Cataracts are a serious pathology that, without proper treatment, can lead to complete loss of vision over time. Most often it appears in both eyes.
This disease of the visual system is characterized by clouding of the lens of the eye. The problem can be either congenital - diagnosed immediately after birth, or acquired - can appear at any age.
Congenital cataracts usually occur due to health problems in the pregnant woman and genetic abnormalities. Taking medications, bad habits, and prolonged exposure to a toxic environment also have an impact.
Acquired cataracts can appear at any age, but problems most often occur after 55 years of age. At this age, natural biological processes begin, the lens loses its elasticity, becomes cloudy and dense. In addition to age-related changes, other factors may influence the early appearance of cataracts:
- long-term use of medications, such as steroid therapy;
- other diseases of the visual system;
- eye and head injuries;
- X-ray irradiation;
- negative effects of ultraviolet and infrared rays;
- poor lifestyle, vitamin deficiency.
If we talk about natural processes, cataracts develop in every person and it is only a matter of time. Some people may experience significant changes in just a few months, while others may not be aware of the presence of the disease for many years.
Treatment with conservative methods is ineffective and makes no sense. The only way to get rid of the problem is through cataract surgery.
Primary cataract – what is it?
Cataract is an age-related disease that manifests itself under the influence of negative factors: genetic disruptions, endocrine disorders, eye injuries, taking potent medications, concomitant ophthalmological diseases, etc. Hereditary predisposition also plays a significant role in the development of the disease.
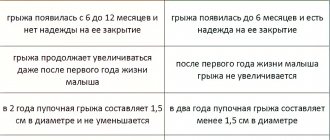
There are 4 stages of cataract development:
- Initial, in which only peripheral damage to the lens is diagnosed.
- Immature, in which the clouding gradually spreads to the optical zone. At this stage, the patient notices a decrease in visual acuity. Surrounding objects are visible as if through a foggy haze.
- Mature. The area of opacity covers the entire lens. At this stage, the patient no longer sees anything, but only feels light.
- Overripe. Complete blindness and disintegration of the lens occurs. At this stage, the damaged fibers disintegrate.
Cataract ranks first in the world among diseases leading to vision loss.
Publications in the media
Congenital cataracts are observed in 5 cases out of 100,000 newborns; it accounts for 10–38% of cases of childhood blindness.
Classification • Coronal (coronary) - opacities are located radially in the deep layers of the cortex of the peripheral parts of the lens and are club-shaped, light gray or greenish-blue in color • Fusiform - fusiform opacities are located along the axis of the lens • Discoid - disc-shaped opacities are located between the nucleus and posterior pole of the lens • Zonular (layered) - lens opacities are located in the form of 1-3 concentric layers around its core • Stellate cataract (lens suture) is characterized by the presence of point opacities in the area of the embryonic sutures of the lens, forming a star figure • Cataract of the anterior embryonic suture - stationary cataract , characterized by multiple point white opacities in the area of the anterior embryonic suture of the lens • Polar cataract - a small round grayish-white opacification, often of a layered structure, located at one of the poles of the lens • Pyramidal cataract - polar cataract, opacification in the form of a cone, the apex is directed towards the pole lens
Genetic aspects. Types and genes: • 182500, SORD gene, 15q15; • blue, type 1, CCA1, 115660, 17q24; • blue, type 2, 601547, CRYB2 (123620), 22q11.2 q12.2; • zonular Marner, CTM, 116800, 16q22.1; • zonular powder, type 1, 116200, GJA8, CX50, CAE1, 600897, 1q12 q21; • zonular powder, type 2, CAE2, CZP2, 601885, 13q11 q12; • zonular, CCZS, 600881, 17q11 q12; • with hyperferritinemia 600886, FTL, 134790, 19q13.3 q13.4; • with microphthalmia, CATM, 156850, 16p13.3; • full, X-linked (?), CCT, 302200; • Volkmann, CCV, 115665, 1pter p36.13; • with late corneal dystrophy, PAX6, AN2, 106210, 11p13; • Coppock similar, CRYGA, CRYG1, 123660, 2q33 q35; • polar posterior, CPP, 116600, 1pter p36.1; • polar anterior, type 1, CTAA1, 115650, 14q24 qter.
