Atrophic gastritis , or the more correct medical name atrophy of the gastric mucosa , is an irreversible process in which the death of cells in the gastric mucosa that produce gastric juice and hydrochloric acid occurs. Atrophy also includes the gradual replacement of stomach cells with connective tissue and cells similar in structure to the cells of the intestinal mucosa.
Atrophy of the gastric mucosa is a dangerous condition for health, since over time and especially in the presence of additional risk factors, it can lead to the development of stomach cancer.
Causes of atrophic gastritis
There are more than ten different causes, each of which can lead to atrophy of the gastric mucosa. Most often, this condition is the result of a long course of inflammation, against the background of chronic gastritis.
Chronic gastritis is a common disease (found in up to 30% of the population in various populations), which has a chronic and recurrent course, manifested by inflammation of the gastric mucosa and confirmed by morphological examination.
The causes of the development of chronic gastritis are:
- presence of Helicobacter pylori infection (H. pylory);
- inflammation caused by an autoimmune process, when your own immune system damages the cells of the gastric mucosa;
- long-term use of medications, such as non-steroidal anti-inflammatory drugs (NSAIDs);
- doudenogastric reflux, when the contents of the duodenum, including bile, are thrown into the stomach;
- prolonged contact with harmful substances during work;
- exposure to radiation;
- the presence of other chronic diseases, for example, celiac disease, Crohn's disease, sarcoidosis;
- food allergies;
- endocrine disorders;
- other infections (except H. pylori), fungi, parasites.
That is, in most cases, atrophy of the gastric mucosa is the result of the most common (80%) chronic gastritis caused by Helicobacter pylori infection, or autoimmune gastritis, which occurs in 1-2% of cases. This article discusses in detail the atrophy associated with these two causes.
Publications in the media
Chronic gastritis is a long-term disease characterized by the development of a number of morphological changes in the gastric mucosa and accompanied by various disorders of its basic functions. Prevalence. 50–80% of the entire adult population, the incidence of chronic gastritis increases with age. Incidence of gastritis and duodenitis: 287.2 per 100,000 population in 2001.
Classification
• By etiological factor • Microbial: Helicobacter pylori, etc. • Non-microbial •• Autoimmune •• Alcoholic •• Post-resection •• Caused by exposure to NSAIDs •• Caused by exposure to chemical agents • Unknown factors, incl. microorganisms.
• By type • Non-atrophic (type B, superficial, diffuse antral, hypersecretory) • Atrophic (type A, diffuse gastric body, associated with B12-deficiency anemia) • Special forms •• Chemical •• Radiation •• Lymphocytic •• Giant hypertrophic ( Ménétrier's disease, adenopapillomatosis) •• Granulomatous •• Eosinophilic •• Other infectious.
• By localization • Antral gastritis • Body gastritis • Pangastritis.
Etiology • Chronic non-atrophic gastritis in 85–90% of cases is caused by Helicobacter pylori • The development of chronic atrophic (autoimmune) gastritis is associated with the genetically determined production of autoantibodies to the lining cells of the gastric mucosa • The most common causes of chemical (reactive) gastritis are bile reflux and long-term use of NSAIDs • The etiology of eosinophilic gastritis is unknown, some patients have a history of bronchial asthma, eczema and other allergic diseases • Granulomatous gastritis is found in 10% of patients with sarcoidosis, 7% of patients with Crohn’s disease, with tuberculosis, mycoses, foreign bodies in the stomach • Etiology of giant hypertrophic gastritis is unknown.
Clinical picture
• Chronic non-atrophic gastritis • The pain syndrome often resembles that of duodenal ulcer (pain in the epigastric region that occurs on an empty stomach, but is usually less intense). The pain can be acute, cramping or aching, not intense; sometimes occur soon after eating • Dyspeptic syndrome - heartburn, sour belching, less commonly nausea, vomiting of gastric contents.
• Atrophic gastritis • Often combined with B12-deficiency anemia, thyroiditis, thyrotoxicosis, primary hypoparathyroidism • Sometimes the disease is latent • The most common manifestations are heaviness in the epigastric region after eating, a feeling of overeating, fullness of the stomach, belching of food and air, unpleasant taste in the mouth , loss of appetite, possible flatulence, unstable stool.
