Pharmacological properties of the drug Cycloserine
bactericidal antibiotic, disrupts cell wall synthesis. Active against gram-negative microorganisms, at a concentration of 10-100 mg/l - against Rickettsia spp., Treponema spp . Currently used only to treat patients with tuberculosis. The MIC against Mycobacterium tuberculosis is 3–25 mg/l in liquid and 5–40 mg/l in solid nutrient medium. Resistance of mycobacteria to cycloserine develops slowly (after 6 months of treatment - in 20–60% of cases). Does not cause the development of cross-drug resistance. Its activity is inferior to streptomycin and ftivazide, but is active against Mycobacterium tuberculosis , resistant to these drugs and PAS. After oral administration, it is quickly and almost completely absorbed into the gastrointestinal tract (70–90%). Time to reach maximum concentration is 3–4 hours. Does not bind to plasma proteins. Penetrates well into body fluids and tissues, including CSF, breast milk, bile, sputum, lymphatic tissue, lungs, ascitic and synovial fluid, pleural effusion, and penetrates the placenta. The abdominal and pleural cavities contain 50–100% of the drug concentration in the blood serum. Up to 35% of the drug is metabolized. The half-life with normal renal function is 10 hours. Excreted by glomerular filtration in the active form (after 6 hours - 20%, after 12 hours - 30%, after 24 hours - 50%, after 2-3 days - up to 70%), small amounts - with feces.
Cycloserine
Manufacturer: ROUTEC Ltd. (Great Britain)
caps. 250 mg: 10, 50 or 100 pcs. Reg. No.: LP-000921
Clinical and pharmacological group:
Antibiotic; Anti-tuberculosis drug
Release form, composition and packaging
Capsules
hard gelatin No. 1, with an opaque white body and an opaque red cap.
| 1 caps. | |
| cycloserine | 250 mg |
Excipients:
lactose 120 mg, purified talc 10 mg, colloidal silicon dioxide (Aerosil) 3 mg, magnesium stearate 10 mg.
Composition of the capsule shell: Capsule body:
gelatin up to 100%, titanium dioxide (E 171) 2.11%;
Capsule cap:
gelatin up to 100%, crimson dye Ponceau 4R (E 124) 0.49%, quinoline yellow dye (E 104) 0.00999%, titanium dioxide (E 171) 2.16%.
10 pieces. — aluminum strips (1) — cardboard packs. 10 pieces. — aluminum strips (5) — cardboard packs. 10 pieces. — aluminum strips (10) — cardboard packs.
Description of the active components of the drug "Cycloserine"
pharmachologic effect
Anti-tuberculosis antibiotic. It acts bacteriostatically or bactericidal depending on the concentration at the site of infection and the sensitivity of microorganisms. It is an analogue of the amino acid D-alanine. Competitively inhibits the activity of the enzymes L-alanine racemase, which converts L-alanine into D-alanine, and D-alanyl-D-alanine synthetase, which includes D-alanine into the pentapeptide necessary for building the bacterial cell wall.
Active against Mycobacterium tuberculosis, Mycobacterium avium.
Indications
Tuberculosis (as part of combination therapy), atypical mycobacterial infections (MAC infections).
Dosage regimen
When taken orally for adults, the dose is 0.25-1 g/day in several divided doses. Maximum dose
- 1 g/day.
For children - 10-20 mg/kg/day in divided doses.
Side effect
From the central nervous system and peripheral nervous system:
headache, dizziness, drowsiness, anxiety, confusion, depression, difficulty speaking, nightmares, muscle twitching, tremors, restlessness, peripheral neuropathy, seizures.
Allergic reactions:
possible skin rash.
Contraindications
Depression, psychosis, alcoholism, renal dysfunction, epilepsy, organic diseases of the central nervous system, history of seizures, pregnancy, hypersensitivity to cycloserine.
Pregnancy and lactation
Contraindicated for use during pregnancy.
Cycloserine is excreted in breast milk, so if it is necessary to use it during lactation, the issue of stopping breastfeeding should be decided.
Use for renal impairment
Contraindicated in case of impaired renal function.
Application for children
Application is possible according to the dosage regimen.
special instructions
With monotherapy with cycloserine, rapid development of mycobacterial resistance is possible, so only combination therapy should be used.
Careful monitoring of patients receiving cycloserine at doses above 500 mg/day is necessary to identify signs of CNS toxicity.
