General information
Cerebral edema is one of the manifestations of various critical conditions and is quite often encountered in clinical practice with various kinds of diseases and the development of pathologies. There are edema of the brain, spinal and bone marrow.
Brain swelling
Brain edema is an increase in its volume, caused by the accumulation of fluid in the intercellular space (interstitium) and accompanied by an increase in the volume of brain tissue. While an increase in brain volume due to intracellular fluid is defined by the term “swelling” of the brain. However, these processes (edema/swelling) can develop simultaneously and transform into each other, therefore both of these concepts can be defined as cerebral edema. ICD-10 cerebral edema code: G93.6
Edema syndrome develops as a nonspecific reaction of the body to the influence of many pathogenic factors. Possible in a number of diseases/pathological conditions that occur with damage to the nervous system - traumatic brain injury , acute cerebrovascular , infectious diseases, hypoxia , intoxication , brain tumors ( perifocal edema ), acute somatic diseases accompanied by impaired water-salt balance / hemodynamics, with endocrine disorders, blood diseases, after surgical interventions, exposure to ionizing radiation, etc. Brain edema is often one of the manifestations of critical conditions and the direct cause of death of the patient.
As a rule, cerebral edema at an early stage (with timely medical correction) is a reversible process, while with inadequate/late treatment, pathological processes increase and often end with the degeneration of brain nerve cells with disruption of their function and, in general, functional failure of brain structures.
Due to the accumulation of fluid in the interstitium of the brain, an increase in brain volume occurs in conditions of limited intracranial space with the development of mass effect (pathological effect of expanding tissue on neighboring structures, causing compression, deformation, displacement, atelectasis), which is primarily manifested by the development of intracranial hypertension (ICP) ) with a controlled increase in cerebral ischemia , and in severe cases - with displacement of brain structures and infringement of the stem sections in the tentorium of the cerebellum, accompanied by dysfunction of vital centers.
Spinal cord swelling
Most often, swelling of the spinal cord develops with traumatic injuries to the spine. Pathological disorders are formed both as a result of traumatic injury and compression of the spinal cord structures due to its edema-swelling, which is accompanied by ischemia of the brain substance, inflammatory changes and a high risk of developing irreversible disorders of the function/structure of the spinal cord. Compression of the spinal cord causes the formation of primary/secondary softening lesions in the spinal cord and is accompanied by neurological symptoms. Clinical manifestations are determined by the level of localization of edema, its severity and duration. With severe edema, it manifests itself as a syndrome of partial/complete disruption of spinal cord conduction.
Bone marrow edema (trabecular bone marrow edema)
There are subchondral and trabecular edema of the bone marrow. Trabecular edema - what is it? Spongy substance (syn. trabecular tissue) of bone consists of loose partitions/plates, the spaces between which are filled with bone marrow, which ensures hematopoiesis in the human body and the formation of immune chains. Edema of the spongy tissue is manifested by the accumulation of exudate (interstitial fluid) in the trabecular plates. At the same time, the liquid level increases from 10 to 20% or more. In most cases, the diagnosis is made late, since there are no specific symptoms and the disease is detected only on MRI.
According to the literature, bone marrow edema occurs more often in middle-aged patients and mainly affects large joints, the condyles of the tibia/femur. The most common (trabecular edema of the lateral condyle of the femur, bone marrow edema of the hip joints, bone marrow edema in the diaphysis of the radius, swelling of the condyle of the femur, etc.). Spinal bone marrow edema is much less common .
The causes of bone marrow edema are extremely diverse ( bruises / fractures , vitamin D deficiency , rheumatoid arthritis , osteoarthritis , benign / malignant tumors , osteomyelitis , spondylitis , arthrosis deformans , endocrine pathologies accompanied by impaired cellular metabolism, status epilepticus , acute neuroinfections , etc.) . The mechanisms of development of bone marrow edema are poorly understood. It is assumed that its development is facilitated by microvascular trauma, abnormal mechanical loads on bones/joints, metabolic disorders, and venous obstruction. Due to the small volume of the article, only cerebral edema will be considered.
Consequences of cerebral edema
As one of the critical conditions, cerebral edema very often ends in the death of the patient. The occurrence of edema marks either decompensated changes in the body of a general nature, or damage to brain tissue that is practically incompatible with life. All this makes cerebral edema an extremely unpredictable pathology, which may not respond to improvement with treatment. Among all the possible outcomes of cerebral edema, only three can be distinguished.
Progression of edema with transformation into brain swelling and death
A similar scenario, unfortunately, occurs in half of cases of cerebral edema of any origin. The danger of the situation is that as swelling progresses, a critical accumulation of fluid occurs in the brain tissue. This causes their pronounced swelling and increase in volume. As long as there is space in the cranial cavity to be filled with edematous cells, the condition of the patients remains relatively stable. But as soon as the free space is filled, compression of the brain occurs. As edema progresses, dense brain structures move into softer ones, which is called dislocation. Its typical variant is the wedging of the cerebellar tonsils into the brain stem, which ends in cessation of breathing and heartbeat.
Complete elimination of edema without consequences for the brain
This scenario is very rare and is possible only when cerebral edema occurs in young somatically healthy people due to intoxication with alcohol or other compounds toxic to the brain. If such patients are delivered on time to specialized toxicology or general intensive care units, and the dose of toxins turns out to be compatible with life, then the cerebral edema will be stopped and will not leave any pathological symptoms.
Elimination of cerebral edema with patient disability
The second most common outcome of this disease. Possible in patients with meningitis, meningoencephalitis of moderate severity, as well as with traumatic brain injuries in the form of small, timely diagnosed and operated on intracranial hematomas. Sometimes the neurological deficit is so minimal that it does not cause any visual manifestations.
Pathogenesis
The development of edema is initially based on microcirculatory disorders. Almost immediately after neuronal damage, regardless of its cause (hemorrhage, trauma, ischemia, tumor, inflammation), cytotoxic perifocal cerebral edema develops, and later, against its background, dysfunction of the capillary epithelium develops with accumulation of fluid in the interstitial space. In the development of endothelial dysfunction, several stages are distinguished, which are accompanied initially by functional (ion edema), then anatomical (vasogenic edema/hemorrhagic transformation) failure, as well as failure of the blood-brain barrier.
The development of cytotoxic edema is based on the accumulation of osmotically active substances inside cells (potassium/sodium/chlorine ions and glutamate molecules), which along the osmolarity gradient contribute to the movement of fluid from the interstitium into the intracellular space. That is, during this phase, cerebral edema is formed due to the trans-epithelial flow of sodium from the vascular bed, along with which chloride ions (to maintain electroneutrality) and water (to maintain osmoneutrality) move. At this stage, there is only a functional impairment of the permeability of the anatomically intact blood-brain barrier. At the same time, against this background, conditions are formed that contribute to the development of the next stages of cerebral edema (in particular, a drop in the concentration of interstitial sodium). The stage of cytotoxic edema does not lead to an increase in the volume of brain tissue and intracranial hypertension.