• Chemical (reactive) gastritis • Characterized by a triad of symptoms: pain in the epigastric region, intensifying after eating, vomiting with bile, bringing relief, weight loss.
• Giant hypertrophic gastritis • Pain in the epigastric region of varying intensity, often aching, occurs after eating and is accompanied by a feeling of heaviness in the stomach • Vomiting and diarrhea are possible; appetite is often reduced, sometimes even to the point of anorexia • In most patients, body weight decreases (by 10–20 kg) • In 25–40% of patients, peripheral edema is detected due to significant loss of protein with gastric juice (more than 8 g/day) • Gastric bleeding from erosions • Gastric carcinoma develops in 10% of cases.
Diagnostics
• OAC: B12-deficiency anemia in chronic gastritis type A
• Stool analysis: possible presence of hidden blood, as well as undigested food debris with reduced secretory activity of the stomach.
• X-ray examination does not allow diagnosing the main forms of chronic gastritis; but with its help it is possible to identify ulcers, cancer, polyposis, duodenal gastric reflux, giant hypertrophic gastritis, chronic obstruction of the duodenum • Chronic obstruction of the duodenum - delay of the contrast mass in the intestinal lumen for more than 45 s, expansion of the intestinal lumen, the presence of duodenum gastric reflux •• Giant hypertrophic gastritis (Menetrier's disease) - pronounced thickening of the folds of the mucous membrane in a limited area (with a local variant) or throughout the stomach (with a diffuse variant). The stomach wall in the affected area is elastic, peristalsis is visible.
• FEGDS •• Non-atrophic (superficial) gastritis: the mucous membrane is shiny (sometimes with a coating of fibrin), edematous, hyperemic, submucosal hemorrhages •• Atrophic gastritis: the mucous membrane is thinned, pale gray in color, with translucent blood vessels, the relief is smoothed •• Reflux -gastritis: the pylorus is gaping, the gastric mucosa is hyperemic, edematous; bile is present in the stomach •• Giant hypertrophic gastritis: there is a large amount of mucus in the stomach, the mucous membrane is easily vulnerable, erosions and hemorrhages are often found.
• Study of the secretory function of the stomach •• Chronic non-atrophic gastritis, reflux gastritis: the secretory function is normal or increased •• Chronic atrophic gastritis, giant hypertrophic gastritis: the secretory function of the stomach is reduced.
• Detection of Helicobacter pylori •• Invasive methods: it is necessary to perform FEGDS with a biopsy of the gastric mucosa; at least five biopsies are taken (two each from the antrum and fundus and one from the angle of the stomach). To confirm the success of eradication, the study is carried out no earlier than the 5th week after completion of the course of treatment ••• Bacteriological method ••• Histological method (detection of bacteria during microscopic examination of stained preparations) ••• Biochemical method (urease test) •• Non-invasive tests •• •Immunological methods (detection of antibodies to Helicobacter pylori) •••Breath test ••PCR diagnostics in biopsy samples of the gastric mucosa (invasive method) and in the patient’s feces (non-invasive method).
• Detection of antibodies to parietal cells and intrinsic factor and hypergastrinemia are a sign of atrophic autoimmune gastritis.
• Floor manometry of the upper gastrointestinal tract: with reflux gastritis, an increase in pressure in the duodenum to 200–240 mm water column is detected. (normally - 80–130 mm water column).
TREATMENT
Chronic non-atrophic gastritis
• Diet: for hypo- and achlorhydria, diet No. 2 is prescribed, for hyperacid conditions - diet No. 1.
• For gastritis caused by Helicobacter pylori - eradication (course of therapy - 1-2 weeks) •• Triple therapy ••• bismuth tripotassium dicitrate 120 mg 4 times / day for 28 days ••• metronidazole 200 mg 4 times / day in for 10–14 days ••• tetracycline 500 mg 4 times/day for 10–14 days •• Quadra-therapy ••• omeprazole 20 mg 2 times/day ••• tripotassium bismuth dicitrate 120 mg 4 times/day •• • tetracycline 500 mg 4 times a day ••• metronidazole 500 mg 3 times a day.
