.D. Novikov S.V.
Diet for pancreatitis
For any form of the disease, the patient is prescribed a strict diet “Table No. 5p”, according to which it is forbidden to eat spicy and fried foods. All dishes are steamed, boiled or baked. Alcohol and smoking are also prohibited.
It is also necessary to limit salt intake and eat small portions 6 times a day. Dishes should always be served warm. It is necessary to exclude all products with a high content of extractives or essential oils (fish, meat broths, cocoa, coffee, etc.), fresh berries, vegetables, herbs, fruits, sour juices, carbonated drinks, marinades.
Surgery
The operation involves removing dead tissue and cleaning the abdominal cavity. Intervention is indicated if the patient has a total or subtotal infection of an infectious nature, a purulent abscess, false cysts, or peritonitis.
If the disease proceeds without infection, surgery is avoided.
Surgeons prefer to resort to minimally invasive techniques, since open abdominal surgery has a high mortality rate and is often accompanied by secondary infection.