Developing vasogenic edema is characterized by more pronounced disturbances in the homeostasis of the interstitial space, which leads to disruption of the function/activity of neurons. As a result of increased permeability of the BBB, water accumulates in the intercellular space, which provokes the development of hypoxia and causes a malfunction of the cellular ion pumps of the brain, leading to the passive penetration of sodium ions into the cell, followed by water (the process of cell swelling).
The accumulation of fluid in a limited space according to the Monroe-Kelly formula leads to an increase in intracranial pressure , and in damaged glia (due to edema) the processes of exchange/capture of transmitter amino acids are disrupted. With the development of severe intracranial hypertension, it leads to displacement of the cerebral structures of the increased volume of the brain with herniation of the cerebellar tonsils/stem parts into the foramen magnum. And further compression of blood vessels further aggravates microcirculatory disorders/ischemia of brain cells. Dysfunction of the cardiovascular/respiratory/thermoregulatory centers located in the brain stem is a common cause of death.
As endothelial dysfunction progresses, it is accompanied by pronounced necrosis of epithelial cells and a sharp increase in the size of the intercellular space, which facilitates the passage of blood cells and leads to hemorrhagic saturation of brain tissue, which causes severe disruption of interstitial homeostasis, incompatible with the functioning of neurons and the development of hemorrhagic necrosis , which is associated with severe outcome of cerebral edema. The figure above shows the pathogenesis of cerebral edema.
Treatment of cerebral edema
The diagnosis of cerebral edema, regardless of its origin, implies hospitalization of the patient exclusively in the intensive care unit. This is due to the presence of an immediate threat to life and the need to artificially maintain basic vital functions in the form of breathing and blood circulation, which is only possible with the appropriate equipment.
The complex of diagnostic and treatment measures should include the following areas:
- Combating existing cerebral edema and its progression;
- Clarification of the causes of cerebral edema and their elimination;
- Treatment of concomitant manifestations that aggravate the condition of patients.
Dehydration therapy
It involves removing excess fluid from tissues. This goal can be achieved by using the following drugs:
- Loop diuretics – Trifas, Lasix, furosemide. Their dose must be very high, which is necessary to create a high concentration and rapid onset of the diuretic effect;
- Osmotic diuretics – beckons. Appointed first. After its infusions, the introduction of loop diuretics is recommended. This combination of drugs will have the maximum dehydration effect;
- L-lysine escinate. The drug does not have a diuretic effect, but perfectly removes fluid from tissues, reducing signs of edema;
- Hyperosmolar solutions – magnesium sulfate 25%, glucose 40%. They briefly increase plasma osmotic pressure, enhancing the diuretic effects of diuretics. Additionally, they supply ischemic brain cells with nutrients.
Adequate oxygenation and improved brain metabolism
Achieved by:
- Instillation of humidified oxygen or artificial ventilation;
- Local hypothermia by placing containers filled with ice around the head;
- Administration of drugs that improve metabolic processes in affected brain cells (Actovegin, Mesquidol, Ceraxon, Cortexin);
- Glucocorticoid hormones. Their action is to membrane stabilization of affected cells and strengthen the weakened vascular wall of the microvasculature.
Classification
Due to the specific development of cerebral edema, 4 types are distinguished:
- Cytotoxic OGM - develops as a result of ischemia , hypoxia , exo/endogenous toxic effects on brain cells, causing changes in the permeability (osmoregulation) of cell membranes and dysfunction of glial cells (disorders of cellular metabolism). Cytotoxic edema is reversible within 6-8 hours due to reactivation of the ion pump, which is achieved by restoring cerebral blood flow.
- Vasogenic OGM is based on an increase in the permeability of the blood-brain barrier . Occurs perifocally in the area of ischemia , abscess , tumor, traumatic brain injury, surgery. The main role is played by the transition of fluid from the vessels to the white medulla. Due to the increase in capillary permeability, fluid partially passes from the vessels into the interstitial space), causing an increase in its volume.
- Osmotic OGM develops when the osmolarity of brain tissue increases without disrupting the blood-brain barrier. Occurs with metabolic encephalopathies , hypervolemia , drowning , inadequate hemodialysis and polydipsia .
- Interstitial OGM is the result of a rapid increase in ventricular pressure.
- It is formed when the walls of the cerebral ventricles sweat from the liquid part of the cerebrospinal fluid in the periventricular zone.
According to the degree of compensation there are:
- Compensated OGM (characterized by the absence of dislocation syndrome).
- Subcompensated OGM (characterized by the presence of dislocation syndrome in the absence of vital lesions of brain structures).
- Decompensated OGM (presence of dislocation syndrome and disturbances of vital functions).
The table below shows a general classification of OGM and characteristics of its forms.
Causes
The causes of cerebral edema are quite numerous, according to which cerebral and extracerebral causes of AMS are distinguished.
Cerebral causes of cerebral edema:
- Brain injuries ( subdural hematoma , brain contusion , basal skull fracture , diffuse axonal injury , intracerebral hematoma ), brain surgery.
- Primary brain tumors ( glioma , medulloblastoma , astrocytoma , hemangioblastoma , etc.) or metastatic lesions of brain tissue that promote displacement of brain structures/disturb the process of outflow of cerebrospinal fluid.
- Cerebrovascular accidents - against the background of arterial hypertension (with a stroke of ischemic / hemorrhagic origin ) or systemic atherosclerosis .
- Neuroinfections ( encephalitis , bacterial meningitis ), purulent processes of the brain (for example, subdural empyema ).
Extracerebral causes:
- Infectious diseases ( influenza , scarlet fever , measles , scarlet fever , toxoplasmosis , mumps , etc.).
- Poisoning with drugs (quinine, antidepressants, neuroleptics, antihistamines, etc.) or various neurotoxic poisons (cyanides, phenols, gasoline, etc.).
- Radiation exposure.
- Development of an allergic reaction ( anaphylactic shock , Quincke's edema ).
- Encephalopathy due to liver/ renal failure , diabetes mellitus , alcohol poisoning.
- A sharp climb without the required acclimatization (mountain edema).
In newborns, cerebral edema can be caused by intracranial birth trauma, severe toxicosis of the pregnant woman, prolonged labor, or entanglement of the umbilical cord.
Cerebral edema in newborns
The relationship between brain tissue and the cranial cavity in newborns is structured completely differently than in adults. This is due to the characteristics of the developing organism and age-related changes in the nervous system. In newborns, cerebral edema is characterized by lightning-fast progression due to imperfect regulation of vascular tone, liquor dynamics, and maintaining intracranial pressure at a stable level. The only thing that saves a newborn is the peculiarities of the joints of the skull bones, which are represented either by soft cartilaginous bridges or are located at a distance from each other (large and small fontanelles). If not for this anatomical feature, any cry of the child could result in the development of compression of the brain and its swelling.
Causes
In newborns, the causes of cerebral edema can be:
- Intrauterine hypoxia of any origin;
- Difficult childbirth and birth trauma;
- Congenital malformations of the nervous system;
- Intrauterine infections;
- Meningitis and meningoencephalitis as a result of infection during or after childbirth;
- Congenital tumors and abscesses of the brain.