• In the absence of Helicobacter pylori and increased secretory function of the stomach •• Antacids, preferably non-absorbable, 1-2 hours after meals 3-4 times / day and before bed • Selective m-anticholinergic blockers (pirenzepine - 50 mg 2 times / day) • Blockers Histamine H2 receptors: ranitidine (150 mg 2 times a day orally or intramuscularly), famotidine (20 mg 2 times a day orally or intravenously) •• H+,K+-ATPase blockers (proton pump blockers) ) - omeprazole, rabeprazole 20 mg 2 times / day, lansoprazole 30 mg 2 times / day.
• Drugs that protect (envelop) the mucous membrane •• Sucralfate •• Bismuth tripotassium dicitrate (also has an antimicrobial effect against Helicobacter pylori).
Chronic atrophic gastritis • Drug therapy is carried out only during the period of exacerbation • Replacement therapy for secretory gastric insufficiency: natural gastric juice, pepsidil, hydrochloric acid with pepsin, acidin-pepsin (these drugs are contraindicated in the presence of erosions of the mucous membrane) • Replacement therapy for decreased excretory function of the pancreas glands (cholenzyme, pancreatin + bile components + hemicellulase, pancreatin, panzinorm forte) • Treatment of B12-deficiency anemia • Herbal medicine: herbal remedies that have an anti-inflammatory effect - infusion of plantain leaves, chamomile, mint, St. John's wort, valerian (1 tbsp. per glass of water) orally, 1/3–1/4 glass 3–4 times a day before meals for 3–4 weeks; plantain juice 1 tbsp. or plantaglucide 0.5–1 g 3 times a day • Drugs that improve tissue trophism and enhance reparative processes: nicotinic acid (1% solution IV from 1 to 10 ml for 10 days or IM 3–5 ml 20 days), solcoseryl 1–2 ml IM 20 days, inosine 0.2 g 3 times a day 40 minutes before meals 20–30 days, thiamine, pyridoxine, folic acid • Blockers of central and peripheral dopamine receptors for pain and severe dyspeptic symptoms (see below Reflux gastritis).
Reflux gastritis • Treatment is aimed at normalizing gastrointestinal motility and binding bile acids • To prevent the reflux of duodenal contents into the stomach, dopamine receptor blockers are prescribed (domperidone, metoclopramide, cisapride 10 mg 3 times a day 30 minutes before meals for 2-3 weeks ) • To neutralize bile acids that have a damaging effect on the gastric mucosa, chenodeoxycholic and ursodeoxycholic acids are used • To protect the mucous membrane from bile acids - antacids in the usual daily dose (aluminum-containing antacids have the ability to bind bile acids, so they are more effective).
Giant hypertrophic gastritis • Long-term treatment (2-3 months) • High-calorie, protein-rich diet • Antisecretory therapy • For treatment-resistant hypoproteinemia, repeated bleeding, surgical treatment (gastric resection) is indicated.
ICD-10 • K29 Gastritis and duodenitis
Application. Eosinophilic (allergic) gastroenteritis is a chronic disease characterized by predominantly eosinophil infiltration of the lamina propria of the gastric antrum mucosa, epithelium, pit glands with the formation of eosinophilic abscesses; characterized by damage to the small and large intestines, esophagus; often accompanies allergic diseases. Clinical picture: chronic diarrhea, abdominal pain, nausea, vomiting, weight loss, eosinophilia. Treatment: exclusion of allergy-provoking foods; diet No. 1; GCs provide long-term remission. ICD-10. K52.8 Other specified non-infectious gastroenteritis and colitis.
What happens to mucosal cells during atrophy?