Risk factors • Metabolic disorders: diabetes in the mother, galactosemia in the fetus • Infectious diseases of the mother in the first trimester of pregnancy: rubella, herpes, mumps, toxoplasmosis, etc.
Clinical picture • The disease is often asymptomatic • Sometimes parents notice disturbances in gaze fixation or strabismus in the child due to the lack of cortical control over the friendly contractions of the external muscles of the eye • Leukocoria (light reflection from the pupil - a visible manifestation of clouding of the lens), nystagmus, signs of the underlying disease ( eg, Down syndrome, rubella) • Lens opacities are detected immediately after birth or within 3 months.
Differential diagnosis • Tumors of the external part of the visual analyzer, pathways • Retinopathy.
Treatment • The most optimal surgical treatment is in the first months of life (cataract extraction) under anesthesia, which allows for the correct formation of the visual cortex and the retina itself, as well as adequate development of muscle coordination necessary for binocular vision •• Implantation of an intraocular lens is not indicated, since the eye is changes the refraction during the growth process •• For bilateral cataracts with visual acuity less than 0.005, not corrected with lenses, surgical intervention is indicated at the age of 2 to 6 months •• With less severe cataracts (visual acuity - below 0.3), object vision is possible, therefore, the operation is performed at the age of 2–5 years •• Postoperative care: to combat amblyopia, it is necessary to wear a patch on the healthy eye for a long time. Correction of the refraction of the operated eye is indicated, frequent repeated examinations of visual acuity •• If visual acuity is above 0.3 (improvement to 0.4 with pupil dilation), surgical extraction is not performed • With delayed surgical treatment, instillation of mydriatic agents into the eye is necessary 1-2 r/ weeks until surgery to ensure the full development of the retina, which often suffers from a lack of light reaching it, to prevent nystagmus, strabismus, and amblyopia.
Forecast. If congenital cataracts are not detected in a timely manner, the prognosis is often unfavorable due to the high risk of developing amblyopia.
ICD-10 • Q12.0 Congenital cataract.
Application. AMC syndrome (from: A taxia- M icrocephaly- C ataract, ataxia-microcephaly-cataract syndrome, 208870, r). Clinically: ataxia, mental retardation, microcephaly, congenital cataract, nystagmus.
What to do when diagnosing cataracts at an early stage
The only effective and sufficient method of treating cataracts is surgery, during which the clouded lens is removed and an implant is installed in its place. Modern implants can restore vision. The patient notices the result almost immediately after the operation, which lasts no more than 15 minutes. Within an hour, vision returns, but not yet in full; the maximum effect will occur after the prosthesis has completely engrafted and the wound has healed.
Does this mean that initial cataracts should not be treated, since the patient is not in danger of going blind? Not really. Symptomatic treatment can be prescribed, as well as eye drops that prevent the development of the disease. Most often at this stage, general strengthening drugs, vitamins, minerals, antioxidants, and catalin are prescribed. However, these remedies can only slightly slow down the regression, but not stop it completely. Cataracts will inevitably progress and, if the patient refuses surgery, eventually complete blindness will occur.
It is also not recommended to perform surgery at the initial stage. Since the damage to the lens is still small, it does not cause physical discomfort and does not cause an aesthetic defect. Surgical intervention is indicated at the second stage, when the lesion is already noticeable and interferes with normal life activities. The doctor will recommend surgery if there is 50% damage to the lens. If the patient wishes, the implant can be installed at the first external signs of the disease.
Important : after the initial diagnosis of cataracts, it is necessary to undergo regular examinations by an ophthalmologist.
Since in the later stages the cloudy lens becomes deformed, which leads to an increase in IOP and the development of glaucoma. It is also possible that other concomitant diseases will appear that will not be noticed by the patient himself against the background of cataract symptoms. The Clean View clinic provides a full range of procedures for successful cataract removal. More details by phone +7 (499) 141-13-75.