Symptoms of cerebral edema in newborns
You can suspect cerebral edema in a newborn based on the following manifestations:
- Restlessness and loud crying;
- Lethargy and drowsiness;
- Breast refusal;
- Tension or swelling of the large fontanel when the child is at rest;
- Vomit;
- Convulsive seizures.
Characterized by a very rapid increase in symptoms and a progressive deterioration in the general condition of the child. In many cases, cerebral edema in newborns cannot be reversed and ends in death.
The presence of risk factors for the development of cerebral edema in a newborn is a reason for clinical observation by specialized specialists. Such a child must be examined by a pediatric neurologist to exclude any signs of intracranial pathology. Mothers should be very attentive during the month after giving birth and respond to any changes in the child’s behavior!
Symptoms
Symptoms of cerebral edema in adults are extremely variable and are caused by dysfunction of various brain structures, disorders of metabolic processes/microcirculation and a developing increase in the volume of brain tissue, especially accompanied by displacement/herniation of certain brain structures, disruption of cerebrospinal fluid dynamics/blood flow in the vessels of the brain. The localization of edema in areas of the brain also plays a significant role, which determines its effect on specific brain structures and forms, in addition to general cerebral symptoms, focal neurological symptoms depending on the affected brain structures. Clinical symptoms of cerebral edema vary significantly depending on the stage of its development, according to which the following are distinguished.
General cerebral syndrome
Clinical signs at this stage are caused by an increase in ICP (intracranial pressure), and their manifestations/severity are determined by the rate of its increase.
headache appears vomiting may occur , often without preceding nausea. The intensity of pain after vomiting usually decreases. Transient dizziness . A common symptom is congested optic discs/transient episodes of visual impairment. Changes in the cardiovascular system are noted: bradycardia , increased systolic blood pressure, decreased breathing (the so-called “Cushing triad).” Characterized by slowly increasing changes in the psyche according to the type of disinhibition: irritability, anxiety, moodiness. Objective symptoms of intracranial hypertension with a slow increase in ICP are congestion of the veins/swelling of the optic disc, radiographically - thinning of the bones of the cranial vault, osteoporosis of the sella turcica.
With a rapid increase in ICP, severe pain of a paroxysmal/paroxysmal nature appears, often bursting pain, accompanied by vomiting, which does not bring relief with the subsequent development of coma . Bradycardia , oculomotor disorders appear Against the backdrop of ICP progression, mental inhibitions are noted, which is manifested by decreased memory, severe drowsiness , non-communication of the patient, and slower speech/thinking.
Syndrome of rostrocaudal diffuse increase in neurological symptoms
Clinical signs of cerebral edema at this stage are determined by the gradual involvement of certain brain structures in the pathological process. As a rule, the pathological process first involves the cortical, later the subcortical, and ultimately the structures of the brain stem. Edema of the cerebral hemispheres is characterized by impaired consciousness and the appearance of generalized clonic seizures.
The spread of the process to the subcortical/deep structures of the brain occurs with psychomotor agitation, the development of grasping/protective reflexes, hyperkinesis , and an increase in epileptic paroxysms .
When the pathological process moves to the hypothalamic region/upper parts of the brain stem, the degree of impairment of consciousness increases sharply, manifesting as coma / stupor with initial manifestations of impaired breathing and function of the cardiovascular system. A posture of decerebrate rigidity (installation of the limbs in an extension position). The convulsions are of a stem nature ( opisthotonus / hormetonia ), mydriasis (dilated pupils) with a sluggish reaction to light is noted.
Swelling of the tegmentum of the cerebral pons causes specific breathing disorders in the form of periodic breathing, maximum bilateral miosis (constriction of the pupils), truncal gaze paresis and leads to the disappearance of the oculovestibular/oculocephalic reflexes. As the edema moves to the medulla oblongata (lower part of the brainstem), disturbances in vital functions increase, which is manifested by a slower pulse/decreased blood pressure and breathing. Neurological examination reveals areflexia of deep reflexes , diffuse muscle hypotonia , lack of pupillary response to light, immobility of the eyeballs.
Phase of dislocation of brain structures
It is based on the process of dislocation and temporo-parietal/occipital herniation of brain structures, which is manifested by characteristic focal symptoms, the main of which are brainstem symptoms ( bradycardia , decerebrate rigidity , dysphagia etc.) with damage to the oculomotor nerves ( mydriasis , ptosis , divergent strabismus ). Often there is sudden vomiting, stiffness of the neck muscles, convulsions of the extensor muscles, lack of pupillary response to light, a decrease in body temperature, a decrease in heart rate and the development of life-threatening conditions - a sharp drop in blood pressure, depression of consciousness (coma), breathing disorders (cessation).
The particular danger of displacement/herniation of supratentorial structures is determined by the high risk of developing vascular disorders and occlusion of the cerebrospinal fluid outflow pathways, which sharply intensifies the primary pathological processes, which turn from potentially reversible disorders into irreversible ones.
Initial manifestations of insufficient blood supply to the brain (treatment, prevention, disability)
L. S. Manvelov, Candidate of Medical Sciences V. E. Smirnov, Doctor of Medical Sciences, Professor
Research Institute of Neurology of the Russian Academy of Medical Sciences, Moscow
The diagnosis of “initial manifestations of insufficiency of blood supply to the brain” (IPNKM) is established in accordance with the “Classification of vascular lesions of the brain and spinal cord” developed by the Research Institute of Neurology of the Russian Academy of Medical Sciences [4], if a patient with signs of a general vascular disease (vegetative-vascular dystonia, arterial hypertension (AH)) , atherosclerosis) there are complaints of headache, dizziness, noise in the head, memory impairment, decreased performance. Moreover, the basis for this diagnosis can only be a combination of two or more of the five listed complaints, which must be noted at least once a week for at least the last three months
The problem of prevention and treatment of early forms of vascular diseases of the brain is of great social and economic importance. Not only are they a serious risk factor for the development of cerebral stroke, one of the leading causes of disability and mortality, but they themselves significantly worsen the quality of life, and often reduce ability to work.
Secondary prevention, which is required by patients with initial manifestations of insufficiency of blood supply to the brain (IBC), includes measures to prevent both exacerbations of major cardiovascular diseases and vascular lesions of the brain.
Therapeutic and preventive measures for NPNCM can be schematically divided into the following types: work, rest and nutrition regimen; physiotherapy; diet, physio and psychotherapy; drug treatment and prevention. Most often, diet No. 10 is prescribed, taking into account anthropometric data and the results of a study of metabolic characteristics.
Treatment of patients with NPNCM should be carried out in three main areas:
- Impact on the mechanism of formation of insufficiency of blood supply to the brain,
- Impact on cerebral metabolism,
- Differentiated individual treatment depending on the clinical symptoms of the disease.
In patients with NPNCM in the early stages of the formation of the underlying vascular disease, rational employment, adherence to work, rest and nutrition regimens, cessation of smoking and alcohol abuse, and the use of drugs that increase the physiological defenses of the body are sometimes sufficient to compensate for the condition. In severe forms of the disease, complex therapy with extensive use of medications is necessary.