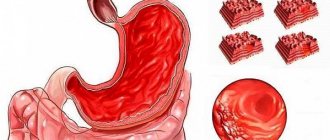
The gastric mucosa consists of three layers. The top layer covering the entire inner surface of the stomach is formed from cells that produce mucus to protect against the aggressive effects of gastric juice. Beneath it is the most important layer, called the “lamina propria of the stomach.” It contains the glands of the stomach, which produce substances that form gastric juice - hydrochloric acid, pepsin, hormones (internal Castle factor). The third layer contains muscle cells, the main task of which is to ensure the mobility of the gastric mucosa to move food along.
Atrophy of the gastric mucosa affects the upper layer and the lamina propria of the stomach and is an almost irreversible process that can be slowed down if the causes of inflammation are eliminated.
The gastric mucosa is exposed to an aggressive environment, so its cells are completely renewed every three days. The inflammatory process, which develops as a result of the influence of external factors, for example, a bacterial infection or internal causes, for example, the reaction of the immune system, disrupts the process of renewal (regeneration) of cells of the gastric mucosa, including the cells of the gastric glands that produce gastric juice. As a result, the cells of the stomach glands die and are replaced by connective tissue cells, as well as cells similar in structure to intestinal cells.
This process can be diagnosed using histological examination of samples of the gastric mucosa. If only a decrease in the number of cells of the gastric glands is detected, then they speak only of atrophy of the gastric mucosa. If intestinal cells are found in the test sample, then a diagnosis of atrophy with intestinal metaplasia is established. Metaplasia is the appearance of cells that are atypical for a given organ.
Development mechanism
The essence of the processes occurring during atrophic gastritis comes down to the cessation of the activity of some of the cells of the mucous membrane to produce the constituent elements of gastric juice, including hydrochloric acid. Changes begin with replacing production with slime. Typically, at the beginning there is an activation of acid formation, then a transition to significantly reduced acidity.
Most researchers are of the opinion that Helicobacter plays a role only in the first stage of the disease. It contributes to an increased consumption of acidity, spending some of it on the operation of its own enzyme systems. By this, Helicobacter completely disrupts the ability of the gastric mucosa to protect itself from external influences and destroy other incoming pathogens and toxic substances from food.
In the future, the main pathological direction is considered to be autoimmune. The body perceives its own cells as foreign and reacts by producing antibodies to them. Since such agents (antigens) are epithelial cells, they are destroyed during the reaction, thus blocking the recovery (regeneration) process.
In a healthy person, the epithelium is completely renewed every 6 days. Mucus production does not replace gastric juice. Complete cells are replaced with connective tissue. The stomach wall gradually becomes thinner and stops participating in digestion. Undigested food accumulates in the stomach cavity, which stimulates increased gastrin synthesis.
Instead of replacement, the epithelium can produce similar cells that have lost the ability to secrete gastric juice
Most often, transformation occurs in areas of the intestinal epithelium (metaplasia, dysplasia). This condition is called precancerous. It is impossible to say exactly how long it will take for the transition to cancer to occur. The problem of whether atrophic gastritis can be cured at this stage rests on preventing further degeneration of the epithelium with the help of diet, diet, and medications.
Atrophied areas of the mucosa permanently lose their properties. The result of therapy depends on how much it is possible to support the remaining cells and compensate for the reduction of working epithelium.
How to correctly diagnose gastric mucosal atrophy?
To diagnose atrophic gastritis, FGDS (gastroscopy) with the collection of at least 5 biopsies (small fragments of mucous membrane) from different parts of the stomach. The number of biopsy samples is determined by the structure of the stomach, since atrophy in different sections develops at different rates, and therefore it is necessary to take samples from all five sections.
The diagnosis is established by a morphologist after a histological examination. Based on this study, treatment is selected and the frequency of examinations is determined for the timely detection of the oncological process.
Also, to assess the severity of atrophy, determination of the activity of the secretory function of the stomach using a laboratory blood test is used - Gastropanel (link).
Diagnosis of Helicobacter pylori infection is carried out using biopsy specimens and a 13C-urease breath test .
For autoimmune gastritis, laboratory diagnostics are carried out using a blood test to determine antibodies to stomach cells and internal Castle factor.