Reviews
All reviews
Successful surgery to correct strabismus
5 ★
24.03.2016
Dear Natalia Ivanovna! I accidentally visited the website of this wonderful clinic again, due to the fact that I advised my friend to contact it, since they work here with great professionals. I would like to once again express my gratitude to you for your attentive and kind attitude and for correcting my strabismus two years ago. Thanks a lot!
This is the second time our family has contacted you.
5 ★
05.03.2016
Natalya Ivanovna. This is the second time our family has contacted you. Thank you for your professional work, attentiveness and sensitive attitude.
Review from Vera
5 ★
08.05.2020
Many thanks to doctor Natalia Ivanovna Fomenko for her quick, clear answer to my question. She explained everything in detail and gave recommendations. She advised me to carry out the necessary examination and take the necessary tests. Together with my 90-year-old mother, we thank you for your attentive and responsible attitude.
Cataract surgery was performed, everything went well
5 ★
10.04.2017
Dear Natalya Ivanovna, we express our gratitude for your experience and attitude towards our family! We have turned to the Moscow Eye Office for help more than once. The first time we came was on the advice of a friend. The cataract was operated on, everything was successful. Thanks to all the doctors with whom we communicated during all this time.
Successful surgery to correct strabismus
5 ★
24.03.2016
Dear Natalia Ivanovna! I accidentally visited the website of this wonderful clinic again, due to the fact that I advised my friend to contact it, since they work here with great professionals. I would like to once again express my gratitude to you for your attentive and kind attitude and for correcting my strabismus two years ago. Thanks a lot!
This is the second time our family has contacted you.
5 ★
05.03.2016
Natalya Ivanovna. This is the second time our family has contacted you. Thank you for your professional work, attentiveness and sensitive attitude.
Review from Vera
5 ★
08.05.2020
Many thanks to doctor Natalia Ivanovna Fomenko for her quick, clear answer to my question. She explained everything in detail and gave recommendations. She advised me to carry out the necessary examination and take the necessary tests. Together with my 90-year-old mother, we thank you for your attentive and responsible attitude.
Cataract surgery was performed, everything went well
5 ★
10.04.2017
Dear Natalya Ivanovna, we express our gratitude for your experience and attitude towards our family! We have turned to the Moscow Eye Office for help more than once. The first time we came was on the advice of a friend. The cataract was operated on, everything was successful. Thanks to all the doctors with whom we communicated during all this time.
Author:
Dagaev Adam Huseinovich 5/5 (1 rating)
Honey. portal:
Causes of optic nerve atrophy
The etiological causes of optic neuropathy can be various chronic or acute eye diseases, pathology of the central nervous system, ophthalmic trauma, general intoxication, severe systemic diseases (endocrine, autoimmune, etc.).[2]
Among the actual ophthalmopathic factors, under the influence of which optic nerve atrophy can begin, glaucoma of various forms is in the lead; pigmentary retinal (retinal) dystrophy; all kinds of blockages of the retinal arteries and drainage veins (for example, occlusion of the central retinal artery); severe myopia; uveitis, retinitis, neuritis, orbital vasculitis and other inflammations. In addition, the optic nerve can be involved and atrophy during the development of oncopathology, in particular, with primary orbital cancer, meningioma or glioma of the optic nerve, neuroma or neurofibroma, osteosarcoma, sarcoidosis.
Diseases of the central nervous system that provoke or “trigger” atrophic processes in the optic nerve include mainly pituitary tumors, chiasms (compressing the optic chiasm), infectious and inflammatory processes of the meninges (encephalitis, meningitis, arachnoiditis) and general brain abscess, demyelinating diseases (eg, multiple sclerosis), traumatic brain injuries and wounds in the maxillofacial area, especially with direct mechanical damage to the optic nerve.