Therapy should be carried out aimed at eliminating foci of infection: odontogenic; chronic tonsillitis, sinusitis, pneumonia, cholecystitis, etc. Patients with diabetes mellitus should receive adequate antidiabetic treatment.
If treatment is not carried out regularly, the risk of developing acute cerebrovascular accidents, as well as dyscirculatory encephalopathy, increases significantly. Thus, according to our data, based on a seven-year prospective observation of 160 patients with hypertension with NPCCM (men 40-49 years old), transient cerebrovascular accidents (TCVA) developed 2.6 times more often, and cerebral stroke - 3.5 times more often in untreated patients. or those who were treated irregularly than those who were treated regularly and followed medical recommendations.
Drug methods of treatment and prevention of exacerbations of the underlying vascular disease
Vegetovascular dystonia. Therapy is carried out in accordance with the principles of dividing autonomic disorders according to sympathicotonic and vagotonic manifestations.
With increased sympathetic tone, a diet with limited proteins and fats, warm baths, and carbon dioxide baths are recommended. Central and peripheral adrenolytics and ganglion blockers are used. Alpha-blockers are prescribed: pyrroxan, redergin, dihydroergotamine, and beta-blockers: anaprilin, atenolol, tenormin, which have a vasodilating and hypotensive effect.
In cases of insufficiency of sympathetic tone, a diet rich in proteins is indicated; salt and radon baths, cool showers. Effective drugs that stimulate the central nervous system: caffeine, phenamine, ephedrine, etc. Improve the sympathetic activity of lemongrass tincture 25-30 drops per day, pantocrine - 30-40 drops, ginseng - 25-30 drops, zamanikha - 30-40 drops, calcium supplements (lactate or gluconate 0.5 g three times a day); ascorbic acid - 0.5-1.0 g three times; methionine - 0.25-0.5 g two to three times a day.
When parasympathetic activity increases, a low-calorie but protein-rich diet and pine baths (36°C) are recommended. They use drugs that increase the tone of the sympathetic system. Belladonna preparations, antihistamines, and vitamin B6 are used.
If the parasympathetic system is weak, the following have a positive effect: foods rich in carbohydrates; coffee; strong tea; low temperature sulfide baths (35°C). Increase parasympathetic tone with cholinomimetic drugs, cholinesterase inhibitors: prozerin 0.015 g orally and 1 ml of 0.05% solution in injections, mestinon 0.06 g, potassium preparations: potassium chloride, potassium orotate, panangin. Sometimes small doses of insulin are used.
Dividing the syndrome of vegetative-vascular dystonia by the nature of its manifestations (predominance of sympathetic or parasympathetic activity) is not always possible. Therefore, drugs that act on both peripheral parts of the autonomic nervous system and have both adrenergic and cholinomimetic activity have found widespread use in practice: belloid, bellaspon, ergotamine preparations.
Arterial hypertension. Therapeutic and preventive measures for hypertension should primarily be aimed at eliminating or correcting risk factors that contribute to the development of the disease, such as psycho-emotional stress, smoking, alcohol abuse, excess body weight, sedentary lifestyle, diabetes mellitus.
It is necessary to limit the consumption of table salt to 4-6 g per day (1/2 teaspoon), and in case of severe hypertension - even to 3-4 g.
Currently, five classes of antihypertensive drugs are considered the most effective for the drug treatment of hypertension: beta blockers, angiotensin-converting enzyme (ACE) inhibitors, diuretics, calcium antagonists and alpha blockers. The report of the WHO Expert Committee provides recommendations for the selection of the initial drug for the treatment of hypertension, presented in Table.
Complex antihypertensive drugs are effective: brinaldix, adelfan-ezidrex, trirezide K, etc. However, they have negative side effects of their ingredients: reserpine, thiazide diuretics and hydralazines. These drugs can be used during exacerbation of hypertension, but in the future it is necessary to select an individual maintenance treatment regimen. Therapy for the malignant form of hypertension should begin in a hospital.
Do not increase the dose of an initially effective drug multiple times if it no longer controls blood pressure reliably. If the prescribed medicine turns out to be ineffective, it needs to be replaced. It is better to add small doses of another antihypertensive drug than to increase the dose of the first one. The effectiveness of treatment increases when using the following combinations of drugs:
- A diuretic in combination with a beta blocker, alpha blocker or ACE inhibitor.
- A beta blocker in combination with an alpha blocker or a dihydropyridine calcium antagonist.
- ACE inhibitor in combination with a calcium antagonist. To achieve maximum results, in some cases it is necessary to use a combination of not only two, but also three antihypertensive drugs.
If in patients with moderate to severe hypertension, blood pressure does not decrease within a month of combined treatment with two or three drugs, it is considered to be resistant. The reasons for resistance are very diverse: irregular drug intake, insufficiently high doses, ineffective drug combinations, use of pressor drugs, increased blood plasma, the presence of symptomatic hypertension, excessive consumption of table salt and alcohol. The “white coat” effect is known (an increase in blood pressure in a patient in the presence of a doctor or nurse), which can create the impression of resistance. The most serious causes of treatment resistance are an increase in blood plasma in response to a decrease in blood pressure, kidney disease and drug side effects. In a number of patients with resistant hypertension, the use of loop diuretics, a combination of ACE inhibitors and calcium antagonists has a positive effect.
It is believed that the hypotensive effect is achieved with a persistent decrease in blood pressure in patients with mild hypertension (140-179/90-104 mm Hg) to a normal or borderline level (below 160/95 mm Hg), and with moderate and severe Hypertension (180/105 mm Hg and above) - by 10-15% of the initial values. A sharp decrease in blood pressure due to atherosclerotic lesions of the great vessels of the head, which occurs in 1/3 of patients with hypertension, can worsen the blood supply to the brain.
After selecting therapy, the patient is invited for examinations until an adequate reduction in blood pressure is achieved. This ensures that blood pressure is kept at an optimal level and risk factors are under control. A gradual and careful decrease in blood pressure significantly reduces side effects and complications of antihypertensive therapy.
When a stable decrease in blood pressure is achieved, the patient should be invited for repeated examinations at intervals of 3-6 months. Antihypertensive therapy is usually carried out indefinitely. However, after long-term adequate control of blood pressure levels, a careful dose reduction or discontinuation of one of the combined drugs is allowed, especially in individuals who strictly adhere to the recommendations for non-drug treatment.
Atherosclerosis. To treat patients with atherosclerosis, it is necessary first of all to identify high levels of serum cholesterol (CS) and take measures to correct it.
The main drugs used in the treatment of patients with NPNCM
A special role belongs to drugs that have a combined effect on blood supply and metabolism of the brain, as well as on central hemodynamics and rheological properties of blood. Cavinton (vinpocetine) 0.005 g is used; cinnarizine (stugeron) - 0.025 g; xanthinol nicotinate (teonicol, complamin) - 0.15 g; parmidine (anginine) - 0.25-0.5 g; sermion - 0.005-0.03 g; tanakan - 0.04 g - three to four times a day.