Prevention
In a conversation with Dr. Boldyreva, we asked a question about the possible prevention of gastritis. According to her, the occurrence of this disease can indeed be prevented. However, for this it is important to adhere to proper nutrition - try to consume fatty and rough foods as little as possible. The same applies to alcohol, which has a detrimental effect on the entire gastrointestinal tract.
In addition, the doctor recommended avoiding stress, because problems with the nervous system primarily affect the stomach. Also, special attention should be paid to physical activity, because a sedentary lifestyle has never made anyone healthier.
Therefore, if unpleasant sensations appear in the stomach area, there is no need to delay treatment. It is better to immediately contact a professional, find the cause of the pain and cure it as soon as possible.
Atrophic gastritis associated with Helicobacter pylori infection
After infection with the bacterium Helicobacter Pylory, inflammation and chronic non-atrophic gastritis develop in the gastric mucosa. At the beginning of the disease, the glands of the stomach produce a sufficient amount of gastric juice. If left untreated, inflammation becomes more active and spreads to all parts of the stomach, leading to mucosal atrophy) and partial replacement of stomach cells with intestinal cells (intestinal metaplasia).
Symptoms
At the onset of the disease, gastritis is asymptomatic. As atrophy progresses, symptoms appear associated with a decrease in the production of hydrochloric acid and other components of gastric juice:
- loss of appetite,
- belching of air or rotten belching;
- nausea;
- feeling of heaviness and fullness in the stomach;
- bad breath; salivation, unpleasant taste in the mouth;
- rumbling, bloating;
- intolerance to certain foods;
- unstable stool;
- dull, aching pain that intensifies after eating;
- weight loss.
Treatment
Eradication (destruction) of Helicobacter Pylory is the first stage of treatment for this variant of atrophic gastritis.
Directions for treatment in the presence of a chronic disease
When infected with Helicobacter pylori, the only cure is eradication of the infectious agent. The functions performed include preventing the spread of infection, preventing the possibility of bacteria becoming unsusceptible to antibiotics, reducing the duration of the course of therapy and the number of drugs and the risk of side symptoms.
Antibiotics like tetracyclines and penicillins and medications based on metronidazole, proton pump inhibitors, bismuth agents, and the like are used as tools that prevent the spread of bacteria or the exacerbation of chronic moderately atrophic gastritis
Autoimmune atrophic gastritis
With this type of chronic gastritis, stomach cells are damaged by antibodies produced by the body's own immune system. In this case, chronic inflammation develops, leading to atrophy of the gastric glands and a decrease in the production of hydrochloric acid and internal Castle factor, which ensures the absorption of vitamin B12. A significant decrease in the production of intrinsic factor of Castle can cause anemia B12-deficiency anemia (pernicious anemia) - a disease characterized by impaired hematopoiesis.
Symptoms
The symptoms of autoimmune atrophic gastritis are similar to the symptoms of atrophy caused by Helicobacter pylori infection.
Additionally, anemia develops; autoimmune gastritis can often be accompanied by other autoimmune diseases.
Treatment
There is no specific treatment for autoimmune gastritis; treatment with corticosteroids is used only in exceptional cases.
Why is eradication necessary?
Eliminating Helicobacter helps:
- suppress further development, the addition of other bacteria, and the growth of antibiotic-resistant strains;
- reduce the duration of treatment for gastritis;
- reduce the negative effects of medications;
- bring the acidity of gastric juice closer to normal.
The most effective treatment regimens are those that combine tetracycline and penicillin antibiotics and Metronidazole (Trichopol). The modern product De-Nol, a drug based on bismuth citrate, is actively used. Doses are selected individually.
Classification of the disease
There are many types of pathology, but according to the severity of the signs of the disease, the degree of damage to the mucous membrane, and the frequency of symptoms, acute and chronic gastritis are distinguished. In the first case we are talking about a newly diagnosed disease, in the second - about repeated attacks of the disease.
Acute gastritis can be:
- Catarrhal.
- Fibrinous.
- Corrosive.
- Phlegmonous.
Chronic gastritis is divided into the following types:
- Bacterial. The cause of the development of pathology is the bacterium Helicobacter Pylori. The pathogen is resistant to the acidic environment of the organ and lives on its inner surface.