Fig. 2 Pale optic nerve discs (OND) with atrophy in the fundus
In some cases, systemic atherosclerosis, chronic malnutrition and exhaustion, vitamin deficiencies and anemia, poisoning with toxic substances become the provoking background and pathogenic soil of optic neuropathy (the most striking examples are frequent methyl poisoning when consuming surrogate alcoholic beverages, as well as intoxication with nicotine, insecticides, and drugs ), massive blood loss (for example, with extensive internal hemorrhages), diabetes mellitus and other endocrinopathy, lupus erythematosus, Wegener's granulomatosis and other autoimmune disorders.
Optic nerve atrophy can be a complication and outcome of severe infections, the causative agents of which in various cases are bacteria (syphilis, Koch’s tuberculous mycobacterium), and viruses (measles, rubella, influenza, herpes, even “ordinary” adenoviral ARVI), and parasites (intracellular toxoplasmosis, intestinal ascariasis, etc.).
In some cases, the optic nerve is atrophied already at birth (as a rule, this occurs with severe chromosomal pathology with gross skeletal and cranial deformations, for example, with acro-, micro- and macrocephaly, Crouzon's disease and other genetically determined anomalies of intrauterine development.
Finally, there is a fairly large proportion of cases (up to 20%) when the direct causes of optic nerve atrophy cannot be established.
Classification of optic nerve atrophy
As shown above, optic neuropathy can be either congenital or acquired. In accordance with this, hereditary forms are distinguished, classifying them according to the type of inheritance: autosomal dominant, autosomal recessive, mitochondrial.
Autosomal dominant optic atrophy can be expressed in varying degrees and in some cases is observed in combination with congenital deafness. Autosomal recessive atrophy is part of the structure of a number of chromosomal syndromes (Wolfram, Kenny-Coffey, Jensen, Rosenberg-Chattorian syndromes, etc.).
Mitochondrial atrophy occurs when mitochondrial DNA is mutated (Leber's hereditary optic neuropathy).[3]
Acquired optic neuropathy can also develop for various reasons and in different types. Thus, primary atrophy is based on long-term mechanical compression of the neural optic canal, while the optic disc when examining the fundus may appear intact, undamaged, with normatively clear boundaries.
Secondary atrophy may be a consequence of swelling of the optic nerve head, which, in turn, is one of the consequences of pathology of the retina or the nerve itself. The degeneration and displacement of specialized, functional neural tissue by neuroglial tissue has more pronounced and obvious ophthalmoscopic correlates: the observed optic disc in this case is usually increased in diameter, its boundaries lose clarity. In glaucoma, the axial symptom of which is chronically increased intraocular fluid pressure, developing collapse of the lamina cribrosa of the sclera leads to atrophy of the optic nerve.
The observed tint of the optic disc has significant diagnostic significance. Thus, initial, partial and complete atrophy of the optic nerve looks different during ophthalmoscopy: in the initial stage there is a slight blanching of the disc with the usual coloring of the nerve itself, with partial atrophy the optic nerve disc turns pale in individual segments and, finally, complete atrophy is observed as total and uniform blanching of the optic disc in combination with a narrowing of the blood vessels supplying the fundus of the eye.
There are also ascending and descending forms of atrophy (with ascending, the atrophic process in the nerve is initiated by damage to the retinal tissue, with descending, it begins in the fibers of the optic nerve itself). Depending on the extent of the process, atrophy is divided into unilateral and bilateral; by the nature of development - stationary (stable) and progressive, which can be diagnosed through regular ophthalmological observations over time.
Some authors take into account the severity of clinical manifestations.[4]
Fig. 3 Timely consultation with a doctor at the first complaints about vision will help preserve it
Symptoms
The vast majority of cases of this disease have a posterior capsular form. This is facilitated by the lack of normal epithelial protection of the lens, which makes its contact with toxins pronounced. Symptoms of violations:
- Increasing pressure in the eyes.
- The color of complicated cataracts (ivory), which is associated with a large number of infiltrates.
- The patient begins to see worse; when looking at a light source, halos appear before the eyes.
- The ability to adapt vision to night time mode decreases, dark spots appear before the eyes more often, and “spots” flash.
Incomplete cataracts are also characterized by disturbances in the perception of background colors, unclear vision of the contours of objects, and contrasting combinations.