In cases of increased cerebral vascular tone in the spastic type of REG, antispasmodic and vasoactive agents are recommended. It is advisable to prescribe aminophylline 0.15 g three times a day. As a result, as a rule, the general condition of patients improves, headaches and dizziness decrease or disappear, and positive changes in rheographic and Doppler sonographic parameters are noted. Patients with unstable vascular tone are prescribed Belloid, Bellaspon, Grandaxin. For hypotension of cerebral vessels and signs of venous insufficiency, stimulating drugs are recommended: eleutherococcus, zamanikha, Leuzea rhizome, pantocrine, duplex, ginseng, tincture of Chinese lemongrass, aloe - and venotonic drugs: troxevasin, aescusan, anavenol, venoruton.
Due to the fact that vascular disease of the brain is often preceded or accompanied by cardiac dysfunction, patients are prescribed drugs that improve coronary blood flow, antiarrhythmics, and cardiac glycosides according to indications. For functional disorders of the heart in patients with NPCM, hawthorn in the form of a liquid extract, 20-30 drops four times a day, has a beneficial effect.
Currently, of the agents that have a positive effect on the rheological properties of the blood coagulation and anticoagulation system, aspirin is the best studied and most widely used. The main disadvantage of this drug is its irritating effect on the gastrointestinal tract. Therefore, it is recommended to take it once in a daily amount of no more than 1 mg per 1 kg of weight. For this purpose, trental 0.1 g, dipyridamole - 0.25 g and methindol - 0.025 g are also used three times a day. In addition, these agents prevent destabilization of the cell membranes of neurons during cerebral ischemia, suppress edema and swelling of the endothelium, increase blood flow to the brain, facilitate venous circulation and have an antispasmodic effect, which ultimately determines their effectiveness for secondary prevention and treatment of vascular diseases of the brain. A number of other drugs also have an antiplatelet effect: papaverine, no-spa, alpha- and beta-adrenergic blockers, etc.
For memory and attention disorders, to increase mental and motor activity, treatment with nootropil (piracetam) 0.4 g, encephabol (pyriditol) 0.1 g, aminalon 0.25-0.5 g two to four times a day is recommended , injections of Cerebrolysin 5.0 ml intravenously or intramuscularly and other means of similar action.
If there are manifestations of a neurosis-like syndrome, tranquilizers are prescribed: chlozepid (Elenium, Napoton) 0.005-0.01 g three to four times, sibazon (Seduxen, Relanium) - 0.005 g once or twice, phenazepam - 0.00025-0.0005 g and mezapam (rudotel) - 0.005 g two to three times a day; sedatives: preparations of valerian, motherwort, peony tincture, etc.
Of the methods of physical therapy, electrophoresis of drugs is most often used using the reflex-segmental (collar) transorbital Bourguignon method, as well as the general method of exposure in both the usual and bipolar ways. Favorable results were noted in treatment with electrophoresis of a 10% solution of acetylsalicylic acid and a 7.5-10% solution of potassium orotate from a 40-50% universal solvent - dimexide using a general method of exposure: longitudinally on the spine with application of electrodes to the collar , interscapular and lumbosacral areas - 8-12 procedures per course.
A new method of treatment is the electrophoretic administration of stugeron in the form of transcerebral reflex iontophoresis of a 0.5% solution. In patients with cephalgia, it is advisable to carry out three or four procedures of endonasal electrophoresis with a 0.1% dihydroergotamine solution before this.
For patients with impaired venous outflow, a method of transcerebral electrophoresis of a 5% solution of troxevasin has been proposed. The combined use of electrophoretic and oral administration of stugeron and troxevasin makes it possible to influence all parts of the vascular system of the brain: arterial tone, microcirculation and venous outflow.
For headaches and autonomic disorders, iodine electrophoresis is used using the collar method, and for neurotic conditions and hyposthenia, novocaine electrophoresis is used. Bipolar electrophoresis of iodine and novocaine is recommended for neurasthenic syndrome, a tendency to dizziness, and pain in the heart. For sleep disturbances and increased general excitability, electrophoresis of bromine and iodine, diazepam or magnesium according to the Vermeule method, and electrosleep are used. Electrophoresis of dallargin has a positive effect on the reflexogenic zones C-4 - T-2 and T-8 - L-2.
It should be emphasized that drug therapy has a number of limitations: side effects, allergic reactions, addiction to drugs, and a decrease in their effectiveness with long-term use. In addition, it is necessary to take into account the possibility of complete insensitivity of patients to a particular drug. Therefore, the use of non-drug treatment methods is of great importance.
Non-drug methods of prevention and treatment for NPNCM
The treatment complex includes diet therapy, active motor regimen, morning hygienic exercises, physical therapy, swimming in the pool, and sports games. If you are overweight, an underwater shower massage is performed. With concomitant osteochondrosis of the cervical spine - massage of the collar area.
Effects of alternating low-frequency magnetic fields and sinusoidal modulated currents on reflexogenic zones and muscle groups of the cervical, collar and waist areas, upper and lower extremities, taking into account daily biorhythms, are successfully used.
Reflexology methods are increasingly being introduced into practical healthcare: acupuncture, moxibustion, electroacupuncture, and exposure to laser radiation. In patients with NPNCM, as a result of treatment with these methods, the general condition significantly improves, subjective disorders decrease or disappear, there is a positive dynamics of REG and EEG indicators, which is explained by the normalizing effect of reflexology on metabolic processes, an increase in physical and mental tone, and the elimination of vegetative-vascular disorders. If the tone of the cerebral veins is increased, a course of microwave irradiation (8-12 sessions) is recommended for reflexogenic zones and acupuncture points.
Hyperbaric oxygenation is considered as a universal component of pathogenetic therapy for vascular diseases of the nervous system, which makes it possible to stabilize the pathological process, reduce treatment time and improve the prognosis. In the process of barotherapy, the general condition of patients, sleep, memory improve, asthenia, psycho-emotional disorders, headaches, dizziness, and autonomic disorders decrease.
A persistent clinical effect and long-term remissions were observed in patients with NPNCM who received complex treatment including hyperbaric oxygenation, acupuncture and physical therapy.
Widespread use of balneotherapy is recommended.
Hydroaeroionotherapy is used both as an independent method and in combination with other types of physiotherapy and medications. It is advisable to use oxygen therapy in the form of oxygen cocktails, which has a general stimulating effect and improves the functional state of the nervous system. The combination of aeroion therapy and oxygen therapy gives a greater clinical effect: well-being and memory improve, headaches disappear, vestibular and emotional-volitional disorders decrease. These treatment methods can be used not only in a hospital, but also in a clinic.
A method of training therapy using intermittent hypoxic exposure is proposed: inhalation of an air-nitrogen mixture containing 10% oxygen.