During the treatment period, avoid drinking alcohol.
Drug interactions
When used simultaneously with ethanol, the risk of developing convulsive seizures increases; with ethionamide, isoniazid - the risk of developing adverse reactions from the central nervous system increases.
Drug interactions
When used simultaneously with ethanol, the risk of developing convulsive seizures increases; with ethionamide, isoniazid - the risk of developing adverse reactions from the central nervous system increases.
Use of the drug Cycloserine
Orally, immediately before meals (if irritation of the gastrointestinal mucosa - after meals), adults - 0.25 g every 12 hours for the first 12 hours, then, if necessary, taking into account tolerance, the dose is gradually increased to 250 mg every 6-8 hours under the control of the concentration of cycloserine in the blood serum. The maximum daily dose is 1 g. Patients over the age of 60 years, as well as with a body weight of less than 50 kg, take 0.25 g 2 times a day. The daily dose for children is 0.01–0.02 g/kg (not higher than 0.75 g/day).
Bedaquiline in the treatment of multidrug-resistant tuberculosis.
Introduction.
According to the World Health Organization (WHO), the incidence of tuberculosis in 2012 was 8.6 million cases with 1.3 million deaths.[1] Despite the fact that over the past 20 years there has been a slight decrease in incidence, the problem of multidrug-resistant tuberculosis (drug resistance to at least isoniazid and rifampicin) is coming to the fore. Thus, in 2012, there were 450,000 cases of multidrug-resistant tuberculosis, which represents a global health problem.[1]
Treatment of this form of tuberculosis is a complex and very long path, requiring the use of old drugs, mostly bacteriostatics with a wide range of adverse drug reactions.[2] In 2012, extensively drug-resistant tuberculosis (additional resistance to second-line injection therapy and fluoroquinolones) was diagnosed in 92 countries worldwide, and the number of cases accounts for 9.6% of all patients with multidrug-resistant tuberculosis.[1]
Bedaquiline (Sirturo, TMC207) is a diarylquinoline that inhibits mycobacterial ATP synthase, an enzyme that plays a key role in cellular respiration.[3] This is the first anti-tuberculosis drug with a fundamentally new mechanism of action that has been approved for the treatment of multidrug-resistant tuberculosis in the last 40 years.
The drug has already proven its effectiveness in vitro and in mouse models, which made it possible to continue its studies in patients.
Target.
To evaluate the effectiveness and safety of bedaquiline in the treatment of multidrug-resistant tuberculosis.
Materials and methods.
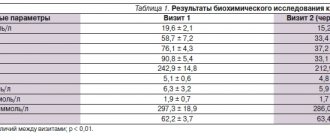
The randomized, double-blind, placebo-controlled clinical trial TMC207-C208 enrolled patients aged 18 to 65 years with newly diagnosed, active (sputum-infected), pulmonary, multidrug-resistant tuberculosis. Exclusion criteria were: previous treatment for multidrug-resistant tuberculosis, a positive HIV test with a CD4+ lymphocyte count of less than 300 per ml3, severe extrapulmonary and neurological manifestations of tuberculosis, severe cardiac arrhythmia requiring drug therapy, a history indicating an increased risk of developing arrhythmias such as torsades. de pointes, alcohol and drug abuse, pregnancy or breastfeeding and previous use of bedaquiline. The use of moxifloxacin, gatifloxacin, and systemic cytochrome P-450 3A4 inhibitors was also prohibited during the study period and for 1 month after completion of the study.
The study included patients from Brazil, India, Latvia, Peru, the Philippines, Russia, South Africa and Thailand.
The patients were divided into 2 groups: the first received bedaquiline at a dose of 400 mg once a day after breakfast for the first two weeks, then 200 mg 3 times a week for 22 weeks), the second received placebo + all patients received a 5-component second-line antituberculosis therapy (ethionamide, pyrazinamide, ofloxacin, kanamycin and cycloserine). At the same time, changes to the above-described scheme were permitted if there was data on serious side effects, low sensitivity to drugs and their absence in the country.
After a 24-week course of bedaquiline treatment, patients received an additional 96 weeks of basic therapy. Those who were excluded from the study due to the development of adverse drug reactions also continued to be observed.
The primary endpoint of the study was the time required for the pathogen to clear from sputum, which was confirmed by the presence of two negative sputum tests at least 25 days apart. The secondary endpoint was the absence of mycobacteria in culture at 24 weeks and at 120 weeks.