- Chemical. This type of gastritis occurs due to the aggressive effects of substances of endogenous and exogenous origin - bile, alcoholic beverages, some medications, various toxic substances.
- Autoimmune. It develops as a result of the erroneous influence of immune system cells on a person’s own tissues.
In rare cases, types of gastritis such as granulomatous, resection, lymphocytic, and radiation are diagnosed. Considering the degree of damage to the gastric mucosa, superficial, widespread, deep and erosive varieties of chronic gastritis are distinguished. Depending on the amount of hydrochloric acid in gastric juice, pathology may be accompanied by low or high acidity.
Advantages of treatment at Elena Malysheva’s clinic
Gastroenterologists at the Elena Malysheva Medical Center have the highest qualified categories and many years of experience (more than 10 years). They constantly improve their skills, study innovative technologies and actively implement them into their practice. Modern equipment makes it possible to diagnose pathological changes at the earliest stages, which contributes to successful treatment.
An appointment with a gastroenterologist at the Elena Malysheva Clinic in Izhevsk is possible by phone or through an online form.
Diagnosis
First, the gastroenterologist listens to the patient’s complaints, studies the medical history, and performs palpation.
If necessary, the doctor can refer for diagnostics (methods are chosen individually):
- pH measurement to assess the secretory activity of parietal cells;
- study of gastric enzyme activity;
- gastrography to study the motor function of the stomach;
- endoscopy - allows you to examine the mucous membrane;
- fibrogastroduodenoscopy - shows thinning of the mucous membrane;
- ultrasound examination - reveals smoothing of the folds of the stomach;
- biopsy followed by histological analysis.
bacterial analysis to determine the presence of the bacterium Helicobacter pylori;
A few words about serum markers
We have a diagnostic algorithm for identifying stomach diseases, which is recommended for all patients who have pain or discomfort in the upper abdomen.
Pepsinogens
There are seven isoforms of pepsin precursors, five of which are designated as group Pepsinogen I of the main cells of the stomach body and Pepsinogen II, uniformly secreted by the glands of the entire stomach and duodenum. Pepsinogens formed in the stomach are absorbed into the blood and determination of their serum level is a generally accepted marker of atrophic gastritis “serological biopsy”.
A decrease in the level of Pepsinogen I indicates the severity of atrophic gastritis of the body of the stomach, and since the activation of Pepsinogen I into active pepsin occurs with the participation of hydrochloric acid, then the level of Pepsinogen I can roughly represent the level of stomach acidity. Pepsinogen II is produced in all parts of the stomach and in the duodenum. As the severity of atrophy increases, the ratio of serum levels of Pepsinogen I and Pepsinogen II decreases, which indicates the severity of atrophy and the spread of the process.
Gastrin
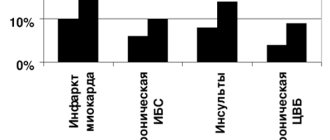
Gastrin-17, produced in the outlet section of the stomach after stimulation of cells by various factors (stomach distension, protein foods). In case of atrophy of the gastric antral mucosa, the secretion of Gastrin-17 decreases. To assess the presence and severity of the atrophic process in the stomach, it is necessary to conduct a protein stimulation test, the decrease of which shows the severity of atrophy; in the case of atrophy of the mucous membrane of the antrum of the stomach, the secretion of Gastrin-17 is proportionally reduced. In patients with severe atrophic gastritis in the antrum of the stomach, the risk of developing stomach cancer is 90 times higher than in people with normal gastric mucosa.
Homocysteine
Homocysteine is an early marker of cellular functional deficiency of B12, B6, folic acid due to the development of atrophic gastritis and other reasons - age, smoking, Helicobacter pylori infection, etc. With atrophic gastritis, the level of homocysteine increases in the blood and becomes toxic to the body. When donating blood for homocysteine, you should avoid protein foods, vitamins, and hormonal contraceptives 1 day before the test. This test can be an addition to the Gastropanel or an independent test for other diseases.