For neurosis-like syndrome, which is detected in a significant number of patients with NPNCM, psychotherapy is recommended. Its most important tasks are to develop in patients the correct attitude towards the disease, adequate psychological adaptation to the environment, and increase the effectiveness of medical and social rehabilitation. Psychotherapy involves the active participation of the patient in all its stages and should begin from the first appointment. In cases of severe manifestations of cerebrasthenia, hypnotherapy is successfully used. Using autogenic training is effective. The best results are achieved with combined treatment with tranquilizers and antidepressants with psychotherapy and autogenic training.
Of great importance is the complex step-by-step therapy of patients with NPNCM, which includes inpatient treatment, sanatorium-resort treatment and outpatient observation. Sanatorium-resort treatment is most appropriate to carry out in sanatoriums of the cardiovascular or general type, without changing the climatic zone, since due to a decrease in adaptive capabilities, patients with NPNCM spend significant time on acclimatization, which shortens the period of active treatment, reduces the durability of its effect, and in some cases even worsens the condition.
The main treating and dispensary doctor for patients with NPNCM should be a local (shop) general practitioner. The neurologist is assigned the responsibility of consultant to these patients. Clinical observation and course treatment, the duration of which is 1-2 months, should be carried out at least twice a year (usually in spring and autumn).
Work ability
Patients with NPNCM are usually able to work. However, sometimes they need easier working conditions, which are recommended by the VKK: exemption from night shifts, additional loads, correction of the work regime. Patients are referred to VTEK in cases where working conditions are contraindicated for them due to health reasons. They cannot work in a caisson, under altered atmospheric pressure, in hot shops (steelmaker, blacksmith, thermal operator, cook), under constant significant psycho-emotional or physical stress. If transfer to another job is associated with a decrease in qualifications, then disability group III is established.
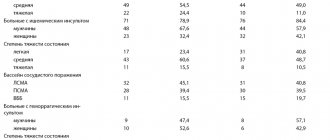
| Choice of drug for the treatment of hypertension (according to WHO recommendations, Geneva, 1996) | |||
| Drug class | Indications | Contraindications | Limited use |
| Diuretics | Heart failure, old age, systolic hypertension, black skin color | Gout | Diabetes mellitus, hyperlipidemia, pregnancy*, increased sexual activity |
| Beta blockers | Angina pectoris, previous myocardial infarction, tachyarrhythmia, pregnancy | Bronchial asthma, obstructive pulmonary diseases, peripheral vascular diseases, heart block** | Hypertriglyceridemia, insulin-dependent diabetes mellitus, heart failure, athletic and physically active persons, black skin color |
| ACE inhibitors | Heart failure, left ventricular hypertrophy, previous myocardial infarction, diabetes with microalbuminuria | Pregnancy, bilateral renal artery stenosis | Black skin color |
| Calcium antagonists | Peripheral arterial disease, angina pectoris, old age, systolic hypertension, low glucose tolerance, black skin color | Pregnancy | Congestive circulatory failure***, heart block**** |
| Alpha blockers | Prostate hypertrophy, low glucose tolerance | Orthostatic hypertension | |
| * Due to a decrease in plasma volume. ** Atrioventricular blockades of the 1st and 2nd degrees. *** Either avoid or use with caution. ****Either avoid or use verapamil and diltiazem with caution. | |||
Tests and diagnostics
Cerebral edema is an urgent condition that requires urgent medical care in a hospital setting (intensive care/resuscitation department), therefore, the initial diagnosis of acute brain injury should be as fast as possible and carried out during treatment. The primary guideline for diagnosing AGM is clinical symptoms, however, it must not be forgotten that at this stage they can be minimally pronounced. If OGM is suspected, a neurological/ophthalmological examination is carried out, during which pain, verbal-acoustic, behavioral reactions, ocular/pupillary reflexes, the condition of the optic nerve head, and intraocular pressure indicators are assessed. A clinical/biochemical blood test and lumbar puncture are required.
The main methods of instrumental diagnostics are computed tomography and nuclear resonance imaging, which allow one to visualize the localization/extension of the area of hyperhydration and identify signs of compression syndrome. According to indications, ultrasound of the skull in different projections, echoencephalography/electroencephalography, neuroophthalmoscopy, and cerebral angiography can be performed.
Differential diagnosis is carried out with thromboembolism of cerebral vessels , metabolic disorders , and status epilepticus .
Causes of head pain and facial swelling
The main cause of swelling is a violation of the outflow of fluid from the intercellular space, a slowdown in blood circulation. Mild swelling causes discomfort and headaches, and gradually decreases during the day. In severe stages, the contours of the face are deformed. The soft tissues acquire a dense consistency, the palpebral fissures narrow, which leads to a sharp deterioration in well-being. Laboratory tests and various diagnostic methods will allow you to determine the cause of edema - treatment is ineffective until an accurate diagnosis is made.
Physiological reasons
Facial swelling can also appear in the absence of various chronic diseases of internal organs. Violation of the daily routine, poor nutrition and other factors cause a deterioration in the outflow of fluid from soft tissues. There are several reasons that can trigger acute headaches and swelling, especially in the first half of the day:
- sleep disturbance, night work, lack of sleep;
- following strict diets;
- use of inappropriate cosmetics for facial skin;
- unhealthy diet, eating foods with a lot of salt and spices;
- sleeping on a large and high pillow - this causes poor circulation in the neck.
If you normalize sleep and nutrition principles, swelling will go away over time. However, the tendency for them to appear remains, so it is important to follow a daily routine. Doctors also recommend drinking plenty of fluids during the day, and before going to bed, eating only light foods with a small amount of salt and spices. This will help maintain fluid balance and speed up blood flow. If swelling appears, it is useful to massage the face and apply a cooling compress.
Endocrine system diseases
Hypothyroidism is a disease of the thyroid gland in which a reduced amount of iodine-containing hormones is recorded in the blood. These include thyroxine and triiodothyronine. These substances are necessary for the proper functioning of metabolism, the absorption and processing of fats, maintaining stable cholesterol levels, and the functioning of the reproductive system. With hypothyroidism, these functions are impaired. There are several types of hypothyroidism. For effective treatment, it is important to determine its exact cause. It can be associated both with insufficiency of the thyroid gland and with disruption of the pituitary gland and hypothalamus, the organs that control it. In addition, hypothyroidism can develop when there is insufficient intake of iodine into the body from food - this is typical for regions where it is practically absent in the soil and drinking water. The following symptoms are characteristic of this disease:
- disruption of the digestive tract, increased appetite or lack thereof, rapid weight gain;
- chronic fatigue and drowsiness during the day, deterioration of memory and concentration;
- pain and aches in the joints, deterioration in the quality of skin, hair and nails;
- swelling of the face, arms and legs, especially in the first half of the day.
Swelling with hypothyroidism may be minor, but in advanced cases the face becomes significantly deformed. Soft tissues acquire a dough-like consistency, and when pressure is applied to them, marks remain. This symptom, like the others, goes away with normalization of hormonal metabolism and replenishment of the concentration of iodine-containing hormones.