Results.
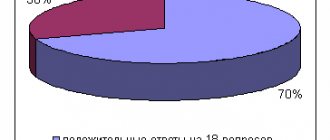
The final analysis included 160 patients (64% men): 79 received bedaquiline and 81 received placebo.
In the first group, the mean time to clearance of the pathogen in sputum was less than in the placebo group - 83 days compared to 125 days (HR = 2.44, 95% CI, 1.57-3.80; P
In the majority of patients receiving bedaquiline, compared with the control group, the absence of mycobacteria in sputum was confirmed at 24 and 120 weeks of the study - in 52 of 66 patients (79%) in the first group, and in 38 of 66 (58%) in the second. 24 weeks (P=0.008); in 41 of 66 (62%) and 29 of 66 (44%), respectively, at week 120 (P=0.04).
At week 120, of the 25 patients in the main group who did not respond to bedaquinil therapy, 8 retained mycobacteria in their sputum, 6 experienced initial disappearance and then rediscovery, and 11 were excluded from the study after the disappearance of mycobacteria. In the placebo group of 37 patients, the above situations were diagnosed in 15, 10 and 12 patients, respectively.
Newly diagnosed resistance to at least one anti-tuberculosis drug was detected in 2 patients from the first group and 16 from the control group.
Safety.
Ten of 79 (13%) patients in the bedaquinil group and 2 of 81 (2%) in the placebo group died (P=0.02).
The most common adverse drug reactions in the main group were: nausea, arthralgia and vomiting.
At week 24, the QT interval duration increased on average by 15.4 MSK in the bedaquinil group and by 3.3 MSK in the control group (P
Conclusion.
The addition of bedaquiline in a 5-component treatment regimen in patients with multidrug-resistant tuberculosis leads to a more rapid disappearance of mycobacteria from sputum and, in a higher percentage of cases, to their absence at 24 weeks of therapy compared to placebo. There were fewer deaths in the placebo group than in the bedaquinil group.
Source: Andreas H. Diacon, MD, Ph.D., Alexander Pym, MD, Ph.D., Martin P. Grobusch, MD, Ph.D., Jorge M. de los Rios, MD, Eduardo Gotuzzo, MD, Irina Vasilyeva, MD, Ph.D., Vaira Leimane, MD, Koen Andries, DVM, Ph.D., Nyasha Bakare, MD, MPH, Tine De Marez, Ph.D., Myriam Haxaire-Theeuwes, DDS, Nacer Lounis , Ph.D., Paul Meyvisch, M.Sc., Els De Paepe, M.Sc., Rolf P.G. van Heeswijk, Pharm.D., Ph.D., and Brian Dannemann, MD Multidrug-Resistant Tuberculosis and Culture Conversion with Bedaquiline. N Engl J Med 2014; 371:723-732. August 21, 2014.
Literature.
- Global tuberculosis report 2013. Geneva: World Health Organization
- Zumla A, Abubakar I, Raviglione M, et al. Drug-resistant tuberculosis - current dilemmas, unanswered questions, challenges, and priority needs. J Infect Dis 2012;205:Suppl 2:S228-S240
Special instructions for the use of the drug Cycloserine
Use with caution in children. The toxic effect of cycloserine can be prevented or reduced by prescribing glutamic acid 0.5 g during treatment 3-4 times a day (before meals), and daily intramuscular administration of the sodium salt of ATP (1 ml of 1% solution). During treatment, it is necessary to monitor renal function (level of creatinine and urea nitrogen in the blood serum), the concentration of cycloserine in the blood serum (should not exceed 30 mcg/ml). Due to the rapid development of resistance during monotherapy with cycloserine, its combination with other anti-tuberculosis drugs is recommended.
Overdose of the drug Cycloserine, symptoms and treatment
Overdose phenomena are observed when the concentration of cycloserine in the blood plasma is 30 mg/ml and higher (taking high doses, impaired renal clearance). Acute poisoning can occur when more than 1 g/day is ingested. Symptoms: headache, dizziness, confusion, increased irritability, paresthesia, psychosis, dysarthria, paresis, convulsions, coma. Treatment is symptomatic. To prevent neurotoxic effects, pyridoxine is administered at a dose of 200–300 mg/day. Hemodialysis is not effective.
List of pharmacies where you can buy Cycloserine:
- Moscow
- Saint Petersburg