Allergy
An allergy is an increased sensitivity of the immune system to certain irritants. They pose no danger to the body, but are recognized as foreign and therefore trigger an immune response. These compounds can enter the body through the air or food, as well as through the skin. Allergies are often caused by plant pollen, animal hair, certain foods, household chemicals and cosmetics, as well as any other environmental substances. A typical manifestation of an allergic reaction is swelling of the mucous membranes and subcutaneous tissues, headaches, and skin rash. There are several main manifestations of allergies, which can occur independently or be combined with each other:
- urticaria - a small rash on the skin and swelling, most often occurs in response to contact of an irritant with the skin;
- contact dermatitis – in the facial area it is often an allergy to cosmetics, after application of which a rash and swelling appears;
- atopic dermatitis is a childhood form of an allergic reaction, which is manifested by swelling, itching and soreness, the appearance of a rash and small blisters;
- bronchial asthma is a chronic disease that can be aggravated by frequent inhalation of polluted air, as well as when allergens (dust, pollen, wool particles) enter the respiratory tract.
The greatest danger is Quincke's edema. It develops at lightning speed, the contours of the face change shape in just a few minutes. This symptom can develop independently or represent one of the stages of anaphylactic shock. In addition to the soft subcutaneous tissues, the mucous membrane of the larynx swells, resulting in impaired respiratory function. In this condition, a person needs urgent medical attention , since swelling is dangerous due to complete closure of the airways. The basis of treatment is antihistamines, which reduce sensitivity to the allergen and relieve the manifestations of an allergic reaction.
Kidney diseases
The appearance of edema is one of the characteristic signs of kidney disease , and they can also appear in the facial area. They are soft, mobile, and when you press on them, no marks remain. The skin in the area of edema does not become bluish - it remains pale and may also acquire a yellowish tint. Their appearance is associated with impaired blood filtration and increased capillary permeability, as a result of which the amount of protein in the blood decreases. There are several kidney diseases that can cause swelling in the face and headaches:
- glomerulonephritis is an inflammatory disease in which periods of exacerbation and remission alternate, and can be treated in the initial stages;
- Kidney amyloidosis is a chronic metabolic disorder in which an increased concentration of protein is detected in the urine;
- nephropathies are non-inflammatory diseases that may be associated with long-term use of medications, acute infectious processes, radiation or chemotherapy;
- chronic renal failure - deterioration of kidney function, which develops slowly over several years or more;
- kidney damage in various systemic diseases, including diabetes mellitus, systemic lupus erythematosus and others.
In the initial stages of kidney disease, morning puffiness under the eyes may be the only symptom. They go away during the day or with cold compresses, so they are not a cause for concern. However, then other symptoms of nephritis, nephropathy or kidney failure develop: lower back pain, pain when urinating, the appearance of blood in the urine. The swelling becomes large and mobile, changing location when turning over to the other side. They can be localized on the extremities, along the veins, as well as on the abdominal wall. They resolve after comprehensive treatment and support of kidney function.
Diseases of the heart and blood vessels
Cardiac edema often differs from renal edema in appearance and consistency. They most often appear on the lower extremities, but in some patients they also occur in the face. They are denser, colder, and the skin at the site of their appearance often acquires a bluish tint. This symptom is characteristic of cardiomyopathies, sclerotic changes, congenital and acquired heart defects, arrhythmias, chronic hypertension, amyloidosis and other cardiac disorders. It is also important to pay attention to additional symptoms:
- headaches and dizziness, weakness during the day;
- increase or decrease in blood pressure;
- chest pain;
- uneven pulse, including skipping heartbeats, fastening or slowing down.
Cardiac edema slowly resolves. To get rid of them, comprehensive treatment of the underlying disease and supportive therapy for the heart are carried out. In the absence of medical attention, swelling will increase. The accumulation of fluid and the deterioration of its excretion increase the load on the myocardium, which is dangerous due to exacerbation of diseases. As maintenance therapy, diuretics (diuretics) are prescribed, which stimulate the removal of excess fluid from the body in a natural way.
Intoxication
Toxins enter the human body every day. They are found in large quantities in the polluted air of large cities and industrial enterprises, as well as in drinking water and products. Their presence has a detrimental effect on the state of the lymphatic system, making it difficult to remove excess fluid. This leads to swelling under the eyes in the morning and chronic headaches. In some cases, poisoning causes rapid swelling of the tissues in the facial area. This may be due to a number of violations:
- bites of poisonous insects - the cause of acute pain, severe swelling, headache, a sharp deterioration in health and an increase in body temperature;
- consumption of alcoholic beverages - ethanol is a toxin that makes it difficult to remove fluid and can also affect the condition of blood vessels, internal organs and the brain;
- smoking is another cause of intoxication;
- consumption of toxic substances or their entry into the body through the skin or respiratory tract - some of them have a nephrotoxic effect and adversely affect the functioning of the kidneys (vinegar in high concentrations).
Alcoholism is a chronic disease characterized by swelling in the facial area. They can have a neutral, purple or yellow tint, and intensify in the morning or after drinking alcohol. Headaches are caused by the toxic effects of ethyl alcohol metabolism products on the nervous system and brain.
Diet
Nutrition in the first 1-3 days of AGM is carried out parenterally, for which protein hydrolysates, glucose solutions, amino acids, plasma, albumin, a complex of vitamins, and special nutritional mixtures are administered. The timing of the start of enteral nutritional support through a tube is determined depending on the patient's condition, however, to restore gastrointestinal motility, it should begin as early as possible. For this purpose, special quickly digestible high-calorie nutritional mixtures are used, enriched with vitamins/microelements, a set of essential/essential amino acids in optimal dosages ( Nutrizon Energy , Nutrizon , Berlamin , Nutrizon Protein , etc.). It is recommended to use highly concentrated mixtures to reduce the volume of fluid administered, but at the same time provide the body with the necessary amount of calories. The patient can begin eating by mouth after regression of brain disorders.
Stroke rehabilitation
Stroke is a disease in which rehabilitation and care are of the utmost importance.
Recovery from a stroke begins in intensive care, from the moment vital functions are stabilized. A multidisciplinary rehabilitation team works with the patient, which includes a rehabilitation doctor, physical therapist or exercise therapy instructor, speech therapist, massage nurse, physiotherapist and physical therapy nurse, psychologist, occupational therapist, guard and rehabilitation nurse. Diagnosis is carried out using special scales that reflect the degree of dysfunction and limitations in the patient’s activity, the influence of environmental factors on the rehabilitation potential. The rehabilitation process continues throughout the entire period of hospitalization. At the second stage, patients with serious disabilities who are unable to move independently are sent to rehabilitation departments or specialized hospitals. Those who can walk independently or with support are rehabilitated in outpatient centers based in clinics and sanatoriums.
The rehabilitation process should not be interrupted, so classes must be continued at home. Of course, there are no high-tech robotic complexes or physiotherapeutic equipment at home, but exercise therapy, massage, and work with a psychologist, speech therapist and occupational therapist are possible. For this purpose, telemedicine technologies are used and visits to rehabilitation specialists are organized.
The individual rehabilitation program includes not only a referral for rehabilitation treatment, but also technical means of rehabilitation. However, usually relatives also have to devote significant physical and financial resources to achieve the best effect [7].
Prevention
There is no specific prevention of cerebral edema, since it develops secondary. Among the general recommendations, we can only cite the need to follow some rules:
- Minimize the risk of head injury: use protective devices when moving (protective helmet when rollerblading/biking/skating, skiing; seat belts when driving in a car, do not jump your head into a body of water, etc.).
- Treat infectious/somatic diseases in a timely manner.
- Monitor your blood pressure .
- Lead a healthy lifestyle.
- When climbing to altitude (mountains), do not forget about the need to acclimatize to the altitude.
Prevention of strokes
Hereditary predisposition to stroke, the presence of cardiac diseases, pathology of blood vessels and blood composition, age over 40 years, obesity and diabetes require a number of preventive measures:
- Maintaining normal blood pressure, taking antihypertensive drugs as prescribed by a doctor, monitoring blood pressure.
- Maintaining a normal level of physical activity, exercise, walking 30-40 minutes a day (for example, walking the dog).
- Conducting preventive examinations, including a standard set of laboratory parameters. During a preventive examination, the following tests are additionally required: gene diagnosis of CADASIL syndrome using the PCR method, plasma factors of the blood coagulation system, antibodies to prothrombin of the IgG and IgM classes to determine the risk of thrombosis, determination of polymorphisms associated with the risk of arterial hypertension, diabetes mellitus, lipid disorders exchange, in order to identify a predisposition to diseases that increase the risk of stroke, von Willebrand factor (a glycoprotein that ensures the formation of blood clots), complex laboratory tests for preclinical diagnosis of cardiovascular diseases are offered (“ELI-ANKOR-Test-12”, “Cardiorisk”).
- Avoiding chronic and acute stress, maintaining mental hygiene.
- Normalization of weight (BMI <25 kg/m2).
- Healthy eating (for example, Mediterranean diet, limiting salt to 5 5 g/day).
- Quitting smoking and taking psychoactive substances.
- Treatment of diseases that are a risk factor for stroke [8, 11].
Consequences and complications
The consequences of cerebral edema, even in cases of rapid relief, can manifest as long-term consequences (absent-mindedness, disturbances in sleep/motor activity, communication abilities, depression). In severe cases, the consequences of cerebral edema can develop in the form of:
- decerebral syndrome (characterized by persistent extensor muscle rigidity, strabismus, severe mental defect);
- decortication syndrome (characterized by impairment/disappearance of speech, motor and mental skills;
- posthypoxic encephalopathy (characterized by dysfunction of the cortex with the development of a cerebral intellectual-mnestic defect).
The most severe complication is death from cerebral edema.
Consequences of a stroke
There are transient ischemic attack (less than a day), minor stroke (from 1 day to 3 weeks) and stroke with persistent residual effects. The consequences of a stroke are expressed mainly in motor and sensory disorders, the formation of muscle contractures (pronounced constant restriction of movements in the joints), speech and swallowing disorders. General symptoms may also remain, including confusion, disturbances in thinking, will, and emotional regulation. Complications can develop: from epilepsy to bedsores, encephalopathy and anxiety-depressive syndrome [1, 3].
Forecast
The prognosis for acute hypertension can vary significantly depending on its etiology, severity, localization, level of intracranial hypertension , and the presence of brain dislocation. Brain edema in the initial stage is a reversible process; as it increases, neuronal death/destruction of myelin fibers develops, leading to irreversible changes in brain structures.
However, even in surviving patients after cerebral edema, in the vast majority of cases there are residual effects, which can vary significantly from subtle manifestations in the form of increased intracranial pressure , frequent headaches , forgetfulness, irritability, absent-mindedness, depression , sleep disturbances, emotional disorders, slowness intellectual processes) to severe disorders of motor/cognitive functions, mental sphere, leading to the patient’s disability.
Severe complications develop especially often during stroke and coma . Accordingly, the prognosis for cerebral edema after a stroke, like the prognosis for coma, is disappointing, at best with disability due to impaired coordination/motor disorders and mental disorders, at worst the patient’s death occurs. Mortality rates for cervical edema, depending on the etiology and severity, vary between 35-70%.
Signs of an incipient stroke
The onset of a hemorrhagic stroke is characterized by the following symptoms:
- severe headache;
- increased blood pressure;
- vomit;
- dizziness;
- loss of consciousness;
- weakness in the limbs;
- visual impairment;
- seizures [1].
The onset of ischemic stroke is gradual; within an hour, some of the following symptoms appear:
- facial asymmetry, numbness;
- difficulty speaking – incoherent, impaired understanding;
- double vision, visual disturbances;
- headache;
- numbness, limited mobility in the limbs, often on one side;
- dizziness, imbalance, staggering, staggering gait;
- confusion with disorientation, subsequently there may be loss of consciousness [3].
If one or more of these signs appear, you should:
- Sit the patient down, providing access to fresh air.
- Call emergency medical help immediately.
- If the patient is conscious and able to chew and swallow, give him one aspirin tablet.
The patient must be hospitalized in a neurological or neurosurgical department, where stroke treatment will be carried out. The sooner the patient is in the hospital, the more effective the therapy.
List of sources
- Pavlenko, A.Yu. Cerebral edema: conceptual approaches to diagnosis and treatment / A.Yu. Pavlenko // Emergency Medicine. - 2007. - No. 2 (9). — P. 11-15.
- Principles and methods of diagnosis and intensive therapy of cerebral edema and swelling: method. recommendations / V.I. Cherny [and others]. - Donetsk, 2003. - 49 p.
- Slynko E.I. Traumatic injuries of the spine and spinal cord / E.I. Slynko, A.N. Honda. - K.: PP Gamma-Print, 2010. - 288 p.
- Martynov V.A., Zhdanovich L.G., Karaseva E.A., Ageeva K.A., Khasanova L.A. Edema-swelling of the brain: tactics of patient management // Infectious diseases: news, opinions, training. 2018. – T. 7. – No. 1. – S. 124-13.
- Zadvornov A.A., Golomidov A.V., Grigoriev E.V. Clinical pathophysiology of cerebral edema. Part 2 // Bulletin of anesthesiology and resuscitation. – 2021. – T. 14. – No. 4. – S. 52-60.
Treatment of headaches and facial swelling
Treatment tactics will depend on the exact diagnosis. It will include drugs to eliminate the underlying cause of the disorders, as well as to symptomatically eliminate swelling. The doctor will prescribe a medication regimen, which may include the following steps:
- for diseases of the cardiovascular system - cardiac glycosides, drugs for vasoconstriction, adrenergic blockers and anticoagulants;
- kidneys and excretory system - antibiotics as necessary, supportive agents;
- for allergies - antihistamines and hormonal anti-inflammatory drugs;
- hypothyroidism - iodine preparations, as well as levothyroxine;
- intoxication - gastric lavage and infusion therapy may be necessary.
Diuretics are prescribed to remove excess fluid. They are used for diseases of the cardiovascular system and for slowing down lymphatic drainage. However, such measures are temporary, so it is important to choose an effective treatment regimen that will eliminate the main cause of edema.